
Abstract
Objective:
To validate the International Classification of Functioning, Disability and Health (ICF) Core Set for individuals with spinal cord injury (SCI) in the early post-acute and long-term context from the perspective of physical therapists.
Setting:
International.
Methods:
Physical therapists experienced in the treatment of SCI were asked about problems, resources and aspects of the environment treated by them, in a three-round electronic mail survey using the Delphi technique. Responses were linked to the ICF by two researches; κ-coefficient was calculated as statistical measure of agreement.
Results:
In all, 81 experts from 27 countries named 3694 concepts. They were linked to 187 ICF categories for the early post-acute context. Three ICF categories from the component body function, five ICF categories from the component body structures and two ICF categories from the component activities and participation were not represented in the ICF Core Set for the early post-acute context. In all, 207 ICF categories were linked for the long-term context. Four ICF categories from the component body function, five ICF categories from the component body structures and two ICF categories from the component activities and participation were not represented in the ICF Core Set for the long-term context.
Conclusion:
Physical therapists addressed a vast variety of problems that they take care of in their interventions in patients with SCI. The Comprehensive ICF Core Sets covered a high percentage of these problems. Further research is necessary on several responses not covered in the ICF.
Similar content being viewed by others


Introduction
Patients with spinal cord injury (SCI), experience abruptly and often permanently, personal, bio-psychological and socioeconomic consequences.1 Decisions regarding medical care and rehabilitation can lead to tremendous annual and lifetime costs.2 Thus, it is important to optimize health services including rehabilitation care to restore the functioning and health of the patients. Interdisciplinary communication and collaboration among health professionals are fundamental owing to the complexity of the problems involved in SCI.
A mutual basis for multidisciplinary collaboration is the International Classification of Functioning, Disability and Health (ICF), which represents a comprehensive and universally accepted framework for describing functioning, disability and health in persons with all kinds of health conditions including SCI.3 According to the ICF, the problems associated with a disease may concern body functions and body structures, as well as activities and participation in a person's life situation, which are then modified by contextual factors such as environmental and personal factors. The detailed hierarchical structure of the contents of the ICF is presented in Figure 1.

Structure of the ICF.
In order to facilitate the implementation of the ICF into the SCI rehabilitation process, ‘ICF Core Sets’ for individuals with SCI in the early post-acute4 and the long-term context5 have been developed. These ICF Core Sets include selections of ICF categories relevant to patients with SCI in the early post-acute context comprising 162 categories and in long-term context of care comprising 168 categories. Based on the work definition used during the development of ICF Core Sets for SCI, the post-acute context commences when multidisciplinary comprehensive rehabilitation starts and finalized with its completion. The subsequent phase is the long-term context.
The standard approach for the development of ICF Core Sets was based on the evidence from preparatory studies followed by a formal decision-making and consensus process, which is then followed by a validation phase. Key aspect of the validation is whether the problems addressed by health professionals involved in a multidisciplinary team are included in the ICF Core Sets for SCI. An essential group of professionals involved in the treatment of patients with SCI in all different health care contexts are physical therapists.6
The objective of this study is to validate the ICF Core Set for SCI in the early post-acute and long-term context from the perspective of physical therapists.
Methods
Study design
The study was conducted as a worldwide electronic-mail survey applying a three-round Delphi technique with invited physical therapists. The Delphi technique enabled experts to repeatedly access the group, explore the complex issue aiming to obtain consensus.7
Recruitment
Persons with specific training as physical therapist and experience in the field of SCI were eligible to participate in this study.
Initially, physical therapy associations, universities, model care units, hospitals and other institutions were identified by internet search and contacted worldwide. To identify experts, author search was undertaken and personal recommendations were followed up. Experts were invited to recommend other physical therapists with expertize in SCI (snow-ball system). Possible participants received an information pack with study details and had to confirm their consent in order to be included in the study.
Delphi process
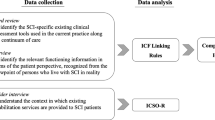
In the first Delphi round, the experts received an open-ended questionnaire. Physical therapists were asked to list problems, resources and aspects of the environment in treating patients with SCI, first for the early post-acute and second for the long-term context (Figure 2). Answers were tabulated and linked to the ICF (see below ‘Linking’). In addition, experts completed questions on demographic characteristics and professional experience. In Delphi round two, experts had to decide whether to agree that the respective ICF categories represent patients’ problems, patients’ resources or aspects of environment treated by physical therapists in patients with SCI.

The Delphi survey.
In order to maintain motivation of the participants, only a selection of the ICF categories from the second round were included in round three. A modified scree test was applied to identify ICF categories, which did not reach sufficient consensus.8 A graph was plotted containing the percentages of expert agreement (ordinate) for each ICF category (abscissa). The scree line was placed onto the downward slope, along the points to see where they approximately form a straight line. Points close to the scree line indicated an insufficient endorsement and were included into Delphi round three.
In Delphi round three, the ratings were tabulated with frequencies of answers from the previous round to inform about the decisions other experts made. Experts were requested to reconsider their answers. Within the Delphi process, experts were returning their responses within 3–5 weeks for each round.
Linking
Each response of the first Delphi round was linked according to the linking rules established9 to the most precise ICF category by two researchers. Each ICF category is coded with a prefix for the components body functions (b), body structures (s), activities and participation (d) and environmental factors (e) and a suffix of one to five digits (Figure 1). Disagreements were discussed with supervisors and a joint decision was made. According to the ICF definition, personal factors were coded as personal factors. Concepts that could not be assigned to ICF categories were coded as not covered.
Data analyses
Descriptive statistics characterize the sample and frequencies of ratings. κ-coefficient was calculated with bootstrapped confidence intervals to analyze the agreement between the two researchers linking the answers of the participants to the ICF.10
ICF categories, which reached an agreement of more than 75% among the participants in the final Delphi round, were considered for comparison with the Comprehensive ICF Core Set for SCI. As no universal agreement on the level of consensus exists, based on experiences from previous studies, this cutoff point was considered as appropriate consensus to be achieved.
Results
Recruitment
A database of experts in SCI worldwide was used. From the 254 experts out of this database, 21 physical therapists agreed to participate. Additional 48 experts were suggested by this group and agreed to participate. In all, 146 associations were contacted and newsletters or emails were sent to their members. Out of 341 individually invited specialists, 22 agreed to participate. Of the 12 experts found by author search, two agreed. In all, 54 institutions were contacted, 12 experts were recruited. From the 105 recruited experts, 98 persons out of 27 countries were eligible for inclusion and agreed to participate in the Delphi survey. Table 1 details the attrition of participants between the Delphi rounds, demographics and professional experience.
Delphi process
The Delphi survey was conducted from April to August 2009. The first-round questionnaire was returned by 86.7% of the participants, seven questionnaires were excluded because they were not completed and six questionnaires were not returned for unknown reasons. The second-round questionnaire was returned by 95.2% of the experts. According to the scree test, 102 categories for the early post-acute and 70 categories for the long-term context with inexplicit consensus among the second-round participants were included for round three. The response rate for the third round was 100%.
Linking
In Delphi round one, 3694 patients’ problems, resources or aspects of environment treated by physical therapists in SCI were named for the early post-acute and long-term context. The answers were linked to 187 ICF categories for the early post-acute and 207 for the long-term context (Tables 2,3,4,5). In all, 45 answers were linked to the personal factors; 34 concepts for the early post-acute and 26 answers were linked for the long-term context (Table 6). In all, 13 responses were found to be not covered by the ICF; 10 concepts for the early post-acute and six for the long-term context (Table 7).
The κ-statistics with bootstrapped confidence interval for the linking was for the early post-acute 0.77 (0.75–0.80) and for the long-term context 0.79 (0.76–0.82).
Representation of responses of physical therapist in the Comprehensive ICF Core Sets for SCI
In total, 187 ICF categories for the early post-acute context and 207 for the long-term context linked to the responses of participants reached an agreement of more than 75% in the final round and were considered for comparison with the current Comprehensive ICF Core Set for SCI.
From the component body functions, 60 categories are represented in the ICF Core Set for the early post-acute context and for the long-term context, 53 categories are represented (Table 2). Few responses for the early post-acute context were linked to third level categories, for example, b4550 general physical endurance or b4551 aerobic capacity, and are represented in the ICF Core Set by the corresponding second level category b455 exercise tolerance function. For the long-term context, answers were linked to a third level category, for example, b2700 sensitivity to temperature is represented by a second level category such as b270 sensory functions related to temperature and other stimuli. For the early post-acute context, three categories were not represented in the ICF Core Set, namely b1646 problem solving, b1801 body image and b4352 functions of the lymphatic vessels. For the long-term context, four categories: b410 heart functions, b450 additional respiratory functions, b755 involuntary movement reaction functions and b7650 involuntary contractions of muscle, were not represented in the respective ICF Core Set.
From the component body structures, 15 categories for the early post-acute context and 11 categories for the long-term are included in the ICF Core Set (Table 3). Few third level categories are represented in the ICF Core Set by a second level category, for example, s4300 trachea, s4031 lungs and s4303 muscles of respiration are represented by s430 structure of the respiratory system. Suggested second level categories of the experts are represented in the ICF Core Set on the fourth level such as s120 spinal cord related structures. Five ICF categories for both the early post-acute and the long-term context are not included, namely s770 additional musculoskeletal structures related to movement, s7700 bones, s7701 joints and s7703 extra-articular ligaments, fasciae, extra muscular aponeuroses so on.
From the component activities and participation, 53 categories mentioned by experts in the early post-acute and 81 in the long-term context are represented in the ICF Core Set (Table 4). Some categories are represented on a different level of classification, for example, in the long-term context, d455 moving around is represented by d4550 climbing, d4551 running, d4552 jumping and d4553 swimming. In some cases, third level categories in the ICF Core Set are represented on the second level, for example, d440 fine hand use was represented more detailed by pulling, pushing, reaching, catching, turning and twisting. Three ICF categories, d175 solving problems, d435 moving objects with lower extremities for the long-term context and d6504 maintaining assistive devices for the early post-acute context are not represented in the ICF Core Set.
From the component environmental factors, all ICF categories with an agreement >75% are represented in the ICF Core Set, namely 25 ICF categories from the early post-acute and 23 from the long-term context (Table 5).
In all, 25 responses for the early post-acute context and 21 for the long-term context were assigned to the not-yet developed ICF component personal factors and reached an agreement surpassing 75% (Table 6). In all, 13 responses, which reached an agreement >75% were not covered by the ICF (Table 7).
Discussion
We found that the categories of the current versions of the ICF Core Sets for SCI were largely representing what physical therapists agreed upon to take care of in their interventions. Some ICF categories regarding the body functions were not included in the ICF Core Set. For the early post-acute context, the experts mentioned b4352 functions of lymphatic vessels. There is evidence to support the expert opinion. Lymph drainage as a therapeutic intervention is aiming to reduce the volume of edema, as well as pain and increasing the range of motion and activating the regeneration of new lymphatic vessels in scarred tissue.11
The experts agreed that b1801 body image is a problem they take care of. Physical impairments are resulting in a changed body, and strongly affect physical and social-psychological well being and performance.12 Body composition may impact satisfaction with physical appearance for some women.13 First, sports therapy has the effect of increasing and developing a new body image and body scheme.12 Second, for example, cognitive-behavioral-therapy is a tool to strengthen physical therapy.14 Physical therapists are increasingly offered cognitive-behavioral-therapy courses for improvement of patient care.15 It can be useful in physical therapy treatment units to help the patients to learn more effective ways to overcome the difficulties that contribute to their distress.14 This leads directly to the ICF category b1646 problem solving, which addresses the mental functions of identifying, analyzing and integrating incongruent information into a solution. Effective problem solving reduces depressive behavior and psychosocial impairment and leads to assertiveness16 irrespective of the onset of injury. Related to this finding, the category of the component activity and participation d175 solving problems was supported by experts for the early post-acute and long-term context. It is used in the sense of finding solutions by identifying and analyzing issues.17
For the long-term context, experts agreed that b450 additional respiratory functions, b755 involuntary movement reaction functions and b7650 involuntary contractions of muscles are problems treated by physical therapists. Involuntary movement reactions are induced by the body position, balance or threatening stimuli affecting the whole body or large muscles. Involuntary contractions of muscles affect one muscle or muscle group and are not intentional.18
The category b410 Heart functions, was mentioned for the long-term context. In fact, abnormal heart rates and rhythms are commonly present after a spinal cord injury. People with SCI experience poor venous return and lower limb blood pooling, resulting from a lack of sympathetic tone and a reduced muscle pump in the lower extremity. Consequently, the increase of aerobic performance by increasing lower limb strength and cycle endurance performance or functional electric stimulation is a common intervention goal in rehabilitation.19 Physical therapists decide on the intensity and type of exercise they prescribe as part of a plan of care. Exercise is an important component of evidence-based treatment in physical therapy settings and is an essential component of improving health.20
The ICF categories from the component body structures not represented in the ICF Core Set are identical for early post-acute and long-term context. The ICF categories s770 additional musculoskeletal structures related to movement, as well as detailed categories s7700 bones, s7701 joints, s7702 muscles and s7703 extra-articular ligaments, Fasciae and so on were identified by the experts to represent problems treated by physical therapists. The impact of musculoskeletal diseases on the overall function and well being of a person with SCI cannot be overstated.21
In our survey, a large number of personal factors were identified mainly related to health conditions or were related to age, coping or adapting to the new role. Personal factors are not classified in the ICF yet. There is consensus in the literature that personal factors are influential to the degree of functioning, disability and well being.22 Thus, it could be useful to develop the ICF component, personal factors, to enable health professionals to comprehensively and systematically describe relevant aspects influencing a patient's functioning and health.
Regarding methodological strengths and limitations, the following aspects should be considered. The Delphi technique was an appropriate method for this study objective. With a total response rate of 82.7%, the criterion of a minimum 70% response rate was clearly exceeded.7 According to the κ-coefficient, there was substantial agreement of the two researchers who performed the linking process. This finding supports the reliability of the study.
However, a potential selection bias cannot be excluded. Random sampling was not possible as no database is available with sufficient number of the targeted population. There is evidence that the Delphi method rather employs experts in the area of interest.7 Furthermore, there are limitations in the external validity. Although physical therapists from all WHO world regions participated, there was an underrepresentation of South East Asia, and the Eastern Mediterranean region. It is possible that health services are not yet established for SCI. Language barriers might have been another reason, as the Delphi survey was conducted in English language only.
A majority of problems treated by physical therapists were covered by the Comprehensive ICF Core Sets for SCI. Few shortcomings concerning body functions, structures, activities and participation and personal factors were disclosed. However, this study supports that the Comprehensive ICF Core Sets in SCI are relevant to the clinical practice of physical therapists. The Comprehensive ICF Core Sets in SCI provide a useful basis for clinical practice to describe and classify functioning, health and disability with a common framework and language. Further results on the validity of the ICF Core Sets will be available from studies involving perspectives from occupational therapists, physicians, psychologists, nurses and social workers.
References
Wyndaele M, Wyndaele JJ . Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord 2006; 44: 523–529.
Ackery A, Tator C, Krassioukov A . A global perspective on spinal cord injury epidemiology. J Neurotrauma 2004; 21: 1355–1370.
World Health Organization. International Classification of Functioning, Disability and Health: ICF. WHO: Geneva, 2001.
Kirchberger I, Cieza A, Biering-Sørensen F, Baumberger M, Charlifue S, Post MW et al. ICF Core Sets for individuals with spinal cord injury in the early post-acute context. Spinal Cord 2010; 48: 297–304.
Cieza A, Kirchberger I, Biering-Sørensen F, Baumberger M, Charlifue S, Post MW et al. ICF Core Sets for individuals with spinal cord injury in the long-term context. Spinal Cord advance online publication 2010; 48: 305–312.
Sullivan PE, Markos PD . Clinical Decision Making in Therapeutic Exercise. Appleion & Lange: East Norwalk, Conn, 1995, pp 1–11.
Sharkey SB, Sharples AY . An approach to consensus building using the Delphi technique: developing a learning resource in mental health. Nurse Educ Today 2001; 21: 398–408.
Zoski K, Jurs S . Priority determination in surveys. An application of the scree test. Eval Rev 1990; 14: 214–219.
Cieza A, Geyh S, Chatterji S, Kostanjsek N, Ustün B, Stucki G . ICF Linking rules: An update based on lessons learned. J Rehabil Med 2005; 37: 212–218.
Vierkant RA . SAS Macro for Calculating Bootstrapped Confidence Intervals about a Kappa Coefficient 2004. http://www2.sas.com/proceedings/sugi22/STATS/PAPER295.PDF (accessed 21.2.2010).
Zäch GA, Koch HG . Paraplegie. Ganzheitliche Rehabilitation. Karger: Basel, 2006, pp 370.
Chau L, Hegedus L, Praamsma M, Smith K, Tsukada M, Yoshida K et al. Women living with a spinal cord injury: Perceptions about their changed bodies. Qual Health Res 2008; 18: 209–221.
Bassett RL, Ginis KM, Buchholz AC . A pilot study examining correlates of body image among women living with SCI. Spinal Cord 2009; 47: 496–498.
Donaghy M, Nicol M, Davidson K . Introduction. In: Donaghy M, Nichol M, Davidson K (eds). Cognitive Behavioural Interventions in Physiotherapy and Occupational Therapy, 1st edn. Butterworth Heinemann Elsevier: Edinburgh, 2008, pp XIII.
The Chartered Society of Physiotherapy. The Scope of Practice of Physiotherapy. PA44. 2004, pp 1–11. http://www.csp.org.uk/uploads/documents/csp_physioprac_pa44.pdf (accessed 15.3.2010).
Elliott TR, Godshall FJ, Herrick SM, Witty TE, Spruell M . Problem-solving appraisal and psychological adjustment following spinal cord injury. Cognit Ther Res 1991; 15: 387–398.
May L, Day R, Warren S . Evaluation of patient education in spinal cord injury rehabilitation: Knowledge, problem-solving and perceived importance. Disabil Rehabil 2006; 28: 405–413.
Butler JE, Godfrey S, Thomas CK . Depression of involuntary activity in muscles paralyzed by spinal cord injury. Muscle Nerve 2006; 33: 637–644.
Phillips WT, Kiratli BJ, Sarkarati M, Weraarchakul G, Myers J, Franklin BA et al. Effect of spinal cord injury on the heart and cardiovascular fitness. Curr Probl Cardiol 1998; 23: 641–716.
Scherer S . Addressing cardiovascular risk as part of physical therapist practice—What about Practice recommendations for Physical therapists?. 2009; 20: 27–29.
Goldstein B . Musculoskeletal conditions after spinal cord injury. Phys Med Rehabil Clin N Am 2000; 11: 91–108.
Duggan CH, Albright KJ, Lequerica A . Using the ICF to code and analyse women's disability narratives. Disabil Rehabil 2008; 30: 978–990.
Acknowledgements
This project was partly funded by Swiss Paraplegic Foundation, Nottwil, Switzerland. We like to thank the participants in the Delphi Survey for their valuable contribution and their time in responding to the demanding questionnaires: Patricia Anthamatten-Burchhard, Marika Augutis, Matthew Azzopardi, Carey Bayliss, Liron Bensimon, Albert Besseling, Matt Buck, Salome Cronje, Huong Dang Thi Thu, Marisa Debattista, Nejla Essafi El Khadiri, Edelle Field-Fote, Barbara Garrett, Liliana Geyser, Manuel Grote, Claire Guy, Kirsten Hart, Lisa Harvey, Rita Henn, Diana Herrington, Benita Hexter, Muzaffor Hossain, Ieva Jamontaitë, Linda Kealey, Ilke Keser, Daniel Kuhn, Umme Kulsum Urmi, Suraj Kumar, Jonathan Kwan, Stephanie Kwok, Jackeline LaBarbera, Irene Lange, Paula Leppänen, Richard Levi, Mirda MacLachlan, Susan MacLeod, Veronica Mamabolo, Lucy Maugham, Janet McCarthy, Isa McClure, Kym McCrea, Shari McDowell, Marina Momen, Sarah Morrison, Witness Mudzi, Akmer Mutlu, Audrey Natale, Lieu Nguyen Thanh, Rudy Niebuhr, Vanessa Noonan, Shohreh Noorizadeh Dehkordi, Malin Nygren-Bonnier, Sue Paddison, Paola Paglierani, Michelle Read, Kerstin Rolle, Jack Ross, Jean-Luc Rossier, Sarianna Savolainen, Carsten Schäfer, Amy Schulz, Boaz Shamir, Josh Simmons, Melanie Skeen, Fred Smedes, Nina Strydom, Sally Taylor, Joy Teo, Rajendra Thapa, Pam Thirlwell, Lasse Thulstrup, Claire Trask, Andrea Marilyn Trout, Jau-Yih Tsauo, Sacha van Langeveld, Anne von Reumont, Natasha Wall, Robert Wellmon, Eric Weerts, Josh Williams, Sultan Yousaf, Anne Zwahlen. The authors also thank Cristina Bostan from the ICF Research Branch in Munich for her most helpful contribution.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Herrmann, K., Kirchberger, I., Stucki, G. et al. The Comprehensive ICF core sets for spinal cord injury from the perspective of physical therapists: a worldwide validation study using the Delphi technique. Spinal Cord 49, 502–514 (2011). https://doi.org/10.1038/sc.2010.155
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.155
Keywords
This article is cited by
-
Content comparison of the Spinal Cord Injury Model System Database to the ICF Generic Sets and Core Sets for spinal cord injury
Spinal Cord (2019)
-
Rehabilitation goals of people with spinal cord injuries can be classified against the International Classification of Functioning, Disability and Health Core Set for spinal cord injuries
Spinal Cord (2016)
