
Abstract
Study design:
Cross-sectional survey.
Objective:
To identify barriers and facilitators to employment after spinal cord injury (SCI) and their relationship with labor force participation.
Methods:
Participants were initially identified through specialty hospitals in the Midwest and Southeastern United States of America. 781 adults with traumatic SCI, at least 1 year post-injury, and between the ages of 18–64, participated. A 30-item instrument on barriers and facilitators to employment was administered. Analyses included exploratory factor analysis (EFA), confirmatory factor analysis (CFA) and comparisons of scores as a function of employment status.
Results:
EFA indicated six primary themes (root mean square error of approximation (RMSEA)=0.040), including: (a) resources, (b) health status, (c) disability considerations, (d) lack of importance, (e) disincentives and (f) motivation. CFA indicated an acceptable fit (RMSEA=0.078). Univariate analyses indicated each item and factor was significantly different as a function of labor force participation. After controlling for biographical and injury factors, multinomial logistic regression indicated three factors significantly differentiated those never employed, those currently unemployed but had worked since injury and those currently employed. Those employed reported higher scores for resources and motivation and lower scores for lack of importance.
Conclusions:
Barriers and facilitators were consistently related to labor force participation, with facilitators more highly related to labor force participation than barriers. Although loss of financial and medical benefits (disincentives) as well as health status have been reported as barriers to employment, they were not as highly correlated with labor force participation as were other factors.
Similar content being viewed by others

Introduction
Employment rates after spinal cord injury (SCI) continue to fall well below that of pre-injury rates and those of the general population.1, 2 Participation in the labor force is important to adult life, and lower employment rates after SCI are indicative of diminished labor force participation. This should be of concern to rehabilitation professionals as labor force participation is highly correlated with both quality of life and life expectancy after SCI.1, 3, 4
A large body of research has identified predictors of employment using mostly biographic, injury and educational characteristics. Recent reviews have been conducted. For instance, Anderson et al.5 identified 14 factors related to employment after SCI including: age, sex, marital status, race, injury severity, time since injury, vocational counseling, employer's attitudes, employment type, education, social support, medical problems, psychological state and environment. Despite this body of research, relatively few studies have specifically focused on barriers and facilitators to employment.
Kewman and Forchheimer6 asked unemployed participants why they felt they were not working. The most common barriers related to injury severity (70%), disincentives (55%) and needs for greater assistance (55%). Similar results were reported in a second study,7 as declining health was related to an increase in barriers to employment. The largest number of barriers was reported by those with the highest number of years post-injury and those with the oldest age at injury. Krause and Anson8 also found physical limitations were related to unemployment, with inability to perform the same type of work being a major barrier.
Krause and Picklesimer9 conducted a longitudinal study of 343 unemployed participants to determine what portion were employed at follow-up. Participants were administered a 30-item checklist of barriers to employment and two items regarding future work intentions. At 5 years after the baseline assessments, just over 10% were working. The two primary perspective predictors of employment at follow-up were maintaining hope for employment and actively seeking employment. Health limitation barriers at baseline (pressure ulcers, poor health and not being physically capable to work) were the most significant barriers to employment at follow-up. Disincentives and lack of resources were not significantly correlated with employment 5 years later.
Our purpose was twofold: (a) identify the underlying dimensions of a 30-item measure of barriers and facilitators to employment, and (b) identify the relationship of barriers and facilitators with labor force participation. The unique contribution of this study is the inclusion of both employed and unemployed participants and the direct comparison of barriers and facilitators as a function of current and post-injury employment status.
Methods
Participants
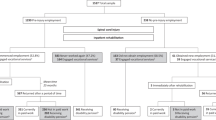
All participants were identified from outpatient records of hospitals in the Midwestern and Southeastern USA. This longitudinal study was initiated in 1973, with new participant cohorts added approximately every 10 years. There were three inclusion criteria: (1) traumatic SCI, (2) minimum 1-year post-SCI onset and (3) minimum age of 18 years. There were 952 participants during the current data collection (61.7% overall response rate). All those over the traditional retirement age of 65 were excluded, leaving a final sample of 781. Although participants were enrolled dating back to 1973, all data were collected during the most recent follow-up (2008–2010).
Procedures
Cover letters were sent to describe the study and alert participants materials were forthcoming. The survey itself was sent ∼4–6 weeks later. There was a second mailing to all non-respondents, followed by a phone call for those who had known numbers. Some participants had lost or discarded materials and requested an additional packet of materials be sent. Participants received $30 remuneration.
Measure
We used a 30-item self-report measure of barriers and facilitators to employment. Each item is measured on a 5-point likert scale ranging from strongly disagree to strongly agree. The items were adapted from a checklist administered to unemployed participants in a previous study.10 There is no data on test-retest reliability.
Analysis
Data were analyzed using a combination of SPSS11 and Mplus.12 The first set of analyses (using SPSS) was descriptive in nature. Second, we compared respondents and non-respondents on demographic and injury related items to better understand the nature of attrition. We then compared item responses as a function of employment status utilizing three categories: (a) currently employed; (b) unemployed but worked previously and (c) chronically unemployed (never employed after SCI). One-way analysis of variance was used to identify differences between the three groups on responses to each item.
The participant sample was randomly divided into two groups for factor analysis (60/40% split). We used exploratory factor analysis (EFA) with maximum likelihood extraction.13 The χ2 and root mean square error of approximation (RMSEA) were used to evaluate model fit. RMSEA reflects the discrepancy per degrees of freedom, with <0.05 representing an excellent fit and 0.05–0.08 representing good fit.14 We used a Promax rotation (Varimax followed by Procrustean targets) so the resultant factors could have a simple structure and be correlated.15 We looked at multiple indicators of fit, including eigenvalues, RMSEA and a minimum number of factors with loadings from only two items.
Confirmatory factor analysis (CFA) was run on the second subsample. When using CFA, the items and factors are specified a priori based on findings from previous analyses. This represents a more rigorous test of the stability of the factor structure across subsamples. Whereas factor loadings of 0.35 and higher were maintained from the EFA, only those with loadings of 0.40 and higher were retained following the CFA. RMSEA was used as the criterion for fit. Alpha coefficients were generated for each factor. Analysis of variance was used to identify the relationship of the factors with labor force participation.
Last, we used multinomial logistic regression to identify the optimal predictors of labor force participation. Those chronically unemployed were used as the reference group. Odds ratios with confidence intervals were reported between the three groups. The predictor variables included age, race, gender, years since injury, injury severity, years of education and the (six) scales identified from the factor analysis of barriers and facilitators. The referent groups were white (race), male (gender) and ambulatory (injury severity). Ambulatory participants were grouped regardless of neurological level and the other three groups were broken down according to neurological level as follows: C1–C4, C5–C8 and non-cervical.
Statement of ethics
We certify all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Results
Comparison of responders and non-responders
Those with the most severe SCI (C1–C4, non-motor functional) were less likely to respond to follow-up (47% compared with 61–63%), χ2 (3, n=1461)=14. 5, P<0.01. Respondents also had more education (13.0, 14.0), were younger at injury (28.1, 31.1), and had more years post-injury (14.4, 16.2). Gender, race and current age were not significant.
Descriptive
Most participants were male (77.1%) and white (77.1%). Motor vehicle crash was the primary etiology (53.0%). Cervical injuries were reported by 51.5%. The average age was 47.3 years, and the average number of years since SCI onset was 21.7 (average age at injury onset was 25.6). Participants averaged 14.3 years of education. In all, 39% were gainfully employed; another 29% were unemployed but had worked previously since SCI onset and the remaining 32% were chronically unemployed. Table 1 summarizes the pattern of agreement with the items.
Measurement model
Six factors were derived using EFA with an excellent fit (RMSEA=0.040; Table 2) and eigenvalues of >1.0. Therefore, six factors were retained in the final solution. One factor was measured by only two items. The CFA for the 6-factor solution indicated an acceptable fit (RMSEA=0.078). We considered a 5-factor solution, as it also had an excellent fit with the EFA (RMSEA=0.049) and would have circumvented the issue of having a factor with less than three items loading. However, it did not produce an acceptable fit upon CFA (RMSEA=0.083).
The first factor appeared to represent availability of resources with items regarding sufficiency of education/training, transportation and other resources. The second factor related to health status, with prominent concerns about stamina, endurance and fatigue. Disability considerations reflected concerns about working with SCI (inaccessibility, employer bias, knowledge of appropriate jobs). Lack of importance included no interest in working, having had a large settlement, family influence and doing other important activities. The fifth factor was financial and medical benefit disincentives. Last, motivation had loadings from items reflecting value placed on working and confidence in ability to work. Alpha coefficients ranged from a low of 0.68 for lack of importance to a high of 0.87 for health status. The average coefficient was 0.79.
Univariate analysis
All items were statistically significant between the three labor force participation groups, with only three items not significant at the P<0.001 level (Table 3). When comparing the six scales among the three groups, all scales were statistically significant. Post hoc contrasts differentiated all groups for all items, except disincentives (there were no differences between those chronically unemployed and those who were unemployed but had worked since SCI onset).
Predictors of labor force participation
The multinomial logistic regression differentiated those who were chronically unemployed (the referent group) with those who were unemployed but had worked post-injury (Table 4, part 1) and those currently employed (Table 4, part 2). Years of education, years post-injury and a less severe SCI were associated with a greater likelihood of having worked since SCI onset. Those who had been employed since SCI onset reported higher levels of motivation and resources and lower scores for lack of importance compared with those chronically unemployed. Gender, race, age and the three other types of barriers and facilitators were not statistically significant in the regression analysis.
A similar, but not identical, pattern of differences was observed between those who were currently employed and those chronically unemployed. Years of education and years since injury were associated with current employment. Compared with those who were ambulatory, those with cervical non-motor functional injuries had significantly greater odds of being unemployed (C1–C4: 6.42, C5–C8: 4.12). Whites had 6.54 greater odds of current employment. Levels of motivation, resources and placing a greater importance on employment were associated with current employment. Age, gender, disability considerations, health and disincentives did not differentiate between the two groups.
Discussion
This study builds upon previous research on factors related to labor force participation after SCI6, 7, 8, 9 by identifying: (a) endorsement rates of barriers and facilitators, (b) underlying themes for barriers and facilitators and (c) the relationship between barriers and facilitators with labor force participation after SCI. The findings will help rehabilitation professionals to understand factors that limit and facilitate labor force participation after SCI and provide improved services to promote better outcomes.
Item endorsements suggest the majority of those with SCI who are within the normal working ages (between 18–64) feel capable of working, are motivated to work, and do not see disincentives as significant barriers to employment. First, over 70% of the participants felt they had sufficient education or training to be employed, and 55% reported they had all the necessary resources to maintain a regular job (transportation, assistants, so on). Education is widely acknowledged to be a primary facilitator of labor force participation after SCI.1, 16, 17, 18, 19 Similarly, the majority of participants reported they indeed felt capable of working and were motivated to work. For instance, 60% of the participants agreed with the statements that they were capable of working and that work was worth the effort. Although disincentives have been described as a prominent barrier to labor force participation, <40% of the participants agreed with such statements. Responses to these items suggest that disincentives were not a barrier to employment for the majority of the sample.
The factor analysis identified six stable factors that were retained after the CFA based on reasonable model fit and acceptable internal consistency. The factors appear to be meaningful in terms of their explanatory value in summarizing the themes underlying barriers and facilitators of employment. The themes themselves reflect a combination of personal factors, such as interest in working and confidence and motivation to work, availability of appropriate resources required to work, specific disability related factors related to work, disincentives and health factors.
Comparisons of items and factor scores as a function of labor force participation indicated that virtually all variables differentiated between those who were currently employed, those unemployed but previously employed since SCI onset, and those who have never been employed since SCI onset. This is powerful evidence for the importance of diverse barriers and facilitators to employment. However, the regression analysis provides greater insight as to the relative importance of the barriers and facilitators and highlights the most important factors after controlling for demographic, injury and educational characteristics.
In sum, the majority of participants perceived themselves capable and motivated to work. In all, 68% of participants had worked since SCI onset. The remaining 32%, who were chronically unemployed, reported significant barriers. Individuals who have worked post-injury but are currently unemployed may be the best candidates for interventions to promote employment since they report fewer barriers and more facilitators than those who are chronically unemployed. Those who are both chronically unemployed and who report significant barriers to employment are the most challenging cases with little likelihood of return to employment.
Limitations
There are several noteworthy study limitations. First, all data are self-report, and this type of data is prone to recall bias. In the current study, such bias would be limited to reporting of actual employment history, as data on barriers, by definition, relate to perceptions by the individual. Second, as with all self-report studies, participation is selective. Our response rate was acceptable (61.7%, a portion of non-response was because of mortality), but must be kept in mind when interpreting the percentage of participants reporting they were employed or reporting a specific barrier or facilitator. The relative frequencies of reported barriers or facilitators and the comparisons between those who are employed and unemployed are more valid than absolute interpretations of the frequencies themselves (that is, they are not population data). Third, participants were selected from two regions—the Midwest and Southeast USA. Barriers and facilitators may vary by geographic location both within the USA and around the globe, so the findings need to be validated in other geographic areas. Fourth, the study focused only on SCI, although this type of analysis would be important with participants who have other disabling conditions. Fifth, there is no data on temporal stability. Sixth, participant attributions may be biased when taken as indicators of objective barriers or facilitators. For example, two individuals may face the same disincentives, yet may perceive the disincentives differently in terms of the extent to which they represent a barrier to employment.
Future research
Additional studies are needed expanding the scope of the study population. Will the same pattern of barriers and facilitators be observed among other cohorts with different disabling conditions, demographic profiles or geographic locations? Another need is for longitudinal research identifying the association of endorsement of barriers and facilitators with future labor force participation. Will endorsement patterns change among those whose labor force participation changes? Will the endorsement patterns be useful in predicting future labor force participation? These questions have to do with the predictive value of current barriers and facilitators. One would expect those who report fewer barriers and identify more facilitators would be more likely to begin labor force participation. This is an empirical question. Last, research is needed utilizing this information to design interventions to limit barriers and promote facilitators to labor force participation. It is most likely that those who either have been employed at some time since SCI onset but are currently unemployed and those who report fewer barriers will be better candidates for intervention. It is only through steadfast research that we will be able to improve the labor force participation outcomes of those with SCI and other disabling conditions.
References
Anderson CJ, Vogel LC . Employment outcomes of adults who sustained spinal cord injuries as children or adolescents. Arch Phys Med Rehab 2002; 83: 791–801.
Athanasou JA, Brown DJ, Murphy GC . Vocational achievements following spinal cord injury in Australia. Disabil Rehabil 1996; 18: 191–196.
DeVivo MJ, Krause JS, Lammertse DP . Recent trends in mortality and causes of death among persons with spinal cord injury. Arch Phys Med Rehab 1999; 80: 1411–1419.
Krause JS . Employment after spinal cord injury. Arch Phys Med Rehab 1992; 73: 163–169.
Anderson D, Dumont S, Azzaria L, Le Bourdais M, Noreau L . Determinants of return to work among spinal cord injury patients: A literature review. J Voc Rehab 2007; 27: 57–68.
Kewman D, Forchheimer M . Factors predicting return to work 3 to 6 years following spinal cord injury. SCI Psychosocial Process 1998; 10: 152.
Krause JS . Aging and self-reported barriers to employment after spinal cord injury. Top Spinal Cord Inj Rehabil 2001; 6: 101–115.
Krause JS, Anson CA . Self-perceived reasons for unemployment cited by persons with spinal cord injury: relationship to gender, race, age and level of injury. Rehabil Counsel Bull 1996; 39: 217–227.
Krause JS, Pickelsimer E . Relationship of perceived barriers to employment and return to work five years later. A pilot study among 343 participants with spinal cord injury. Rehabil Counsel Bull 2008; 51: 118–121.
Krause JS, Coker JL . Aging after spinal cord injury: a 30-year longitudinal study. J Spinal Cord Med 2006; 29: 371–376.
SPSS for Windows. SPSS for Windows, 17.0 ed. Chicago, IL: SPSS Inc., 2009.
Muthen L, Muthen B . Mplus, The Comprehensive Modeling Program for Applied Researchers User's Guide, 4th edn Muthen & Muthen: Los Angeles, CA, 2006.
McDonald R . Factor analysis and related methods. Lawrence Erlbaum Associates: Mahwah, NJ, 1985.
Browne M, Cudeck R . Alternative ways of assessing model fit. In: Bollen K, Long S (eds). Testing Structural Equation Models. Sage: Beverly Hills, CA, 1993, pp 136–162.
Browne MW . An overview of analytic rotation in exploratory factor analysis. Multivariate Behav Res 2001; 36: 111–150.
Krause JS, Reed KS . Obtaining employment after spinal cord injury: relationship with pre- and post-injury education. Rehabil Counsel Bull 2009; 53: 27–33.
Hess DW, Ripley DL, McKinley WO, Tewksbury M . Predictors for return to work after spinal cord injury: a 3-year multicenter analysis. Arch Phys Med Rehab 2000; 81: 359–363.
Pflaum C, McCollister G, Strauss DJ, Shavelle RM, DeVivo MJ . Worklife after traumatic spinal cord injury. J Spinal Cord Med 2006; 29: 377–386.
Tomassen PC, Post MW, van Asbeck FW . Return to work after spinal cord injury. Spinal Cord 2000; 38: 51–55.
Acknowledgements
The contents of this publication were developed under grants from the Department of Education, NIDRR Grant number H133G060126.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The contents of this paper do not necessarily represent the policy of the Department of Education, and you should not assume endorsement by the Federal Government. The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Krause, J., Reed, K. Barriers and facilitators to employment after spinal cord injury: underlying dimensions and their relationship to labor force participation. Spinal Cord 49, 285–291 (2011). https://doi.org/10.1038/sc.2010.110
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.110
Keywords
This article is cited by
-
The association between secondary health conditions and indirect costs after spinal cord injury
Spinal Cord (2021)
-
Labor market participation of individuals with spinal cord injury living in Switzerland: determinants of between-person differences and counterfactual evaluation of their instrumental value for policy
Spinal Cord (2021)
-
Gender, class, employment status and social mobility following spinal cord injury in Denmark, the Netherlands, Norway and Switzerland
Spinal Cord (2020)
-
Employment, health outcomes, and life satisfaction after spinal cord injury: comparison of veterans and nonveterans
Spinal Cord (2020)
-
Factors associated with labor market participation of persons with traumatic SCI in Switzerland: analyzing the predictive power of social background, health, functional independence, and the environment
Spinal Cord (2020)
