
Abstract
Study Design:
Retrospective cohort design.
Objectives:
To compare socio-demographic, impairment characteristics and utilization (physician and emergency department (ED) visits) for non-traumatic (NTSCI) and traumatic (TSCI) spinal cord injury 1 year post inpatient rehabilitation.
Setting:
Ontario, Canada.
Methods:
Inpatient stays (2003–2006) were identified from the National Rehabilitation Registry System. Exclusions were: in-hospital mortality; discharge after 31 March 2006; death within 1 year after discharge. Multivariate logistic regression analyses were used to determine factors predicting high utilization.
Results:
NTSCI cases (n=1002) were greater than TSCI (n=560). NTSCIs were older (mean=61.6, s.d.=15.8) with more co-morbidities, paraplegic (39.5%) and female (P<0.001). NTSCI had higher FIM admission and discharge scores but lower change scores. Mean number of physician visits for NTSCI and TSCI were 31.2 (median=24) and 29.7 (median=22), with no significant differences in mean specialist visits (NTSCI 16.5: TSCI 17.0). Factors predicting 30 or more physician visits included age 60 years or above (OR=1.5; 95% CI=1.2–1.9), urban living (OR=1.59; 95% CI=1.12–2.22) and lowest quartile (18–88) discharge FIM (OR=1.8; 95% CI=1.4–2.3). Charlson score of 3 or more (OR=2.1; 95% CI=1.3–3.2), urban living (OR=1.92; 95% CI=1.3–2.86) and lowest quartile discharge FIM (OR=1.5; 95% CI=1.2–2.0) were associated with 20 or more specialist visits. Factors for high ED use were: rurality (OR=1.5; 95% CI=1.1–2.1), low income (OR=1.4; 95% CI=1.1–1.9) and low (18–88) discharge FIM (OR=1.7; 95% CI=1.3–2.2).
Conclusion:
Both demonstrated significant health care utilization requiring attention to health care needs; particularly for those living in rural settings, with low income and/or low functional ability.
Similar content being viewed by others


Introduction
Spinal cord injury (SCI) often results in significant changes in long-term functional status and quality of life.1, 2 To date, the majority of literature on SCI characterizing the incidence, impairments, demographics and health care utilization has largely focused on people with traumatic SCI (TSCI), with minimal research related to non-traumatic spinal cord injury (NTSCI) population.3, 4
NTSCIs are caused by a variety of medical conditions including but not limited to: vertebral spondylosis, tumor compression, vascular ischemia, neuronal motor disease, infectious abscess and transverse myelitis.5 Ones et al.,6 suggest that NTSCI accounts for approximately one-third of all SCI cases admitted to inpatient rehabilitation; however, with the rising incidence of cancer-related SCI and aging population, others suggest that NTSCI represents at least 50% of all inpatient rehabilitation SCI cases.4
The demographics of the NTSCI population have been previously reported to differ from TSCI: they are generally older, retired, paraplegic and have more co-morbidities.6, 7 Further, the prevalence of NTSCI is relatively similar among men and women.6, 7 Respiratory disease, urinary tract infections, heart disease and skin infections are purported to be more prevalent in the TSCI population compared with NTSCI;3, 7 however, Ones et al.6 suggest that the frequency and type of complications after SCI are similar among these two subgroups in the rehabilitation setting.
High rates of health care service utilization have been observed within the TSCI population8 and are likely related to preventable secondary complications.8 Munce et al.9 found that individuals with TSCI had an average of 31.7 physician visits in the first year following the injury; further, individuals with TSCI are 2.7 times more likely to have physician visits.8 Given that the NTSCI population tends to be older and have more co-morbidities at the time of diagnoses,6, 7 outpatient health care utilization for this potentially vulnerable subpopulation of SCI needs examination.
There is a paucity of literature related to NTSCI prevalence in the rehabilitation setting on a population-based level. Further, there is a lack of research on outpatient utilization of primary health care services. We speculated that this NTSCI population warrants further examination, as they likely represent a larger portion of the SCI population than previously described due to rising cancer rates and an aging population.10 The objectives of this study were: (1) to compare the prevalence and impairment characteristics of NTSCI and TSCI patients admitted to inpatient rehabilitation; (2) to determine and compare the outpatient health care utilization patterns (that is, family physician (FP), specialist and emergency department (ED) visits) of patients with NTSCI and NTSCI during the first year after their index inpatient rehabilitation admission; and (3) to determine factors that are associated with outpatient health care utilization in both NTSCI and TSCI populations.
Methods
Setting
Ontario is located in central Canada and is the most populous province with over 12 million residents, representing 40% of the Canadian population. Ontario has a universal publicly funded health care system.
Design
This study used a retrospective cohort design with administrative data housed at the Institute for Clinical Evaluative Sciences (ICES). Prevalence, sociodemographics and impairment characteristics of Ontarians with TSCI and NTSCI were examined and compared for the fiscal years April 2003 to June 2005 (1 April 2003 to 31 March 2006). Outpatient health care service utilizations (FP, specialist and ED visits) of NTSCI and TSCI patients were identified and compared during the first year after discharge from inpatient rehabilitation.
Privacy/ethics
This study was approved by the Research Ethics Board at ICES and Sunnybrook Health Sciences Centre in Toronto. The ICES Confidentiality Committee maintains compliance with current Ontario Health Information legislation and data protection practices.
Data sources
National Rehabilitation Reporting System
The collection of data in the National rehabilitation reporting system was mandated for adult clients (18 years and over) receiving care in designated rehabilitation beds. The main data elements for individuals with SCI are patient demographics, admission and discharge dates, level of injury and the Functional Independence Measure (FIM) outcome measure. FIM is a global assessment measure that was developed for use as part of the Uniform Data System for Medical Rehabilitation (UDSMRSM) in the United States.11
Ontario Health Insurance Plan
The Ontario health insurance plan database contains all physicians' fee-for-service claims.12 The main data elements included in a claim are patient and physician unique identifying number, date of the service/claim, fee code for service provided and fee paid.
The National Ambulatory Care Resource System
This database provides information on all visits to emergency departments in Ontario and was mandated for use in 2001. The main data elements are reasons for the ED visit and patient demographics.
Study population
The initial population comprised of men and women admitted to inpatient rehabilitation in the province of Ontario with an initial (index) diagnosis of NTSCI or TSCI between the fiscal years of April 2003 to June 2005. Diagnoses were based on the Rehabilitation Client Groups11 04.1–04.3 (see Appendix A). Individuals were included if they had a valid identifier, were greater than or equal to 18 years of age and did not have an admission for rehabilitation in the year before the index admission (this was to capture the incident rehabilitation stay related to the SCI and minimize prevalent cases). The following exclusion criteria were then applied (in order): (1) in-hospital mortality; (2) index discharge after 31 March 2006; and, (3) died within 1 year after discharge (a minimum of 1 year was needed for follow-up).
Measures
Level of injury
Injury level was categorized as paraplegia, tetraplegia or other/unspecified.
Length of stay in inpatient rehabilitation
This is a measure of number of days that an SCI case stayed in the inpatient rehabilitation (admission to discharge) during the index admission to rehabilitation.
Functional independence measure
The FIM ranges from 18 (total dependence) to 126 (total independence) and captures information on 18 items in six domains: self-care, sphincter control, mobility, locomotion, communication and cognition.12
Charlson co-morbidity index (deyo-adaptation)
The Charlson Index is a weighted measure (ranges from 0 to 31) of relative effects of a combination of 16 diseases/risk factors and has been adapted for use with administrative data International Classification of Diseases (ICD-10) codes.14 Most patients have a score of zero. The Charlson Index is widely used in all aspects of outcome research and has been translated to an administrative data format.14
Rurality
The Rurality Index of Ontario is made up of 10 components which are related to population factors and distance. The Rurality Index of Ontario is a scaled index that ranges between 0 and 100 and is calculated for all census subdivisions within Ontario. Communities with higher values are relatively more rural compared with communities with lower values and values equal to or above the cut-point of 45 are considered ‘rural’.15
Socioeconomic status (SES)
As individual household income level is not available in these administrative databases, income levels are based on Canadian 2001 Census data. Similar to other published studies,16 SES was assessed based on the median income of the enumeration area associated with the individual's residential dissemination area, which is the smallest geographical standard unit (usually 400–700 people) used in Canadian Census data. The Ontario population was divided into income quintiles with 1 being the lowest and 5 being the highest, which are proxy measures for individual SES.
Analysis
Parametric and non-parametric statistics were used to describe and compare the clinical characteristics and health care utilization of patients with NTSCI and TSCI. Multivariate logistic regressions were conducted to examine factors associated with high utilization defined as 30 or more physician visits, 20 or more specialist visits and two or more visits to the ED. These cut-points for high health care utilization were based on the highest quartiles. The cut-point for age (that is, 60+ years) was determined based on median values. Variable selection in the regression were based on conceptual clinical knowledge rather than stepwise selection, as the latter methodology has been shown to have deficiencies such as decreased predictive information and decreased model stability.17 All statistical tests were performed at the 5% level of significance and were two-sided.
Results
Demographics and clinical characteristics
The number of NTSCI and TSCI cases admitted for rehabilitation that met our inclusion criteria over the 3-year study period was 1623 and 842 cases, respectively. The exclusion criteria eliminated 16 for discharged dead, 124 for discharged after March 2006 and 156 who died within 1 year after index discharge. These criteria yielded 1002 NTSCI and 560 TSCI cases.
Individuals admitted to inpatient rehabilitation for NTSCI were more likely to be older (mean=61.6, s.d.=15.8), paraplegic (39.5%, n=396) and have more co-morbidities compared with TSCI cases (P<0.001; Table 1). There was an approximately even sex distribution in the NTSCI group (52.2% were male patients, n=523) whereas 75% (n=422) of the sample was male in the TSCI group. Differences between the two groups were also observed for FIM scores, as individuals with NTSCI had significantly higher FIM scores on admission (median=83; IQR 68–97) and discharge (median=111; IQR 96–118); however, the change in FIM scores was less for NTSCI (median=20; IQR 9–31) compared with TSCI (median=22; IQR 7–40; Table 2). With respect to the Charlson Index, the most prevalent conditions for NTSCI were diabetes (n=58, 5.8%), cancer (n=53, 5.3%) and COPD (n=21, 2.1%). Diabetes (n=8; 1.4%) and chronic obstructive pulmonary disease/other respiratory disease (n=8, 1.4%) and acute myocardial infarction (n=7, 1.3%) were the most common conditions within the Charlson Index for TSCI.
Health care utilization
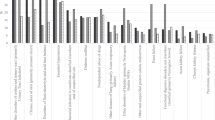
Both TSCI and NTSCI had high primary care utilization during the year after inpatient rehabilitation (Table 2). The mean number of physician visits for NTSCI and TSCI cases was 31.2 (median=24) and 29.7 (median=22), respectively. There were no significant differences identified between the mean number of specialist visits for NTSCI (16.5) and TSCI (17.0); however there were differences in the type of specialty seen. NTSCI patients had more mean visits to neurosurgeons (1.0), internists (2.6) and FPs (14.7) whereas individuals with TSCI had significantly more mean visits to physiatrists (4.1). The mean number of ED visits was similar for both NTSCI (1.2) and TSCI (1.3).
Type of injury was not a significant predictor of health care utilization after controlling for other clinical and socio-demographic factors in multivariate modeling (Table 3). Older age (⩾60 years), living in an urban setting (OR=1.6) and having the lowest quartile FIM (18–88) score upon discharge (OR=1.8) were significantly associated with having 30 or more physician visits within the first year after inpatient rehabilitation. Paraplegia level of injury (OR=1.5), higher co-morbidity (OR=2.1), living in an urban setting (OR=1.9) and the lowest quartile FIM (18–88) score upon discharge (OR=1.5) were significantly associated with having 20 or more specialist visits. Using multivariate analyses, results showed that living in a rural environment (OR=1.5), having a lower income (OR=1.4) as well as a lower discharge FIM score (OR=1.7) were significantly associated with two or more ED visits (Table 4).
Discussion
The present study demonstrates that individuals with NTSCI represent a significant proportion (64%) of SCI cases in the inpatient rehabilitation setting. Consistent with other studies,7, 18, 19 NTSCI patients had significantly fewer days spent in inpatient rehabilitation compared to TSCI and had higher FIM scores upon discharge. Both NTSCI and TSCI had high outpatient health care utilization patterns; however, there were differences in the types of health care used. TSCI patients had higher mean visits to physiatrists and urologists, whereas NTSCI patients had higher mean visits to internists and FPs. Despite these differences, type of injury was not a significant predictor in utilization when adjusting for other clinical factors such as age, co-morbidity, rurality, income and discharge FIM scores. Rather, results showed that individuals with SCI who may be more marginalized because they have lower levels of income, lower levels of functioning and live in rural areas, are more likely to have higher ED visits.
Socio-demographic and clinical characteristics
The clinical characteristics of the NTSCI and TSCI cases are similar to previous studies.6, 7, 18, 19 In particular, our NTSCI sample had a mean age of 61.6 years with 52.2% of the sample being male patients. Other studies have reported mean ages for NTSCI ranging from 31 to 61 years with a relatively even sex distribution.3, 18, 19 The majority of the NTSCI sample had paraplegia compared with the TSCI group which is also consistent with previous work.6, 7 It is noteworthy that 42% of the NTSCI sample did not have a level of injury specified whereas only 14.3% were non-specified for TSCI. This discrepancy might suggest that the coding process in the inpatient rehabilitation setting needs to be reviewed with particular attention to NTSCI and the adoption of the international NTSCI etiology nomenclature using ICD-10 codes.
Health care utilization
Our study has identified high outpatient health care utilization patterns, approximately three times higher than mean number of visits in the general population within the same age strata20 for both groups. These visits may be related to secondary complications.8 Importantly, rather than type of injury, specific socio-demographic and impairment variables such as age, income, discharge FIM score and rurality, were found to be significant predictors of health care utilization. Individuals living in a rural area were less likely to have high overall physician and specialist visits, but were more likely to be admitted to the ED.
Several barriers have been previously proposed to influence health care utilization with this population.21 Specifically pertinent to a rural setting, there may be issues with access to and availability of community health care services.22, 23 Physical access, such as transportation to physician clinics and accessibility into offices, as well as limited availability of specialist care may be influencing increased ED use.
We also identified that low income and low discharge FIM scores were significantly associated with the likelihood of high ED visits. Individuals with lower income and/or lower functional ability may have less informal networks of care resulting in an increased vulnerability with negotiating the health care system. Further, patients with lower SES have been shown to be perceived as less attractive by physicians which may influence the inequities observed in medical management.24
Our findings suggest that the discharge FIM score can be informative with respect to community health care utilization. These results are similar to those of Gabbe et al.25 which showed the predictive utility of discharge FIM scores with functional abilities at 6 months following inpatient rehabilitation.
Limitations
There are a few limitations to this study. At this time, we are only able to identify NTSCI from the inpatient rehabilitation setting as no ICD-10 codes are available for this group in the acute care database. As a result, we are only able to comment on utilization patterns of individuals who have received inpatient rehabilitation, so there is a segment of NTSCI population, which was not captured. Second, data were not available on services provided outside the province of Ontario or in private settings. Third, due to coding issues, we do not know the specific reasons for high outpatient health care utilization (that is, type of complication). There are likely important differences between the types of secondary health complications between those with NTSCI versus TSCI.
Conclusion
Despite the aforementioned limitations, to our knowledge this is the first study that has examined and compared outpatient health care utilization for individuals with NTSCI and TSCI at a population-based level. Our findings suggest that there may be limited access for more vulnerable individuals with SCI living in rural settings, with low income and/or low functional ability, which may subsequently influence ED use.
Future research is warranted to investigate in more specific detail reasons for high utilization and the nature of the interaction with the health care system to help inform the research, clinical and policy-related communities.
References
Paker N, Soy D, Kesiktaş N, Nur Bardak A, Erbil M, Ersoy S, et al. Reasons for rehospitalization in patients with spinal cord injury: 5 years' experience. Int J Rehabil Res 2006; 29: 71–76.
Hammell KW . Quality of life after spinal cord injury: a meta-synthesis of qualitative findings. Spinal Cord 2007; 45: 124–139.
New PW, Rawicki HB, Bailey MJ . Nontraumatic spinal cord injury: demographic characteristics and complications. Arch Phys Med Rehabil 2002; 83: 996–1001.
Citterio A, Franceschini M, Spizzichino L, Reggio A, Rossi B, Stampacchia G . Nontraumatic spinal cord injury: an Italian survey. Arch Phys Med Rehabil 2004; 85: 1483–1487.
Ho CH, Wuermser LA, Priebe MM, Chiodo AE, Scelza WM, Kirshblum SC . Spinal cord injury medicine. 1. epidemiology and classification. Arch Phys Med Rehabil 2007; 88 (3 Suppl 1): S49–S54.
Ones K, Yilmaz E, Beydogan A, Gultekin O, Caglar N . Comparison of functional results in non-traumatic and traumatic spinal cord lesion. Disabil Rehabil 2007; 29: 1185–1191.
McKinley WO, Jackson AB, Cardenas DD, DeVivo MJ . Long-term medical complications after traumatic spinal cord injury: a regional model system analysis. Arch Phys Med Rehabil 1999; 80: 1402–1410.
Dryden DM, Saunders LD, Rowe BH, May LA, Yiannakoulias N, Svenson LW et al. Utilization of health services following spinal cord injury: a 6-year follow-up study. Spinal Cord 2004; 42: 513–525.
Munce S, Guilcher SJ, Couris CM, Fung K, Craven C, Verrier M et al. Physician utilization among adults with traumatic spinal cord injury in ontario: a population-based study. Spinal Cord 2009; 47: 470–476.
Canadian Cancer Society/National Cancer Institute of Canada. Canadian Cancer Statistics 200, Toronto, Canada, 2008. Available at: www.cancer.ca/statistics and www.ncic.cancer.ca. Accessed October 12, 2008.
The Rehabilitation Client Groups have been adapted from the UDSMRimpairment codes Copyright © 1997 Uniform Data System for Medical Rehabilitation, adivision of UB Foundation Activities, Inc., all rights reserved. Used with permission.
Granger CV, Hamilton BB, Linacre JM, Heinemann AW, Wright BD . Performance profiles of the functional independence measure. Am J Phys Med Rehabil 1993; 72: 84–89.
OHIP. Schedule of Benefits. Bulletin on BMD. Ontario MHLTC: Toronto, Canada, 1999.
Hall SF, Groome PA, Streiner DL, Rochon PA . Interrater reliability of measurements of comorbid illness should be reported. J Clin Epidemiol 2006; 59: 926–933.
Kralj B . Measuring ‘rurality’ for purposes of health-care planning: an empirical measure for Ontario. Ont Med Rev 2000; 67: 37–40.
Alter DA, Naylor CD, Austin PC, Tu JV . Long-term MI outcomes at hospitals with or without on-site revascularization. JAMA 2001; 285: 2101–2108.
Steyerberg EW, Eijkemans MJ, Harrell FE, Habbema JD . Prognostic modeling with logistic regression analysis: in search of a sensible strategy in small data sets. Med Decis Making 2001; 21: 45–56.
Gupta A, Taly AB, Srivastava A, Vishal S, Murali T . Traumatic vs non-traumatic spinal cord lesions: comparison of neurological and functional outcome after in-patient rehabilitation. Spinal Cord 2008; 46: 482–487.
McKinley WO, Huang M, Tewksbury MA . Neoplastic vs traumatic spinal cord lesion: an inpatient rehabilitation comparison. Am J Phys Med Rehabil 2000; 79: 138–144.
Chan BTB, Schultz SE . Supply and Utilization of General Practitioner and Family Physician Services in Ontario, ICES Investigative Report Institute for Clinical Evaluative Sciences: Toronto, 2005.
Kroll T, Jones GC, Kehn M, Neri MT . Barriers and strategies affecting the utilization of primary preventive services for people with physical disabilities: a qualitative inquiry. Health Soc Care Community 2006; 14: 284–293.
Cox RJ, Amsters DI, Pershouse KJ . The need for a multidisciplinary outreach service for people with spinal cord injury living in the community. Clin Rehab 2000; 15: 600–606.
LaVela SL, Smith B, Weaver FM, Miskevics SA . Geographical proximity and health care utilization in veterans with SCI&D in the USA. Soc Sci Med 2004; 59: 2387–2399.
O'Reilly D, Steele K, Patterson C, Milsom P, Harte P . Might how you look influence how well you are looked after? A study which demonstrates that GPs perceive socio-economic gradients in attractiveness. J Health Serv Res Policy 2006; 11: 231–234.
Gabbe BJ, Simpson PM, Sutherland AM, Williamson OD, Judson R, Kossman T et al. Functional measures at discharge: are they useful predictors of longer term outcomes for trauma registries? Ann Surg 2008; 247: 854–859.
Acknowledgements
This research was supported by a grant from the Ontario Neurotrauma Foundation (ONF). Dr Jaglal is the Toronto Rehabilitation Institute (TRI) Chair at the University of Toronto in Health Services Research. Ms Guilcher's doctorate is supported by the Women's College Research Institute, ONF, TRI and Ontario Training Collaborative Program in Health Services and Policy Research. We acknowledge the support of TRI which receives funding under the Provincial Rehabilitation Research Program from the Ministry of Health and Long-Term Care in Ontario. The views expressed do not necessarily reflect those of the Ministry. Many thanks are expressed to Xuesong Wang at ICES who conducted statistical programming for this work.
Author information
Authors and Affiliations
Corresponding author
Appendix A
Appendix A
Rights and permissions
About this article
Cite this article
Guilcher, S., Munce, S., Couris, C. et al. Health care utilization in non-traumatic and traumatic spinal cord injury: a population-based study. Spinal Cord 48, 45–50 (2010). https://doi.org/10.1038/sc.2009.78
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2009.78
Keywords
This article is cited by
-
Multimorbidity in persons with non-traumatic spinal cord injury and its impact on healthcare utilization and health outcomes
Spinal Cord (2023)
-
Examining the impact of COVID-19 on health care utilization among persons with chronic spinal cord injury/dysfunction: a population study
Spinal Cord (2023)
-
The effect of rurality and distance from care on health outcomes, environmental barriers, and healthcare utilization patterns in persons with traumatic spinal cord injury
Spinal Cord (2023)
-
Primary Care in the Spinal Cord Injury Population: Things to Consider in the Ongoing Discussion
Current Physical Medicine and Rehabilitation Reports (2023)
-
The relationship between health behaviors and emergency department visits and hospitalizations after traumatic spinal cord injury
Spinal Cord (2022)
