
Abstract
Study design:
Case report.
Objectives:
To present an unusual type of penetrating objects causing Brown–Séquard syndrome (BSS) and its clinical character.
Setting:
Department of Orthopaedic Surgery, Shanghai Changzheng Hospital, Second Military Medical University, Shanghai, PR China.
Methods:
A 54-year-old man fell from a height of 4 m onto an iron fence, and a sharp iron fence point penetrated the right side of his back. He developed left-sided BSS. Both X-ray film and computed tomography scanning of the thoracic spine showed a right vertebral plate of Th5 fracture and metal fragments inclining through the posterior and left lateral of the spinal canal. Emergency decompressive laminectomy and removal of the foreign metal piece were performed. No improvement in neurological function was observed 10 days after surgery, and thus hyperbaric oxygen treatment was initiated twice a day for the next 1 month.
Results:
Forty days after surgery, his bladder function returned to normal. The motor deficit had regressed and he could walk without assistance 70 days after the operation. One year later, his lower extremity functions recovered almost completely, except for slight numbness on the right side.
Conclusion:
As far as we know, on the basis of existing literature, the injury mechanism to BSS by a sharp iron fence point has not been reported so far. The satisfactory recovery after injury may in part be attributed to timely surgery and continuing hyperbaric oxygen treatment.
Similar content being viewed by others


Introduction
Brown–Séquard syndrome (BSS) is characterized by ipsilateral motor paralysis and contralateral loss of pain and temperature sensation. BSS is commonly caused by knifelike objects penetrating the spine. Bizarre penetrating objects such as a drill bit1 and a pen2 have also been reported in the literature. However, it seems to us that this is the first case report involving a sharp iron fence point puncturing the back causing this syndrome.
Case report
The patient was a 54-year-old man who fell from a height of 4 m while he was dealing with a telephone wire. He fell atop an iron fence, as a result of which a sharp iron fence point penetrated the patient's right side of the back and caused a fracture. The broken iron fence point resided in his back. He complained of severe back pain and had neurological deficit in his left leg. Five hours after injury, he was transferred to our hospital. Physical examination revealed a 2-cm long irregular wound in his back (Figure 1). A possible metal object was found in the radiograph of the thoracic spine (Figure 2). Computed tomography revealed a metal-related fracture of the right vertebral plate of Th5 and a metal fragment inserted into the spinal canal, which reached the left vertebral body (Figure 3). Neurological examination showed that his left leg was completely flaccid, whereas his right leg could move normally. There was a loss of pain, temperature sensation and touch sensation on the right side below the Th5 level. There was a decrease in touch sensation, but pain and temperature sensation was intact on the left side below the Th5 level. Sensation in the right sacral area was spared, but he developed urinary retention. A urinary catheter was inserted in the former hospital. Cremasteric reflex was absent on the left side but present on the right side. Deep tendon reflexes were absent on the left leg. A positive Babinski's sign was induced bilaterally. His clinical signs and symptoms can be characterized as BSS.

External sign of injury on the left-sided back contused wound.

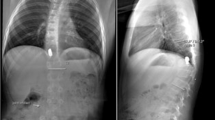
Radiograph revealing the foreign metal piece in the thoracic spine.

Preoperative computed tomography with intraspinal iron fence point and right Th5 vertebral plate fracture.
Prophylactic intravenous ceftazidime was administered in the emergency room until 7 days after operation. He underwent an emergency decompressive laminectomy of Th5, as well as removal of iron fragments. With surgical exposure, it was noted that the right hemilamina of Th5 was fractured and an iron fragment entered into the spinal canal through the lateroposterior aspect of the spinal column (Figure 4), penetrating the dura in the midline and causing contusion of the spinal cord on the left side. The remaining iron fence point was carefully removed, but the dura could not be repaired because of excessive damage to it. A closed negative pressure drainage system was placed for 5 days. A postoperative radiograph did not show any residual foreign body in the spine (Figure 5). No improvement in neurological function was observed 10 days after surgery, and thus hyperbaric oxygen treatment was initiated twice a day for the next 1 month. The urinary catheter was not required and was removed 40 days after the injury. He could walk without assistance 70 days after injury, but had a mild spastic gait. Nine months later, he recovered almost completely and his gait was normal, except for a persistent decreased sensation in his right leg. No improvement in the sensory deficit in his right leg was observed even 1 year after surgery.

Intraoperative views demonstrating the iron fence point within the spinal canal (white arrow).

Postoperative radiographs after removal of the foreign metal fence point.
Discussion
In China, stab wounds of the spinal cord are uncommon. Approximately 50% of stab wound patients with incomplete lesions had BSS.3 BSS secondary to stab wounds involving work-place incidence is rare. In this report, the patient accidentally fell onto an iron fence at work and the sharp fence point penetrated the thoracic spinal cord causing BSS. In this case, the wound was on the right-hand side but the spinal cord hemilateral injury was on the left. The path of the iron fence point may explain this clinical paradox. The fence point perforated the right lamina of Th5, but the fragment entered the lateroposterior aspect of the Th5 spinal canal through the left side.
Early debridement and removal of the foreign body can prevent infection, relieve compression and help to improve neurological function. Spinal stabilization was not compromised from stab injury. In addition, there was a higher risk of wound infections in patients treated with internal fixation as compared with those who were not. We suggest that implant should not be applied in these open spine injuries. Its role is controversial in the context of hyperbaric oxygen treatment for complete spinal cord injury. In contrast, it may be effective in the treatment of incomplete spinal cord injury.4 Our case as reported supported the value of hyperbaric oxygen treatment in patients with BSS.
The patient with BBS had a better prognosis.5 In this report, the patient recovered except for slight numbness in his right side 1 year after surgery.
References
Russell JH, Joseph SJ, Snell BJ, Jithoo R . Brown–Séquard syndrome associated with Horner's syndrome following a penetrating drill bit injury to the cervical spine. J Clin Neurosci 2009; 16: 975–977.
Moin H, Khalili HA . Brown–Séquard syndrome due to cervical pen assault. J Clin Forensic Med 2006; 13: 144–145.
Waters RL, Sie I, Adkins RH, Yakura JS . Motor recovery following spinal cord injury caused by stab wounds: a multicenter study. Paraplegia 1995; 33: 98–101.
Asamoto S, Sugiyama H, Doi H, Iida M, Nagao T, Matsumoto K . Hyperbaric oxygen (HBO) therapy for acute traumatic cervical spinal cord injury. Spinal Cord 2000; 38: 538–540.
Pollard ME, Apple DF . Factors associated with improved neurologic outcomes in patients with incomplete tetraplegia. Spine 2003; 28: 33–39.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Ye, T., Jia, L., Chen, A. et al. Brown–Séquard syndrome due to penetrating injury by an iron fence point. Spinal Cord 48, 582–584 (2010). https://doi.org/10.1038/sc.2009.174
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2009.174
Keywords
This article is cited by
-
Management of non-missile penetrating spinal injury
Neurosurgical Review (2019)
-
Brown-Séquard syndrome in a 11-year-old girl due to penetrating glass injury to the thoracic spine
European Journal of Orthopaedic Surgery & Traumatology (2013)
