
Abstract
Purpose:
Wheelchair sports have become popular in Germany. This is important because of the difficulty experienced by wheelchair-dependent people in maintaining cardiovascular health and fitness by daily activities. Increasing energy expenditure (EE; kcal h−1) is one of the most effective ways of decreasing risk of cardiovascular disease. The purpose of this study was to evaluate the EE of individuals with spinal cord injury in ball games for wheelchair-dependent persons.
Methods:
Fourteen tennis players (WT), 10 basketball players (WB) and 12 rugby players (WR) completed a basal metabolism evaluation and a training test to measure respiratory parameters.
Results:
In the basal metabolism test EE in WT was 66.8±12.8 kcal h−1, in WB 62.7±15.0 kcal h−1 and in WR 63.5±12.9 kcal h−1. During training EE in WT was 325.8±73.0 kcal h−1, in WB 374.8±127.1 kcal h−1 and in WR 248.5±69.4 kcal h−1. The average EE of the whole group was: 316.4±89.6 kcal h−1 with a corresponding heart rate of 118.5±23.1 b.p.m. and a lactate concentration of 2.09±0.7 mmol l−1. Statistical analysis showed significantly lower values of EE, heart rate and oxygen uptake for the WR group in comparison to the other groups.
Conclusion:
The results indicate that the additional leisure time EE of persons participating in WB and WT is sufficient to maintain fitness. This level of EE is comparable to the recommendations of the ACSM for able-bodied persons, and therefore might be sufficient to prevent the development of cardiovascular diseases.
Similar content being viewed by others


Introduction
Sport for wheelchair-dependent persons has traditionally focused on therapy and rehabilitation purposes.1 It continues to play an important and beneficial role in the rehabilitation of patients after a spinal cord injury. However, wheelchair sport is now an organized leisure time activity as well as a competitive sport and has gained popularity especially in ball games such as wheelchair basketball, wheelchair tennis or wheelchair rugby.
In view of the increased life expectancy and the elevated risk of atherogenic diseases for people who are wheelchair dependent, research to identify effective measures to prevent disease is of central importance.2 Recommendations for preventive medical measures are mainly based on extensive longitudinal investigations focusing on the relation of additional energy expenditure due to physical activity on the one hand and mortality and morbidity rates on the other hand.3, 4, 5 Most of the studies measure total energy expenditure, or energy expenditure exceeding resting energy expenditure. From these findings recommendations have been derived for the intensity and amount of sport and physical exercise needed to minimize the risk of developing cardiovascular disease. According to the Harvard alumni study, a weekly energy expenditure of 2000–2500 kcal or a daily energy consumption of approximately 300–350 kcal, respectively, leads to the most effective decrease in the probability of suffering myocardial infarction.5 To follow these recommendations in everyday life, it is necessary to quantify the energy expenditure involved in different types of physical activity. These indications exist for able-bodied people for almost every conceivable physical activity.6 Unfortunately such recommendations are not available for people dependent on a wheelchair, especially for those participating in wheelchair sports. Recommendations are needed because people dependent on a wheelchair are more likely to have a low-exercise lifestyle and lower muscle mass in comparison with able-bodied people. This lower energy expenditure leads to an increased risk of developing cardiovascular diseases.7 This lack of information concerning experimental quantifications of energy expenditure in persons with a spinal cord injury consequently eliminates the possibility of conducting systematic, prospective longitudinal studies on the relationship between energy expenditure and cardiovascular mortality and morbidity. Examinations of the energy expenditure associated with various wheelchair sports are, thus, an essential prerequisite for investigating the benefit for cardiovascular disease risk. In addition, the resting energy expenditure could be helpful to create diet recommendations for persons with a spinal cord injury participating in the given sport forms. As the total energy expenditure during sport is mainly generated by active muscle mass the question comes up that whether a reduced muscle mass depending on different lesion levels correlates with a reduced energy expenditure. The aim of this study was to examine the energy expenditure of wheelchair-dependent individuals in the sports of tennis, quad rugby and basketball. In combination with our previous findings in hand biking and wheelchair racing this is one of the preconditions to examine the effects of additional energy expenditure in wheelchair-dependent persons.2
The aim of the study was to determine the load-induced energy expenditure in three wheelchair ball game sports. Furthermore, we wanted to determine the extent of training required in the field of these wheelchair sports to attain the energy expenditure values recommended from a sports medical point of view, and the weekly energy expenditure of the study group as a result of their physical activity.
Method
Instruments
The resting oxygen uptake and carbon dioxide production was measured using the Cosmed K4b2 portable spirometric system (Cosmed, Rome, Italy). The system measures breath-by-breath ventilation (V̇E), fraction of expired oxygen (FEO2) and carbon dioxide (FECO2). Subjects breathe through a rubber face mask (Hans Rudolph Inc., Kansas City, MO, USA), which directs air into the ventilation turbine and into the portable unit housing the O2 and CO2 gas analyser. Those lightweight systems (total mass ∼1.5 kg) are attached via harness to the subject's body in such a manner that their movements are not hampered during the measurement periods. Expired gas concentrations were measured with a polarographic electrode for the O2 fraction and with an infrared electrode for the CO2 fraction. These gas analysers were thermostated and compensated for barometric pressure and environmental humidity variations. The Cosmed K4 system was calibrated before each test according to the manufacturer's recommended procedures (operator's manual of K4 system). Measurements were made at approximately 0700 hours for not less than 30 min in a supine position after an overnight fasting period. The system estimates the energy expenditure by measuring breath-by-breath oxygen uptake (ml O2 min−1) and converts this to kilocalories per minute (or kcal kg min−1) using the Haldane correction for inspired minimum ventilation and standard equations.8 Kilocalories instead of the SI (Système international d'unités) value joule were used to ease the comparison of results with published data. The conversion factor is 4.1868. The K4b2 has been accepted to accurately measure V̇O2 and estimate energy expenditure over a wide range of metabolic rates in adults.9
Energy expenditure during load was measured with the same open-circuit system during training sessions in the gym (basketball and rugby), on an outdoor clay court as well as on an indoor hard court (tennis). Measurements were made during a typical training session focusing on the player skills development and on game situations. It was possible to measure one athlete per training session using the portable spirometric system. According to this, we performed tests in 10 different training sessions on wheelchair tennis, 12 on wheelchair rugby and 10 on wheelchair basketball. Training time was standardized beginning at 1900 hours for approximately one hour without fasting periods or special diet. To compare the metabolic training intensities of the athletes, blood samples to estimate lactate concentrations were taken four times each training hour. Heart rate was continuously measured using X-Trainer heart rate monitors (Polar, Oy, Finland). Borg Scale was used to rate subjective exertion.10
Participants
Thiry-six male athletes with spinal cord injuries (tennis: 14 athletes with paraplegical spinal cord injury, rugby: 12 athletes with quadriplegically spinal cord injury and basketball: 10 athletes with paraplegical spinal cord injury) took part in the investigation. Participants were fully informed of the procedures and possible risks associated with the investigations and were allowed to withdraw from the study at any time. Each volunteer provided written consent before taking part, and all investigations were approved by the German Sports University ethical advisory committee. Lesion levels were between cervical areas (C5) to lumbar areas (L3). All athletes played in the first and second national German league of their specific sport. Anthropometric data are given in Table 1.
For 34 athletes, a traumatic spinal cord injury had caused their disability. Two individuals had spinal cord injury due to inflammatory injuries. Time of wheelchair dependence and sport activity as well as training time are listed in Table 2. We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Statistics
Analyses were performed using STATISTICA for Windows Version 5.1. F (StatSoft Inc, Tulsa, OK, USA). The effects between the groups were determined by a one-way analysis of variance. Post hoc (least significant difference Test LSD) analysis was performed to test whether the interactions were significant. Correlations between the energy expenditure and the lesion levels were made using Spearman rank correlation coefficient. A P-value less than 0.05 was considered significant.
Results
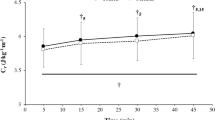
In the basal metabolism test the energy expenditure at rest in tennis players was 66. 8±12.8 kcal h−1, in rugby players 63.5±12.9 kcal h−1 and in basketball 62.7±15.0 kcal h−1. The respiratory exchange ratio at rest for the different sport forms differed between 0.86±0.060 (tennis), 0.88±0.061 (rugby) and 0.84±0.095 (basketball). The values of the respiratory exchange ratio and the calculated percentage of fatty acid combustion at rest without taking into account the protein metabolism are shown in Figure 1. For the training test the values of energy expenditure and lactate are shown in Figures 2 and 3. The calculated sport-specific training durations per day to fulfil the recommendations of energy expenditure given by Paffenbarger et al.11 are given in Table 3. The calculated weekly energy expenditure of the athletes is given in Table 4.

Respiratory exchange ratio and the calculated percentage of fatty acid combustion at rest.

Energy expenditure during training.

Lactate concentrations during training.
The mean value of energy expenditure of all wheelchair-dependent athletes was 313.6±101.14 kcal h−1. The values of the rugby players showed significantly lower values of energy expenditure in comparison to the values of the tennis and basketball athletes. There was a significant but poor relationship between the lesion level and the energy expenditure (r=0.49). The lactate values showed no significant differences between the groups. The subjective exertion rating during the lower intensities was 12–13 on the Borg Scale,10 which corresponds to an assessment of ‘moderately hard’.
Discussion
Energy expenditure at rest
Participant's values in the three different ball games did not show any difference in energy expenditure at rest. This was unexpected as the group of rugby players included people with tetraplegical disabilities who have reduced muscle mass in comparison to those with paraplegical lesions. At rest about 26% of required energy expenditure is due to muscle activities.12 Thus, a reduction in muscle mass could have evoked a reduced oxygen demand and with this a reduced energy expenditure at rest. In our subgroup we did not find this pattern of results. One reason for this could be the high level of fitness of the elite rugby players leading to a muscle mass comparable to those of subjects in the other subgroups. However, the energy expenditure calculated according to the equation recommended by the WHO, taking the anthropometric data of the athletes such as age, weight and sex into account, amounted to 73.9 kcal h−1.13 The discrepancy between measured and calculated energy expenditure during rest can, nevertheless, be explained by the lower total muscle mass of the individual athletes and is attributed to the atrophy of the muscles of the paralysed lower extremities. It should be added here that the WHO calculations refer to people without any chronic disease or disability.13 There is a lack of information concerning the energy expenditure at rest of people with spinal cord diseases or injuries. Due to methodological differences, findings by Huang et al.14 are only partially comparable to the results of this study. The expenditure values at rest were measured in a sitting position, whereas in our study the measurements were performed in a supine position. In 48 paraplegic subjects, Mollinger et al.15 found expenditure values at rest of 62.6 kcal h−1 for persons with a high lesion level paraplegical spinal cord injury and of 65.4 kcal h−1 in low level paralysed persons with a paraplegical lesion level. In this study, the measured values also fell considerably below the energy expenditure calculated by standard equations.
Energy expenditure during exercise
Additional physical activity provides a protective mechanism against cardiovascular disease. This has been shown in several longitudinal studies focusing on the relation of additional energy consumption due to physical activity and mortality and morbidity rates.3 In recent studies, Wei et al.16 highlighted the importance of cardiovascular fitness, which results from an appropriate level of physical activity. Additional energy consumption due to physical activity can be estimated using activity questionnaires, heart rate as a predicator of physical stain or the use of accelerometers.17, 18 An accurate evaluation of physical activity is the quantification of the energy expenditure during various activities. Such studies have been performed, with able-bodied people for almost any physical load and results have been recorded. For example, Ainsworth et al.6, calculated the value of energy expenditure in metabolic units (METs). In the field of sports, for the disabled and in particular people who are wheelchair dependent, however, this specific information is unavailable. For example, Ainsworth et al.6 present three categories of energy expenditure during sexual activity, but only one for wheelchair sport.
The low intensity load during the training sessions was subjectively experienced by the participants as moderate (RPE∼12).10 This was intended, as we wanted to simulate an aerobic training of basic endurance, which is usually recommended from the point of view of preventive medicine.19, 20 Reaching this aim could be confirmed by the examination of the lactate concentrations, which resulted in a mean value of 2.09±0.7 mmol l−1. As predicted, the energy expenditure during load in rugby was significantly lower than in tennis and basketball. This result is mainly caused by the reduced muscle mass of the subgroup and a following lower functional ability with a reduced oxygen demand. These findings are supported by a low but significant correlation between the lesion level and the energy expenditure during load.
Comparative values of the energy expenditure of wheelchair athletes are only available for basketball. Burke et al.21 demonstrated an energy expenditure of 6.5 METs, or 516 kcal h−1. This value is also quoted by Ainsworth et al.6 These authors furthermore stated the energy expenditure of pushing a wheelchair to be 8 METs, however, without mentioning any respective source. The values of energy expenditure for basketball reported by Burke et al.21 are 1.5 METs or approximately 141.2 kcal h−1 higher than the mean values of the basketball players in our study. The differing results reflect the differences in intensities of exercise and methodological settings in each study. In contrast to our study Burke and co-workers tested the energy expenditure during competition and used a Douglas bag. Recommendations for maintaining cardiorespiratory and muscular fitness like those published by the American College of Sports Medicine19 can be implemented in the examined wheelchair sports. This would require a training frequency of 3–5 units with a duration of 20–60 min each at a moderate intensity. According to the examinations of Paffenbarger et al.11 a considerably higher additional weekly energy expenditure of 2000–2500 kcal or an additional daily energy expenditure of approximately 300–350 kcal leads to the greatest possible reduction of the risk of myocardial infarction. Transferred to the wheelchair athletes, they would have to exercise between 48 and 84 min per training session to achieve the target values.
It is important to consider that the obtained values refer to a moderate level of training. It could be hypothesized that competition-specific training units would lead to considerably higher energy expenditures. This in turn could demand a reduction of the training units, to obtain the described energy expenditures. If the actual training of the athletes is taken into account, total weekly sport-relevant energy expenditure reaches values between 1489 kcal (rugby), 1913 kcal (basketball) and 2199 kcal (tennis). According to this rather hypothetic extrapolation only the group of the tennis athletes reached the recommendation of Paffenbarger et al.11 although the basketball players missed the target only marginally. Nevertheless, there are some studies showing that an additional energy expenditure of only 1000 kcal w−1 could reduce the risk of developing cardiovascular disease.22 This finding could be of particular interest for disabled people who do not play sport.
The athletes achieved encouragingly high weekly energy expenditures. In this context, however, it should be pointed out that these energy expenditures cannot be considered representative of people dependent on a wheelchair for transportation and sports, as the majority of the examined athletes are highly ambitious competition athletes. It must be stressed, that the preparation time for a training session of wheelchair bound athletes is longer than that of able-bodied persons. This might be an additional barrier for being active and reaching prevention goals. Based on the energy expenditure data gathered in various wheelchair sports it would be possible and desirable to gather data from larger subject groups, using questionnaires on physical activity to measure energy expenditure. Prospective studies of the relationship between physical activity in disabled people and their morbidity and mortality are needed.
Conflict of interest
The authors state no conflict of interest.
References
Guttmann L . Sport and the spinal cord sufferer. Nurs Mirror Midwives J 1975; 141: 64–65.
Abel T, Kroner M, Rojas Vega S, Peters C, Klose C, Platen P . Energy expenditure in wheelchair racing and handbiking—a basis for prevention of cardiovascular diseases in those with disabilities. Eur J Cardiovascul Prevent Rehabil 2003; 10: 371–376.
Blair SN, Brodney S . Effects of physical inactivity and obesity on morbidity and mortality: current evidence and research issues. Med Sci Sports Exerc 1999; 31 (11 Suppl): S646–S662.
Morris JN, Clayton DG, Everitt MG, Semmence AM, Burgess EH . Exercise in leisure time: coronary attack and death rates. Br Heart J 1990; 63: 325–334.
Paffenbarger Jr RS, Hyde RT, Wing AL, Hsieh CC . Physical activity, all-cause mortality, and longevity of college alumni. N Engl J Med 1986; 314: 605–613.
Ainsworth BE, Haskell WL, Leon AS, Jacobs Jr DR, Montoye HJ, Sallis JF et al. Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc 1993; 25: 71–80.
Schlegel A, Koch IPA, Jaschke B . The relevance of training for wheelchair depend persons with a spinal cord injury. Med u Sport 1981; 21: 366–375.
Wassermann K, Hansen JE, Sue DY, Stringer WW, Whipp BJ . Principles of exercise testing and interpretation. Lippincott Williams & Wilkins, 2005.
McLaughlin JE, King GA, Howley ET, Bassett Jr DR, Ainsworth BE . Validation of the COSMED K4 b2 portable metabolic system. Int J Sports Med 2001; 22: 280–284.
Borg G . Perceived exertion as an indicator of somatic stress. Scand J Rehabil Med 1970; 2: 92–98.
Paffenbarger Jr RS, Hyde RT, Wing AL, Lee IM, Jung DL, Kampert JB . The association of changes in physical-activity level and other lifestyle characteristics with mortality among men. N Engl J Med 1993; 328: 538–545.
Schmidt RF, Thews G . Human Physiology. Springer: Berlin, 1997 pp. 556–565.
WHO. Preparation and Use of Food-based Dietary Guidelines—Report of a Joint FAO/WHO Consultation-. Genf: Technical Report Series 1998.
Huang CT, Jackson JR, Moore NB, Fine PR, Kuhlemeier KV, Traugh GH et al. Amputation: energy cost of ambulation. Arch Phys Med Rehabil 1979; 60: 18–24.
Mollinger LA, Spurr GB, El Ghatit AZ, Barboriak JJ, Rooney CB, Davidoff DD et al. Daily energy expenditure and basal metabolic rates of patients with spinal cord injury. Arch Phys Med Rehabil 1985; 66: 420–426.
Wei M, Kampert JB, Barlow CE, Nichaman MZ, Gibbons LW, Paffenbarger Jr RS et al. Relationship between low cardiorespiratory fitness and mortality in normal-weight, overweight, and obese men. JAMA 1999; 282: 1547–1553.
Janssen TW, van Oers CA, Rozendaal EP, Willemsen EM, Hollander AP, van der Woude LH . Changes in physical strain and physical capacity in men with spinal cord injuries. Med Sci Sports Exerc 1996; 28: 551–559.
van der Ploeg HP, Streppel KR, van der Beek AJ, van der Woude LH, Vollenbroek-Hutten M, van Mechelen W . The physical activity scale for individuals with physical disabilities: test-retest reliability and comparison with an accelerometer. J Phys Act Health 2007; 4: 96–100.
American College of Sports Medicine. Position stand. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Med Sci Sports Exerc 1998; 30: 975–991.
Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction–executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2004; 110: 588–636.
Burke EJ, Auchinachie JA, Hayden R, Loftin JM . Energy Cost of Wheelchair Basketball. Physician Sportsmed 1985, 13: 99–105.
Franklin BA, Swain DP SRJ . New insights in the prescription of exercise for coronary patients. J Cardiovasc Nurs 2003; 18: 116–123.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Abel, T., Platen, P., Rojas Vega, S. et al. Energy expenditure in ball games for wheelchair users. Spinal Cord 46, 785–790 (2008). https://doi.org/10.1038/sc.2008.54
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2008.54
Keywords
This article is cited by
-
The effect of the Sport Education Model in physical education on student learning attitude: a systematic review
BMC Public Health (2024)
-
Energy expenditure after spinal cord injury in people with motor-complete tetraplegia or motor-complete paraplegia
Spinal Cord (2018)
-
The effect of autonomic nervous system dysfunction on oxygen consumption during daily living activities in patients with spinal cord injury
Spinal Cord (2017)
-
Effects of variable practice on the motor learning outcomes in manual wheelchair propulsion
Journal of NeuroEngineering and Rehabilitation (2016)
-
Match activity and physiological load in wheelchair tennis players: a pilot study
Spinal Cord (2016)
