
Abstract
There is increasing evidence that the complexity of the retinal vasculature measured as fractal dimension, Df, might offer earlier insights into the progression of coronary artery disease (CAD) before traditional biomarkers can be detected. This association could be partly explained by a common genetic basis; however, the genetic component of Df is poorly understood. We present a genome-wide association study (GWAS) of 38,000 individuals with white British ancestry from the UK Biobank aimed to comprehensively study the genetic component of Df and analyse its relationship with CAD. We replicated 5 Df loci and found 4 additional loci with suggestive significance (P < 1e−05) to contribute to Df variation, which previously were reported in retinal tortuosity and complexity, hypertension, and CAD studies. Significant negative genetic correlation estimates support the inverse relationship between Df and CAD, and between Df and myocardial infarction (MI), one of CAD’s fatal outcomes. Fine-mapping of Df loci revealed Notch signalling regulatory variants supporting a shared mechanism with MI outcomes. We developed a predictive model for MI incident cases, recorded over a 10-year period following clinical and ophthalmic evaluation, combining clinical information, Df, and a CAD polygenic risk score. Internal cross-validation demonstrated a considerable improvement in the area under the curve (AUC) of our predictive model (AUC = 0.770 ± 0.001) when comparing with an established risk model, SCORE, (AUC = 0.741 ± 0.002) and extensions thereof leveraging the PRS (AUC = 0.728 ± 0.001). This evidences that Df provides risk information beyond demographic, lifestyle, and genetic risk factors. Our findings shed new light on the genetic basis of Df, unveiling a common control with MI, and highlighting the benefits of its application in individualised MI risk prediction.
Similar content being viewed by others


Introduction
Coronary artery disease (CAD) remains the leading cause of death and disability worldwide1. Early diagnosis and preventive therapies are essential strategies to control CAD morbidity and the mortality associated with its outcomes, such as myocardial infarction (MI). There is increasing evidence that morphological changes in the retinal vasculature, for instance in vessel width and vascular complexity, might offer insights into CAD before traditional risk factors (such as systolic blood pressure and cholesterol levels)2,3. Recent studies reported that a reduced degree of vascular complexity, quantified through estimates of the fractal dimension (Df), is found in individuals who had a higher CAD risk, independent of their age4. In one of the most extensive studies to date, Zekavat et al. showed associations between Df and incident CAD, amongst several other conditions5. This suggests that Df could be a promising non-invasive and highly accessible biomarker. However, these findings have not translated so far to a substantial increase in prediction accuracy for major adverse cardiac events (MACE) risk when leveraging retinal vascular information in epidemiological models, compared to models based on patient demographics and lifestyle risk factors6,7. Likewise, in a landmark study, Poplin et al. developed a deep learning approach capable of accurately predicting some known MACE risk factors from retinal fundus images that only attained marginal improvements in MACE risk estimation compared to known risk factors alone8. More recently, Diaz-Pinto et al.9 demonstrated another deep-learning-based model capable of predicting two measures of left ventricular mass volume, recognised as MI biomarkers, from fundus images and subsequently showed risk prediction improvement over a demographic-based risk model (including age, sex, SBP, DBP, cholesterol levels, glucose levels, Hba1c, daily alcohol intake and smoking status). However, it remains unknown whether these ‘blackbox’ approaches leverage vascular information or otherwise. Finally, little is known about the degree of overlap between MI risk information provided by Df and established genetic risk factors. Such knowledge would provide invaluable data for untangling genetic and environmental contributors. Beyond retinal vascular structural phenotyping, Theuerle et al. showed the potential of functional testing of retinal microvasculature for the prediction of MACE risk10. However, it remains unclear what improvement functional testing offers over the ubiquity of retinal fundus photography.
Evidence points towards coronary and retinal vessels experiencing similar pathophysiological changes at even early CAD stages11,12,13,14, plausibly influenced by a shared genetic basis13,15,16,17,18,19,20. Population-based studies demonstrated that both tortuosity and width of arteries and veins have a genetic basis16,17. Veluchamy et al. described two novel loci near the COL4A2 and ACTN4 genes associated with retinal tortuosity, previously reported in genetic atrial fibrillation and CAD17 studies. During the preparation of this manuscript, a genome-wide association study (GWAS) was published identifying 7 loci contributing to Df5. Zekavat et al.5 calculated Df from available fundus images of a subset of 54,813 multi-ancestry participants in the UK Biobank cohort. That study, however, did not investigate shared Df and MI molecular regulation and the GWAS is based on a linear model with multiple ancestries that do not account for individuals’ genomic relatedness.
We report here a GWAS of Df, from ~38,000 white-British participants from the UK Biobank. The aim is twofold: to comprehensively study the genetic control of Df and to assess the extent of its relationship with CAD (Fig. 1). We replicated 5 Df loci and found 4 additional loci that are suggestive to contribute to Df variation. Two of these loci (SLC12A9 and RDH5 genes) were previously associated with cardiovascular risk factors and diseases21. Genetic correlation estimates indicate a shared genetic signal between Df and CAD, suggesting that decreasing Df might be influenced by clinical CAD manifestations and, in part, by common genetic effects. Fine-mapping and enrichment analysis on Df loci identified Notch signalling regulatory variants supporting a shared mechanism with MI outcomes. Given this strong connection, we developed a model to predict incident MI cases in the UK Biobank over the 10 years following ophthalmic examination at baseline, including Df and a CAD polygenic risk score (PRSCAD). Internal 10-fold cross-validation shows a considerable performance improvement compared with the SCORE model22, an established CAD risk prediction score based on epidemiological variables. This enhancement can be partly explained by the additional predictive power of retinal and genetic determinants, as these respectively capture early vascular morphological abnormalities and personalised MI risk (Fig. 1). Furthermore, our ablation study demonstrates that our model improves on an extension of SCORE including PRSCAD, evidencing that Df provides risk information beyond epidemiological and genetic risk factors in a population subset of UKBB. Our findings shed new light on the genetic component of Df, suggesting an intricate common genetic basis with CAD aetiology, and demonstrate its potential for individual MI risk prediction.

The authors created this figure with BioRender.com.
Results
Automated quality control and fractal dimension calculation in UK Biobank fundus images reveal interocular asymmetry in vascular complexity at an individual level
For this study, we first developed a semi-automated pipeline to segment the vasculature and select good-quality segmentations in 175,611 fundus images available in the UK Biobank (Fig. 2a) using VAMPIRE software (version 3.1, Universities of Edinburgh, and Dundee)23,24, and a previously published fundus image classifier25. An image quality score (IQS) was computed as part of the classification process (see section “Methods”). Df was subsequently calculated from binary vessel maps produced automatically by VAMPIRE for ~98,600 good-quality images.

a Study design diagram describing the stepwise development of this project. b Left and right Df histogram. c Individual variation distribution between left and right Df. d Overlapping left and right Df histograms including the regression line. e Example of individual interocular asymmetry in UKBB fundus images.
We completed the, to our knowledge, largest within individual interocular Df comparison (n = 39,656 participants) reported so far. The population median (1.492 ± 0.043) and Df distributions appear identical between left and right eyes (Fig. 2b and Supplementary Data 1). However, their moderate correlation (r = 0.61, P-value = 2 × 10−16 Fig. 2d) and the significant difference between left and right Df (paired T-test P-value = 1.59 × 10−75) highlight an individual interocular asymmetry (Fig. 2c), where 50% of the individuals have a right Df 1 SD unit larger than their respective left Df. As shown in Fig. 2d, differences occur in both directions and are more pronounced when any of the Df is lower than the median. To control for this individual asymmetrical effect (Fig. 2e), we performed further analysis in both eyes separately.
We next fitted univariate linear models using Df as the dependent variable and estimated the Pearson correlation between Df and 779 UKBB binary and quantitative traits (see “Methods”) and IQS. Amongst these 780 variables, IQS has the strongest effect (βright = 0.033, P-value < 10−300; βleft = 0.024, P-value < 10−300; r2right = 0.39, P-value < 10−300; r2left = 0.36, P-value < 10−300). Supplementary Figure 1 illustrates this association and that a larger interocular IQS difference moderately affects Df variation (β = 0.014, P-value < 10−300). Therefore, we account for IQS influence in our following analysis.
Besides IQS, 75 quantitative and 161 binary traits were significantly associated with Df after Bonferroni correction26 (P-value < 0.05/780 = 6.41 × 10−5). Age, sex, height, retinal disorders, smoking, hypertension, and CAD have the greatest significant effect on Df in both eyes amongst all measurements (Supplementary Data 2).
Fine-mapping reveals nine fractal dimension loci and their association with cardiovascular risk factors
Here we present a GWAS on Df. This was completed with 38,811 and 38,017 unrelated white-British UK Biobank participants that had a right and left Df measure, respectively. After QC (see “Methods”), there were 9,275,849 imputed SNPs with HWE > 10−6, MAF > 5 × 10−3, a call rate >0.9, and an imputation score >0.9. The GWAS model included hair and skin colour to control for spurious associations given the influence of eye and skin colour on fundus colour27,28. Hair colour replaced eye colour because the latter is not recorded during UKBB assessments. In addition, we completed a supplementary GWAS including an eye colour PRS based on the study by Lona-Durazo et al.29, which indicated no eye colour effect in our GWAS results (see section “Methods”). The quantile-quantile plot of both GWASs indicated an adequate control of the genomic inflation in our analysis (λGC = 1.065 and λGC= 1.067 in the right and left eye, respectively, see Supplementary Figure 2). Fig. 3c illustrates the SNPs effects comparison between eyes GWAS studies, highlighting analogous results. Furthermore, an additional GWAS of mean Df including participants from both left and right eye populations (see “Methods” section) reported equivalent SNP associations to those from eye-specific populations (Supplementary Figure 3). The genetic correlation estimates close to 1 between mean Df and eye-specific GWAS (Mean Df and right Df: 0.93 ± 0.03, P-value = 3.89e−201; mean Df and left Df: 0.89 ± 0.07, P-value = 2.62e−38) revealed that mean Df GWAS was equivalent to those of left and right Df measures.

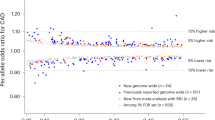
Manhattan plot of a left (top) and b right (bottom) Df. Points are truncated at –log10(P) = 50 for clarity. c Comparison of the genetic variant effects between left and right Df results. Colour depth indicates the significance of each variant (navy, violet, and purple for non-significant, close to genome-wide significance and significant, respectively). Genetic variants included are truncated at a minimum –log10(p) = 3 for clarity.
Fine-mapping analysis of Df GWAS observations indicated that there were nine independent credible SNP sets with a posterior inclusion probability (PIP) > 0.95 (Supplementary Table 1). The credible SNP sets with strongest associations were located at OCA2 (rs72714116, P-value = 7.41 × 10−48) and HERC2 (rs12913832, P-value = 2.16 × 10−96) genes in chromosome 15 (Fig. 3a, b and Supplementary Table 2). We observed another significant association near IRF4 gene (rs12203592, P-value = 6.59 × 10−24). These results are consistent with Zekavat et al. GWAS. Phenome-wide association studies (PheWAS), using GeneATLAS30 and GWASCatalog31, have commonly reported these SNPs in skin, hair, and eye colour analyses. Recent ocular studies demonstrated their implication in lens disorders, cataract, glaucoma, visual acuity, and retinal venular and arteriolar width and tortuosity5,17,20,28,32,33,34,35,36,37,38,39,40.
In addition to these regions, we found 4 credible SNPs that had suggestive significance (P-value < 10−06) which did not reach genomic-wide significance (Table 1). The SNP located at SLC45A2 gene was previously reported in pigmentation analyses29,41, whereas those near EIF2B5 and AGPAT3 genes were described in blood content and inflammation GWASs34,36,42. Those SNPs located at RDH5/ORMLD2 and AGPAT3 genes also have a strong effect on multiple ocular traits and diseases (such as macular thickness and retinal detachment), hypertension, and arterial disorders. The effect of the SNP at SLC45A2 gene is in line with Zekavat et al.5 results. We could not make a complete comparison between studies as the available summary statistics are truncated at a P-value = 10−4. The comparison between reported variants is in Supplementary Table 3.
The SNP heritability (h2SNP) of the left and right Df estimate are, respectively, 0.09 ± 0.015 and 0.10 ± 0.014. These h2SNP magnitude is in line with previous results from retinal vascular tortuosity17,20, retinal width18, and the recently published Df5 GWAS.
We completed additional Df GWAS using independent UKBB participants with European (nleft = 4340 and nright = 4288), Asian (nleft = 562 and nright = 568), and African (nleft = 498 and nright = 509) ancestry to assess if these populations replicated our observations. Only the GWAS including participants with a white European ancestry replicated the strongest associations (P-value < 0.05/9 = 0.0056), which can be explained by the considerably larger number of participants in this analysis when compared with Asian and African ancestries. Little heterogeneity and forest plots of Df loci indicate that multiple significant genetic variants (rs16891982, rs12203592, rs12913832 and rs31381412) have a similar effect across Asian, African, European, and white-British ancestries (Supplementary Fig 4).
We complemented the replication of our GWAS results with an association study in the Canadian Longitudinal Study on Aging (CLSA). This consisted on fitting a linear regression on Df that controlled for the 20 first principal components and a genetic risk score (GRS) for Df, which was estimated using the summary statistics of the GWAS reported above (see “Methods”). We found that the Df GRS had a significant effect on left, right and mean Df phenotypes (Table 2), suggesting thus that the SNPs previously described in the UKBB GWAS contribute to Df variation in the CLSA population.
Genetic correlation estimates and functional analysis indicate shared genetic signal between fractal dimension and coronary artery disease
To assess the link between Df and CAD risk factors and outcomes, we calculated their genome-wide genetic correlation using LD score regression (LDSC)43. Genetic correlation estimates (rg) indicated a negative correlation between Df and hypertension (rg = −0.30, P-value = 4.52 × 10−06), acute MI (rg = −0.16, P-value = 0.03), and CAD (rg = −0.18, P-value = 0.025) (Table 3). All these estimates agree in direction with phenotypic correlations (see Supplementary Data 2) and published studies, which reported that retinal Df decreases as people develop these conditions2,3,11,44. Therefore, our results suggest that these correlations of phenotypes could be partly explained by its shared genetic basis.
Moreover, we estimated the rg between pigmentation traits and Df to examine the similarities in their genetic basis (Supplementary Fig 5). Although the estimates are non-significant (rg = −0.0751, P-value = 0.64), local genetic correlation near to GWAS peaks may be significant.
We investigated possible causal relationships between CAD, hypertension, MI and Df using Mendelian randomisation. We found evidence of horizontal pleiotropy on the loci of interest (pleiotropy analysis P-value = 0.0056), which indicated that we are unable to infer the causality between Df and such cardiovascular events (Supplementary Table 4).
A subset of credible genetic variants points towards associated myocardial infarction post-conditioning signalling pathways
We examined the potential for transcription factor binding site (TFBS) disruption of the lead snps from each credible set from the fine-mapping analysis. We observed 20 TFBS with a strong disruptive effect described in Supplementary Table 5. Eight of these TFBS remained significant after applying a more restrictive threshold to the predicted disruptiveness of its activity between reference and alternative alleles (|AlleleDif| > 1.5). We investigated those associated TF whose binding activity influenced the expression of a gene within 150 kb in the chromosome. This left us with 4 Df SNPs, 5 TFBS and 9 regulated genes. Protein–protein interaction networks show that these TFs and regulated genes participate in Notch and VEGF signalling pathways. Numerous studies indicate that the upregulation of both signalling pathways after an MI event leads to reduced infarct size, improved angiogenesis, and cardiac function, increasing the survival rate and limiting cardiac injury45,46,47.
Fractal dimension improves prediction of incident myocardial infarction in UK Biobank cases
Given our findings, we hypothesized that Df and PRSCAD can provide additional information for MI risk estimation at an individual patient level. We thus developed a model to predict incident cases of MI over the 10 years following ophthalmic examination at baseline (Fig. 4a). Briefly, the model includes PRSCAD derived from a meta-analysis completed by the CARDIoGRAMplusC4D Consortium21, clinical variables from an established CAD risk assessment strategy named SCORE22 (age, sex, smoking status, SBP and BMI), and the Df of both eyes. We also considered model versions excluding either PRSCAD or Df to elucidate their independent effect. As a baseline for comparison, we retrained the original SCORE model22. The MI model was trained with the 526 individuals who experienced an MI event after their UKBB ophthalmic examination. We created a control group with an equal number of individuals with an equivalent age range and had no underlying MI and CAD (Supplementary Table 6). The mean age and SD in the case and control group are respectively 57.31 ± 6.47 and 54.21 ± 7.84 years. We chose the random forest classifier (RFC) as this method allows one to model non-linear associations with the outcome and interactions between the predictor variables, which boosts the prediction while being interpretable48,49. Internal 10-fold cross-validation (FCV) indicates that our models dominate the ROC curve of the SCORE model, achieving a greater precision, recall, and AUC (Fig. 4b and Table 4). Amongst our considered models, the model including PRSCAD (AUC = 0.741 ± 0.001) yielded an AUC significantly different from the one introducing Df (AUC = 0.763 ± 0.001), and the one combining both Df and PRSCAD (AUC = 0.770 ± 0.001) (Table 4 and Supplementary Table 7). Additional assessments in our proposed model indicated that the replacement of Df measures with Df adjusted by IQS, the introduction of one-eye Df measurements in our MI model, or the use of mean Df in our model yielded a comparable performance to the aforementioned ones (Supplementary Table 8).

a Diagram illustrating the development of our MI model. b ROC curve of MI predictive models. c Kaplan–Meier curve of incident MI cases separated by predicted MI probability. * Df fractal dimension, PRSCAD CAD polygenic risk score, BMI body-mass index, SBP systolic blood pressure.
Next, we investigated survival rate differences between low and high MI-risk groups. These groups were defined by the predictions obtained with our top-performing MI model and by subsequently separating these with a probability threshold of 0.5 (high MI-risk>0.5 and low MI-risk = <0.5). The Kaplan-Meier curve (Fig. 4c) illustrates a significant divergence between these groups (Log-rank test P = 3.52 × 10−30), which can be explained by the pronounced decrease in survival during the first 4 years in the high MI risk group.
Finally, we performed an ablation study to understand the origin of the performance improvement in our new model. Briefly, we evaluated the performance of all possible variations between SCORE and the top-performing model (see “Methods” section). This assessment revealed three key contributors to the reported improvement: the use of quantitative variables, the introduction of PRSCAD and Df, and the use of a random forest classifier. An extended discussion can be found in Supplementary Table 9. The added predictive value of Df is supported by the RFC development analysis which reveals that age, BMI and Df are the most important features in its architecture (Supplementary Figure 6). PRSCAD is also a determinant of the model’s development as its RFC importance is equivalent to SBP and smoking taken together, which is in line with recently published results14.
Discussion
This work provides a comprehensive examination of the Df genetic basis, unveiling regulatory mechanisms at the Notch signalling pathway that contribute to an intricate shared genetic basis with MI. Given the strong Df and MI connection, we presented a predictive model for MI based on a random forest algorithm that includes Df and a CAD polygenic risk score (Fig. 1). This novel model improves MI individual risk prediction compared to state-of-the-art approaches, demonstrating the additional predictive power of these complimentary traits to early identify high-risk groups.
We identified an individual interocular Df asymmetry in UKBB that led us to perform most of the analyses in both eyes separately. This finding is in line with published studies that reported lateral asymmetry in Df, tortuosity, and retinal width50. We observed that this asymmetry is more pronounced when one of the two eyes has a Df below the population median. Interestingly, the regression coefficients and the Pearson’s correlation estimates between Df and UKBB traits, and the genetic findings are equivalent in both eyes independently, suggesting that the asymmetrical effect has a negligible influence at a population level. A quantitative assessment of the asymmetry of retinal vascular measurements between eyes seems crucial for studies on retinal vascular biomarkers, often conducted on a single eye, and require further work.
We found that age, sex, smoking, and developing ocular and cardiovascular diseases have a significant effect on Df, agreeing with studies reporting that Df decreases with age or by developing these conditions2,11,15,19. Interestingly, IQS has the strongest effect on this trait. To overcome quality imaging differences, numerous studies elaborate on the importance of assessing quantitatively image quality, especially in large cohorts analysed automatically51. In our case, IQS is computed from the binary vessel map and encapsulates the vessels segmentation’s sharpness and connectivity, which are key features frequently used51,52 to compute vascular branching complexity.
We replicated the effect of 5 loci associated with Df with similar effects across European, Asian, and African UKBB participants. We found 4 loci close to genome-wide significance that are suggestive to contribute to Df. The effect of these 4 novel loci could not be compared with Zekavat et al.5 due to the P-value < 10−04 truncation in their summary statistics. Nevertheless, differences between both Df GWAS can be attributed to our different strategies as the previously published GWAS combines multiple ancestries and does not control for individuals' relatedness, increasing then the type I error. Furthermore, published tortuosity GWAS17,20 reported the significant effect of COL4A2 and ACTN4 genes. Neither this study nor the Zekavat et al.5 paper found an association at these genomic regions, suggesting that Df and tortuosity also have distinct associated loci contributing to their regulation, which is consistent with published GWAS in retinal width and tortuosity17,20,32.
Most of the genetic variants we report here are relevant to multiple traits and diseases; for instance, the one located near HERC2 has been previously associated with hair33, skin40, and eye colour35; but recent studies also suggest a strong effect in AMD36, glaucoma37, intraocular pressure38, visual acuity39, retinal arterial width18,32, retinal vascular complexity and density5, and arterial and venular retinal tortuosity17,20. Another interesting associated SNP is the one near the SLC12A9 gene as it has been reported in pigmentation33,35,40, mean arterial pressure34, and resting heart rate42 GWAS. We found significant negative r2g estimates between Df and hypertension, CAD, and MI. The direction of these estimates agrees with their phenotypical correlations and published papers4,5,11, suggesting the correlation of phenotypes is influenced by its genetic correlation. This finding agrees with four aforementioned studies5,17,20,32 which identified novel retinal width and tortuosity loci associated with CAD but did not estimate a genetic correlation between retinal phenotypes and CAD.
We complemented our functional analysis with in silico TFBS disruptiveness prediction of credible variants. We observed four credible Df gene sets with a strong disruptive effect in 5 TFBS and 9 regulated genes, which participate at different Notch signalling pathway stages (Fig. 5). One possible mechanism to modulate its activity is through the alteration of ESRRA binding affinity, which influences VEGFA transcription. In-vitro and animal model studies indicate that after an MI event, VEGFA upregulation activates VEGF signalling pathway, which has a cross-link with Notch pathway and increases its activity45,53,54,55. Another mechanism derives from HES1 binding site affinity. HES1 influences MAML1 and NOTCH1 expression and directly affect Notch signalling45,46,47,56. The last mechanism influencing Notch activity is mediated through TBX20 binding site affinity, which plays a role in TLE3 transcription. Under a MI event, multiple studies indicate that TLE3 upregulation activates PI3K/Akt signalling pathway, a downstream process of Notch signalling pathway57,58. Numerous in-vitro and animal models studies support that this increased Notch activity, mediated by HES1, ESRRA and TBX20 upregulation, leads to reduction of cellular oxidative stress consequently improving myocardial viability, regeneration, and survival rate after a MI event45,46,47. We hypothesize that the TF binding disruption caused by these genetic variants influence Notch activity and, in the case of MI, might have a risk-conferring effect46,47,56,57,58,59,60,61,62. Furthermore, the alleles which predict a stronger TFBS disruptiveness have a negative effect size on Df (see Supplementary Figure 7). Then, we could speculate that individuals with higher Df might not have a disrupted Notch signalling pathway, which might be protective towards the response of a myocardial infarction event. An extended discussion is available in the Supplementary Table 5. Thus, these analyses suggest that there is an intricate shared genetic basis between vascular complexity and MI and further in-vitro experiments are needed to characterise gene expression and regulation of retinal tissue to better understand it.

a Protein–Protein interaction network of enriched TF and regulated genes. Upregulation of b ESRRA (top), c HES1 (middle) and d TBX20 (bottom) in VEGF and Notch signalling pathway after an MI event.
The potential of the retinal vasculature for stratifying the risk of Major Adverse Cardiac Events (MACE) has already been assessed in diabetic6,7 and non-diabetic8,10 individuals. Several predictive models have included retinal traits, either in a semantic6 or a non-semantic construction8, but reported very modest improvements in terms of AUC compared to the established risk estimation strategies based on epidemiological variables (e.g., 0.73 vs 0.72 in ref. 8). This discrepancy with our results might be attributed to the different clinical definitions of MACE, comprising normally a heterogeneous group of cardiovascular events where some of which might be not well captured in secondary care data. This situation reduces the model’s statistical power as there might be an overlap in case-control groups. In the case of diabetic population studies, both cases and controls also have comorbidities directly affecting the architecture of the retinal vasculature that might reduce predictive power for MACE risk. Theuerle et al.10 reported that retinal arterial dilation response to induced flickering light (FI-RAD) promisingly stratified MACE risk over 200 individuals from a local medical centre. Even though they found CAD family history and reduced FI-RAD to be the strongest MACE risk predictors, no comparison with traditional models is described. We could not assess the effect of this functional phenotype in this work as its computation derives from an invasive procedure that is not possible to apply retrospectively to existing imaging repositories (e.g. UKBB, SCONe). In this work, we focused on retinal structural variations, and MI events, and considered available ICD10 guidelines and UKBB validation reports of MI data to characterize cases, achieving the maximum possible statistical power.
Recent papers have addressed the additional predictive value of a CAD PRS in MACE and CAD risk stratification6,7,14,63,64,65. These approaches, although mainly developed in European populations, achieve a better identification of high-risk MI individuals than those strategies based only on epidemiological variables14,63,64,65. Given this promising finding and the observed shared genetic basis between Df and MI, we examined the effect of both retinal and genetic determinants on MI event risk stratification. We found that adequate clinical phenotyping is key to our models’ performance, but, as shown by our ablation study, the choice of the random forest algorithm, the use of continuous variables and the introduction of Df and PRSCAD in the model all independently improve traditional individual MI risk predictions in this moderate population of study. In addition, the model including these three modifications achieves the greatest performance. Df thus provides an early indication of coronary abnormalities not fully captured in clinical variables of these participants and that PRS accounts for the individual protective/risk-conferring effect on the genetic architecture of the disease. Hence, the proposed model has the potential, as illustrated in the Kaplan-Meier analysis, to stratify UKBB individuals by MI risk. This could be applicable to equivalent populations and after further external validations, allow for early targeted preventive efforts, like the administration of cholesterol-lowering treatments.
Our work has multiple limitations. Firstly, there are only 526 MI cases with a good-quality fundus image taken in UKBB. Higher numbers of such participants would allow us to train and evaluate our models more robustly. Secondly, the study population for the predictive models only consisted of UKBB participants with European ancestry with similar sociodemographic status, restricting the application of translational strategies to non-white European and British individuals among different sociodemographic profiles. Furthermore, the PRS included in the proposed predictive model is based on a meta-analysis completed with participants with mainly white European non-British and white British ancestries. Then, it is of utmost importance to complete GWAS in non-European populations to provide input for PRS estimations so that they are included in such medical applications. Thirdly, the stability of numerical estimates of the fractal dimension is the object of a continuing debate in the retinal image analysis community66,67,68. Fourth, we did not have an external validation cohort to complete an external validation of our MI model. This matter is attributed to the lack of available datasets containing extensive phenotyping from its participants. Finally, there is little information about the genetic expression profiles and the regulation mechanisms of retinal and ocular tissues in public databases. This might be influenced by the minority of studies across these tissues and the complicated protocols to extract and characterise them.
In conclusion, our study contributes to a growing body of evidence showing associations between abnormal morphologic characteristics in coronary vessels and retinal vascular remodelling. In particular, we found that credible fractal dimension loci modulate Notch signalling regulation, and partly explains the intricate shared genetic basis with MI. Remarkably, our MI model improved the stratification of the high-risk population. This is of great interest as it discloses a promising holistic strategy that can prevent MI incidence and triage those with an elevated MI hazard. This study ultimately sheds new light on the value of easily accessible vascular imaging phenotypes and their promising application in personalised medicine.
Methods
UK Biobank
UK Biobank (https://www.ukbiobank.ac.uk) is a large multi-site cohort study that consists of 502,655 individuals aged between 40 and 69 years at baseline, recruited from 22 centres across the UK during 2006–2010. The study was approved by the National Research Ethics Committee, reference 11/NW/0382, and informed consent was obtained from all participants as part of the recruitment and assessment process. From these, a baseline questionnaire, physical measurements, and biological samples were undertaken for each participant. Ophthalmic examination was not included in the original baseline assessment and was introduced as an enhancement in 6 UKBB centres across the UK. This examination consisted on capturing paired retinal fundus with a 45º primary field of view obtained with Topcon 3D OCT-1000 MKII (Topcon Corporation). This project was completed using fundus images collected in the first and the repeated ophthalmic examination which took place in 2012 and 2013. It includes 175,709 fundus images (87,552 left and 88,157 from the right) from 67,725 participants.
Image classification
Image quality was not reported in the UKBB cohort and was found wanting for the purpose of automatic analysis in the first study of this kind69. A previous study defined an automated classifier for this dataset using three imaging features following vessels segmentation: white pixel ratio (WPR), largest connected component ratio (LCCR) and the number of connected components (NCC) on a support vector machine (SVM) classifier25. We reproduced this classifier using a data subset of 448 random fundus images and VAMPIRE 3.1 software running in MATLAB 2018a23,24. The software performs automatic detection of the retinal vasculature, creating a binary vessel map for each image. A.V.V. manually classified the quality of these images based on the connectivity and the sharpness of the binary vessel map, and the lack of imaging artefacts. Manual classification was repeated 2 times using the same random subset of 100 images and the intra-classifier agreement coefficient was 0.897. This dataset was subsequently split in a training (n = 278) and validation (n = 170) sets. Both data subsets included an even number of manually classified good and bad quality images. We obtained a precision of 0.95, and a recall of 0.87, agreeing with the original study.
The classifier found 98,603 images with good quality from a total of 175,709 fundus images, of which 49,903 were from the right eye and 48,700 from the left eye. These images were derived from ~45,000 participants with different ancestries and included individuals with both or one eye examined at least one time. In the case of those participants that had two good quality images from one eye, following analyses are completed using the images obtained at the first examination.
Besides classification, the classifier returns an imaging quality score (IQS) based on the distance of an image from the classification boundary computed at the training phase of the SVM. We retrieved IQS using the score parameter in the prediction function running in MATLAB 2018a. We thus quantify individually the reliability of each image being classified as bad and good image.
Calculating fractal dimension
Retinal fractal dimension, Df, was computed from the binarized good-quality images using VAMPIRE software based on the multifractal analysis method70. This process was parallelised using 12 cores and 10GB per core.
Statistics and reproducibility
To compare left and right Df values we used participants who had both eyes scanned at the same UKBB examination and whose images were classified as good quality. 39,659 participants met these criteria. Both Df distributions were compared using a paired T-Test and by estimating the Pearson correlation with the SciPy package in python 3. We also fitted a linear regression using respectively left and right Df as dependent and independent variables.
We estimated the Pearson correlation and the effect of 779 UKBB traits on Df by fitting univariate linear regressions with each variable and using Df as the dependent variable. This included 121 quantitative variables (such as age, height, and BMI) and 658 binary variables (such as sex, diagnosed myopia, and diagnosed hypertension) which were extracted as reported elsewhere in30. The effect of IQS was also analysed following this approach. In addition, we evaluated the IQS difference effect on Df variability by fitting univariate linear regression using participants who had a good-quality image of both eyes scanned at the same UKBB examination. These analyses were completed using SciPy in python 3. Allied graphs were created using matplotlib and seaborn graphical packages in python 3.
Genome-wide association studies
We included 38,811 and 38,017 individuals in the right and left GWAS, respectively, with a self-reported and genotyped confirmed unrelated white-British ancestry71. Unrelated individuals were selected using a 0.0442 threshold from UKBB data and a previous work that established unrelated UKB participants with a white British ancestry30. Variants included were autosomal SNPs present in the genotyping arrays employed by UKBB and from the UKBB imputation panel with HWE > 10−6, MAF > 5 × 10−3, call rate >0.9 in unrelated white British individuals (kinship < 0.0442) and imputation score >0.9 in the imputed SNPs. The number of total SNPs analysed after quality control was 9,275,849.
Following genotype-level QC, a linear regression model was used to analyse the association of each SNP genotype with Df using PLINK v2.0. We assumed an additive genetic model, adjusting for age at examination, sex, IQS, assessment centre, the first 10 genomic principal components and genotyping batch. In addition, we included hair and skin colour as covariates to control for the influence of skin and eye colour on the fundus image colour, which can affect image segmentation and Df calculation. Hair colour replaced eye colour as the latter was not recorded during UKBB assessments, and it has a similar genetic control to eye pigmentation. Besides, we performed an additional GWAS including a polygenic risk score (PRS) for eye colour to assess its influence on our GWAS results. This PRS derives from an eye colour GWA study that defines it quantitatively (i.e., 1 = blue or grey, 2 = green, 3 = hazel, and 4 = brown) completed by Lona-Durazo et al. using the CanPath cohort, which includes ~5000 participants with European ancestry29. We estimated this PRS for each participant by extracting those independent genetic variants with a P-value < 5 × 10−8 from the summary statistics and applying linear regression to the effects of these SNPs and the genotypes of our UKBB participants (Supplementary Table 10). We then included this PRS as a covariate in an additional GWAS. Supplementary Figure 8 demonstrates that the results of these GWAS are analogous to those of GWAS including both skin and hair colour.
Furthermore, we completed a supplementary mean Df GWAS using those participants with white British ancestry from both left and right eye populations. We decided that mean Df was calculated only on those participants whose image quality score for both eyes was within 3SD from the population mean. If this condition was not met, we used the Df measure from the eye with the highest IQS or the available measure. This left us with a sample size of 39,799 participants.
QQ plots were generated using the R package qqman and ggplot2, and Manhattan plots and GWAS comparisons plots were generated using Matplotlib and seaborn libraries in python 3.
We completed a PheWAS to assess whether Df loci have a significant effect on other traits. To this end, we searched Df-associated SNPs in GWASCatalog31 and GeneATLAS30. GWAScatalog contains hundreds of GWAS performed in different traits and populations and it constantly updates new GWAS to its database. GeneATLAS contains GWAS summary statistics for 778 UKBB traits and diseases using individuals from European ancestry from UKBB. These genetic variants have a P-value smaller than 5 × 10−8 on the trait in order to assume a strong association common to Df.
GWAS and meta-analysis of Df loci across UKBB ancestries
We performed additional GWAS including UKBB participants with European non-British (nleft = 4340 and nright = 4288), Asian (nleft = 562 and nright = 568) and African ancestries (nleft = 498 and nright = 509) following the aforementioned model and procedure.
The multi-ancestry GWAS comparison was completed with those significant and independent SNPs from the Df GWAS including white British participants. We extracted the summary statistics of these SNPs from the Asian, African, and white-European GWAS and compared their effects across UKBB ancestries. Forest plots were carried out with Meta package in R 4.0 software.
Association between Df genetic risk score and Df measures in the CLSA
We complemented our replication study with an association analysis using Df measures and the genotypes from CLSA participants with a white European ancestry. The Canadian Longitudinal Study on Aging (CLSA) is a large, national, stratified, random sample of ~50,000 Canadians aged 45 to 85 years at the time of recruitment (2010–2015), followed until 2033 (or until death), which aims at investigating the associations between various risk factors and incidence of chronic diseases72. A subset of 30,000 participants (i.e., comprehensive subset) had physical examinations and biological specimen collection, including fundus photographs (1 for each eye) obtained using the Topcon TRC-NW8 non-mydriatic retinal camera. A total of 50,957 retinal photographs, from 25,717 CLSA participants, were analysed using VAMPIRE (Vascular Assessment and Measurement Platform for Images of the Retina) software version 3.1, to compute the image quality (good/moderate/poor) and the fractal dimension (Df) of the retinal vascular pattern. Participants with poor quality images for both eyes were excluded for subsequent analyses.
Among the comprehensive subset, 26,622 CLSA participants (with 93% of Europeans) were successfully genotyped using the UK Biobank Array71. Quality control steps have been detailed elsewhere73. Briefly, phasing and imputation were conducted using the TOPMed reference panel74 at the University of Michigan Imputation Service75. We used the TOPMed reference panel version r2, and then pre-phased and imputed the genotype data using EAGLE276 and Minimac77 respectively, for both autosomal and X chromosomes. Samples with low call rates (<95%), sex mismatches, or cryptic relatedness were removed. Imputed SNPs were excluded on the basis of HWE > 10−6, MAF > 1 × 10−4, call rate >0.9, and imputation quality (imputation score <0.6).
A total of 19 independent genetic variants significantly associated with Df in the UKB were selected to calculate a genetic risk score (GRS) (Supplementary Table 11). CLSA Individual’s risk score consisted in the sum of each SNP dosage weighted by each SNP-Df association coefficient given in Df unit per effect allele. A linear regression was performed to estimate the association between FD measures and Df GRS in 16,205 CLSA participants, with at least one retinal image of moderate or good quality of either side, and suitable genetic material. Models were adjusted for the 20 first principal components.
Genetic correlation and heritability estimation
To investigate the shared genetic signal between Df and associated traits, we estimated their genome-wide genetic correlation. For this purpose, we obtained the GWAS summary statistics of traits of interest to our study from GeneATLAS and the eye colour study29. These calculations were computed with LD Score43, a toolbox that estimates genetic correlation using GWAS summary statistics considering possible inflation caused by SNPs in linkage disequilibrium (LD). To ascertain the LD blocks within each variant, the software uses the 1000 Genomes panel as reference. Heatmaps were created with the genetic correlation estimate using the seaborn library in python 3.
LD Score was also used to calculate the SNP heritability of both eyes’ Df. In this case, the software uses the reference map and the GWAS summary statistics to estimate the fraction of Df variance explained by the SNPs’ additive effect.
Mendelian randomization
To infer the causality between the shared genetic basis of CAD, MI, hypertension and Df, we performed a Mendelian randomization analysis. For this procedure, we extracted the summary statistics of MI, hypertension, and CAD from GeneATLAS. We next selected for each cardiovascular condition separately those SNPs with a P-value < 5 × 10−08, and MAF > 0.01. We then selected those independent SNPs which were not palindromic by clumping these regions in windows of 10,000 kb and applying a r2 < 0.001 and a significance of 0.99 thresholds. The effect and the significance of these variants were also extracted from Df GWAS summary statistics. We then estimated the causal effect of these genetic variants through different methods (inverse-variance weighted regression, Egger’s regression, and Maximum likelihood) to analyse whether using different scenarios could better characterise the causality. This process was completed with TwoSamplesMR package in R 4.078. This package applies a quality control and a sensitivity analysis to evaluate the presence of palindromic SNPs, pleiotropy and heterogeneity which might influence the results of the study.
Fine-mapping
Fine-mapping of significant Df SNPs was completed with SusieR v.0.11.42 R package79. For each significant variant locus, we selected those variants that were located within 1 Mbp window at each side and estimated the correlation matrix among them with plink v1.9. Next, we ran the Susie_rss function with the Z-score from Df GWAS and the correlation matrix of the previously selected variants. We ascertained that each credible set must have a coverage >0.95 and a minimum and median correlation coefficient (purity) of r = 0.1 and 0.5, respectively.
Transcription factor binding sites prediction
The identification of variants with strong evidence to disrupt TF binding activity based on position probability matrices (PPM) was carried out with the R library motifbreakR v2.2.080. For the TFBS we used default settings except the P-value threshold to declare TF binding site matching either of the allelic configurations, which was set to 5 × 10−04, and the relative entropy scoring method set to information content algorithm (method = ic) as performed in81. MotifDb and motifbreakR_motif were the selected databases of TF motifs which contain 14 public collections (including JASPAR, HOCOMOCO, ENCODE, HOMER and FactorBook) to perform this analysis. We calculated accurate P-values for both reference and alternative alleles by implementing calculatePvalue() function. We investigated those TFBS motifs with a P-value < 0.001 in both alleles and an absolute allelic score difference > 1.5.
Protein–protein interaction networks analyses were completed with those TF that bind at significant TFBS and the regulated genes located within a 150 kb window using DAVID82 and STRING83 software. We considered associated pathways those with an FDR and Bonferroni correction < 0.001.
Development of MI predictive model
We used a subset of the UKBB data for MI model training and evaluation. We extracted white British UKBB participants who had good-quality images and a MI event after UKBB recruitment. MI events were defined in UKBB as a participant self-reporting MI at first repeated assessment visit [code 1075 from UKBB data field 20002] and MI hospitalizations identified using ICD10 codes [codes I21.1, I21.2, I21.3, I21.4, I21.9, I22, I22.0, I22.1, I22.8, I22.9, I23, I23.0, I23.1, I23.2, I23.3, I23.4, I23.5, I23.6, I23.8, I24.1, and I25.2 from UKBB data field 41204 and 41202]. The UKBB team previously validated this MI extraction algorithm and reported a minimum precision of 75%84. To define incident cases occurring after UKBB recruitment we used the date of the MI event [UKBB algorithmically defined MI event date from data field 42000] and the approximate period when participants underwent the ophthalmic examination, resulting in 526 incident cases. We randomly selected an equal number of age-matched participants with good-quality images of both eyes no cardiovascular event within the CAD spectrum and no known risk factor (e.g., hypertension, and family history of heart disease). This match was completed using the age range of the cases (i.e. 45–61 years) and constricting the random selection of controls to these ages.
Our MI predictive model uses age at baseline, sex, systolic blood pressure, smoking status, BMI, and a polygenic risk score for CAD and Df of both eyes separately as features in a classification algorithm. We chose a random forest classifier algorithm allowing both non-linear associations between outcome and variables as well as inter-variable interaction in the model. Permutation-based feature importance scores85 were extracted in the modelling phase to assess the effect of each variable in the random forest construction using the feature_importances_ function from the scikit-learn package. Given the influence of IQS on Df, we trained an additional model replacing Df to Df adjusted by IQS to assess the existence of major differences in the model’s performance. We also tested whether introducing just one eye Df in the model implied major differences in its performance.
We then extracted the information of the established risk variables, that is, age, sex, SBP, BMI, and smoking status, for the population of study using the curated phenotypes from UK Biobank July 2017 release30 We extracted controls only considering those UKBB participants with no missing data and both Df measures, as the majority of individuals with a Df measure were healthy. 56 MI cases had a missing Df measure from one eye. In these cases, we did not predict the missing value and only used the available Df measure.
To evaluate the performance of the predictive model, we reproduced SCORE with this MI dataset. SCORE uses age, sex, systolic blood pressure, smoking status, and BMI as input variables for logistic regression, with quantitative variables being discretized using healthcare guidelines8. We then assessed each model’s performance by using internal 10-fold cross-validation and computing its AUC, precision, and recall. We used the same data partitions across SCORE and our MI models. A Wilcoxon signed-rank test was completed across all the trained models to evaluate the significance of the AUC differences.
We used Kaplan–Meier curves to assess the difference in survival rate difference between patients with high and low predicted MI probability, dichotomised at a probability of 0.5. This probability was obtained with our top-performing MI model. A Log-rank test was completed to evaluate the difference between these groups’ curves.
We investigated the sources of improvement of our MI model compared to the SCORE model through an ablation study. The model differs from SCORE in four key aspects: (1) introducing Df, (2) the use of not-discretized quantitative variables, (3) using Random Forest instead of logistic regression, and (4) introducing PRSCAD. This ablation study consisted of assessing the performance of a modified version of SCORE through its AUC, recall and precision. These modifications included all the possible independent combinations across these alterations.
This part of the study was written in Python 3.5.7 using the sci-kit-learn, NumPy and Pandas packages. ROC curves were plotted using the predicted MI probability from each model using the ROCurve plot package in R 4.0. Both Kaplan–Meier curves and the Log-rank test were completed with the lifelines Python package.
Estimating CAD polygenic risk score
PRSCAD derives from the CARDIoGRAMplusC4D Consortium21 which is one of the largest completed CAD meta-analyses. This study does not include UKBB data, but it is developed with multiple CAD databases with different ancestries to better characterise the genetic control of this outcome. We estimated PRSCAD for each participant in the MI dataset by using PRSice-2 software86, the summary statistics of the meta-analysis, and the genotypes of this MI dataset. We then included this PRS as a variable in our MI predictive model.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The authors declare that the data supporting the findings of the present study are available within the paper and its supplementary information files. The fractal dimension GWAS summary statistics of all fitted models are openly available from the University of Edinburgh DataShare repository within the following collection: https://datashare.ed.ac.uk/handle/10283/4794. Data are available from the Canadian Longitudinal Study on Aging (www.clsa-elcv.ca) for researchers who meet the criteria for access to de-identified CLSA data.
Code availability
The authors declare that the customised code for the myocardial infarction predictive model is available within the following GitHub repository: //github.com/Anavillaplana/MI_risk_prediction.
References
Roth, G. A. et al. Global burden of cardiovascular diseases and risk factors, 1990–2019. J. Am. Coll. Cardiol. 76, 2982–3021 (2020).
Wong, T. Y. et al. Retinal vascular caliber, cardiovascular risk factors, and inflammation: the multi-ethnic study of atherosclerosis (MESA). Invest. Ophthalmol. Vis. Sci. 47, 2341–2350 (2006).
MacGillivray, T. J. et al. Retinal imaging as a source of biomarkers for diagnosis, characterization and prognosis of chronic illness or long-term conditions. Br. J. Radiol. 87, (2014).
Wang, S. B. et al. A spectrum of retinal vasculature measures and coronary artery disease. Atherosclerosis 268, 215–224 (2018).
Zekavat, S. M. et al. Deep learning of the retina enables phenome- and genome-wide analyses of the microvasculature. Circulation 145, 134–150 (2022).
Fetit, A. E. et al. A multimodal approach to cardiovascular risk stratification in patients with type 2 diabetes incorporating retinal, genomic and clinical features. Sci. Rep. 9, 3591 (2019).
Mordi, I. R. et al. Prediction of major adverse cardiovascular events from retinal, clinical, and genomic data in individuals with type 2 diabetes: a population cohort study. Diabetes Care 45, 710–716 (2022).
Poplin, R. Prediction of cardiovascular risk factors from retinal fundus photographs via deep learning. Nat. Biomed. Eng. 2, 9 (2018).
Diaz-Pinto, A. et al. Predicting myocardial infarction through retinal scans and minimal personal information. Nat. Mach. Intell. 4, 55–61 (2022).
Theuerle, J. D. et al. Impaired retinal microvascular function predicts long-term adverse events in patients with cardiovascular disease. Cardiovasc. Res. https://doi.org/10.1093/cvr/cvaa245 (2020).
Liew, G. et al. Fractal analysis of retinal microvasculature and coronary heart disease mortality. Eur. Heart J. 32, 422–429 (2011).
Sim, X. et al. Genetic loci for retinal arteriolar microcirculation. PLoS ONE https://doi.org/10.1371/journal.pone.0065804 (2013).
Fedele, F., Pucci, M. & Severino, P. Genetic Polymorphisms and Ischemic Heart Disease. https://doi.org/10.5772/intechopen.69621 (IntechOpen, 2017).
Riveros-Mckay, F. et al. Integrated Polygenic Tool Substantially Enhances Coronary Artery Disease Prediction. Circ. Genom. Precis. Med. 14, e003304 (2021).
Agrawal, H., Choy, H. K., Liu, J., Auyoung, M. & Albert, M. A. Coronary artery disease. Arterioscler. Thromb. Vasc. Biol. 40, 85–192 (2020).
Elosua, R. & Sayols-Baixeras, S. The genetics of ischemic heart disease: from current knowledge to clinical implications. Rev. Esp. Cardiol. Engl. Ed. 70, 754–762 (2017).
Veluchamy, A. et al. Novel genetic locus influencing retinal venular tortuosity is also associated with risk of coronary artery disease. Arterioscler. Thromb. Vasc. Biol. https://doi.org/10.1161/ATVBAHA.119.312552 (2019).
Ikram, M. K. et al. Four novel loci (19q13, 6q24, 12q24, and 5q14) influence the microcirculation in vivo. PLOS Genet. 6, e1001184 (2010).
Fahy, S. J. et al. The relationship between retinal arteriolar and venular calibers is genetically mediated, and each is associated with risk of cardiovascular disease. Invest. Ophthalmol. Vis. Sci. 52, 975–981 (2011).
Tomasoni, M. et al. Genome-Wide Association Studies of retinal vessel tortuosity identify 173 novel loci, capturing genes and pathways associated with disease and vascular tissue pathomechanics. Preprint at medRxiv https://doi.org/10.1101/2020.06.25.20139725 (2021).
Nikpay, M. et al. A comprehensive 1000 Genomes–based genome-wide association meta-analysis of coronary artery disease. Nat. Genet. 47, 1121–1130 (2015).
Conroy, R. M. et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur. Heart J. 24, 987–1003 (2003).
Trucco, E. et al. Novel VAMPIRE algorithms for quantitative analysis of the retinal vasculature. in 2013 ISSNIP Biosignals Biorobotics Conf. Biosignals Robot. Better Safer Living BRC (2013).
Mookiah, M. R. K., Hogg, S., MacGillivray, T. & Trucco, E. On the quantitative effects of compression of retinal fundus images on morphometric vascular measurements in VAMPIRE. Comput. Methods Prog. Biomed. 202, 105969 (2021).
Welikala, R. A. et al. Automated retinal image quality assessment on the UK Biobank dataset for epidemiological studies. Comput. Biol. Med. 71, 67–76 (2016).
Bonferroni, C. E. Il calcolo delle assicurazioni su gruppi di teste (Tipografia del Senato, 1935).
Rochtchina, E., Wang, J. J., Taylor, B., Wong, T. Y. & Mitchell, P. Ethnic variability in retinal vessel caliber: a potential source of measurement error from ocular pigmentation?—The Sydney childhood eye study. Invest. Ophthalmol. Vis. Sci. 49, 1362–1366 (2008).
Li, X. et al. Racial differences in retinal vessel geometric characteristics: a multiethnic study in healthy Asians. Invest. Ophthalmol. Vis. Sci. 54, 3650–3656 (2013).
Lona-Durazo, F. et al. Investigating the genetic architecture of eye colour in a Canadian cohort. iScience. 25, 104485 (2022).
Canela-Xandri, O., Rawlik, K. & Tenesa, A. An atlas of genetic associations in UK Biobank. Nat. Genet. 50, 1593–1599 (2018).
Buniello, A. et al. The NHGRI-EBI GWAS Catalog of published genome-wide association studies, targeted arrays and summary statistics 2019. Nucleic Acids Res. 47, D1005–D1012 (2019).
Jensen, R. A. et al. Novel genetic loci associated with retinal microvascular diameter. Circ. Cardiovasc. Genet. 9, 45–54 (2016).
Morgan, M. D. et al. Genome-wide study of hair colour in UK Biobank explains most of the SNP heritability. Nat. Commun. 9, 5271 (2018).
Liu, C. et al. Meta-analysis identifies common and rare variants influencing blood pressure and overlapping with metabolic trait loci. Nat. Genet. 48, 1162–1170 (2016).
Adhikari, K. et al. A GWAS in Latin Americans highlights the convergent evolution of lighter skin pigmentation in Eurasia. Nat. Commun. 10, 358 (2019).
Guenther, F. et al. Chances and challenges of machine learning-based disease classification in genetic association studies illustrated on age-related macular degeneration. Genet. Epidemiol. 44, 759–777 (2020).
Craig, J. E. et al. Multitrait analysis of glaucoma identifies new risk loci and enables polygenic prediction of disease susceptibility and progression. Nat. Genet. 52, 160–166 (2020).
Zhou, W. et al. Efficiently controlling for case-control imbalance and sample relatedness in large-scale genetic association studies. Nat. Genet. 50, 1335–1341 (2018).
Currant, H. et al. Genetic variation affects morphological retinal phenotypes extracted from UK Biobank optical coherence tomography images. PLoS Genet. 17, e1009497 (2021).
Liu, F. et al. Genetics of skin color variation in Europeans: genome-wide association studies with functional follow-up. Hum. Genet. 134, 823–835 (2015).
Lona-Durazo, F. et al. A large Canadian cohort provides insights into the genetic architecture of human hair colour. Commun. Biol. 4, 1253 (2021).
Eijgelsheim, M. et al. Genome-wide association analysis identifies multiple loci related to resting heart rate. Hum. Mol. Genet. 19, 3885–3894 (2010).
Bulik-Sullivan, B. et al. An atlas of genetic correlations across human diseases and traits. Nat. Genet. 47, 1236–1241 (2015).
Lemmens, S. et al. Systematic review on fractal dimension of the retinal vasculature in neurodegeneration and stroke: assessment of a potential biomarker. Front. Neurosci. 14, 16 (2020).
Aquila, G. et al. The Notch pathway: a novel therapeutic target for cardiovascular diseases? Expert Opin. Ther. Targets 23, 695–710 (2019).
Gude, N. A. et al. Activation of Notch-mediated protective signaling in the myocardium. Circ. Res. 102, 1025–1035 (2008).
Pei, H. et al. Notch1 cardioprotection in myocardial ischemia/reperfusion involves reduction of oxidative/nitrative stress. Basic Res. Cardiol. 108, 373 (2013).
Lee, J., Cai, J., Li, F. & Vesoulis, Z. A. Predicting mortality risk for preterm infants using random forest. Sci. Rep. 11, 7308 (2021).
Chowdhury, A. R., Chatterjee, T. & Banerjee, S. A Random Forest classifier-based approach in the detection of abnormalities in the retina. Med. Biol. Eng. Comput. 57, 193–203 (2019).
Cameron, J. R. et al. Lateral thinking – Interocular symmetry and asymmetry in neurovascular patterning, in health and disease. Prog. Retin. Eye Res. 59, 131–157 (2017).
Sevik, U., Kose, C., Berber, T. & Erdol, H. Identification of suitable fundus images using automated quality assessment methods. J. Biomed. Opt. 19, 046006 (2014).
Chalakkal, R. J., Abdulla, W. H. & Thulaseedharan, S. S. Quality and content analysis of fundus images using deep learning. Comput. Biol. Med. 108, 317–331 (2019).
Zhou, Y. et al. The role of the VEGF family in coronary heart disease. Front. Cardiovasc. Med. 8, 738325 (2021).
Zhao, T., Zhao, W., Chen, Y., Ahokas, R. A. & Sun, Y. Vascular endothelial growth factor (VEGF)-A: role on cardiac angiogenesis following myocardial infarction. Microvasc. Res. 80, 188–194 (2010).
Collén, A. et al. VEGFA mRNA for regenerative treatment of heart failure. Nat. Rev. Drug Discov. 21, 79–80 (2022).
Zhou, X., Zhao, Y., Fang, Y., Xu, Q. & Liu, J. Hes1 is upregulated by ischemic postconditioning and contributes to cardioprotection. Cell Biochem. Funct. 32, 730–736 (2014).
Shen, T. et al. Tbx20 regulates a genetic program essential to adult mouse cardiomyocyte function. J. Clin. Invest. 121, 4640–4654 (2011).
Xiang, F., Guo, M. & Yutzey, K. E. Overexpression of Tbx20 in adult cardiomyocytes promotes proliferation and improves cardiac function after myocardial infarction. Circulation 133, 1081–1092 (2016).
Croquelois, A. et al. Control of the adaptive response of the heart to stress via the Notch1 receptor pathway. J. Exp. Med. 205, 3173–3185 (2008).
Xie, M., Tang, Y. & Hill, J. A. HDAC inhibition as a therapeutic strategy in myocardial ischemia/reperfusion injury. J. Mol. Cell. Cardiol. 129, 188–192 (2019).
Ferreira, J. P., Pitt, B. & Zannad, F. Histone deacetylase inhibitors for cardiovascular conditions and healthy longevity. Lancet Healthy Longev. 2, e371–e379 (2021).
Zou, J. et al. VEGF-A promotes angiogenesis after acute myocardial infarction through increasing ROS production and enhancing ER stress-mediated autophagy. J. Cell. Physiol. 234, 17690–17703 (2019).
Fahed, A. C. et al. Polygenic background modifies penetrance of monogenic variants for tier 1 genomic conditions. Nat. Commun. 11, 3635 (2020).
Yanes, T., McInerney-Leo, A. M., Law, M. H. & Cummings, S. The emerging field of polygenic risk scores and perspective for use in clinical care. Hum. Mol. Genet. 29, R165–R176 (2020).
Mars, N. et al. Polygenic and clinical risk scores and their impact on age at onset and prediction of cardiometabolic diseases and common cancers. Nat. Med. 26, 549–557 (2020).
Huang, F. et al. Reliability of using retinal vascular fractal dimension as a biomarker in the diabetic retinopathy detection. J. Ophthalmol. 2016, e6259047 (2016).
Cosatto, V. F. et al. Retinal vascular fractal dimension measurement and its influence from imaging variation: results of two segmentation methods. Curr. Eye Res. 35, 850–856 (2010).
McGrory, S. et al. Towards standardization of quantitative retinal vascular parameters: comparison of SIVA and VAMPIRE Measurements in the Lothian Birth Cohort 1936. Transl. Vis. Sci. Technol. 7, 12 (2018).
MacGillivray, T. J. et al. Suitability of UK Biobank retinal images for automatic analysis of morphometric properties of the vasculature. PLoS ONE 10, e0127914 (2015).
Stosic, T. & Stosic, B. D. Multifractal analysis of human retinal vessels. IEEE Trans. Med. Imaging 25, 1101–1107 (2006).
Bycroft, C. et al. The UK Biobank resource with deep phenotyping and genomic data. Nature 562, 203–209 (2018).
Raina, P. et al. Cohort profile: the Canadian Longitudinal Study on Aging (CLSA). Int. J. Epidemiol. 48, 1752–1753j (2019).
Forgetta, V. et al. Cohort profile: genomic data for 26 622 individuals from the Canadian Longitudinal Study on Aging (CLSA). BMJ Open 12, e059021 (2022).
Taliun, D. et al. Sequencing of 53,831 diverse genomes from the NHLBI TOPMed Program. Nature 590, 290–299 (2021).
Das, S. et al. Next-generation genotype imputation service and methods. Nat. Genet. 48, 1284–1287 (2016).
Loh, P.-R. et al. Reference-based phasing using the Haplotype Reference Consortium panel. Nat. Genet. 48, 1443–1448 (2016).
Fuchsberger, C., Abecasis, G. R. & Hinds, D. A. minimac2: faster genotype imputation. Bioinformatics 31, 782–784 (2015).
Davey Smith, G. & Hemani, G. Mendelian randomization: genetic anchors for causal inference in epidemiological studies. Hum. Mol. Genet. 23, R89–R98 (2014).
Zou, Y., Carbonetto, P., Wang, G. & Stephens, M. Fine-mapping from summary data with the “Sum of Single Effects” model. PLoS Genet. 18, e1010299 (2022).
Coetzee, S. G., Coetzee, G. A. & Hazelett, D. J. motifbreakR: an R/Bioconductor package for predicting variant effects at transcription factor binding sites. Bioinformatics 31, 3847–3849 (2015).
Jiang, X. et al. Fine-mapping and cell-specific enrichment at corneal resistance factor loci prioritize candidate causal regulatory variants. Commun. Biol. 3, 1–12 (2020).
Huang, D. W., Sherman, B. T. & Lempicki, R. A. Systematic and integrative analysis of large gene lists using DAVID bioinformatics resources. Nat. Protoc. 4, 44–57 (2009).
Szklarczyk, D. et al. The STRING database in 2021: customizable protein–protein networks, and functional characterization of user-uploaded gene/measurement sets. Nucleic Acids Res. 49, D605–D612 (2021).
Schnier, C., Bush, K., Nolan, J. & Sudlow, C. Definitions of Acute Myocardial Infarction and Main Myocardial Infarction Pathological Types UK Biobank Phase 1 Outcomes Adjudic. https://biobank.ndph.ox.ac.uk/showcase/showcase/docs/alg_outcome_mi.pdf (2017).
Breiman, L. Random forests. Mach. Learn. 45, 5–32 (2001).
Choi, S. W., Mak, T. S.-H. & O’Reilly, P. F. Tutorial: a guide to performing polygenic risk score analyses. Nat. Protoc. 15, 2759–2772 (2020).
Acknowledgements
This research has been conducted using the UK Biobank Resource under project 788. This research was funded in part by the Medical Research Council grant (MR/N013166/1) to A.V.V. This research was also made possible using the data/biospecimens collected by the Canadian Longitudinal Study on Aging (CLSA). Funding for the Canadian Longitudinal Study on Aging (CLSA) is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference: LSA 94473 and the Canada Foundation for Innovation, as well as the following provinces, Newfoundland, Nova Scotia, Quebec, Ontario, Manitoba, Alberta, and British Columbia. This research has been conducted using the CLSA dataset 1906019_McMaster_GPare_Baseline (Baseline Comprehensive (COM) version 4.2), under Application Number 1906019. The CLSA is led by Drs. Parminder Raina, Christina Wolfson and Susan Kirkland. This work is supported by the Roslin Institute Strategic Programme Grant from the BBSRC (BBS/E/D/30002275 and BBS/E/D/30002276) to A.T.; Health Data Research UK grants (references HDR-9004 and HDR-9003) to A.T.; the Engineering and Physical Sciences Research Council (EPSRC) grant (EP/R029598/1, EP/T008806/1) to M.O.B.; Fondation Leducq grant (17 CVD 03) to M.O.B., the European Union’s Horizon 2020 research and innovation programme under grant agreement No 801423 to M.O.B.; Diabetes UK grant (20/0006221) to M.O.B.; Fight for Sight grant (5137/5138) to M.O.B.; and British Heart Foundation and The Alan Turing Institute (which receives core funding under the EPSRC grant EP/N510129/1) as part of the Cardiovascular Data Science Awards Round 2 (SP/19/9/34812) to M.O.B. Support from NHS Lothian R&D and the Edinburgh Clinical Research Facility is acknowledged. M.P. was supported by the E.J. Moran Campbell Internal Career Research Award from McMaster University, and the Early Career Research Award from Hamilton Health Sciences (HHS). Retinal images analyses of the CLSA were supported by a New Investigator Fund from HHS (NIF-18453 to M.P.), and the Canadian Institutes of Health Research (CIHR) (ACD-170312 and PJT-178302 to M.P.). For the purpose of open access, the author has applied a creative commons attribution (CC BY) licence to any author accepted manuscript version arising.
Author information
Authors and Affiliations
Contributions
M.O.B., E.P.C. and A.T. contributed to the study design. A.V.V., M.P. and J.E. contributed to data analysis. A.V.V prepared the initial manuscript. A.V.V., M.P., J.E., K.Rawlik, O.C.X., F.L.D., C.T., M.R.K.M., A.D, E.J.P., E.T., T.M., K.Rannikmae, A.T., E.P.C. and M.O.B. contributed to writing and reviewing the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Biology thanks Anthony Khawaja and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editors: Helene Choquet and Manuel Breuer. Peer reviewer reports are available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Villaplana-Velasco, A., Pigeyre, M., Engelmann, J. et al. Fine-mapping of retinal vascular complexity loci identifies Notch regulation as a shared mechanism with myocardial infarction outcomes. Commun Biol 6, 523 (2023). https://doi.org/10.1038/s42003-023-04836-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s42003-023-04836-9
This article is cited by
-
A hybrid ResNet-ViT approach to bridge the global and local features for myocardial infarction detection
Scientific Reports (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
