
Abstract
Providing accessible and effective healthcare solutions for people living in low- and middle-income countries, migrants, and indigenous people is central to reduce the global mental health treatment gap. Internet- and mobile-based interventions (IMI) are considered scalable psychological interventions to reduce the burden of mental disorders and are culturally adapted for implementation in these target groups. In October 2020, the databases PsycInfo, MEDLINE, Embase, Cochrane Central Register of Controlled Trials, and Web of Science were systematically searched for studies that culturally adapted IMI for mental disorders. Among 9438 screened records, we identified 55 eligible articles. We extracted 17 content, methodological, and procedural components of culturally adapting IMI, aiming to consider specific situations and perspectives of the target populations. Adherence and effectiveness of the adapted IMI seemed similar to the original IMI; yet, no included study conducted a direct comparison. The presented taxonomy of cultural adaptation of IMI for mental disorders provides a basis for future studies investigating the relevance and necessity of their cultural adaptation.
PROSPERO registration number: CRD42019142320.
Similar content being viewed by others


Introduction
The World Health Organisation has called to take action in order to address global health inequalities1 as one of the major global health challenges2,3,4,5. Particularly when it comes to mental health, the treatment gap in low- and middle-income countries (LMIC) is estimated to be far higher than that in high-income countries: Whereas ~76–85% of people with a serious mental disorder living in LMIC do not get treated, ~35–50% of people living in high-income countries do not get treated1,6,7. Similarly, migrants and refugees make less use of mental health services8,9,10, although they face many stressors before, during, and after migration11 and show an increased prevalence of mental disorders12,13,14. Such a mental health treatment gap can also be observed in indigenous people, caused by lower mental health15,16 and lower use of health services17. In order to improve global health equality, existing barriers of these populations need to be addressed on a structural and individual level.
Existing structural barriers, such as a lack of mental health services and difficulties in accessing services18,19,20,21, could be reduced by low intensity interventions22,23,24,25. Low intensity interventions are interventions aiming to be easy to access by a high number of people, due to a resource-saving and flexible delivery (e.g., self-help interventions, interventions delivered by non-professionals)26. Internet- and mobile-based interventions (IMI) as one kind of low intensity intervention offer anonymity, temporal and local independency, easy accessibility, and scalability27,28,29,30 and are thus suggested to hold potential in overcoming structural healthcare barriers31,32. Despite reports of lower treatment completion rates33, IMI have been proven effective in preventing and treating mental disorders34,35,36,37,38. However, they were mostly developed for and evaluated in majority populations from high-income countries, and were found to be less effective for people with a differing cultural or ethnic background39. When it comes to the use of healthcare, populations living in LMIC, as well as migrants, refugees, or indigenous people face a range of individual barriers, such as language and cultural barriers (e.g., understanding of disease and treatment processes) or poor knowledge on the healthcare system17,18,19,20,21,40. These individual barriers may be reduced by considering cultural aspects in the intervention development, i.e., including knowledge on potential cultural differences41. However, newly developing interventions for each population requires significant effort. A more resource-saving possibility could be to use the high number of already existing and evaluated psychological treatments and to culturally adapt them for the new target groups42,43.
A cultural adaptation should be conducted in a structured, systematic way by following adaptation guidelines44,45. Various research groups established such guidelines, focussing (a) on specific treatment components that should be culturally adapted46,47,48,49,50,51, or (b) on the procedure that should be followed to gradually adapt the treatment45,52,53,54. The Ecological Validity Framework by Bernal et al.47 was the first model describing in detail what to culturally adapt. The authors recommended the consideration of eight intervention components, including language (translation, differences in regional or subcultural groups), persons (patient–therapist relationship, roles), metaphors (symbols, sayings), content (values, customs, traditions), concepts (theoretical model of the treatment), goals (agreement of therapist and patient), methods (procedures for achieving the treatment goals), and context (broader social, economic, and political contexts). This model was widely reused and can be seen as a base for later frameworks. For example, Resnicow et al.50 differentiated the components to adapt into surface characteristics, such as language, locations, and persons, and deep structure characteristics of treatment, which comprise the inclusion of cultural, social, environmental, and historical factors to consider the understanding of disease and its treatment of the respective clients, such as cultural values (e.g., family) and specific stressors (e.g., racism). Regarding frameworks on the procedure of culturally adapting treatments, Barrera and Castro summarised various suggestions of other frameworks in their Heuristic Framework for the Cultural Adaptations of Interventions54. They describe the procedural components of how to culturally adapt by (1) gathering information by literature searches or qualitative research, (2) developing a preliminary adaptation based on this information, (3) testing the preliminary adaptation in case or pilot studies, and (4) refining the adaptation based on the findings of case or pilot studies.
Considering both the suggested content and procedural components of cultural adaptation intends to facilitate access to psychological treatments for people with a cultural background differing from that of the original target group44. Correspondingly, findings of meta-analyses aiming to investigate the relevance and necessity of cultural adaptation suggest that, in populations that the intervention was originally not developed for, culturally adapted treatments are more effective as compared to non-adapted versions of the treatment55,56. The higher the extent of cultural adaptation, the higher seems their effectiveness57,58. Based on this revealed relevance of culturally adapting face-to-face treatments, it may also be of relevance to culturally adapt IMI to reach out to people with a cultural background differing from the original target group25,59,60. Various research groups culturally adapted IMI to fit new target groups and showed their effectiveness61,62,63. Furthermore, a meta-analysis indicated that an enhanced cultural adaptation of an IMI was associated with its increased effectiveness in the respective target group59. However, studies directly comparing the effectiveness or acceptance of culturally adapted versus non-/less-adapted IMI are lacking59,64,65,66, which would allow for drawing conclusions on the added value of cultural adaptation. A precondition for such comparison trials and for examining the relevance of adapting specific components following a specific procedure would be a systematic and well-documented adaptation67,68. Yet, components and procedures considered in the cultural adaptation of IMI are often only poorly reported69,70,71,72,73. Thus, research on the cultural adaptation of IMI is still in its early stages66, and there is a particular lack of knowledge on specific aspects of IMI that might need cultural adaptation in addition to the components adapted in face-to-face treatments. In this context, following aspects of evaluation frameworks of IMI could provide an orientation, such as methodological components to enhance the user engagement with the IMI, its ease of use, or design and aesthetics74,75,76.
Thus, this review aims to
-
(1)
systematically identify and summarise content, methodological, and procedural components considered in the previous cultural adaptations of IMI for mental disorders;
-
(2)
summarise results on the adherence and effectiveness of culturally adapted IMI.
By providing a taxonomy on the cultural adaptation of IMI, this review may inform researchers on systematically developing scalable interventions for underserved people.
Results
Study selection
A total of 20,012 articles were retrieved from the electronic databases; 21 articles were added by hand searching relevant articles. After removing duplicates, 9438 titles and abstracts were screened, leading to 258 records that were included in the full-text screening. In 24% of the decisions, the inclusion of a study was discussed between the reviewers. Finally, 55 studies were found eligible for the present qualitative synthesis, of which 28 provided quantitative data (see Fig. 1).

Process of study identification, screening, eligibility verification, and inclusion decision (adapted from Liberati et al.115).
Study characteristics
All 55 included articles were published between 2012 and 2020, with 38 (69.1%) published in 2018–2020. Eight of them were study protocols, three of which additionally described conducted qualitative studies. Across the studies conducted in the included articles, a total of 3789 participants took part, plus a sample of 23,235 participants of a study analysing existing data of a patients cohort77. The studies were conducted or planned to be conducted in various countries: 26 in North America and Europe, 16 in Asia, 5 in Australia, 4 in the Middle East, and 2 in South or Central America. Similarly, the ethnicities of the participants were diverse across the studies: 34.6% of the studies included Asian participants, 26.9% Arabic, 15.4% European, 11.5% Northern American (including 7.7% American Indian/Alaskan Native), and 11.5% participants with other ethnic backgrounds. The included articles reported on the cultural adaptation of 42 different interventions. For 23 interventions, detailed information on their cultural adaptation had been published; for 19 interventions, less detailed information was available in published articles. Partly, more details were provided by the authors upon request (n = 9)77,78,79,80,81,82,83,84,85. Sixteen interventions described in the articles addressed depression, also in combination with anxiety, ten addressed stress or traumatisation, four substance abuse disorders, and the remaining interventions addressed other mental disorders or a combination of the named ones.
An overview of the study characteristics can be found in Table 1. Details on the interventions used in the studies are illustrated in Supplementary Table 3.
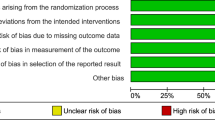
Quality assessment
The initial interrater reliability between the two independent raters was κ = 0.62, which can be considered a substantial agreement86. Overall, the quality of the included articles revealed an average quality score of 75.4%. The assessed quality score ranged from 35.7 (ref. 87) to 95.2% (ref. 63). Nearly all articles provided an explicit theoretical framework (93.9% of the maximum score), named the aims of their conducted or planned study (95.8%), and described their research setting (93.9%) and their procedure for data collection (90.3%) in a satisfactory way. Often, there was only poor evidence of the sample size (40.1%), and users were rarely involved in the study design (42.4%).
Table 1 presents the individual quality score of every article and Supplementary Table 4 contains the comprehensive ratings of the two independent reviewers.
Components of cultural adaptation
Various components of which the authors reported the cultural adaptation were identified across the included articles and grouped in distinguishable aspects of culturally adapting IMI. Using the frameworks of previous literature as a base47,54,74,75,76, the classification had been continuously refined in the course of data synthesis, resulting in ten content, four methodological, and three procedural components that provided qualitative information on the cultural adaptation of IMI for mental disorders. Generally, the consideration of these components was used by the authors to enhance the fit of the IMI to the context, lives, and burdens of the new target group. Across all interventions averaged consideration of content (68.8%) versus methodological (69.0%) versus procedural (66.7%) components was comparable with 68.5% of all components being considered. The 17 components of culturally adapting IMI that were identified across the articles are illustrated in Table 2, including specific adaptation examples of the articles. A more detailed illustration of the conducted adaptations of each IMI can be found in Supplementary Table 5. An overview of the 17 components illustrating the respective extent of consideration across the articles is provided in Fig. 2.

Percentages of the 42 included IMI that fulfilled the respective content, methodological, and procedural components of the taxonomy.
Regarding content components, (1) an important element to adapt were the characters illustrated in the IMI (adapted in 35 of 42 interventions). (2) Alongside the characters, activities were added, removed, or tailored to make them relevant to the target group (25/42 IMI). (3) Furthermore, environments, settings, and, associated with this, specific burdens illustrated in the IMI were adapted (36/42 IMI). (4) Related to these aspects, researchers changed the content to accommodate culturally relevant values and traditions (28/42 IMI). Beside the adaptation of the daily life illustrated in the IMI, language adaptation was considered important: (5) numerous studies translated the entire intervention into the main language or the regional dialect of the target group (35/42 IMI). In addition, language and texts were (6) tailored to the target group (34/42 IMI), and (7) visualised with appropriate quotes, symbols, and metaphors (18/42 IMI). (8) When culturally adapting their IMI, researchers also considered potential differences in the target groups’ concepts of mental health and its treatment (26/42 IMI). Correspondingly, (9) the aims (23/42 IMI) and (10) the used treatment methods in the IMI (27/42 IMI) were changed occasionally.
Regarding methodological components of cultural adaptation, (11) the general structure of IMI was adapted (34/42 IMI). (12) Also, researchers adapted their IMI to enhance its functionality and ease of use for the specific target group (26/42 IMI), e.g., by including interactive elements or simplifying the navigation. (13) Moreover, the design and the aesthetics were adjusted (34/42 IMI). (14) As another aspect of culturally adapting IMI, researchers have changed the format or amount of guidance (22/42 IMI).
With regard to the procedure of cultural adaptation, (15) researchers used a wide range of methods to obtain information about necessary cultural adaptations of their IMI and about the adequacy of the conducted adaptations (32/42 IMI used at least two different methods). (16) During the cultural adaptation process, different people were involved, including healthcare professionals or the target group itself (32/42 IMI involved at least two groups of people). (17) Many authors also based their adaptation process on theoretical frameworks for cultural adaptations of face-to-face therapies (20/42 IMI).
Extent of cultural adaptation
The consideration of each of the 17 components of cultural adaptation of IMI was evaluated across the articles to illustrate the extent of cultural adaptation for each intervention. The points were added up (0–17 points), revealing an average extent of cultural adaptation of M = 11.6 (SD = 3.7), with the smallest extent being three (17.7%)88 and the highest being 17 points (100%)69,89,90,91 for the respective interventions. A list of articles considering the respective components is provided in Table 3.
Adherence and effectiveness of the culturally adapted interventions
Characteristics of those articles providing quantitative data, and their adherence and effectiveness outcomes are illustrated in Table 4, including the measures of the respective non-adapted interventions, if available.
The interventions varied widely in their length (range: 1 (ref. 83)–32 (ref. 92) modules) and duration (range: 1 day83–8 months93). The average percentage of completed sessions of the culturally adapted IMI was 63.7% (CI: 52.3–75.1%, n = 21 interventions), ranging from 20.4% (ref. 94) to 100% (ref. 95). The average percentage of participants who completed all sessions of the adapted IMI was 50.6% (CI: 36.8–64.3%, n = 21 interventions), ranging from 0% (ref. 96) to 100% (ref. 95).
Eight single group studies reported on the effectiveness of their IMI comparing mental disorder symptoms of the participants between pre- and post-treatment assessments, three of which assessed the effectiveness of the same intervention97,98,99. Fourteen (randomised) controlled trials (Chen et al.81 stopped randomisation) reported on the effectiveness of their IMI comparing mental disorder symptoms of the participants who had access to an adapted IMI to those who had no access (control group receiving delayed access, no access, or psychoeducational information). Outcomes of one randomised controlled trial were published in two articles100,101. Primary outcomes varied between the studies, with the Patient Health Questionnaire102 being the scale most used (n = 9), followed by the General Anxiety Disorder Scale103 (n = 4) and the Post-traumatic Disorder Scale104 (n = 3). Similarly, the time between pre- and post-assessments differed between the studies, ranging from 4 weeks96 to 6 months105. Effect sizes of randomised controlled trials ranged from Hedges' g = 0.15 (ref. 100) to 2.70 (ref. 106; see Fig. 3).

Twenty-two included articles provided relevant information on the effect of their intervention. If more than one primary outcome was reported, the effect size of the Patient Health Questionnaire102 is illustrated. Both single group studies and randomised controlled trials are included. Full information on the respective effect sizes can be found in Table 4.
Post hoc analyses
Correlation analyses did not reveal any significant links between the intervention characteristics (amount of modules, provided guidance) and the extent of (specific components of) cultural adaptation, r(40) ≤ 0.12, p ≥ 0.330. The extent of culturally adapting content components significantly differed between the target groups of the IMI (people living in LMIC, in high-income countries, immigrants, indigenous people), F(3,38) = 6.09, p = 0.002, with pairwise comparisons suggesting a lower extent of content cultural adaptation for people from high-income countries, as compared to migrants and people living in LMIC. No link was revealed between the amount of modules, guidance, or extent of cultural adaptation and the effectiveness (r(13) ≤ 0.20, p ≥ 0.487) or adherence of the IMI (r(9) ≤ −0.35, p ≥ 0.287). Nor did the effectiveness (F(2,12) = 0.39, p = 0.683) or adherence (F(2,8) = 0.10, p = 0.909) of the IMI significantly differ between the target groups of the IMI. Detailed results of the post hoc analyses can be found in Supplementary Table 6.
Discussion
This is a systematic review synthesising the components and procedures used in the cultural adaptation of IMI for mental disorders. The proposed taxonomy comprises 17 components, covering the key domains of content (e.g., illustrated daily life and mental health concepts), methodological (e.g., structure and design), and procedural components (e.g., used methods and involved persons).
The 55 articles included in this review explored, conducted, and reported on the cultural adaptation of 42 IMI that were originally used for a culturally differing target group. Cultural adaptations were done to illustrate relatable situations (e.g., persons, activities), to fit the characteristics of the communities (e.g., collectivism, values, traditions), to consider specific risk factors for low mental health (e.g., burdens due to migration, war, discrimination, and low socio-economic status), and to address health-related problems (e.g., low mental health literacy and corresponding distrust, risky behaviour, or limited access to treatment). Twenty-eight studies, including 14 (randomised) controlled trials, evaluated the culturally adapted IMI in terms of adherence and/or effectiveness for the new target group. Adherence rates and effect sizes of randomised controlled trials seem to be comparable to both those found in the studies on the respective original IMI (see Table 4), and those found in studies investigating the adherence and effectiveness of IMI in general36,107. However, enrolment and adherence rates of IMI are generally low108,109,110. Above that, we could not identify any study on a direct comparison of a culturally adapted with a non-adapted IMI. Hence, we believe it is premature to conclude that cultural adaptation is a prerequisite to make IMI work in people living in LMIC, migrants, or indigenous people.
Our taxonomy of cultural adaptation of IMI may provide a base for future researchers to systematically adapt IMI by considering the 17 identified components. The included ten content components overlap with components that are culturally adapted in face-to-face psychological treatments47. Thus, both surface (e.g., the adaptation of characters, activities, and language) and deep (e.g., the adaptation of burdens, values, mental health concepts, and goals and methods of treatment) structure adaptations were shown to be important50. Also, the three procedural components seem to reflect the procedure proposed in the adaptation of face-to-face psychological treatments54. Accordingly, the study investigators used multiple methods to obtain information from various groups of people (e.g., mental health experts, target group) on necessary adaptations of the IMI, including focus groups and feasibility trials. Thereby, about half of the IMI were adapted following theoretical frameworks of cultural adaptation of face-to-face treatments. However, in addition to the content and procedural components, we identified four unique methodological components specifically considered in the cultural adaptation of IMI. These include components related to the structure (e.g., shortened text sequences or modules), functionality (e.g., the consideration of a potentially bad internet connection), design and aesthetics (e.g., the amount or design of pictures), and human guidance (e.g., level of guidance). Hence, it may not be sufficient to rely on existing frameworks for cultural adaptation of face-to-face treatments when culturally adapting IMI, as also highlighted by Lal et al.72 and implemented by Burchert et al.111.
By enabling a systematic cultural adaptation of IMI, our taxonomy on cultural adaptation of IMI can furthermore serve as a base to measure the extent and type of cultural adaptation, and thus can lay an initial foundation for further examining the relevance and necessity of the cultural adaptation of (specific elements of) IMI. This relevance and necessity of cultural adaptation could differ, for example, depending on the target group, the addressed disorder, or the language of the IMI. Conducted exploratory post hoc analyses indicate that culturally adapting IMI for people with a migrant background and people living in LMIC might be more important as compared to culturally adapting IMI for new target groups in western countries, especially with respect to content components. However, in the current systematic review, no link between the extent of the conducted cultural adaptations, and the effectiveness or adherence of the IMI was revealed. The analyses should be interpreted with caution, as the present systematic review included very heterogeneous IMI and did not yield sufficient outcome data. Even with more randomised controlled trials included in meta-analyses, the heterogeneity of interventions studied remains mostly very high, making it difficult to draw conclusions on the influence of specific intervention characteristics or components of cultural adaptation on the effectiveness of the IMI. Thus, questions on possible differences in the necessity of cultural adaptation and its influence on the effectiveness of IMI could be addressed in other study designs. By using randomised factorial trials112,113, different versions of the same IMI that were systematically culturally adapted to varying degrees could be tested against each other. For example, deep structure content components versus surface structure content components versus no content components of an IMI could be culturally adapted. The effectiveness of each of the versions could then be evaluated and compared, herewith enabling to draw conclusions on the benefit of culturally adapting these specific components.
Some limitations of this systematic review need to be considered. First, we excluded studies that did not report (n = 14) or provide details on (n = 6) their cultural adaptation. At the same time, we excluded grey literature with potential unpublished reports on conducted cultural adaptation. This might have led to biased findings and hindered us from drawing conclusions on a potential influence of the (extent of) cultural adaptation of IMI on the adherence or effectiveness of the respective IMI. Second, we also excluded studies that newly developed culturally sensitive IMI for a target group of people living in LMIC, migrants, or indigenous people (n = 32), in contrast to studies that culturally adapted previously used and evaluated IMI. Yet, the 17 components of the taxonomy of cultural adaptation might also be helpful in the development of culturally sensitive IMI. Thus, it may be a fruitful next step to conduct a review on the development of culturally sensitive IMI and compare the results with the current review. Third, the wide range of target groups in our review makes it difficult to interpret the findings across all included target groups. Following the cultural diversity approach114, the necessary extent and depth of culturally adapting IMI may differ between target groups, also depending on the similarities and differences between the original and new target groups. Fourth, although we extracted and summarised aspects of cultural adaptation that the authors have reported to be adapted in order to enhance the cultural fit, we cannot fully rule out that there might have been other reasons (e.g., resources of the researchers and technical innovations). Fifth, the choice of the two cultural adaptation models used as a basis for data extraction47,54 was not based on a systematic approach, but mainly on the frequent use of the models in previous research. Sixth, as the extracted components of cultural adaptation represent differing intensities of adaptation (surface structure adaptations, such as language translation, versus deep structure adaptations, such as the consideration of differences in the concepts of mental health and its treatment), the extent to which the components are considered is not equal to the extensiveness of cultural adaptation. Seventh, reliability regarding data extraction and data synthesis was not evaluated and may thus be limited.
Conclusions
The mental health treatment gap for people in LMIC and for migrants or indigenous people in high-income countries needs to be addressed with innovative and scalable approaches5. To provide impactful interventions, an efficient and systematic cultural adaptation is central24. The present systematic review illustrates a taxonomy of 17 components of culturally adapting IMI, making them more relatable to the new target group by considering their specific context, burdens, and understanding of mental health. This taxonomy can serve as a base for the systematic cultural adaptation of IMI. The next steps should be to investigate the relevance and necessity of a systematic cultural adaptation of IMI, which could help provide adequate and effective mental healthcare to underserved populations, herewith contributing to reduce global public mental health inequalities.
Methods
This systematic review is reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses, the PRISMA guidelines (see Supplementary Table 1 for PRISMA checklist)115. A systematic review protocol has been published116 and registered in the International Prospective Register of Systematic Reviews of the National Institute for Health Research (PROSPERO; registration number: CRD42019142320).
Eligibility criteria
We included (a) peer-reviewed journal articles that reported on an intervention that (b) was primarily provided in an internet-, computer-, app-, or mobile-based setting (with or without human support; pure videoconferencing interventions were excluded), (c) used psychological methods to address mental disorders or disturbances, and (d) was adapted from a previously used and evaluated IMI to fit a new and culturally differing target group. Interventions newly developed for a culturally differing target group were excluded due to assumed differences in the procedure and content of cultural adaptation versus culturally sensitive development of IMI. Psychological interventions were defined according to Kampling et al. and include, among other psychological-oriented interventions, cognitive behaviour therapy, psychodynamic psychotherapy, behaviour therapy or behaviour modification, systemic therapy, third-wave cognitive behaviour therapies, humanistic therapies, and integrative therapies117.
There were no restrictions in the participants’ age nor the language of the articles. Articles were translated to English, if necessary. Furthermore, study protocols were included, if they provided information on the cultural adaptation of the used interventions.
Search strategy
A systematic literature search was conducted on October, 15th 2020 in EbscoHost/Medline, EbscoHost/PsycINFO, Ovid/Embase, Cochrane Central Register of Controlled Trials (CENTRAL), and Web of Science. The search covered two parallel reviews, with the second review including articles on the cultural adaptation of IMI for health promotion118. Keywords of the search term for the present review included a combination of terms and synonyms of (1) internet-based interventions, (2) mental health, and (3) cultural adaptation. The search was complemented by hand search, as well as backward and forward searches. The publication of studies described in an included study protocol was checked before the final data extraction. The full search term can be found in Supplementary Table 2.
Study selection
The selection of articles was conducted in two steps using Covidence119. First, two independent reviewers screened titles and abstracts of all articles against the inclusion criteria. Second, the full-texts of seemingly relevant or ambiguous articles were screened against the inclusion criteria by two independent reviewers. Reasons for exclusion were documented. Disagreement was resolved in discussion, and, if no consensus could be reached, by consulting a third reviewer. The study selection process is illustrated in the PRISMA flow chart (see Fig. 1).
Data extraction
Using a data extraction form in Covidence119, the following information was extracted from the selected articles: (a) study identification items, (b) sample characteristic, (c) study design characteristics, (d) study settings, (e) original intervention characteristics, (f) culturally adapted intervention characteristics, (g) details on content and methodological components of cultural adaptation, (h) details on procedural components of cultural adaptation, as well as (h) primary and secondary outcomes of the studies (adherence and effectiveness). The study authors were contacted if the variables of interest were not available or not clearly presented in the studies. All extracted data was double-checked by an independent reviewer.
Quality assessment
Two independent reviewers assessed the Quality Assessment Tool for Reviewing Studies with Diverse Designs (QATSDD)120. The tool comprises 16 criteria that are applicable to diverse research designs, of which 14 apply to quantitative and to qualitative methods respectively. Thus, the QATSDD enabled an overall quality rating for included quantitative, qualitative, and mixed-methods studies. Beside items assessing completeness and clarity of reporting, further items can help rate the risk of bias of the studies (e.g., fit between stated research question and method of data collection, format and content of data collection tool, or method of analysis; good justification for analytical method selected). The criteria were rated on a four-point scale, producing a global score showing a low or high study quality. The quality score is presented as percentage of the highest possible points. Arising discrepancies between the two reviewers were resolved in discussion; if further needed, a third reviewer was consulted. Cohen’s Kappa was used to assess interrater agreement between low (0 and 1 point) and high (2 and 3 points) study quality121.
Data synthesis
A qualitative synthesis of all included articles was conducted to describe the characteristics and findings of the studies. To answer the research questions, details on the cultural adaptation reported in the included studies were summarised and classified; only adaptations that the authors reported to have been made for cultural reasons were considered. The classification included content components, based on Bernal et al.47, methodological components, based on IMI evaluation frameworks74,75,76, and procedural components, based on Barrera and Castro54. We additionally rated which of the extracted components were culturally adapted versus not adapted in which intervention (one versus zero point), so to provide descriptive cultural adaptation scores to illustrate the extent of the conducted cultural adaptation for each of the interventions, and each of the components.
Findings related to the adherence to and the effectiveness of the culturally adapted IMI for mental disorders were summarised and descriptively illustrated. Adherence was evaluated using the percentage of completed modules (average number of completed modules divided by the number of all modules of the IMI). In addition, the percentage of study participants who completed all modules of the IMI was illustrated. The effectiveness of the intervention was evaluated using the effect size Hedges’ g122. In case of conducted randomised controlled trials, the effect size was calculated for the mean differences in the primary outcome(s) of the intervention and control groups at post-treatment assessments. In case of single group study designs, the effect size was calculated for the mean differences in the primary outcome(s) between pre- and post-treatment assessments. If available, adherence and effectiveness outcomes of the original IMI were illustrated in comparison to those of the culturally adapted IMI.
Post hoc analyses
To exploratively investigate intervention characteristics that might influence the conducted cultural adaptation and the effectiveness and adherence of the adapted IMI, we conducted post hoc analyses. First, potential links between intervention characteristics (duration, provided guidance, and target group of the IMI) and the extent of cultural adaptation or the extent of specific components of cultural adaptation (content, methodological, and procedural) were analysed using Pearson’s correlation coefficients and an analysis of variance. Second, potential links between intervention characteristics or the extent of cultural adaptation and the effectiveness or the adherence (percentage of completers) of the interventions were analysed also using Pearson’s correlation coefficients or analyses of variance. Due to the explorative character of the analyses, no adjustments for multiple comparisons were applied.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
World Health Organization. Mental health action plan 2013-2020 https://www.who.int/publications/i/item/9789241506021 (2013).
Braveman, P. Health disparities and health equity: concepts and measurement. Annu. Rev. Public Health 27, 167–194 (2005).
Fiscella, K., Franks, P., Gold, M. R. & Clancy, C. M. Inequality in quality: addressing socioeconomic, racial, and ethnic disparities in health care. JAMA 283, 2579–2584 (2003).
Goesling, B. & Firebaugh, G. The trend in international health inequality. Popul. Dev. Rev. 30, 131–146 (2004).
Patel, V. et al. The Lancet Commission on global mental health and sustainable development. Lancet Comm. 392, 1553–1598 (2018).
World Health Organization. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization world mental health surveys. J. Am. Med. Assoc. 291, 2581–2590 (2004).
Patel, V. Mental health in low- and middle-income countries. Br. Med. Bull. 81–82, 81–96 (2007).
Lamkaddem, M. et al. Course of post-traumatic stress disorder and health care utilisation among resettled refugees in the Netherlands. BMC Psychiatry 14, 90–97 (2014).
Laban, C. J., Gernaat, H. B. P. E., Komproe, I. H. & Jong, J. T. V. M. Prevalence and predictors of health service use among Iraqi asylum seekers in the Netherlands. Soc. Psychiatry Psychiatr. Epidemiol. 42, 837–844 (2007).
Slewa-Younan, S. et al. The mental health and help-seeking behaviour of resettled Afghan refugees in Australia. Int. J. Ment. Health Syst. 11, 49 (2017).
Steel, J. L., Dunlavy, A. C., Harding, C. E. & Theorell, T. The psychological consequences of pre-emigration trauma and post-migration stress in refugees and immigrants from. Afr. J. Immigr. Minor. Heal. 19, 523–532 (2017).
Turrini, G. et al. Common mental disorders in asylum seekers and refugees: umbrella review of prevalence and intervention studies. Int. J. Ment. Health Syst. 11, 51 (2017).
Fazel, M., Wheeler, J. & Danesh, J. Prevalence of serious mental disorder in 7000 refugees resettled in western countries: a systematic review. Lancet 365, 1309–1314 (2005).
Lindert, J., Carta, M. G., Schäfer, I. & Mollica, R. F. Refugees mental health - a public mental health challenge. Eur. J. Public Health 26, 374–375 (2016).
Kirmayer, L. J., Brass, G. M. & Tait, C. L. The mental health of aboriginal peoples: transformations of identity and community. Can. J. Psychiatry 45, 607–616 (2000).
Nelson, S. E. & Wilson, K. The mental health of Indigenous peoples in Canada: a critical review of research. Soc. Sci. Med. 176, 93–112 (2017).
Marrone, S. Understanding barriers to health care: a review of disparities in health care services among indigenous populations. Int. J. Circumpolar Health 66, 188–198 (2007).
Eaton, J. et al. Scale up of services for mental health in low-income and middle-income countries. Lancet 378, 1592–1603 (2011).
Patel, V., Chowdhary, N., Rahman, A. & Verdeli, H. Improving access to psychological treatments: lessons from developing countries. Behav. Res. Ther. 49, 523–528 (2011).
Kiselev, N. et al. Structural and socio-cultural barriers to accessing mental healthcare among Syrian refugees and asylum seekers in Switzerland. Eur. J. Psychotraumatol. 11, 1717825 (2020).
Byrow, Y., Pajak, R., Specker, P. & Nickerson, A. Perceptions of mental health and perceived barriers to mental health help-seeking amongst refugees: a systematic review. Clin. Psychol. Rev. 75, 101812 (2020).
Sijbrandij, M. et al. Strengthening mental health care systems for Syrian refugees in Europe and the Middle East: integrating scalable psychological interventions in eight countries. Eur. J. Psychotraumatol. 8, 1388102 (2017).
Trilesnik, B. et al. Implementing a need-adapted stepped-care model for mental health of refugees: preliminary data of the state-funded project ‘Refukey’. Front. Psychiatry 10, 688 (2019).
Holmes, E. A. et al. The Lancet Psychiatry Commission on psychological treatments research in tomorrow’s science. Lancet Psychiatry 5, 237–286 (2018).
Bockting, C. L. H., Williams, A. D., Carswell, K. & Grech, A. E. The potential of low-intensity and online interventions for depression in low- and middle-income countries. Glob. Ment. Heal 3, e25 (2016).
Bennett-Levy, J., Richards, D. A. & Farrand, P. in Oxford Guide to Low Intensity CBT Interventions (eds Bennett-Levy, J. et al.) 3–18 (Oxford University Press, 2010).
Griffiths, F., Lindenmeyer, A., Powell, J., Lowe, P. & Thorogood, M. Why are health care interventions delivered over the Internet? A systematic review of the published literature. J. Med. Internet Res. 8, e10 (2006).
Carroll, K. M. & Rounsaville, B. J. Computer-assisted therapy in psychiatry: be brave - it’s a new world. Curr. Psychiatry Rep. 12, 426–432 (2010).
Moock, J. Support from the Internet for individuals with mental disorders: advantages and disadvantages of e-mental health service delivery. Front. Public Health 2, 65–70 (2014).
Andersson, G. & Titov, N. Advantages and limitations of Internet-based interventions for common mental disorders. World Psychiatry 13, 4–11 (2014).
Muñoz, R. F. et al. Massive open online interventions: a novel model for delivering behavioral- health services worldwide. Clin. Psychol. Sci. 4, 194–205 (2016).
Mohr, D. C., Schueller, S. M., Araya, R., Gureje, O. & Montague, E. Mental health technologies and the needs of cultural groups. Lancet Psychiatry 1, 326–327 (2014).
Waller, R. & Gilbody, S. Barriers to the uptake of computerized cognitive behavioural therapy: a systematic review of the quantitative and qualitative evidence. Psychol. Med. 39, 705–712 (2009).
Sander, L., Rausch, L. & Baumeister, H. Effectiveness of internet-based interventions for the prevention of mental disorders: a systematic review and meta-analysis. JMIR Ment. Heal 3, e38 (2016).
Andersson, G., Titov, N., Dear, B. F., Rozental, A. & Carlbring, P. Internet-delivered psychological treatments: from innovation to implementation. World Psychiatry 18, 20–28 (2019).
Karyotaki, E. et al. Internet-based cognitive behavioral therapy for depression: a systematic review and individual patient data network meta-analysis. JAMA Psychiatry 78, 361–371 (2021).
Weisel, K. K. et al. Standalone smartphone apps for mental health—a systematic review and meta-analysis. npj Digit. Med. 2, 1–10 (2019).
Rigabert, A. et al. Effectiveness of online psychological and psychoeducational interventions to prevent depression: systematic review and meta-analysis of randomized controlled trials. Clin. Psychol. Rev. 82, 101931 (2020).
Karyotaki, E. et al. Do guided internet-based interventions result in clinically relevant changes for patients with depression? An individual participant data meta-analysis. Clin. Psychol. Rev. 63, 80–92 (2018).
Saraceno, B. et al. Barriers to improvement of mental health services in low-income and middle-income countries. Lancet 370, 1164–1174 (2007).
Zayas, L. H., Torres, L. R., Malcolm, J. & DesRosiers, F. S. Clinicians’ definitions of ethnically sensitive therapy. Prof. Psychol. Res. Pr. 27, 78–82 (1996).
Gearing, R. E. et al. Adaptation and translation of mental health interventions in Middle Eastern Arab countries: a systematic review of barriers to and strategies for effective treatment implementation. Int. J. Soc. Psychiatry 59, 671–681 (2013).
Sue, S., Zane, N., Nagayama Hall, G. C. & Berger, L. K. The case for cultural competency in psychotherapeutic interventions. Annu. Rev. Psychol. 60, 525–548 (2009).
Castro, F. G., Barrera, M. & Steiker, L. K. H. Issues and challenges in the design of culturally adapted evidence-based interventions. Annu. Rev. Clin. Psychol. 6, 213–239 (2010).
Sangraula, M. et al. Development of the mental health cultural adaptation and contextualization for implementation (mhCACI) procedure: a systematic framework to prepare evidence-based psychological interventions for scaling. Glob. Ment. Health 8, e6 (2021).
Chu, J. & Leino, A. Advancement in the maturing science of cultural adaptations of evidence-based interventions. J. Consult. Clin. Psychol. 85, 45–57 (2017).
Bernal, G., Bonilla, J. & Bellido, C. Ecological validity and cultural sensitivity for outcome research - issues for the cultural-adaptation and development of psychosocial treatments with hispanics. J. Abnorm. Child Psychol. 23, 67–82 (1995).
Rathod, S., Phiri, P. & Naeem, F. An evidence-based framework to culturally adapt cognitive behaviour therapy. Cogn. Behav. Ther. 12, e10 (2019).
Hwang, W. C. The psychotherapy adaptation and modification framework: application to Asian Americans. Am. Psychol. 61, 702–715 (2006).
Resnicow, K., Baranowski, T., Ahluwalia, J. S. & Braithwaite, R. Cultural sensitivity in public health: defined and demystified. Ethn. Dis. 9, 10–21 (1999).
Hinton, D. E. & Jalal, B. Guidelines for the implementation of culturally sensitive cognitive behavioural therapy among refugees and in global contexts. Intervention 12, 78–93 (2014).
Heim, E. & Kohrt, B. A. Cultural adaptation of scalable psychological interventions: a new conceptual framework. Clin. Psychol. Eur. 1, e37679 (2019).
Hwang, W. C. The formative method for adapting psychotherapy (FMAP): a community-based developmental approach to culturally adapting therapy. Prof. Psychol. Res. Pr. 40, 369–377 (2009).
Barrera, M. & Castro, F. G. A heuristic framework for the cultural adaptation of interventions. Clin. Psychol. Sci. Pract. 13, 311–316 (2006).
Benish, S. G., Quintana, S. & Wampold, B. E. Culturally adapted psychotherapy and the legitimacy of myth: a direct-comparison meta-analysis. J. Couns. Psychol. 58, 279–289 (2011).
Hall, G. C. N., Ibaraki, A. Y., Huang, E. R., Marti, C. N. & Stice, E. A meta-analysis of cultural adaptations of psychological interventions. Behav. Ther. 47, 993–1014 (2016).
Smith, T. B., Domenech Rodríguez, M. & Bernal, G. Culture. J. Clin. Psychol. 67, 166–175 (2011).
Soto, A., Smith, T. B., Griner, D., Rodríguez, M. D. & Bernal, G. Cultural adaptations and therapist multicultural competence: two meta‐analytic reviews. J. Clin. Psychol. 74, 1907–1923 (2018).
Harper Shehadeh, M. J., Heim, E., Chowdhary, N., Maercker, A. & Albanese, E. Cultural adaptation of minimally guided interventions for common mental disorders: a systematic review and meta-analysis. JMIR Ment. Health 3, e44 (2016).
Sijbrandij, M. Expanding the evidence: key priorities for research on mental health interventions for refugees in high-income countries. Epidemiol. Psychiatr. Sci. 27, 105–108 (2017).
Knaevelsrud, C., Brand, J., Lange, A., Ruwaard, J. & Wagner, B. Web-based psychotherapy for posttraumatic stress disorder in war-traumatized Arab patients: randomized controlled trial. J. Med. Internet Res. 17, e71 (2015).
Arjadi, R. et al. Internet-based behavioural activation with lay counsellor support versus online minimal psychoeducation without support for treatment of depression: a randomised controlled trial in Indonesia. Lancet Psychiatry 5, 707–716 (2018).
Lindegaard, T. et al. Internet-based cognitive behavioural therapy for depression and anxiety among Arabic-speaking individuals in Sweden: a pilot randomized controlled trial. Cogn. Behav. Ther. 50, 47–66 (2020).
Heim, E. et al. Effect of cultural adaptation of a smartphone-based self-help programme on its acceptability and efficacy: study protocol for a randomized controlled trial. PsychArchives https://doi.org/10.23668/PSYCHARCHIVES.3152 (2020).
Fu, Z., Burger, H., Arjadi, R. & Bockting, C. L. H. Effectiveness of digital psychological interventions for mental health problems in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Psychiatry 7, 851–864 (2020).
Ramos, G. & Chavira, D. A. Use of technology to provide mental health care for racial and ethnic minorities: evidence, promise, and challenges. Cogn. Behav. Pract. https://doi.org/10.1016/j.cbpra.2019.10.004 (2019).
Escoffery, C. et al. A systematic review of adaptations of evidence-based public health interventions globally. Implement. Sci. 13, 125–136 (2018).
Stirman, S. W., Baumann, A. A. & Miller, C. J. The FRAME: an expanded framework for reporting adaptations and modifications to evidence-based interventions. Implement. Sci. 14, 58 (2019).
Abi Ramia, J. et al. Community cognitive interviewing to inform local adaptations of an e-mental health intervention in Lebanon. Glob. Ment. Health 5, e39 (2018).
Arjadi, R., Nauta, M. H., Suryani, A. O. & Bockting, C. L. H. Guided Act and Feel Indonesia - Internet-based behavioral activation intervention for depression in Indonesia: a systematic cultural adaptation. Makara Hubs-Asia 22, 3–11 (2018).
Juniar, D. et al. Web-based stress management program for university students in Indonesia: systematic cultural adaptation and protocol for a feasibility study. JMIR Res. Protoc. 8, e11493 (2019).
Lal, S. et al. Cultural and contextual adaptation of an ehealth intervention for youth receiving services for first-episode psychosis: adaptation framework and protocol for Horyzons-Canada phase 1. JMIR Res. Protoc. 20, e100 (2018).
Salamanca-Sanabria, A., Richards, D. & Timulak, L. Adapting an internet-delivered intervention for depression for a Colombian college student population: an illustration of an integrative empirical approach. Internet Inter. 15, 76–86 (2019).
Stoyanov, S. R. et al. Mobile App Rating Scale: a new tool for assessing the quality of health mobile apps. JMIR mHealth uHealth 3, e27 (2015).
Baumel, A., Faber, K., Mathur, N., Kane, J. M. & Muench, F. Enlight: a comprehensive quality and therapeutic potential evaluation tool for mobile and web-based eHealth interventions. J. Med. Internet Res. 19, e82 (2017).
Kim, P., Eng, T. R., Deering, M. J. & Maxfield, A. Review of published criteria for evaluating health-related websites. West. J. Med. 170, 329–332 (1999).
Titov, N., Schofield, C., Staples, L., Dear, B. F. & Nielssen, O. A comparison of Indigenous and non-Indigenous users of MindSpot: an Australian digital mental health service. Australas. Psychiatry 27, 352–357 (2018).
Bolinski, F. et al. Effectiveness of a transdiagnostic individually tailored Internet-based and mobile-supported intervention for the indicated prevention of depression and anxiety (ICare Prevent) in Dutch college students: study protocol for a randomised controlled trial. Trials 19, 1–13 (2018).
Rahmadiana, M. et al. Guided internet-based transdiagnostic intervention for Indonesian university students with symptoms of anxiety and depression: a pilot study protocol. Internet Inter. 15, 28–34 (2019).
Imamura, K. et al. Effects of two types of smartphone-based stress management programmes on depressive and anxiety symptoms among hospital nurses in Vietnam: a protocol for three-arm randomised controlled trial. BMJ Open 9, e025138 (2019).
Chen, H. et al. Predictors of treatment outcomes and adherence in internet-based cognitive behavioral therapy for social anxiety in China. Behav. Cogn. Psychother. 48, 291–303 (2020).
Kaal, E. et al. Testing the efficacy of a minimal-guidance online self-help intervention for alcohol misuse in Estonia: study protocol of a randomized controlled trial. BMC Public Health 20, 790 (2020).
Wasil, A. R. et al. Harnessing single-session interventions to improve adolescent mental health and well-being in India: development, adaptation, and pilot testing of online single-session interventions in Indian secondary schools. Asian J. Psychiatr. 50, 101980 (2020).
Okujava, N. et al. Digital cognitive behavioral therapy for insomnia – The first Georgian version. Can we use it practice?. Internet Interv. 17, 100244 (2019).
Yokomitsu, K. et al. Gamified mobile computerized cognitive behavioral therapy for Japanese university students with depressive symptoms: protocol for a randomized controlled trial. JMIR Res. Protoc. 9, 1–10 (2020).
Landis, J. R. & Koch, G. G. The measurement of observer agreement for categorical data. Biometrics 33, 159–174 (1977).
Brooks, L. A., Bloomer, M. J. & Manias, E. Culturally sensitive communication at the end-of-life in the intensive care unit: a systematic review. Aust. Crit. Care 32, 516–523 (2019).
Wang, Z., Wang, J. & Maercker, A. Chinese My Trauma Recovery, a web-based intervention for traumatized persons in two parallel samples: randomized controlled trial. J. Med. Internet Res. 15, 112–125 (2013).
Harper Shehadeh, M. J. et al. Step-by-Step, an e-mental health intervention for depression: a mixed methods pilot study from Lebanon. Front. Psychiatry 10, 986 (2020).
Shala, M. et al. Cultural adaptation of Hap-pas-Hapi, an internet and mobile-based intervention for the treatment of psychological distress among Albanian migrants in Switzerland and Germany. Internet Inter. 21, 100339 (2020).
Spanhel, K. et al. Cultural adaptation of internet interventions for refugees: results from a user experience study in Germany. Internet Inter. 18, 100252 (2019).
Campbell, A. N. C. et al. Acceptability of a web-based community reinforcement approach for substance use disorders with treatment-seeking American Indians/Alaska Natives. Community Ment. Health J. 51, 393–403 (2015).
Ip, P. et al. Effectiveness of a culturally attuned Internet-based depression prevention program for Chinese adolescents: a randomized controlled trial. Depress Anxiety 33, 1123–1131 (2016).
Ünlü Ince, B. et al. Internet-based, culturally sensitive, problem-solving therapy for Turkish migrants with depression: randomized controlled trial. J. Med. Internet Res. 15, e227 (2013).
Wagner, B., Schulz, W. & Knaevelsrud, C. Efficacy of an Internet-based intervention for posttraumatic stress disorder in Iraq: a pilot study. Psychiatry Res. 195, 85–88 (2012).
Kanuri, N. et al. Examining the initial usability, acceptability and feasibility of a digital mental health intervention for college students in India. Int. J. Psychol. 55, 657–673 (2020).
Kayrouz, R. et al. A feasibility open trial of guided Internet-delivered cognitive behavioural therapy for anxiety and depression amongst Arab Australians. Internet Inter. 2, 32–38 (2015).
Kayrouz, R., Dear, B. F., Karin, E., Fogliati, V. J. & Titov, N. A pilot study of a clinician-guided internet-delivered cognitive behavioural therapy for anxiety and depression among Arabs in Australia, presented in both English and Arabic languages. Internet Inter. 5, 5–11 (2016).
Kayrouz, R. et al. A pilot study of self-guided internet-delivered cognitive behavioural therapy for anxiety and depression among Arabs. Internet Inter. 3, 18–24 (2016).
Paris, M. et al. Culturally adapted, web-based cognitive behavioral therapy for Spanish-speaking individuals with substance use disorders: a randomized clinical trial. Am. J. Public Health 108, 1535–1542 (2018).
Silva, M. A. et al. Changes in DSM criteria following a culturally-adapted computerized CBT for Spanish-speaking individuals with substance use disorders. J. Subst. Abus. Treat. 110, 42–48 (2020).
Spitzer, R. L., Kroenke, K. & Williams, J. B. W. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. JAMA 282, 1737–1744 (1999).
Spitzer, R. L., Kroenke, K., Williams, J. B. W. & Löwe, B. A brief measure for assessing generalized anxiety disorder. Arch. Intern. Med. 166, 1092–1097 (2006).
Foa, E. B., Cashman, L., Jaycox, L. & Perry, K. The validation of a self-report measure of posttraumatic stress disorder: The Posttraumatic Diagnostic Scale. Psychol. Assess. 9, 445–451 (1997).
Muroff, J. et al. An outcome study of the CASA-CHESS smartphone relapse prevention tool for Latinx Spanish-speakers with substance use disorders. Subst. Use Misuse 54, 1438–1449 (2019).
Lin, L. Y. et al. An internet-based intervention for individuals with social anxiety and different levels of Taijin Kyofusho in China. J. Cross Cult. Psychol. 51, 387–402 (2020).
Kelders, S. M., Kok, R. N., Ossebaard, H. C. & Van Gemert-Pijnen, J. E. W. C. Persuasive system design does matter: a systematic review of adherence to web-based interventions. J. Med. Internet Res. 14, e152 (2012).
Baumel, A., Muench, F., Edan, S. & Kane, J. M. Objective user engagement with mental health apps: aystematic search and panel-based usage analysis. J. Med. Internet Res. 21, e14567 (2019).
Van Ballegooijen, W. et al. Adherence to internet-based and face-to-face cognitive behavioural therapy for depression: a meta-analysis. PLoS ONE 9, e100674 (2014).
Simon, N. et al. Acceptability of internet-based cognitive behavioural therapy (i-CBT) for post-traumatic stress disorder (PTSD): a systematic review. Eur. J. Psychotraumatol. 10, 1646092 (2019).
Burchert, S. et al. User-centered app adaptation of a low-intensity e-mental health intervention for Syrian refugees. Front. Psychiatry 9, 663 (2019).
Watkins, E. R. & Newbold, A. Factorial designs help to understand how psychological therapy works. Front. Psychiatry 11, 429 (2020).
Collins, L. M. Optimization of Behavioral, Biobehavioral, and Biomedical Interventions: the Multiphase Optimization Strategy (MOST) (Springer International Publishing, 2018).
von Lersner, U. & Kizilhan, J. I. Kultursensitive Psychotherapie [Culture-sensitive psychotherapy]. Fortschritte der Psychotherapie - Band 64 (Hogrefe, 2017).
Liberati, A. et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J. Clin. Epidemiol. 62, e1000100 (2009).
Spanhel, K., Balci, S., Baumeister, H., Bengel, J. & Sander, L. B. Cultural adaptation of Internet- and mobile-based interventions for mental disorders: a systematic review protocol. Syst. Rev. 9, 207 (2020).
Kampling, H., Baumeister, H., Jackel, W. H. & Mittag, O. Prevention of depression in chronically physically ill adults. Cochrane Database Syst. Rev. 3, CD011246 (2014).
Balci, S., Spanhel, K., Sander, L. B. & Baumeister, H. Protocol for a systematic review and meta-analysis of culturally adapted internet- and mobile-based health promotion interventions. BMJ Open 10, e037698 (2020).
Covidence. Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org.
Sirriyeh, R., Lawton, R., Gardner, P. & Armitage, G. Reviewing studies with diverse designs: the development and evaluation of a new tool. J. Eval. Clin. Pract. 18, 746–752 (2012).
Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 20, 37–46 (1960).
Hedges, L. & Olkin, I. Statistical Methods for Meta-analysis (Academic Press, 1985).
Abuwalla, Z. et al. Proposed model for the cultural adaptation of an Internet-based depression prevention intervention (CATCH-IT) for Arab adolescents. Int. J. Adolesc. Med. Health 31, 1–24 (2017).
Arjadi, R., Nauta, M. H. & Bockting, C. L. H. Acceptability of internet-based interventions for depression in Indonesia. Internet Inter. 13, 8–15 (2018).
Choi, I. et al. Culturally attuned internet treatment for depression amongst Chinese Australians: a randomised controlled trial. J. Affect. Disord. 136, 459–468 (2012).
Daponte, D. et al. Facilitating the dissemination of iCBT for the treatment of anxiety and depression: a feasibility study. Behav. Chang 35, 139–151 (2018).
Eylem, O. et al. Reducing suicidal ideation among Turkish migrants in the Netherlands and in the UK: the feasibility of a randomised controlled trial of a guided online intervention. Pilot Feasibility Stud. 7, 30 (2021).
Garabiles, M. R., Harper Shehadeh, M. & Hall, B. J. Cultural adaptation of a scalable World Health Organization e-mental health program for overseas Filipino workers. JMIR Form. Res. 3, e11600 (2019).
Gorman, J. R. et al. Creating a culturally appropriate web-based behavioral intervention for American Indian/ Alaska native women in Southern California: the healthy women healthy native nation study. Am. Indian Alsk. Nativ. Ment. Health Res. 20, 1–15 (2013).
Hiratsuka, V. Y. et al. An internet-based therapeutic tool for American Indian/Alaska native adults with posttraumatic stress disorder: user testing and developmental feasibility study. J. Med. Internet Res. 3, e13682 (2019).
Lal, S. et al. Adaptation of a digital health innovation to prevent relapse and support recovery in youth receiving services for first-episode psychosis: results from the Horyzons-Canada phase 1 study. JMIR Form. Res 4, e19887 (2020).
Luo, Y. J., Jackson, T., Stice, E. & Chen, H. Effectiveness of an internet dissonance-based eating disorder prevention intervention among body-dissatisfied young Chinese women. Behav. Ther. 52, 221–233 (2021).
Muroff, J. et al. Use of a smartphone recovery tool for Latinos with co-occurring alcohol and other drug disorders and mental disorders. J. Dual Diagn. 13, 280–290 (2017).
Nygren, T., Berg, M., Sarkohi, A. & Andersson, G. Development of an Internet-based cognitive behavioral therapy self-help program for arabic-speaking immigrants: mixed-methods study. JMIR Res. Protoc. 7, e11872 (2018).
Nygren, T. et al. Internet-based treatment of depressive symptoms in a Kurdish population: a randomized controlled trial. J. Clin. Psychol. 75, 985–998 (2019).
Patel, U. et al. Cultural considerations for the adaptation of an Internet-based intervention for depression prevention in Mainland China. Int. J. Adolesc. Med. Health 29, 20150099 (2017).
Pinto-Bruno, Á. C., Pot, A. M., Kleiboer, A., Droes, R.-M. & van Straten, A. An online minimally guided intervention to support family and other unpaid carers of people with dementia: protocol for a randomized controlled trial. JMIR Res. Protoc. 8, e14106 (2019).
Salamanca-Sanabria, A. et al. A culturally adapted cognitive behavioral internet-delivered intervention for depressive symptoms: randomized controlled trial. JMIR Ment. Health 7, e13392 (2020).
Saulsberry, A. et al. Chicago urban resiliency building (CURB): an internet-based depression-prevention intervention for urban African-American and Latino adolescents. J. Child Fam. Stud. 22, 150–160 (2013).
Silva, M. A. et al. Computer-based training for cognitive behavioral therapy for Spanish-speaking substance users: adaptation and satisfaction (unpublished).
Sit, H. F. et al. The cultural adaptation of Step-by-Step: an intervention to address depression among Chinese young adults. Front. Psychiatry 11, 650 (2020).
Sobowale, K. et al. Adaptation of an internet-based depression prevention intervention for Chinese adolescents: from ‘ CATCH-IT’ to ‘grasp the opportunity. Int. J. Adolesc. Med. Health 25, 127–137 (2013).
Teles, S., Napolskij, M. S., Paúl, C., Ferreira, A. & Seeher, K. Training and support for caregivers of people with dementia: The process of culturally adapting the World Health Organization iSupport programme to Portugal. Dementia https://doi.org/10.1177/1471301220910333 (2020).
Vöhringer, M. et al. Should I stay or must I go? Predictors of dropout in an internet-based psychotherapy programme for posttraumatic stress disorder in Arabic. Eur. J. Psychotraumatol. 11, 1706297 (2020).
Kishimoto, T. et al. Internet-based cognitive behavioral therapy for social anxiety with and without guidance compared to a wait list in China: a Propensity Score Study. Psychother. Psychosom. 85, 317–319 (2016).
Berger, T., Hohl, E. & Caspar, F. Internet‐based treatment for social phobia: a randomized controlled trial. J. Clin. Psychol. 65, 1021–1035 (2009).
Perini, S., Titov, N. & Andrews, G. Clinician-assisted Internet-based treatment is effective for depression: randomized controlled trial. Aust. N. Z. J. Psychiatry 43, 571–578 (2009).
Titov, N. et al. Transdiagnostic internet treatment for anxiety and depression: a randomised controlled trial. Behav. Res. Ther. 49, 441–452 (2011).
Van Spijker, B. A. J., Van Straten, A. & Kerkhof, A. J. F. M. Effectiveness of online self-help for suicidal thoughts: results of a randomised controlled trial. PLoS ONE 9, e90118 (2014).
Kuhn, E. et al. A randomized controlled trial of a smartphone app for posttraumatic stress disorder symptoms. J. Consult. Clin. Psychol. 85, 267–273 (2017).
Voorhees, B. W. Van et al. Randomized clinical trial of an Internet-based depression prevention program for adolescents (Project CATCH-IT) in primary care: twelve-week outcomes. J. Dev. Behav. Pediatr. 30, 23–37 (2009).
Lange, A. et al. Interapy: a controlled randomized trial of the standardized treatment of posttraumatic stress through the internet. J. Consult. Clin. Psychol. 71, 901–909 (2003).
Stice, E., Rohde, P., Durant, S. & Shaw, H. A preliminary trial of a prototype internet dissonance-based eating disorder prevention program for young women with body image concerns. J. Consult. Clin. Psychol. 80, 907–916 (2012).
McTavish, F. M., Chih, M. Y., Shah, D. & Gustafson, D. H. How patients recovering from alcoholism use a smartphone intervention. J. Dual Diagn. 8, 294–304 (2008).
Andersson, G. et al. Internet-based self-help for depression: randomised controlled trial. Br. J. Psychiatry 187, 456–461 (2005).
Van Straten, A. et al. Guided Internet-delivered cognitive behavioural treatment for insomnia: a randomized trial. Psychol. Med. 44, 1521–1532 (2014).
Kiluk, B. D. et al. Randomized trial of computerized cognitive behavioral therapy for alcohol use disorders: efficacy as a virtual stand-alone and treatment add-on compared with standard outpatient treatment. Alcohol. Clin. Exp. Res. 40, 1991–2000 (2016).
Richards, D. et al. A randomized controlled trial of an internet-delivered treatment: its potential as a low-intensity community intervention for adults with symptoms of depression. Behav. Res. Ther. 75, 20–31 (2015).
Van Straten, A., Cuijpers, P. & Smits, N. Effectiveness of a web-based self-help intervention for symptoms of depression, anxiety, and stress: randomized controlled trial. J. Med. Internet Res. 10, 1–11 (2008).
Steinmetz, S. E., Benight, C. C., Bishop, S. L. & James, L. E. My Disaster Recovery: a pilot randomized controlled trial of an Internet intervention. Anxiety, Stress Coping 25, 593–600 (2012).
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J. & Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 4, 561–571 (1961).
Beck, A. T., Steer, R. A. & Ranieri, W. F. Scale for suicide ideation: psychometric properties of a self‐report version. J. Clin. Psychol. 4, 499–505 (1988).
Weathers, F. W., Litz, B. T., Herman, D. S., Huska, J. A. & Keane, T. M. The PTSD Checklist (PCL): reliability, validity,and diagnostic utility. Paper presented at the Annual convention of the international society for traumatic stress studies, San Antonio, TX, October (1993).
Radloff, L. S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1, 385–401 (1977).
Horowitz, M., Wilner, N. & Alvarez, W. Impact of Event Scale: a measure of subjective stress. Psychosom. Med. 41, 209–218 (1979).
Mattick, R. P. & Clarke, J. C. Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behav. Res. Ther. 36, 455–470 (1998).
Stice, E., Fisher, M. & Martinez, E. Eating Disorder Diagnostic Scale: additional evidence of reliability and validity. Psychol. Assess. 16, 60–71 (2004).
Kessler, F. et al. Psychometric properties of the sixth version of the Addiction Severity Index (ASI-6) in Brazil. Rev. Bras. Psiquiatr. 34, 24–33 (2012).
Bastien, C. H., Valliéres, A. & Morin, C. M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep. Med. 2, 297–307 (2001).
Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R. & Kupfer, D. J. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 28, 193–213 (1989).
Kessler, R. C. et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 32, 959–976 (2002).
Acknowledgements
The authors wish to thank all contacted authors who provided missing information. K.S. is supported by the German Academic Scholarship Foundation, and S.B. receives a scholarship granted by the Ministry of Education in Turkey. Open Access funding was provided by Projekt DEAL. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
K.S., S.B., J.B., H.B., and L.B.S. conceived the study design. K.S. is the guarantor of the review. K.S., S.B., F.F., and L.B.S. developed the search strategy, K.S., S.B., and F.F. conducted the search, and made the inclusion decisions and the quality assessment. J.B., H.B., and L.B.S. provided methodological expertise. K.S. and F.F. wrote the draft of the manuscript; S.B., J.B., H.B., and L.B.S. revised the work. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
K.S., S.B., F.F., and J.B. declare that they have no competing interests. H.B. received consultancy fees, reimbursement of congress attendance, and travel costs as well as payments for lectures from Psychotherapy and Psychiatry Associations, as well as Psychotherapy Training Institutes in the context of E-Mental-Health topics. He has been the beneficiary of study support (third-party funding) from several public funding organisations. L.B.S. received personal fees from Psychotherapy Training Institutes and clinics in the context of E-Mental-Health topics and supervision outside the submitted work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Spanhel, K., Balci, S., Feldhahn, F. et al. Cultural adaptation of internet- and mobile-based interventions for mental disorders: a systematic review. npj Digit. Med. 4, 128 (2021). https://doi.org/10.1038/s41746-021-00498-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41746-021-00498-1
This article is cited by
-
Culturally adapted Turkish version of an internet-based mindfulness intervention for university students: a randomized controlled feasibility trial
BMC Digital Health (2024)
-
Needs for mobile and internet-based psychological intervention in patients with self-injury and suicide-related behaviors: a qualitative systematic review
BMC Psychiatry (2024)
-
Digital tools to support mental health: a survey study in psychosis
BMC Psychiatry (2023)
-
Examining equity in access and utilization of a freely available meditation app
npj Mental Health Research (2023)
-
Access to Virtual Mental Healthcare and Support for Refugee and Immigrant Groups: A Scoping Review
Journal of Immigrant and Minority Health (2023)
