
Abstract
Air pollution is high on the global agenda and is widely recognised as a threat to both public health and economic progress. The World Health Organization (WHO) estimates that 4.2 million deaths annually can be attributed to outdoor air pollution. Recently, there have been major advances in methods that allow the quantification of air pollution-related indicators to track progress towards the Sustainable Development Goals and that expand the evidence base of the impacts of air pollution on health. Despite efforts to reduce air pollution in many countries there are regions, notably Central and Southern Asia and Sub-Saharan Africa, in which populations continue to be exposed to increasing levels of air pollution. The majority of the world’s population continue to be exposed to levels of air pollution substantially above WHO Air Quality Guidelines and, as such, air pollution constitutes a major, and in many areas, increasing threat to public health.
Similar content being viewed by others

Introduction
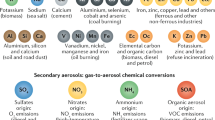
In 2016, the WHO estimated that 4.2 million deaths annually could be attributed to ambient (outdoor) fine particulate matter air pollution, or PM2.5 (particles smaller than 2.5 μm in diameter)1. PM2.5 comes from a wide range of sources, including energy production, households, industry, transport, waste, agriculture, desert dust and forest fires and particles can travel in the atmosphere for hundreds of kilometres and their chemical and physical characteristics may vary greatly over time and space. The WHO developed Air Quality Guidelines (AQG) to offer guidance for reducing the health impacts of air pollution. The first edition, the WHO AQG for Europe, was published in 1987 with a global update (in 2005) reflecting the increased scientific evidence of the health risks of air pollution worldwide and the growing appreciation of the global scale of the problem2. The current WHO AQG states that annual mean concentration should not exceed 10 μg/m3 2.
The adoption and implementation of policy interventions have proved to be effective in improving air quality3,4,5,6,7. There are at least three examples of enforcement of long-term policies that have reduced concentration of air pollutants in Europe and North America: (i) the Clean Air Act in 1963 and its subsequent amendments in the USA; (ii) the Convention on Long-range Transboundary Air Pollution (LRTAP) with protocols enforced since the beginning of the 1980s in Europe and North America8; and (iii) the European emission standards passed in the European Union in the early 1990s9. However, between 1960 and 2009 concentrations of PM2.5 globally increased by 38%, due in large part to increases in China and India, with deaths attributable to air pollution increasing by 124% between 1960 and 200910.
The momentum behind the air pollution and climate change agendas, and the synergies between them, together with the Sustainable Development Goals (SDGs) provide an opportunity to address air pollution and the related burden of disease. Here, trends in global air quality between 2010 and 2016 are examined in the context of attempts to reduce air pollution, both through long-term policies and more recent attempts to reduce levels of air pollution. Particular focus is given to providing comprehensive coverage of estimated concentrations and obtaining (national-level) distributions of population exposures for health impact assessment. Traditionally, the primary source of information has been measurements from ground monitoring networks but, although coverage is increasing, there remain regions in which monitoring is sparse, or even non-existent (see Supplementary Information)11. The Data Integration Model for Air Quality (DIMAQ) was developed by the WHO Data Integration Task Force (see Acknowledgements for details) to respond to the need for improved estimates of exposures to PM2.5 at high spatial resolution (0.1° × 0.1°) globally11. DIMAQ calibrates ground monitoring data with information from satellite retrievals of aerosol optical depth, chemical transport models and other sources to provide yearly air quality profiles for individual countries, regions and globally11. Estimates of PM2.5 concentrations have been compared with previous studies and a good quantitative agreement in the direction and magnitude of trends has been found. This is especially valid in data rich settings (North America, Western Europe and China) where trends results are consistent with what has been found from the analysis of ground level PM2.5 measurements.
Results
Figure 1a shows average annual concentrations of PM2.5 for 2016, estimated using DIMAQ,; and Fig. 1b the differences in concentrations between 2010 and 2016. Although air pollution affects high and low-income countries alike, low- and middle-income countries experience the highest burden, with the highest concentrations being seen in Central, Eastern Southern and South-Eastern Asia12.

a Concentrations in 2016. b Changes in concentrations between 2010 and 2016.
The high concentrations observed across parts of the Middle East, parts of Asia and Sub-Saharan regions of Africa are associated with sand and desert dust. Desert dust has received increasing attention due to the magnitude of its concentration and the capacity to be transported over very long distances in particular areas of the world13,14. The Sahara is one of the biggest global source of desert dust15 and the increase of PM2.5 in this region is consistent with the prediction of an increase of desert dust due to climate change16,17.
Globally, 55.3% of the world’s population were exposed to increased levels of PM2.5, between 2010 and 2016, however there are marked differences in the direction and magnitude of trends across the world. For example, in North America and Europe annual average population-weighted concentrations decreased from 12.4 to 9.8 μg/m3 while in Central and Southern Asia they rose from 54.8 to 61.5 μg/m3. Reductions in concentrations observed in North America and Europe align with those reported by the US Environmental Protection Agency and European Environmental Agency (EEA)18,19. The lower values observed in these regions reflect substantial regulatory processes that were implemented thirty years ago that have led to substantial decreases in air pollution over previous decades18,20,21. In high-income countries, the extent of air pollution from widespread coal and other solid-fuel burning, together with other toxic emissions from largely unregulated industrial processes, declined markedly with Clean Air Acts and similar ‘smoke control’ legislation introduced from the mid-20th century. However, these remain important sources of air pollution in other parts of the world22. In North America and Europe, the rates of improvements are small reflecting the difficulties in reducing concentrations at lower levels.
Assessing the health impacts of air pollution requires detailed information of the levels to which specific populations are exposed. Specifically, it is important to identify whether areas where there are high concentrations are co-located with high populations within a country or region. Population-weighted concentrations, often referred to as population-weighted exposures, are calculated by spatially aligning concentrations of PM2.5 with population estimates (see Supplementary Information).
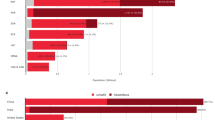
Figure 2 shows global trends in estimated concentrations and population-weighted concentrations of PM2.5 for 2010–2016, together with trends for SDG regions (see Supplementary Fig. 1.1). Where population-weighted exposures are higher than concentrations, as seen in Central Asia and Southern Asia, this indicates that higher levels of air pollution coincide with highly populated areas. Globally, whilst concentrations have reduced slightly (from 12.8 μg/m3 in 2010 to 11.7 in 2016), population-weighted concentrations have increased slightly (33.5 μg/m3 in 2010, 34.6 μg/m3 in 2016). In North America and Europe both concentrations and population-weighted concentrations have decreased (6.1–4.9 and 12.4–9.8 μg/m3, respectively). The association between concentrations and population can be clearly seen for Central Asia and Southern Asia where concentrations increased from 29.6 to 31.7 μg/m3 (a 7% increase) while population-weighted concentrations were higher both in magnitude and in percentage of increase, increasing from 54.8 to 61.5 μg/m3 (a 12% increase).

a Concentrations. b Population-weighted concentrations.
For the Eastern Asia and South Eastern Asia concentrations increase from 2010 to 2013 and then decrease from 2013 to 2016, a result of the implementation of the ‘Air Pollution Prevention and Control Action Plan’21 and the transition to cleaner energy mix due to increased urbanization in China23,24,25. Population-weighted concentrations for urban areas in this region are strongly influenced by China, which comprises 62.6% of the population in the region. Population-weighted concentrations are higher than the concentrations and the decrease is more marked (in the population-weighted concentrations), indicating that the implementation of policies has been successful in terms of the number of people affected. The opposite effect of population-weighting is observed in areas within Western Asia and Northern Africa where an increasing trend in population-weighted concentrations (from 42.0 to 43.1. μg/m3) contains lower values than for concentrations (from 50.7 to 52.6 μg/m3). In this region, concentrations are inversely correlated with population, reflecting the high concentrations associated with desert dust in areas of lower population density.
Discussion
Long-term policies to reduce air pollution have been shown to be effective and have been implemented in many countries, notably in Europe and the United States. However, even in countries with the cleanest air there are large numbers of people exposed to harmful levels of air pollution. Although precise quantification of the outcomes of specific policies is difficult, coupling the evidence for effective interventions with global, regional and local trends in air pollution can provide essential information for the evidence base that is key in informing and monitoring future policies. There have been major advances in methods that expand the knowledge base about impacts of air pollution on health, from evidence on the health effects26, modelling levels of air pollution1,11 and quantification of health impacts that can be used to monitor and report on progress towards the air pollution-related indicators of the Sustainable Development Goals: SDG 3.9.1 (mortality rate attributed to household and ambient air pollution); SDG 7.1.2 (proportion of population with primary reliance on clean fuels and technology); and SDG 11.6.2 (annual mean levels of fine particulate matter (e.g., PM2.5 and PM10) in cities (population weighted))1. There is a continuing need for further research, collaboration and sharing of good practice between scientists and international organisations, for example the WHO and the World Meteorological Organization, to improve modelling of global air pollution and the assessment of its impact on health. This will include developing models that address specific questions, including for example the effects of transboundary air pollution and desert dust, and to produce tools that provide policy makers with the ability to assess the effects of interventions and to accurately predict the potential effects of proposed policies.
Globally, the population exposed to PM2.5 levels above the current WHO AQG (annual average of 10 μg/m3) has fallen from 94.2% in 2010 to 90.0% in 2016, driven largely by decreases in North America and Europe (from 71.0% in 2010 to 48.6% in 2016). However, no such improvements are seen in other regions where the proportion has remained virtually constant and extremely high (e.g., greater than 99% in Central, Southern, Eastern and South-Eastern Asia Sustainable Development Goal (SDG) regions. See Supplementary Information for more details).
The problem, and the need for solutions, is not confined to cities: across much of the world the vast majority of people living in rural areas are also exposed to levels above the guidelines. Although there are differences when considering urban and rural areas in North America and Europe, in the vast majority of the world populations living in both urban and rural areas are exposed to levels that are above the AQGs. However, in other regions the story is very different (see Supplementary Information Fig. 7.1 and Supplementary Information Sections 7 and 8), for example population-weighted concentrations in rural areas in the Central and Southern Asia (55.5 μg/m3), Sub-Saharan Africa (39.1 μg/m3), Western Asia and Northern Africa (42.7 μg/m3) and Eastern Asia and South-Eastern Asia (34.3 μg/m3) regions (in 2016) were all considerably above the AQG. From 2010 to 2016 population-weighted concentrations in rural areas in the Central and Southern Asia region rose by approximately 11% (from 49.8 to 55.5 μg/m3; see Supplementary Information Fig. 7.1 and Supplementary Information Sections 7 and 8). This is largely driven by large rural populations in India where 67.2% of the population live in rural areas27. Addressing air pollution in both rural and urban settings should therefore be a key priority in effectively reducing the burden of disease associated with air pollution.
Attempts to mitigate the effects of air pollution have varied according to its source and local conditions, but in all cases cooperation across sectors and at different levels, urban, regional, national and international, is crucial28. Policies and investments supporting affordable and sustainable access to clean energy, cleaner transport and power generation, as well as energy-efficient housing and municipal waste management can reduce key sources of outdoor air pollution. Interventions would not only improve health but also reduce climate pollutants and serve as a catalyst for local economic development and the promotion of healthy lifestyles.
Methods
Assessment of trends in global air pollution requires comprehensive information on concentrations over time for every country. This information is primarily based on ground monitoring (GM) from 9690 monitoring locations around the world from the WHO cities database for 2010–2016. However, there are regions in this may be limited if not completely unavailable, particularly for earlier years (see Supplementary Information). Even in countries where GM networks are well established, there will still be gaps in spatial coverage and missing data over time. The Data Integration Model for Air Quality (DIMAQ) supplements GM with information from other sources including estimates of PM2.5 from satellite retrievals and chemical transport models, population estimates and topography (e.g., elevation). Specifically, satellite-based estimates that combine aerosol optical depth retrievals with information from the GEOS-Chem chemical transport model29 were used, together with estimates of sulfate, nitrate, ammonium, organic carbon and mineral dust30.
The most recent release of the WHO ambient air quality database, for the first time, contains data from GM for multiple years, where available The version of DIMAQ used here builds on the original version11,30 by allowing data from multiple years to be modelled simultaneously, with the relationship between GMs and satellite-based estimates allowed to vary (smoothly) over time. The result is a comprehensive set of high-resolution (10 km × 10 km) estimates of PM2.5 for each year (2010–2016) for every country.
In order to produce population-weighted concentrations, a comprehensive set of population data on a high-resolution grid (Gridded Population of the World (GPW v4) database31) was combined with estimates from DIMAQ. In addition, the Global Human Settlement Layer32 was used to define areas as either urban, sub-urban or rural (based on land-use, derived from satellite images, and population estimates). A further dichotomous classification of whether grid-cells within a particular country were urban or rural (allocating sub-urban as either urban or rural) was based on providing the best alignment (at the country-level) to the estimates of urban-rural populations produced by the United Nations27.
It is noted that the estimates from DIMAQ used in this article may differ slightly from those used in the WHO estimates of the global burden of disease associated with ambient air pollution1, and the associated estimates of air pollution related SDG indicators, due to recent updates in the database and further quality assurance procedures.
Data availability
The estimates of PM2.5 data that support the findings of this work are available from https://www.who.int/airpollution/data/en/.
References
Ambient air pollution: Global assessment of exposure and BOD, update 2018. WHO (2020) (In press).
Krzyzanowski, M. & Cohen, A. Update of WHO air quality guidelines. Air Qual. Atmosphere Health 1, 7–13 (2008).
Zheng, Y. et al. Air quality improvements and health benefits from China’s clean air action since 2013. Environ. Res. Lett. 12, 114020 (2017).
Turnock, S. T. et al. The impact of European legislative and technology measures to reduce air pollutants on air quality, human health and climate. Environ. Res. Lett. 11, 024010 (2016).
Zhang, Y. et al. Long-term trends in the ambient PM2.5- and O3-related mortality burdens in the United States under emission reductions from 1990 to 2010. Atmos. Chem. Phys. 18, 15003–15016 (2018).
Kuklinska, K., Wolska, L. & Namiesnik, J. Air quality policy in the U.S. and the EU – a review. Atmos. Pollut. Res 6, 129–137 (2015).
Guerreiro, C. B. B., Foltescu, V. & de Leeuw, F. Air quality status and trends in Europe. Atmos. Environ. 98, 376–384 (2014).
Byrne, A. The 1979 convention on long-range transboundary air pollution: assessing its effectiveness as a multilateral environmental regime after 35 Years. Transnatl. Environ. Law 4, 37–67 (2015).
Crippa, M. et al. Forty years of improvements in European air quality: regional policy-industry interactions with global impacts. Atmos. Chem. Phys. 16, 3825–3841 (2016).
Butt, E. W. et al. Global and regional trends in particulate air pollution and attributable health burden over the past 50 years. Environ. Res. Lett. 12, 104017 (2017).
Shaddick, G. et al. Data integration model for air quality: a hierarchical approach to the global estimation of exposures to ambient air pollution. J. R. Stat. Soc. Ser. C. Appl. Stat. 67, 231–253 (2018).
World Bank Country and Lending Groups—World Bank data. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (Accessed 3rd December 2018).
Guo, H. et al. Assessment of PM2.5 concentrations and exposure throughout China using ground observations. Sci. Total Environ. 601–602, 1024–1030 (2017).
Ganor, E., Osetinsky, I., Stupp, A. & Alpert, P. Increasing trend of African dust, over 49 years, in the eastern Mediterranean. J. Geophys. Res. 115, 1–7 (2010).
Goudie, A. S. & Middleton, N. J. Desert Dust in the Global System. (Springer Science & Business Media, 2006).
Mahowald, N. M. et al. Observed 20th century desert dust variability: impact on climate and biogeochemistry. Atmos. Chem. Phys. 10, 10875–10893 (2010).
Stanelle, T., Bey, I., Raddatz, T., Reick, C. & Tegen, I. Anthropogenically induced changes in twentieth century mineral dust burden and the associated impact on radiative forcing. J. Geophys. Res. Atmosph 119, 13526–13546 (2014).
Air quality in Europe (European Environment Agency, 2018). https://www.eea.europa.eu/publications/air-quality-in-europe-2018.
Particulate Matter (PM2.5) Trends | National Air Quality: Status and Trends of Key Air Pollutants | US EPA. https://www.epa.gov/air-trends/particulate-matter-pm25-trends.
Chay, K., Dobkin, C. & Greenstone, M. The clean air act of 1970 and adult mortality. J. Risk Uncertain. 27, 279–300 (2003).
Huang, J., Pan, X., Guo, X. & Li, G. Health impact of China’s air pollution prevention and control action plan: an analysis of national air quality monitoring and mortality data. Lancet Planet. Health 2, e313–e323 (2018).
Heal, M. R., Kumar, P. & Harrison, R. M. Particles, air quality, policy and health. Chem. Soc. Rev. 41, 6606–6630 (2012).
Chen, J. et al. A review of biomass burning: emissions and impacts on air quality, health and climate in China. Sci. Total Environ. 579, 1000–1034 (2017).
Zhao, B. et al. Change in household fuels dominates the decrease in PM2.5 exposure and premature mortality in China in 2005–2015. Proc. Natl. Acad. Sci. 201812955 (2018). https://doi.org/10.1073/pnas.1812955115.
Shen, H. et al. Urbanization-induced population migration has reduced ambient PM2.5 concentrations in China. Sci. Adv. 3, e1700300 (2017).
Burnett, R. et al. Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proc. Natl Acad. Sci. 115, 9592–9597 (2018).
World Urbanization Prospects - Population Division - United Nations. https://population.un.org/wup/Download/ (Accessed: 10th December 2018).
Towards Cleaner Air Scientific Assessment Report 2016- UNECE (2016). https://www.unece.org/index.php?id=42861.
van Donkelaar, A. et al. Global estimates of fine particulate matter using a combined geophysical-statistical method with information from satellites, models, and monitors. Environ. Sci. Technol. 50, 3762–3772 (2016).
Shaddick, G. et al. Data Integration for the assessment for population exposure to ambient air pollution for global burden of disease assessment. Environ. Sci. Technol. 52, 9069–9078 (2018).
Center for International Earth Science Information Network (CIESIN) Columbia University. 2016. Gridded Population of the World, Version 4 (GPWv4): Population Count. NASA Socioeconomic Data and Applications Center (SEDAC), Palisades, NY. https://doi.org/10.7927/H4X63JVC. Accessed 3rd December 2018.
Pesaresi, M. et al. GHS Settlement grid following the REGIO model 2014 in application to GHSL Landsat and CIESIN GPW v4- multitemporal (1975-1990-2000-2015). European Commission, Joint Research Centre (JRC)[Dataset] http://data.europa.eu/89h/jrc-ghsl-ghs_smod_pop_globe_r2016a. Accessed: 3rd December 2018.
Acknowledgements
The authors would like to thank the WHO Data Integration Task Force, a multi-disciplinary group of experts established as part of the recommendations from the first meeting of the WHO Global Platform for Air Quality, Geneva, January 2014. The Task Force developed the Data Integration Model for Air Quality and consists of the first author, Michael Brauer, Aaron van Donkelaar, Rick Burnett, Howard H. Chang, Aaron Cohen, Rita Van Dingenen, Yang Liu, Randall Martin, Lance A. Waller, Jason West, James V. Zidek and Annette Pruss-Ustun. The authors would like to give particular thanks to Michael Brauer who provided specialist expertise, together with data on ground measurements, and Aaron van Donkelaar and the Atmospheric Composition Analysis Group at Dalhousie University for providing estimates from satellite remote sensing. The authors would also like to thank Dan Simpson for technical expertise on implementing extensions to DIMAQ. Matthew L Thomas is supported by a scholarship from the EPSRC Centre for Doctoral Training in Statistical Applied Mathematics at Bath (SAMBa), under the project EP/L015684/1. The views expressed in this article are those of the authors and they do not necessarily represent the views, decisions or policies to institutions with which they are affiliated.
Author information
Authors and Affiliations
Contributions
GS, PM, and SG conceived the project and led the writing of the manuscript. MLT and GR performed the data analysis. GS and MLT developed the statistical model used to produce the estimates. All authors contributed to the writing of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shaddick, G., Thomas, M.L., Mudu, P. et al. Half the world’s population are exposed to increasing air pollution. npj Clim Atmos Sci 3, 23 (2020). https://doi.org/10.1038/s41612-020-0124-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41612-020-0124-2
This article is cited by
-
Higher air pollution in wealthy districts of most low- and middle-income countries
Nature Sustainability (2024)
-
Mineralogical Characteristics and Sources of Coarse Mode Particulate Matter in Central Himalayas
Aerosol Science and Engineering (2024)
-
Role of short-term campaigns and long-term mechanisms for air pollution control: lessons learned from the “2 + 26” city cluster in China
Environmental Science and Pollution Research (2024)
-
A Review of the Interactive Effects of Climate and Air Pollution on Human Health in China
Current Environmental Health Reports (2024)
-
Indoor Air Pollution in Kenya
Aerosol Science and Engineering (2024)
