
Abstract
Despite gaming disorder now being diagnosable by the International Classification of Diseases (ICD-11) as a new mental disorder due to addictive behaviors, little is known about the concrete reasons for which people seek treatment for their videogame play. As the current literature is mainly based on children and adolescents, there is a strong need for better understanding adult treatment-seekers in particular. This preregistered study responds to the gap in research by qualitatively investigating the reasons for treatment-seeking with 110 participants who had sought help for their videogame play from a Finnish treatment program. We applied template analysis to the open-ended data, which consist of the participants’ personal accounts regarding their problems. Additionally, we report the game titles that the participants had problems with, as well as Internet Gaming Disorder Test (IGDT-10) scores, which were measured from 89 participants. The template analysis suggested five themes, which cover the main reasons for treatment-seeking: social reasons, existential reasons, practical reasons, self-perceived addiction, and wish for support. Many of these themes overlap with the ICD-11 description of gaming disorder, but several issues, such as loss of meaning and financial harms, are not part of the current diagnosis. The average IGDT-10 score among participants was 3.86 (SD = 2.55) and 37 (42%) individuals met the disorder cutoff (5.00). Numerous videogames with different designs were mentioned as sources of problems, of which 26 were mentioned more than once. The study indicates that adults seek treatment for many kinds of games and gaming-related problems, including but not limited to those, which are described part of the ICD-11 gaming disorder diagnoses. We recommend both researchers and practitioners to implement an expanded perspective on gaming behaviors, acknowledging that adults may seek treatment for diverse gaming-related problems, some of which not necessarily relevant to gaming disorder or mental disorders in general.
Similar content being viewed by others

Introduction
A lot of research has been carried out on addictive gaming behaviors, especially after the recent inclusion of “gaming disorder” diagnosis in the 11th edition of the International Classification of Diseases (ICD-11). Nevertheless, studies with treatment-seekers are still rare, and qualitative studies that allow treatment-seekers to share their experiences and thoughts are even rarer. As a result, while the current diagnostic manual(s) include detailed descriptions of gaming problems, it remains widely unknown why people seek related treatment (Karhulahti, 2022). For instance, according to the official ICD-11 diagnosis, “gaming behavior results in marked distress or significant impairment in personal, family, social, educational, occupational, or other important areas of functioning,” but it is not known whether these types of impairment are the same ones that lead people to seek related treatment. Our study aims to answer this question by a qualitative analysis of a unique clinical dataset, consisting of adults who have sought treatment for their gaming.
Literature
Historically, several methods have been applied to identify different types of players with and without gaming problems. For instance, cluster analytic (Billieux et al., 2015a; Musetti et al., 2019), latent class analytic (Colder Carras, Kardefelt-Winther, 2018; Myrseth & Notelaers, 2018), and theory-driven (Lee et al., 2017) approaches have resulted in diverse typologies of gaming disorder or related habits more generally. Most of these studies explicitly aim at charting distinctions between clinical and non-clinical populations, but few have treatment-seeking data that would allow making typological inferences within clinical groups. Moreover, because gaming disorder diagnoses were not effective before 2022, virtually none of the studies in the current literature have been able to identify their participants with an official gaming disorder diagnosis yet (ICD-11). Following this limitation, numerous different criteria have been used to identify gaming disorder or related problems. Although one of the strongest means for identifying clinically significant individuals has been their treatment-seeking status, it is also important to remember that this alone does not qualify for a gaming disorder diagnosis; meanwhile, many who might meet diagnostic criteria do not seek treatment. People can seek treatment for many kinds of gaming-related problems, and for various reasons.
In one of the few qualitative interview studies with treatment-seekers, Beranuy et al. (2013) interviewed nine young men (age 16–26, M = 20.5) from Chile/Spain whose parents had requested hospital care for them. Treatment-seeking for these (mainly underage) participants was thus decided by their parents and not the participants themselves. This indicates external treatment-seeking motivations to be significant for young individuals, while leaving internal motivations and understandings of the related problems unclear. In an exceptionally large clinical study, in turn, Starcevic et al. (2020) carried out diagnostic interviews with 100 treatment-seekers in South Korea (age >13, M = 21.2). Although seeking motivations were not explicitly studied, the authors noted that “a large proportion of these participants sought treatment under pressure from their family members or on the advice of friends” (p. 32). Qualitative research in the Chinese context echoes similar findings (Bax, 2013), albeit it remains generally unstudied how hospital patients in major clinical studies (e.g., Tao et al., 2010) subjectively perceive their treatment-seeking. Alternatively, as countries like South Korea organize systematic student screening for gaming disorder—and the risk groups are guided to receive an intervention—in some cases people are also known to seek treatment due to authoritarian recommendations (Jeong et al., 2019). Because almost all clinical gaming disorder studies are dominated by child and adolescent participants (ages 12–20 as per ICD-11), it is indeed likely that caregivers and other authorities are a strong driver for treatment-seeking (see, Carbonell, 2017). Globally, the individuals’ subjective motivations and thoughts on treatment-seeking remain unstudied.
At the same time, caregivers tend to have less influence on adults, and it is possible that adults end up in treatment for different reasons. To our knowledge, there are no previous systematic studies on these reasons, with the caveat that many adolescent samples (such as those cited above) do include some adults as well. In other words, the reasons for which adults seek treatment for their gaming-related problems remains unmapped. To better understand these reasons is the goal of our study.
Data and methods
Our data consist of adult participants who sought treatment for their gaming problems in Finland between 2020 and 2022. All participants had personally applied for government-funded remotely provided treatment in the “Restart” program, which is a subservice of Peluuri that has provided help for gambling problems since 2004 (supported by national gambling monopoly Veikkaus revenues through the Funding Centre for Social Welfare and Health Organisations, which, again, operates under the Ministry of Social Affairs and Health). “Restart” was opened as a specialized program for helping Finnish-speaking people with videogame-related problems. We applied to access the program data and received written permission on January 31, 2022. We consulted the local ethics committee and were advised not to utilize the ethics review process. According to Finnish Research Integrity guidelines, a study like this (existing data without personal identifiers) should not be submitted to ethics review.
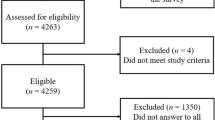
At the time of accessing the data, a total of 112 people with gaming-related problems had applied, but two did not share their data for research. Thus, our final sample is N = 110 (91 men, 83%; three preferred not to disclose gender). More than half (51%) had found the treatment program by personally searching for related help services (e.g., internet), and many (33%) were referred from other services (e.g., healthcare and psychologists). A minority had applied due to a recommendation of friend or family member (15%). Of all participants (age M = 30.5, SD = 6.8), at the time of applying, 60 (55%) were in a romantic relationship and 41 (37%) lived alone. All participants had filled out a long entrance survey, which included both closed and open items. Three open questions inquire about the reasons for applying as well as the context surrounding them:
-
1.
Why have you decided to apply for the Restart program?
[Miksi olet hakenut Restart-ohjelmaan?]
-
2.
What are your expectations regarding the program?
[Mitä odotat ohjelmalta?]
-
3.
What kind of aid do you need?
[Millaista tukea tarvitset?]
We chose these three key items for analysis, as they collectively provide a relatively large qualitative dataset that can answer our research question. For descriptive reporting, we additionally included the items concerning the length, type, and self-assessment of gaming problems as well as the Internet Gaming Disorder Test 10 (Király et al., 2017) scores. As the videogames played by the participants are essentially a part of their reasons for treatment-seeking, we also report the gaming titles with which the participants expressed having problems. The study was preregistered in the Open Science Framework.Footnote 1 The second preregistered research question—“What are the contextual-motivational differences between help-seekers who commit to treatment and those who do not commit to treatment?”—was not pursued because we considered the treatment-seeking data not yet sufficient for answering the question meaningfully. Many participants had started their treatment recently, for which we were unable to assess their degree of commitment during the time of analysis. Due to the program’s clinical policy, we are not allowed to reshare the data, however, the data are available for scientific use in Peluuri’s own repository by request. All our code and coding materials are shared as supplements (Supplement Appendix 1–3).
Template analysis
We apply qualitative template analyses (Brooks et al., 2015), which is a flexible thematic analysis method specialized in producing multilevel-structures. Due to its capacity to generate rich theme hierarchies, the method was considered suitable for the present data and goals. Because the present number of participants is relatively large for qualitative research, in-depth analytical methods (e.g., reflexive thematic analysis or interpretive phenomenological analysis) would not have been optimal. On the other hand, the open-ended narrative responses also did not provide such rich social cues that, for instance, face-to-face interview data often do. In this context, template analysis, in the below adapted form, is suitable by allowing us to systematically map out and organize the reasons for applying.
Coding instructions were developed by one author (Supplement Appendix 1) after having read all the data. Two other authors then independently coded the data using the instructions; the outcomes of these independent coding processes are attached (Supplement Appendix 2). One of the coders deviated from the instructions by coding in Finnish instead of English because we agreed—after preregistration—that it would be beneficial have both native and non-native codes to capture possible conceptual differences in local language. Afterwards, the full team met to negotiate agreement upon the highest thematic levels. Following the above, the non-coding author iterated the two independent micro-level code hierarchies and produced the first version of the template by re-reflecting on the data (Supplement Appendix 2). Last, the team negotiated changes and produced the final template (Fig. 1). Regarding positionality, both coders (man and woman) are mental health professionals, the former as a licensed psychologist and the latter as a treatment expert with a demonstrated history on helping both gambling and gaming treatment-seekers. The non-coding author is a senior researcher specialized in gaming disorder and qualitative research methods.

Final template.
Results
Quantitative descriptive analysis
The average length of gaming-related problems was 8.7 years (SD = 6.5) and the types of problems, based on four closed response options, are presented descriptively in Table 1. The gaming titles that were reported to cause problems (each treatment-seeker was allowed to name three) are listed in Table 2. Additionally, the Internet Gaming Disorder Test 10 (Király et al., 2017)—Finnish translation has previously been found reliable (Männikkö et al., 2019)—was filled by 89 individuals who proceeded from the application phase to treatment start. Total omega coefficient (0.86) indicated reliability for the scale. The average test score was 3.86 (SD = 2.55), which is below the scale’s official internet gaming disorder cutoff (5.00). In total, 42% (n = 37) of all treatment-starters met the cutoff. The code for the above descriptive statistics is shared in Supplement Appendix 3.
Of all treatment-seekers, four (4%) did not consider gaming to be a problem for them based on the binary response item “Do you consider your gaming to be problematic?” [Koetko pelaamisesi ongelmalliseksi?]. For two of these four, the reason for applying that was disclosed in the present data was to comply with friend or family members’ wishes; the third considered previously having had problems, and the fourth explicitly talked about gaming-related problems, even though having marked “no problems” as the closed response option.
Qualitative template analysis
The template analysis suggested five themes, which cover the main reasons for treatment-seeking: social reasons, existential reasons, practical reasons, self-perceived addiction, and wish for support (Fig. 1). Many of the reasons overlap, and one participant often expressed multiple different reasons, which were coded separately. In other words, individual participants were not considered belonging to a single theme, but their response content and the derived codes typically characterized several themes. As some of the below examples also echo elements of multiple themes, underlining has been added to highlight relevance for the represented theme. All themes are presented in Fig. 1 as a three-tier template.
Within social reasons, we identified two general categories, which largely correspond with external and internal reasons. The first category, to comply socially, refers to applying to the program by request of others (usually the spouse). In this case, the motivation to apply for treatment is coming from others. In the second category, to improve socially, the individual has clearly applied for intrinsic reasons. The three most common expectations under this theme were the wish to be a better partner or parent, and the wish to enrich social life in general.
Example 1:
“I would like to have my gaming under control in a way that it would not interfere with my relationship.”
Example 2:
“My wife told me I need this.”
Example 3:
“My husband and daughter need me, but I just play the console all day. I have anxiety disorder and severe depression.”
Example 4:
“Gaming takes too much time from my other interests and social life, and in the end, it feels that I do nothing else but play videogames.”
Within existential reasons, we identified the applicants desiring to resolve lost meaning in gaming and life, respectively with overlap. In the former category, gaming had either stopped being fun, there were problems in the community, the applicant identified their specific play style problematic, or the applicant was confused about what was valuable to them anymore. Similar issues occurred in the larger domain of life, i.e., the applicant wished to find other life interests or motivation, or they needed to self-reflect or reconsider their priorities in life. Their lives had become either uncomfortably narrow (around gaming), or the role of gaming in those lives had become questionable against their own system of values.
Example 1:
“Although I get my responsibilities done, gaming has started to feel like a forced activity, not intrinsically fun. But instead of doing fun things, I just end up gaming. There’s no joy in it.”
Example 2:
“Success in this videogame is the most meaningful thing in my life. [I] want to reduce the meaning of gaming in my life.”
Example 3:
“I would like to replace my gaming with ‘real’ life.”
Example 4:
“I’ve spent my entire life on the computer. I wake up, go to the computer, eat, drink, go shopping, back to the computer, then sleep. [I need] help, support, and self-reflection.”
Practical reasons consist of three categories. In the first category, the applicants wished to ameliorate performance harms; namely, educational, occupational, or routine duties. In the second category, the applicants wished to ameliorate health harms that involved anxiety and sleep problems, as well as other serious mental health comorbidity issues. Finally, some participants felt they spend too much money on gaming and wished to ameliorate financial harms.
Example 1:
“Often I play late until night, and this leaves me with little low-quality sleep. Then I am tired and don’t have the energy to spend time with my children.”
Example 2:
“I would like to have support for learning how to not use money in gaming.”
Example 3:
“Gaming sucks my creative energy, rhythms the entire day, prevents me from sleeping and makes going to school difficult.”
Example 4:
“Gaming harms my work performance and limits my life development.”
Self-perceived addiction [both Finnish terms were used: addiktio, riippuvuus], which was associated with gaming, resulted in two related categories. In the first one, the applicants wanted to change their behavior by learning to control gaming or otherwise “break” the addictively experienced process. Additionally, some individuals explicitly expressed gaming to align with their avoidance behavior, which they wanted to change. In the second category, the applicants acknowledged having gaming problems, such as those related time use, relapse, and strong urge to play.
Example 1:
“I want to reduce, but not entirely quit, my gaming. This feels impossible, but it has troubled me for 10 years now.”
Example 2:
“I identify as a videogame addict, and videogames recently led to an end of my relationship.”
Example 3:
“I feel that life is not in my control. I could accomplish so much, but instead of studying, going to hobbies, or carrying out other responsibilities, I just open the internet and videogames because it’s easy.”
Example 4:
“I’ve been diagnosed with general anxiety disorder and online gaming is my default escape from anxiety and boredom.”
Our final theme is wish for support, which is distinct from the other themes by representing the need for solutions (rather than problems as such). In general, many participants felt they were “lost” or “perplexed” and could not solve the situation on their own, which led them to seek any or specific kind of help, depending on individual histories. This theme likewise had two dimensions. Many applicants sought to gain guidance and models that they could use in everyday life. The three main expectations in this category were the desire to learn regulation skills, practical tips, and support to maintain control. In the second category, the applicants wished to interact and share their experiences, seeking empathy, a listener, or peer support.
Example 1:
“I would prefer to have a weekly conversation with a therapist, this is what I need. In group [therapy], things are often discussed generally, and people are in different situations, so the personal connection is thin.”
Example 2:
“[I need] tools and help for finding myself and for identifying/controlling gaming and computer use. For instance, how to handle feelings of obligation when others go gaming and it feels that I should too, and then I feel guilt for betraying them for not being there.”
Example 3:
“[I need] advise for how to quit gaming and how to avoid spending money on it and running into debt (if I don’t quit entirely)”
Example 4:
“[I need] advice and monitoring. I’ve learned that if I am accountable for myself alone, I cannot take responsibility. If someone else expects me to do something, it’s easier.”
As a meta-theme prevalent in all five main themes, a large part of the applicants had their problems strongly connected to the prioritization, regulation, and understanding of time. Although some felt gaming was associated with various concrete harms, the mere loss of time (with or without other consequences) was a central component in their treatment-seeking (“Gaming just takes too much of my time,” “I want to use my time differently,” “The time I spend on gaming harms my daily routines and housework”). As such, the concept of time extends beyond the single mention as one of the acknowledged problems and is linked to treatment-seeking in diverse ways.
Para-exploratory analysis
Considering that 42% of our participants who started treatment met the polythetic cutoff determined by the Internet Gaming Disorder Test (Király et al., 2017), we became curious—encouraged by our peer reviewers—whether there could be thematic differences between those who did and did not meet the clinical criteria. Accordingly, we decided the carry out a second round of coding, this time using the five themes with a deductive approach. The same two researchers independently coded all cases with up to two of the discovered themes, thus aiming to identify the most prevalent reasons for treatment-seeking (Supplement Appendix 3). Among those who started treatment and filled out the scale (n = 89), the coders agreed in 87 cases (98%) at least on the primary theme, and in 61 cases (69%) on both the primary and secondary themes (Table 3). Due to the para-exploratory nature of these analyses, we report the results based on these single-round ratings without assessing statistical significance or effect sizes of interest (Table 3).
Although these non-confirmatory findings should be taken with a grain of salt, they allow for two potentially valuable observations to be further assessed and tested in confirmatory study designs. In general, the thematic differences between groups are very small with one visible exception: individuals who did not meet the disorder cutoff sought treatment for practical reasons twice as often compared to the cutoff group. If replicated in the future, we believe this effect is caused by the scale (and the applied DSM-5 criteria more widely) not giving much weight for the practical health, financial, and performance harms for which treatment-seekers seek help.
In fact, only one or two (out of the nine) symptoms listed by the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) explicitly address harms, while the rest of the symptoms largely align with classic substance use components such as “preoccupation”, “withdrawal”, and “tolerance”. It is worth noting that the DSM-5 defines “clinically significant disturbance” as a general criterion for mental disorders, but this criterion is almost never measured by DSM-5-based scales, including the present one. Moreover, neither the scale nor the DSM-5 address financial problems related to gaming, for which such treatment-seekers are unlikely to meet DSM-5 criteria (e.g., Example 2 in Practical Reasons did not meet the scale cutoff). Secondly, the wider lack of thematic differences between the two groups raises a question regarding the screened “internet gaming disorder” construct. When 58% of treatment-seekers do not meet the cutoff but experience a need for help and start the program for the same thematic reasons as do those who meet the cutoff, it remains unclear what the scale’s measured construct is.
Discussion
Our qualitative analysis of 110 treatment-seekers demonstrates that people seek help for their gaming for many reasons, and in relation to numerous different types of gaming. Due to the qualitative nature of this study, we do not make claims about the most or least common reasons. Rather, our study is among the firsts to report what the different reasons are.
First, we note that some individuals sought treatment due to issues that correspond with “significant impairment,” such as educational and occupational problems, as described in the (ICD-11) gaming disorder diagnostic criteria. Some other criteria, such as “increasing priority given to gaming” (over the past 12 months) appear less relevant in this context, as gaming had typically been a priority for the participants for several years—the average duration of problems was 8.7 years (see also, Brand et al., 2020). In some cases, the reasons for treatment-seeking were severe; for example, attempted suicide was associated with some of the participants’ reasons for applying help. In the future efforts to better treat and understand gaming-related problems, it remains important to carefully assess comorbidity and especially common disorders such as anxiety, which were mentioned as reasons for treatment-seeking in various forms.
Second, the diverse reasons for seeking treatment suggest that gaming disorder (as a diagnosable mental disorder by the ICD-11) is unlikely the only reason for adults to seek help for their gaming. For instance, problems related to financial harms and the lost meaning of gaming are not included in the ICD-11 diagnosis. Additionally, we witnessed only 37 applicants meeting the cutoff (5.00/9.00) of a validated screening scale with the total average score being relatively low (3.86/9.00). Although this discrepancy is surprising, it is worth noting that low scores in such screening scales can still correlate with weaker wellbeing in comparison to null scores (Ballou & Zendle, 2022). Our results qualitatively illustrate how people with gaming problems that do not meet scale cutoffs also seek treatment for their gaming specifically. Likewise, social compliance and the fact that four applicants (4%) did not consider their gaming problematic in any way voiced that, for some treatment-seekers, help was needed for solving other life issues. The subjective perceptions and understandings of gaming-related problems also seem to differ significantly between individuals.
In Finland, programs like “Restart” currently respond to the above problems by providing free, immediate, and continuous support regardless of the problems’ type. To a large degree, this aligns with the local Open Dialogue philosophy (Mosse et al., 2023), which avoids approaching people with mental health needs through symptom-focused diagnoses and medication solutions; rather, such people are perceived as individuals in challenging sociocultural life contexts where empathy, presence and listening can serve as primary antidotes. In the same vein, we suggest that not all gaming-related problems should be perceived nor treated as “mental disorders,” while at the same time, intensively gaming people without mental disorders may also have an increased need for empathy, presence, and listening.
Third, it is important to comment on the variety of games that were mentioned as sources of problems. No less than 26 titles were mentioned more than once, and dozens of additional titles gained a single mention. Considering our sample size (N = 110), it is reasonable to conclude that people seek treatment for many types of gaming. For instance, in addition to the oft-referenced online roleplaying games, such as World of Warcraft, multiple mentions of different esports games (League of Legends, Counter Strike, etc.), single-player storygames (Cyberpunk 2077, Dark Souls, etc.), and browser/mobile games (Clash Royale, Howrse, etc.) were given. As our qualitative approach does not allow drawing quantified inferences regarding different types of gaming being connected to different types of treatment-seeking, we encourage future research to investigate this issue explicitly. That said, we do observe a clear majority of the listed titles providing competitive features, and most of them operate by free-to-play gaming services. The latter may simply reflect the trends in the current market, but also suggests that the availability and easy access to gaming should be given attention in future research. Multiple “gambling-related titles” with the reported financial difficulties that overlap with gambling harms (Langham et al., 2015) further corroborate that academic as well as public discussion on videogame monetization and loot box design (e.g., Xiao et al., 2022) must continue.
Fourth, a key reason for many participants to apply for treatment was their wish to share experiences, thoughts, and problems. This implies that, at least in Finland, discussing about gaming problems is still a taboo and likely involves difficult emotions, such as confusion and shame. As similar challenges are known to concern problematic behaviors more widely (e.g., Barry et al., 2014; Broyles et al., 2014), we repeat our suggestion to consider alternative conceptualizations to classificatory “mental disorder” approaches and encourage the promotion of open discussion for screening and initial support. We recognize that this may be specifically suitable for the Finnish sociohistorical context: after the Nokia-driven IT industry in the 1990s, Finland has been a technology-centered country with videogame companies being perceived positively through a long cultural history of reserved privacy (Puro & Karhulahti, 2022). In such environment, expressing technology-related health issues might be more difficult than in other environments; however, this remains a hypotheses to be properly investigated in the future. Ultimately, we believe that a helpful approach would be to acknowledge that gaming problems can also be like relationship problems: it may be advisable to consult non-psychiatric experts for overcoming them. This wider view of gaming-related problems—in which gaming disorder represents only one extreme, clinically significant problem class—could facilitate different kinds of help services for people who need different kinds of help, without systematically associating all treatment-seekers with a mental disorder. The costs and benefits of diagnosis should be carefully assessed in each individual case and sociocultural context.
Last, we briefly reflect on existing models and theories. In fact, due to the wide-ranging reasons we witnessed for treatment-seeking, it would be possible to support almost any previous position with reference to our data. For example, West and Brown’s (2013) synthetic theory could be perceived supported; according to it, addiction develops in individuals whose motivational systems give damagingly high priority to a particular activity, as our themes of practical reasons and self-perceived addiction demonstrate. Likewise, Orford’s (2001) theory of addiction as an “excessive appetite”—the problem being not attaching to activities but rather the conflicts that follow—could be corroborated by our social reasons for treatment-seeking, among others. Process-based models (e.g., Brand et al., 2020; Perales et al., 2020), too, could be corroborated with our listed reasons voicing domain-specific compulsions that have evolved over many years. Unsurprisingly, the coping models (e.g., Bleckmann & Jukschat, 2015; Kardefelt‐Winther, 2017) fit the data as well, considering the numerous instances of underlying anxiety, depression, and other forms of comorbidity. To avoid the confirmatory fallacy (see Billieux et al., 2015b), we do not claim any of the models nor theories corroborated, but rather encourage researchers to consider: what could falsify such models and theories in the future? As long as all models and theories remain supported, their practical value is limited. On the other hand, perhaps gaming-related treatment-seeking is a phenomenon that cannot be captured by one model or theory.
Limitations
The data did not include clinical mental health diagnoses, due to which we do not know how many of the treatment-seekers met gaming disorder or other mental disorder criteria by a gold standard. Also, we stress that data generated via open questions are not equally rich as interview data coproduced with researchers, which sets an epistemological limitation to our analysis. The wording of the third open item (“What kind of aid do you need?”) likely led the participants to express a large proportional amount of content regarding their support needs, which is our fifth theme. However, the descriptive nature of the study and the applied template approach are generally resistant to such quantitative biases: what matter most in these results are the types of support described and expressed, which we hope to have presented in valuable depth and detail.
Conclusions
To our knowledge, this study is the first one to focus explicitly on gaming adults’ treatment-seeking experiences. We utilized qualitative data representing the treatment-seekers’ (N = 110) own views regarding the reasons for their application to receive help for gaming-related problems. Template analysis suggested five main sources of problems—social reasons, existential reasons, addictive experiences, practical reasons, wish for support—which further involved 11 sub-reasons and 29 specific expectations. The study indicates that adults seek treatment for many kinds of gaming-related problems, including but not limited to those, which are described as part of gaming disorder diagnoses. We recommend both researchers and practitioners to implement an expanded perspective on problematic gaming behaviors, acknowledging that adults seek treatment for many different types of gaming-related problems, with different degrees and kinds of clinical relevance.
Data availability
Due to the Restart program’s clinical policy, we are not allowed to reshare the data (qualitative nor quantitative responses), however, these data are available for open scientific use in Peluuri’s private repository by request. The materials related to analyzing the data are available at the Open Science Framework: https://osf.io/s4kdj/.
Notes
The preregistration is publicly available here: https://doi.org/10.17605/OSF.IO/H6M7N.
References
Ballou N, Zendle D (2022) “Clinically significant distress” in internet gaming disorder: an individual participant meta-analysis. Comput Hum Behav 129:107140
Barry C, McGinty E, Pescosolido B et al. (2014) Stigma, discrimination, treatment effectiveness, and policy: public views about drug addiction and mental illness. Psychiat Serv 65(10):1269–1272
Bax T (2013) Youth and internet addiction in China. Routledge, London
Beranuy M, Carbonell X, Griffiths M (2013) A qualitative analysis of online gaming addicts in treatment. Int J Ment Health Ad 11(2):149–161
Billieux J, Thorens G, Khazaal Y et al. (2015a) Problematic involvement in online games: a cluster analytic approach. Comput Hum Behav 43:242–250
Billieux J, Schimmenti A, Khazaal Y (2015b) Are we overpathologizing everyday life? A tenable blueprint for behavioral addiction research. J Behave Addict 4(3):119–123
Bleckmann P, Jukschat N (2015) The integrated model of (dys-) functionality: Reconstructing patterns of gaming as self-medication in biographical interviews with video game addicts. Forum: Qual Soc Res 16(3):Art. 8
Brand M, Rumpf HJ, King DL et al. (2020) Clarifying terminologies in research on gaming disorder and other addictive behaviors: distinctions between core symptoms and underlying psychological processes. Curr Opin Psych 1(36):49–54
Brooks J, McCluskey S, Turley E et al. (2015) The utility of template analysis in qualitative psychology research. Qual res psychol 12(2):202–222
Broyles L, Binswanger I, Jenkins J et al. (2014) Confronting inadvertent stigma and pejorative language in addiction scholarship: a recognition and response. Subst Abus 35(3):217–221
Carbonell X (2017) From Pong to Pokemon go, catching the essence of the Internet gaming disorder diagnosis: Commentary on: Chaos and confusion in DSM-5 diagnosis of Internet Gaming disorder: issues, concerns, and recommendations for clarity in the field (Kuss et al.). J Behave Addict 6(2):124–127
Colder Carras M, Kardefelt-Winther D (2018) When addiction symptoms and life problems diverge: a latent class analysis of problematic gaming in a representative multinational sample of European adolescents. Eur child adoles psy 27:513–525
Jeong EJ, Ferguson CJ, Lee SJ (2019) Pathological gaming in young adolescents: a longitudinal study focused on academic stress and self-control in South Korea. J Youth Adolesc 48(12):2333–2342
Kardefelt‐Winther D (2017) Conceptualizing internet use disorders: addiction or coping process? Psychiat Clin Neuros 71(7):459–466
Karhulahti VM (2022) Registered reports for qualitative research. Nat Hum Behav 2022 6(1):4–5
Király O, Sleczka P, Pontes HM et al. (2017) Validation of the ten-item Internet Gaming Disorder Test (IGDT-10) and evaluation of the nine DSM-5 Internet Gaming Disorder criteria. Addict behav 64:253–260
Langham E, Thorne H, Browne M (2015) Understanding gambling related harm: a proposed definition, conceptual framework, and taxonomy of harms. BMC Public Health 16(1):1–23
Lee S, Lee H, Choo H (2017) Typology of internet gaming disorder and its clinical implications. Psychiat Clin Neuros 71(7):479–491
Mosse D, Pocobello R, Saunders R et al. (2023) Introduction: open dialogue around the world–implementation, outcomes, experiences and perspectives. Front Cult Psychol 13:1093351
Musetti A, Mancini T, Corsano P et al. (2019) Maladaptive personality functioning and psychopathological symptoms in problematic video game players: a person-centered approach. Front Psychol 10:2559
Myrseth H, Notelaers G (2018) A latent class approach for classifying the problem and disordered gamers in a group of adolescence. Front Psychol 9:2273
Männikkö N, Ruotsalainen H, Tolvanen A et al. (2019) Psychometric properties of the Internet Gaming Disorder Test (IGDT‐10) and problematic gaming behavior among Finnish vocational school students. Scand J Psychol 60(3):252–60
Orford J (2001) Excessive appetites: a psychological view of addictions. Wiley, New York
Perales J, King DL, Navas JF et al. (2020) Learning to lose control: a process-based account of behavioral addiction. Neurosci Biobehav R 108:771–780
Puro JP, Karhulahti VM (2022) Hiljaa: Silent and slow media use. In: Herzogenrath B (ed.). Concepts. Bloomsbury Academic, London, pp. 143–152
Starcevic V, Choi TY, Kim TH et al. (2020) Internet gaming disorder and gaming disorder in the context of seeking and not seeking treatment for video-gaming. J Psychiat Res 129:31–39
Tao R, Huang X, Wang J et al. (2010) Proposed diagnostic criteria for internet addiction. Addiction 105(3):556–564
West R, Brown J (2013) Theory of addiction, 2nd edn. Addiction Press, New York
Xiao LY, Henderson LL, Newall PW (2022) Loot boxes are more prevalent in United Kingdom video games than previously considered: Updating Zendle et al. (2020). Addiction 117(9):2553–2555
Acknowledgements
The authors thank Peluuri and its program participants for the permission to utilize their valuable data for research. The authors also thank Matúš Adamkovič for assistance. VMK: Finnish Work Environment Fund (200349), Academy of Finland (312397), and European Research Council (ERC) under the European Union’s Horizon Europe research and innovation program (grant agreement No 101042052). LL: Technology Industries of Finland Centennial Foundation, Jane and Aatos Erkko Foundation, and Sigrid Juselius Foundation grants to J. Matias Palva. SB: no funding to declare.
Author information
Authors and Affiliations
Contributions
VMK conceptualized the study, methodology, and investigation. VMK acquired funding, created visuals, and carried out the synthesizing part of formal analysis. VMK wrote the original drafted and edited it. SB carried out original formal analysis, data curation, and validation. SB edited and reviewed the original draft. LL carried out original formal analysis and validation. LL edited and reviewed the original draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no relevant conflicts. For transparency, however, they wish to disclose that SB is the project manager of the Restart program, which was involved in generating the data. The Restart program is funded from the Finnish gambling monopoly company Veikkaus revenues through the Funding Centre for Social Welfare and Health Organisations (STEA) that operates under the Ministry of Social Affairs and Health. These funds did not support the present study. More than a decade ago, VMK was one of the co-founders and developers of the IGDB website, which is an open online database for various types of game knowledge. VMK never received salaries for that work, but when the website was turned into a company, he became a co-shareholder until a merger (2019) and has not been involved since. LL is researching a game-based digital intervention for depression at Aalto University.
Ethical approval
We consulted the local ethics committee and were advised not to utilize the ethics review process. According to Finnish Research Integrity guidelines, a study like this (existing data without personal identifiers) should not be submitted to ethics review.
Informed consent
Informed consent was obtained from all participants by Restart as part of the treatment application documents.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Karhulahti, VM., Behm, S. & Lukka, L. Why do adults seek treatment for gaming (disorder)? A qualitative study. Humanit Soc Sci Commun 10, 299 (2023). https://doi.org/10.1057/s41599-023-01775-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1057/s41599-023-01775-y
