
Abstract
Energy poverty (EPOV) is considered to have a significant impact on health and has become an essential issue on the policy agenda in most countries, especially those with rapid aging. Cognitive and mental health (CMH) for aging well is just as important a component as physical health, but the literature on the effect of EPOV on CMH is still rare. Using 2014–2018 China Family Panel Studies (CFPS), this study explores EPOV and its impacts on CMH among middle-aged and older adults. Six measures based on energy affordability are constructed to capture the state of EPOV. The results show that the proportion of middle-aged and older adults living in EPOV in China ranges from 24.3% to 27.8%, according to different measures. Applying a two-way FE model, the estimates show that overall, the impact of EPOV on CMH is significantly negative. Furthermore, physical health is an important channel through which EPOV affects CMH. Although EPOV has a significant adverse effect on the CMH of both middle-aged and older adults, it harms the latter more.
Similar content being viewed by others


Introduction
Poverty is not the mere lack of income to meet basic needs but multidimensional deprivations in basic human capabilities (Sen, 1995; Sen, 1999). Energy drives human life and is crucial for continued human development (Asif and Muneer, 2007). In the composition of poverty, energy-related deprivations are known as “energy poverty” (EPOV), which adversely affects people’s wellbeing (Awaworyi Churchill and Smyth, 2021; Llorca et al., 2020). EPOV is a global problem affecting both developing and developed countries. The International Energy Agency (IEA) states that nearly 1 billion people were still in EPOV in 2019 (IEA, 2019), and more than 100 million people who already had electricity connections will again rely on dirtier and less efficient energy sources in 2020 because they cannot afford basic electricity expenditure (IEA, 2020). In some countries, EPOV has been officially recognized as a distinct problem, separate from general poverty (Bednar and Reames, 2020). Many researchers have explored the negative impact of EPOV, especially on health (Banerjee et al., 2021; Bukari et al., 2021; Kahouli, 2020). Several of these studies point out that such impacts are more severe among older adults than others (Porto Valente et al., 2021). Considering the close correlation between EPOV and health (Bukari et al., 2021; Rafi et al., 2021), EPOV may become a severe challenge to healthy aging.
Population aging is associated with various societal impacts, especially health issues (Lin et al., 2010). Healthy aging is related to the quality of life of older adults and potentially lessens the burden on the whole society by reducing or delaying the need for economic support and elderly care (Smith et al., 2014). With the aging issues becoming severe, the studies increasingly emphasize the importance of health promotion targeting middle-aged and older adults (Elliott et al., 2021; Sun and Yang, 2021). A comprehensive understanding of the factors affecting the health of middle-aged and older adults is a prerequisite for health promotion. Cognitive and mental health (CMH), such as dementia and depression, are essential components of healthy aging. Taking dementia as an example, its annual cost in the United States is $109 billion, which remains the costliest of all diseases (Hurd et al., 2013). For the influencing factors of CMH, the current research mainly discusses gender (Zhao et al., 2021), cultural context (Haas et al., 2021), residential settings (Lee et al., 2019), family involvement (Hawkins et al., 2021), but rarely explores how EPOV affects CMH.
As the most populous country, China is facing severe challenges brought by population aging. According to the statistics of the National Bureau of Statistics of China (NBSC), the proportion of people over 60 years old increased from 10.27% to 18.70% in China (NBSC, 2021). Like many developed countries, China needs to implement health promotion interventions conducive to healthy aging, especially for CMH, to reduce the burden of aging. On the one hand, the rapid socioeconomic transition may lead to a decline in mental health (MH) among Chinese older adults, such as depression (Zeng, 2012), which are common and often neglected (Fang et al., 2015). On the other hand, the cognitive health (CH) of older adults in China is also not optimistic. In 2010, about 9.19 million people in China had dementia, and 5.69 million had Alzheimer’s disease (Chan et al., 2013). However, compared with physical health (PH), CMH in older adults receives less attention in China (Fang et al., 2015). Meanwhile, China is facing a severe challenge with EPOV. Some researchers have measured the incidence of EPOV in China, ranging from 22.6% to 41.3% (Nie et al., 2021; Zhang et al., 2019; Zhang et al., 2021b). Therefore, China provides a typical example to explore the impact of EPOV on CMH in the context of rapid aging.
Our research contributes to studies of the relationship between EPOV and CMH in the following aspects. Apart from being one of the first studies to use nationally representative data to investigate this relationship among middle-aged and older adults, this study also provides a rich set of EPOV measures regarding energy affordability. To our knowledge, only one recent research indicates that EPOV harms the MH of the head of household in China (Zhang et al., 2021b). However, our research differs significantly from Zhang et al. (2021b): First, our sample is mainly for people aged 45 and above, which helps obtain accurate information about the impact of EPOV on healthy aging. Second, based on the concept of healthy aging, PH, CH, and MH are put into the same framework to explore the comprehensive effects of EPOV on the health status of middle-aged and older adults. Third, unlike the EPOV measure based on energy availability in Zhang et al. (2021b), we measure EPOV from the perspective of energy affordability, which is more in line with the actual situation in China. Fourth, we use panel data instead of cross-sectional data, which makes the conclusion more accurate and enables more informative discussion, such as the lag effect of EPOV.
The rest of this research is as follows. Section “Literature review” presents relevant literature on the concept and measure of EPOV, EPOV-CMH association, and its potential mechanism. Data sources, variables definitions, and empirical strategies are discussed in Section “Methodology”. Empirical results are reported in Section “Results”. Section “Conclusion” summarizes our research.
Literature review
The concept and measure of EPOV
The concept of EPOV was first put forward in 1982 (Lewis, 1982). There are many definitions of EPOV, but most believe that EPOV is a state that does not meet people’s energy consumption needs (Bukari et al., 2021; Druică et al., 2019; Nie et al., 2021; Rafi et al., 2021). According to Reddy (2000), EPOV is considered to be “the absence of sufficient choice in accessing adequate, affordable, reliable, high quality, safe and environmentally benign energy services to support economic and human development.” This definition is selected here because it not only includes the absence of sufficient choice in accessing energy services, which meets the deprivations in human capabilities, but also describes the observable characteristics of energy services, including availability, affordability, reliability, high quality, safety, and environmental friendliness (González-Eguino, 2015).
Among these characteristics proposed by Reddy (2000), researchers often use energy availability and affordability to measure EPOV. Some studies emphasized the importance of energy availability (Acheampong et al., 2021; Pan et al., 2021; Poblete-Cazenave and Pachauri, 2021; Zhang et al., 2021a). They construct some representative indicators, such as the use of electricity or other fuels and the use of household appliances to measure EPOV. Some studies focus on energy affordability, measuring EPOV by the proportion of household energy consumption. The earliest studies set the threshold of energy expenditure at 10% of household income (Legendre and Ricci, 2015; Mould and Baker, 2017). As this field of research continues to grow, several studies employ improved measures to suit local conditions and energy costs in different regions (Koomson and Danquah, 2021; Prakash and Munyanyi, 2021). We summarize some widely used EPOV measures in Table 1.
However, different countries have different performances in EPOV (Awaworyi Churchill and Smyth, 2021; Zhang et al., 2019; Rafi et al., 2021; Phoumin and Kimura, 2019). Some countries are still striving to achieve universal energy access, while others have already achieved this goal and need to focus on energy affordability. Thus, when choosing the specific EPOV measure, the research object’s actual situation must be considered. Considering that China’s electrical access has reached 100% since 2013 (World Bank, 2020), and energy infrastructure in backward areas has been improved after China’s poverty alleviation policy. The problem of energy accessibility in China has been roughly solved. Therefore, energy affordability is more representative of EPOV than energy availability in China.
Impacts of EPOV on CMH
Many researchers have analyzed the linkage between EPOV and health, but direct evidence for the effect of EPOV on CMH is still rare. A small body of extant research provides evidence of EPOV’s detrimental effects on MH. For instance, Shupler et al. (2022), drawing on data from Africa, find that eliminating EPOV helps reduce the probability of depression in women. Mould and Baker (2017) conduct fifteen case studies in Scotland and find that EPOV can lead to MH problems, such as depression and anxiety. Similarly, Zhang et al. (2019) use household-level survey data from the China Family Panel Studies further confirm a statistically significant and robust negative impact on MH from EPOV.
Fortunately, various studies provide indirect evidence for the effect of EPOV on CMH. On the one hand, some researchers provide evidence on the linkage between EPOV and academic achievement, one of the common indicators representing cognitive function (Pascoe et al., 2021). Rafi et al. (2021) research Indian children and find that EPOV harms children’s academic achievements. Based on the data from 50 developing countries, Banerjee et al. (2021) find that lower EPOV can bring higher educational outcomes. On the other hand, some researchers have studied the influence of EPOV on subjective wellbeing, which is closely related to MH (Okbay et al., 2016). For instance, Phoumin and Kimura (2019) use survey data from Cambodia to find that EPOV lowers subjective wellbeing. Using data from 13 waves of the Household, Income and Labour Dynamics in Australia (HILDA) survey, Awaworyi Churchill et al. (2020) link EPOV with poor subjective wellbeing. Nie et al. (2021) conduct the same research in China, supporting the above conclusions.
The mediating role of PH
To explore the potential channel between EPOV and CMH, we tested the mediating role of PH. The impact of EPOV on PH is widely discussed. Most researchers suggest that EPOV has a negative effect on the PH. Specifically, these households living in EPOV may turn to alternative energy sources to meet their daily energy needs. Some researchers find that these alternative energy sources are usually of poor quality, and may emit toxic gases and damage body functions, leading to chronic diseases and other health problems (Lacroix and Chaton, 2015; Sharpe et al., 2015). Meanwhile, due to financial constraints, many households need to trade between adequate nutrition and energy services, leading to the “heat or eat” dilemma (Anderson et al., 2012). Some of them may limit their energy costs to avoid debt from energy consumption (Awaworyi Churchill et al., 2020), resulting in insufficient energy use and affecting their health. With limited literature, EPOV is also confirmed to have a negative impact on food expenditure (Nie et al., 2021), and inadequate food intake ultimately affects health.
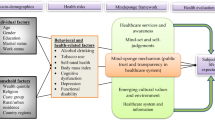
The correlation between PH and CMH has been widely discussed, especially among older adults (Kivimäki and Livingston, 2022; Kubzansky et al., 2018; Yang and D’Arcy, 2022). Human function deteriorates with age, which in turn affects CMH (Walston et al., 2006). On the one hand, PH is significantly related to MH (Kubzansky et al., 2018). The probability of suffering from chronic diseases increases with age, and chronic diseases negatively affect MH (Yang and D’Arcy, 2022). On the other hand, PH also has significant effects on CH. For instance, Kivimäki and Livingston (2022) find that poor PH significantly increases the long-term risk of Alzheimer’s disease. Therefore, EPOV may have an indirect effect on CMH by affecting PH. Considering that both CMH and PH are important components of healthy aging, we attempt to put them into the same framework to explore the comprehensive effects of EPOV on the health status of middle-aged and older adults. Fig. 1 shows a simple heuristic of the above factors as a possible mechanism by which EPOV affects CMH among middle-aged and older adults in China.

The mechanism of the impact of EPOV on the health of middle-aged and older adults.
Methodology
Data
The data of this paper comes from a nationally representative survey in China, China Family Panel Studies (CFPS), conducted by the Institute of Social Science Survey of Peking University. The survey collects data from the individual, household, and community levels, covering all members of 16,000 households in 25 provincial administrative units, including detailed information on various aspects of China, such as culture, economy, education, and healthcare. Many previous studies use CFPS data to explore China issues, including EPOV (Nie et al., 2021; Zhang et al., 2021a) and CMH (Gao et al., 2021; Xue et al., 2019), have verified the validity of the database. CFPS has disclosed five waves of data, but the details about energy related to our research only have been collected since 2014. Therefore, three waves are used in this study: 2014, 2016, and 2018. Considering that our research targets are middle-aged and older adults, we limit the sample age to 45 years old and above. To focus on energy affordability, we delete the samples using cheap solid fuels and those with an income of 0. Finally, the analysis unit in this study is individual. We obtain an unbalanced panel of 19,664 individuals from 11,108 households. Among all individuals, 9972 individuals span all three waves, and 4319 individuals appear in only one. So we obtain 44,981 individual observations.
Variables
Measures of CH and MH
Memory is an important component of cognitive function in older adults (Shin, 2021). Many studies on the CH of older adults regard memory as a crucial criterion for evaluating cognitive function (Ahn et al., 2021; Zhao et al., 2021). Our main proxy of CH is memory. This indicator is selected from the question, “to what extent can you remember the main things that happened to you in a week”. Responses are scored on a 5-point scale, from 1 (I can only remember a little) to 5 (I can remember anything). In addition, some researchers use academic test scores to measure CH (Gao et al., 2021; Zhang et al., 2018). Therefore, we introduce mathematics and verbal test scores into the robustness test as another measure of CH.
The measure of MH is based on a series of indicators. Consistent with the previous literature to measure MH (Ao et al., 2021; Jiang et al., 2020), we select six indicators to measure comprehensively, all of which belong to the 10-item Center for Epidemiologic Studies Depression (CES-D) scale for older adults (Andresen et al., 1994). These indicators are selected from the question “the frequency of your feelings or behaviors in the past week”, involving six aspects: depressed, hard to do things, sleepless, lonely, sad, and cannot go on with life. Scale responses are made on a 4-point rating scale, from 1 (5–7 days), 2 (3–4 days), 3 (1–2 days), to 4 (less than 1 day). We take the average of these indicators as a measure of MH. In the robustness test, we use satisfaction and happiness as another measure of MH.
Measures of EPOV
We adopt six different measures based on energy affordability to evaluate EPOV. Consistent with the current research, our multiple measures of EPOV are based on the proportion of energy consumption to household income (Awaworyi Churchill et al., 2020; Farrell and Fry, 2021; Nie et al., 2021; Pan et al., 2021; Zhang et al., 2021a). Since the energy consumption of one household is shared, we measure the EPOV at the household level and allocate this value to each individual sample according to the household ID. According to the items in the questionnaire, energy consumption is a summary of the amount of annual spending on household energy. The specific measure methods are as follows:
Our first measure of EPOV (EPOV1) is a commonly used method, regarding EPOV as the standard that the proportion of energy expenditure in income exceeds a certain threshold. The most widely used measure proposed by Boardman (1991) in the book “Fuel Poverty: From Cold Homes to Affordable Warmth”, which defines EPOV as the situation where energy consumption accounts for 10% of income. Following this definition, EPOV1 depends on whether energy expenditure is greater than 10% of income.
However, many researchers point out that the 10% standard of Boardman (1991) may lead to the misjudgment of EPOV (Farrell and Fry, 2021; Kahouli, 2020; Lin and Wang, 2020). Some vulnerable people may ration energy expenditure to avoid debt caused by energy consumption (Awaworyi Churchill et al., 2020). To improve measuring accuracy, Kahouli (2020) proposes the amended 10% measure, which only targets the low-income people in the last three deciles of the income distribution. Referring to the amended 10% measure proposed by Kahouli (2020), the second measure of EPOV (EPOV2) is mainly aimed at the low-income population whose income is in the bottom 50% of the total distribution.
In addition to taking fixed values like 10% as recognition thresholds, some researchers measure EPOV according to the median percentage level. For example, Moore (2012) proposes using a double median percentage to identify EPOV. Nie et al. (2021) adopt this measure in their research. Therefore, we define the third measure of EPOV (EPOV3) as twice the median ratio of energy consumption to income in the total sample. Further, we construct the fourth measure of EPOV (EPOV4) due to possible regional differences. The identification standard of EPOV4 is a double median percentage of the province where the sample is located.
Referring to the idea of “low-income-high-cost (LIHC)” by Hills (2011), the fifth measure of EPOV (EPOV5) combines energy consumption with residents’ income level. This measure eliminates the situation in which people with high energy consumption and income are identified as EPOV (Li et al., 2014). According to this measure, we select the sample whose income level is at the bottom 25% of the total as the low-income group and regard those whose energy consumption exceeds the median as EPOV5.
The sixth measure of EPOV (EPOV6) is the comprehensive generation from EPOV1 to EPOV5. The score of EPOV6 is between 0 and 1, which is expressed as:
where αi is the weight corresponding to EPOVi. Owing to the lack of evidence to judge the importance of each measure, we adopt an equal weighting method for the above measures according to Awaworyi Churchill et al. (2020), i.e., αi = 1/5. EPOV6 is the main research object in this paper, and the other five measures are used for robustness checks. Nie et al. (2021), Phoumin and Kimura (2019) also adopt this method to measure EPOV.
Control variables
Referring to previous relevant studies, we control a series of variables that may affect EPOV-CMH relation (see, e.g., Awaworyi Churchill and Smyth (2021); Nie et al. (2021); Prakash and Munyanyi (2021)). This paper selects the control variables of age, gender, education levels, employment status, training frequency, social status, marital status, and Hukou (registered residence location). Details of the variables in this study are shown in Table 2.
Empirical strategy
Considering the possible deviation of individual time-invariant unobservables, the effect of EPOV on CMH is estimated by a two-way FE model as follows:
where CHit is the scores of CH of individual i at time t; MHit is the scores of MH of individual i at time t; EPOVit stands for EPOV; Xit is a series of control variables at the individual level, such as education level and gender; Pi and Yt represent provincial and year dummies, respectively; δit refers to error term; μi reflects the unobservable time-invariant individual effects; β indicates the relationship between CMH and related variables.
For our baseline, using FE estimators may create endogenous problems caused by omitted variables, reverse causation, sample selection bias, measurement errors, and other factors. Since FE estimation cannot eliminate the potential time-varying unobserved factors simultaneously affecting both EPOV and CMH, it may lead to bias in the estimation coefficient of EPOV. Some studies demonstrate the reverse causality between EPOV and types of health (e.g., PH and MH) (Awaworyi Churchill and Smyth, 2021; Zhang et al., 2019; Zhang et al., 2021b). We adopt two-stage-squares (2SLS) estimations to address this concern by taking the average of EPOV at the provincial level as an instrumental variable (IV). In previous studies, the provincial average is proved to be a valid IV of EPOV (Zhang et al., 2021b). The logic is that people in the same province have similar income and living habits and enjoy the semblable municipal services and infrastructure. Therefore, the provincial average of EPOV is closely related to individual EPOV. Meanwhiles, residents’ CMH status is usually influenced by personal or family factors (Ang, 2021) and has an inappreciable relation with the provincial average of EPOV at the macro level.
Results
Descriptive statistics
As shown in Table 2, the average scores of CH and MH of the middle-aged and older adults in our sample are 2.975 and 3.410, respectively. The proportion of the sample in EPOV ranges from 24.3% to 27.8%, according to different measures of EPOV. In terms of the demographics, the average age of the sample is 60.133, and the proportion of men and women is balanced (men account for 49.5%). In terms of the highest level of education received by the sample, primary school is the most (33.3%), followed by middle school (23.3%), and then high school (19.3%). 13.5% of the sample are illiterate. Those with the highest degrees in vocational school and university or higher are the least, 8.2% and 2.4%, respectively. On average, respondents exercise 2.57 times per week. In the total sample, 60.4% of the respondents are employed, 86.7% are married, and 46% have urban hukou. The average self-reported score of respondents on their current social status is 3.083, which is at a relatively medium level.
The spatial distribution of EPOV in 2014, 2016, and 2018 is shown in Fig. 2. Overall, EVOP shows a downward trend year by year. In 2014 and 2016, the EPOV in the eastern provinces is lower than that in the central and western regions, especially in the Yangtze River Delta (i.e., Shanghai, Zhejiang, Jiangsu, and Anhui). The possible reason for this is that the socioeconomic conditions of the provinces in the Yangtze River Delta are more prosperous than in other provinces. In 2018, EPOV has been better improved nationwide. Among the 25 provincial administrative units included in the statistics, 18 provinces have EPOV lower than 25%, accounting for 72% of the total.

The spatial distribution of EPOV in 2014, 2016, and 2018.
Figures 3 and 4 show the average CH and MH scores of samples with and without EPOV under six different EPOV measures, respectively. It can be seen that from EPOV1 to EPOV5, the samples living in EPOV scored lower than those not living in, regardless of MH and CH.

EPOV1-EPOV6 represent six different EPOV measures. Higher scores represent better CH status.

EPOV1-EPOV6 represent six different EPOV measures. Higher scores represent better MH status.
Baseline results
The baseline results of EPOV6 on CMH are shown in Table 3. We first use ordinary least squares (OLS) estimators to examine the relationship between EPOV6 and CMH. As reported in columns (1) and (4), the coefficients of EPOV6 are both significant at magnitudes of −0.213 and −0.146, denoting that EPOV significantly negatively affects CMH. Then we add various control variables in columns (2) and (5). The inclusion of provincial and year dummies decreases the effects of EPOV but remains consistent with the results in columns (1) and (4). The results of FE estimators are shown in columns (3) and (6). Comparing the results of these six columns makes it not difficult to find that the FE estimate of EPOV6-associated effects on CMH is smaller than the OLS estimate. The difference in results may be because the FE estimators control the time-invariant individual fix effects, alleviating part of the endogeneity of EPOV caused by ignoring unobserved factors. Overall, all regression results of baseline regression display that EPOV is related to low CMH scores. Our results are consistent with previous studies (Lin and Okyere, 2020; Mohan, 2022; Zhang et al., 2021b).
Endogeneity corrected results
Considering that the endogeneity of EPOV6 may lead to deviation in the analysis results, we take the provincial average of EPOV6 as the instrumental variable and use the 2SLS method for robustness tests. Table 4 displays the estimates of 2SLS and the related first-stage diagnostic test results. The F-statistics calculated in the first stage are larger than 10 in all regression, suggesting that the IV is not weakly associated with EPOV6 (Stock and Yogo, 2005). After correcting for endogeneity, we find that the relationship between EPOV6 and CMH is still significantly negative. Further, we employ FE-IV estimators for robustness tests and get a similar consequence. Admittedly, the bias-corrected estimates from both 2SLS and FE-IV models are larger than the baseline estimates across CH and MH, indicating that the baseline estimates are downward biased. This is consistent with Prakash and Munyanyi (2021) results on the impact of EPOV on obesity using Australian data. Earlier studies from China also report that the bias-corrected estimates are higher than the baseline results when detecting the impacts of EPOV on health and subjective wellbeing (Nie et al., 2021; Zhang et al., 2021a; Zhang et al., 2021b). Hence, we conclude that EPOV has significant adverse effects on CMH.
Robustness checks
Considering the sensitivity of the research results, we examine a series of robust checks. Firstly, we test the robustness of the results under alternative EPOV measures, using EPOV1–EPOV5 to replace the EPOV6, respectively (see Table 5). Panel A is the results of the impacts of different EPOV measure standards on MH, and Panel B is the impacts on CH. The results in Table 5 indicate the negative impacts of EPOV on CMH, which are consistent with the baseline estimates.
Second, we measure CH and MH in alternative ways. Some researchers select standardized verbal tests and math tests from CFPS to measure CH (Gao et al., 2021; Zhang et al., 2018). Specifically, the test score depends on the most difficult question that the respondent can answer. The higher the test score, the better the CH of the respondent. Meanwhiles, researchers use positive measures, such as happiness and life satisfaction, to represent MH (Awaworyi Churchill et al., 2020; Druică et al., 2019; Nie et al., 2021; Zhang et al., 2021a). Life satisfaction and happiness show people’s thoughts and feelings about life (Pénard et al., 2013), reflecting on their mental situation. The CFPS asks respondents “how happy are you” on a scale of 10 (not happy at all = 1, very happy = 10) and “are you satisfied with your life” with a 5-point scale (not satisfied at all = 1, very satisfied = 5). Therefore, we introduce four CMH proxies of happiness, satisfaction, mathematics test score, and verbal test score. Since the questionnaires of the above four variables are various in different survey waves, we only employ OLS estimators to test the robustness based on the data of 2018 CFPS. The results reported in Table 6 also support the conclusion that EPOV significantly negatively impacts CMH.
Mechanisms and further investigations
This section further explores whether PH is a channel through which EPOV affects CMH. To conduct this investigation, we introduce the indicator: self-reported health. In the CFPS, respondents need to answer questions related to this: “how is your health” with a five-point scale (very unhealthy = 1, very healthy = 5). Self-reported health (SRH) has been widely used as a proxy variable for PH (Awaworyi Churchill and Smyth, 2021; Kahouli, 2020; Nie et al., 2021). We adopt a two-step procedure that is frequently used in earlier studies (Koomson and Danquah, 2021; Zhang et al., 2021a). The results are shown in Table 7.
In the first step, we examine whether potential channels are related to EPOV. The results of Panel A indicate that increased EPOV reduces the self-reported health level (see columns (2) and (5)). As expected, EPOV significantly negatively affects PH, suggesting that it is difficult for middle-aged and older adults with EPOV to have good PH. Our findings are well in accordance with those of Oliveras et al. (2020) for Spain, Zhang et al. (2019) for China, Oum (2019) for Lao PDR. After measuring the correlation between PH and EPOV, we included PH as an additional covariate in the baseline regression in the second step (see columns (3) and (6)). We find that self-reported health is positively related to both CH and MH, manifesting that PH has a significant positive impact on CMH. Moreover, after taking self-reported health as an additional covariate, the absolute values of EPOV coefficients on both CH and MH decrease, indicating that self-reported health is a mediator of EPOV affecting CMH. Overall, the results of this section suggest that PH is a channel through which EPOV affects CMH.
Considering that there may be a lag or delay in the impact of EPOV on CMH, we discuss the lagged effects of EPOV on CMH in Table 8. To conduct this investigation, we remove the samples with interruptions in the tracking survey and convert the unbalanced panel data into balanced panel data. Column (1) shows the contemporary effect of EPOV6 on CH in time t, and columns (2) and (3) report the lagged effects in time t – 1 and t – 2. Our result suggests that EPOV6 significantly negatively impacts CH in time t – 1, but not in time t – 2. To capture the cumulative impact of EPOV6 on CH, we then include EPOV from time t to time t – 2 in the same regression (see column (4)). The results show that the coefficients of EPOV6 in time t and t – 1 are significantly negative. The above results indicate that EPOV not only has a negative impact on CH in the current period but also has a continuous impact. Similar consequences are found in MH, indicating that both current and periods EPOV status have significant negative impacts on MH. Obviously, the magnitudes of the total impacts of the current period and the previous periods are substantially greater than the effect estimated using the current period alone, indicating that earlier studies may underestimate the negative impacts of EPOV on CMH and even general health.
Next, we further investigate the effects of EPOV on different sub-groups. Many studies have shown that EPOV has diversified effects on different age groups (Awaworyi Churchill and Smyth, 2021; Prakash and Munyanyi, 2021). Considering that the health of older adults is more vulnerable to external influence than the middle-aged (Liu et al., 2021), we divide the sample into the middle-aged group and the older adults group for in-depth analysis. According to the Law on the Protection of the Rights and Interests of older adults in China, all residents over the age of 60 belong to older adults. In Table 9, we explore the different effects of EPOV on CMH of respondents whether they are older than 60 years old. The results show that the impact of EPOV6 on CMH is a significant negative for both middle-aged and older adults. However, the magnitude of the EPOV6 coefficient of the middle-aged subgroup is relatively small. The seemingly unrelated estimation test is used to test for age differences in the coefficients between models using Wald chi-squared tests (Weesie, 2000). We find a significant difference between middle-aged and older adults for MH (χ2 = 5.95, p = 0.01), but no significant difference for CH (χ2 = 0.08, p = 0.78). This result indicates that the negative impact of EPOV on older adults is more severe, which is consistent with Nie et al. (2021) that the middle-aged generally have better socioeconomic status to address potential health challenges posed by EPOV.
Conclusion
Population aging is a global issue. Health promotion targeting middle-aged and older adults is a critical way to deal with aging, which requires a comprehensive understanding of the factors affecting the health of middle-aged and older adults. EPOV is a global problem in both developing and developed countries, and is considered to have a significant impact on health. Although researchers have paid much attention to the detrimental effects of EPOV on health, there are few empirical studies on the effects of EPOV on CMH in middle-aged and older adults. We use nationally representative data from the 2014–2018 CFPS to provide insights into EPOV-CMH relations among middle-aged and older adults.
The analysis yields several key findings: First, the proportion of middle-aged and older adults living in EPOV in China ranges from 24.3% to 27.8%, according to different measures based on energy affordability, which indicates that there are still a large number of middle-aged and older adults facing the challenge of energy affordability. Second, EPOV has a significantly negative effect on CMH, and the effect is persistent. These results are robust to various robustness tests. PH is confirmed to be an important channel through which EPOV affects CMH. Finally, EPOV has greater negative impacts on older adults than on the middle-aged, which suggests the importance of preventing the influence of EPOV on CMH in health promotion. These findings provide incremental information for promoting healthy aging in China. Eliminating EPOV can not only improve the current CMH status of middle-aged and older adults, but also prevent them from CMH problems due to insufficient use of energy services.
The study’s conclusion echoes previous studies and has important implications for policy. Although the problem of extreme poverty has been alleviated, China still faces the challenge of multidimensional poverty represented by EPOV. To solve the challenge of EPOV, policymakers should shift the focus from energy availability to energy affordability. Considering the differences in the incidence of EPOV across provinces, policymakers can implement differentiated policies based on local conditions. On the one hand, policymakers can develop local renewable energy sources, reducing the energy cost for residents. For example, solar and wind energy resources are rich in northwest China, and hydropower resources are abundant in southwest China. On the other hand, policymakers can reduce the incidence of EPOV by improving the housing structure, and reducing residents’ electricity consumption of energy devices, such as air conditioners.
Moreover, the government can reduce energy prices through market-oriented reforms (Ren et al., 2022), and solve the problem of EPOV through accurate identification and targeted energy subsidies, especially for middle-aged and older adults who lack competitiveness in the labor market. Since solving EPOV is not an overnight solution, the government should pay attention to the changes in the CMH of middle-aged and older adults while improving their energy affordability, and take various measures to improve their CMH. For example, the government can conduct regular visits to households in EPOV to understand their CMH status, and provide appropriate assistance, such as financial assistance and psychological support, to those at risk of CMH deterioration. It is hoped that this study can inspire future researchers interested in EPOV, CMH, and aging. Future studies can further explore the different mechanisms of EPOV’s impacts on CMH.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Acheampong AO, Erdiaw-Kwasie MO, Abunyewah M (2021) Does energy accessibility improve human development? Evidence from energy-poor regions. Energy Econ 96:105165. https://doi.org/10.1016/j.eneco.2021.105165
Ahn S, Mathiason MA, Lindquist R et al. (2021) Factors predicting episodic memory changes in older adults with subjective cognitive decline: A longitudinal observational study. Geriatr Nurs (Minneap) 42(1):268–275. https://doi.org/10.1016/j.gerinurse.2020.08.016
Andresen EM, Malmgren JA, Carter WB et al. (1994) Screening for depression in well older adults: evaluation of a short form of the CES-D. Am J Prev Med 10(2):77–84. https://doi.org/10.1016/s0749-3797(18)30622-6
Anderson W, White V, Finney A (2012) Coping with low incomes and cold homes. Energy Policy 49:40–52. https://doi.org/10.1016/j.enpol.2012.01.002
Ang S (2021) Your friends, my friends, and our family: Informal social participation and mental health through the lens of linked lives. Soc Sci Med 276:113848. https://doi.org/10.1016/j.socscimed.2021.113848
Ao CK, Dong Y, Kuo PF (2021) Industrialization, indoor and ambient air quality, and elderly mental health. China Econ Rev 69:101676. https://doi.org/10.1016/j.chieco.2021.101676
Asif M, Muneer T (2007) Energy supply, its demand and security issues for developed and emerging economies. Renew Sustain Energy Rev 11(7):1388–1413. https://doi.org/10.1016/j.rser.2005.12.004
Awaworyi Churchill S, Smyth R (2021) Energy poverty and health: panel data evidence from Australia. Energy Econ 97:105219. https://doi.org/10.1016/j.eneco.2021.105219
Awaworyi Churchill S, Smyth R, Farrell L (2020) Fuel poverty and subjective wellbeing. Energy Econ 86:104650. https://doi.org/10.1016/j.eneco.2019.104650
Banerjee R, Mishra V, Maruta AA (2021) Energy poverty, health and education outcomes: Evidence from the developing world. Energy Econ 101:105447. https://doi.org/10.1016/j.eneco.2021.105447
Bednar DJ, Reames TG (2020) Recognition of and response to energy poverty in the United States. Nat Energy 5(6):432–439. https://doi.org/10.1038/s41560-020-0582-0
Boardman B (1991) Fuel poverty: from cold homes to affordable warmth. Belhaven Press, London
Bukari C, Broermann S, Okai D (2021) Energy poverty and health expenditure: evidence from Ghana. Energy Econ 103:105565. https://doi.org/10.1016/j.eneco.2021.105565
Chan KY, Wu JJ, Liu L et al. (2013) Epidemiology of Alzheimer’s disease and other forms of dementia in China, 1990-2010: a systematic review and analysis. Lancet 381(9882):2016–2023. https://doi.org/10.1016/S0140-6736(13)60221-4
Druică E, Goschin Z, Ianole-Călin R (2019) Energy poverty and life satisfaction: structural mechanisms and their implications. Energies 12(20):3988. https://doi.org/10.3390/en12203988
Elliott M, Jones J, Elliott Melissa et al. (2021) Expanding arts therapies provision: a pilot project in Older Adult Mental Health Services, Aneurin Bevan University Health Board. Public Health 194:270–273. https://doi.org/10.1016/j.puhe.2021.01.013
Fang EF, Scheibye-Knudsen M, Jahn HJ et al. (2015) A research agenda for aging in China in the 21st century. Ageing Res Rev 24:197–205. https://doi.org/10.1016/j.arr.2015.08.003
Farrell L, Fry JM (2021) Australia’s gambling epidemic and energy poverty. Energy Econ 97:105218. https://doi.org/10.1016/j.eneco.2021.105218
Gao H, Shi J, Cheng H et al. (2021) The impact of long- and short-term exposure to different ambient air pollutants on cognitive function in China. Environ Int 151:106416. https://doi.org/10.1016/j.envint.2021.106416
González-Eguino M (2015) Energy poverty: an overview. Renew Sustain Energy Rev 47:377–385. https://doi.org/10.1016/j.rser.2015.03.013
Haas BW, Hoeft F, Omura K (2021) The role of culture on the link between worldviews on nature and psychological health during the COVID-19 pandemic. Pers Individ Dif 170:110336. https://doi.org/10.1016/j.paid.2020.110336
Hawkins M, Misra D, Zhang L et al. (2021) Family involvement in pregnancy and psychological health among pregnant Black women. Arch Psychiatr Nurs 35(1):42–48. https://doi.org/10.1016/j.apnu.2020.09.012
Hills J (2011) Fuel poverty: the problem and its measurement. Department for Energy and Climate Change, London
Hurd MD, Martorell P, Langa KM (2013) Monetary costs of dementia in the United States. N Engl J Med 369(5):489–490. https://doi.org/10.1056/nejmc1305541
IEA (2020) World Energy Outlook 2020. IEA, Paris
IEA (2019) World Energy Outlook 2019. IEA, Paris
Jiang W, Lu Y, Xie H (2020) Education and mental health: evidence and mechanisms. J Econ Behav Organ 180:407–437. https://doi.org/10.1016/j.jebo.2020.09.032
Kahouli S (2020) An economic approach to the study of the relationship between housing hazards and health: the case of residential fuel poverty in France. Energy Econ 85:104592. https://doi.org/10.1016/j.eneco.2019.104592
Kivimäki M, Livingston G (2022) Health conditions linked to heightened risk of Alzheimer’s disease. Lancet Digit Heal 4(3):e150–e151. https://doi.org/10.1016/S2589-7500(21)00293-4
Koomson I, Danquah M (2021) Financial inclusion and energy poverty: empirical evidence from Ghana. Energy Econ 94:105085. https://doi.org/10.1016/j.eneco.2020.105085
Kubzansky LD, Huffman JC, Boehm JK et al. (2018) Positive psychological well-being and cardiovascular disease. J Am Coll Cardiol 72(12):1382–1396. https://doi.org/10.1016/j.jacc.2018.07.042
Lacroix E, Chaton C (2015) Fuel poverty as a major determinant of perceived health: the case of France. Public Health 129(5):517–524. https://doi.org/10.1016/j.puhe.2015.02.007
Lee EE, Martin AS, Kaufmann CN et al. (2019) Comparison of schizophrenia outpatients in residential care facilities with those living with someone: study of mental and physical health, cognitive functioning, and biomarkers of aging. Psychiatry Res 275:162–168. https://doi.org/10.1016/j.psychres.2019.02.067
Legendre B, Ricci O (2015) Measuring fuel poverty in France: which households are the most fuel vulnerable. Energy Econ 49:620–628. https://doi.org/10.1016/j.eneco.2015.01.022
Lewis P (1982) Fuel poverty can be stopped. National Right to Fuel Campaign, Bradford
Li K, Lloyd B, Liang XJ et al. (2014) Energy poor or fuel poor: What are the differences? Energy Policy 68:476–481. https://doi.org/10.1016/j.enpol.2013.11.012
Lin B, Okyere MA (2020) Multidimensional energy poverty and mental health: micro-level evidence from Ghana. Int J Environ Res Public Health 17(18):6726. https://doi.org/10.3390/ijerph17186726
Lin B, Wang Y (2020) Does energy poverty really exist in China? From the perspective of residential electricity consumption. Energy Policy 143:111557. https://doi.org/10.1016/j.enpol.2020.111557
Lin MH, Chou MY, Liang CK et al. (2010) Population aging and its impacts: strategies of the healthcare system in Taipei. Ageing Res Rev 9:S23–S27. https://doi.org/10.1016/j.arr.2010.07.004
Liu Y, Lu S, Guo Y et al. (2021) Longitudinal associations between neighbourhood physical environments and depressive symptoms of older adults in Hong Kong: the moderating effects of terrain slope and declining functional abilities. Health Place 70:102585. https://doi.org/10.1016/j.healthplace.2021.102585
Llorca M, Rodriguez-Alvarez A, Jamasb T (2020) Objective vs. subjective fuel poverty and self-assessed health. Energy Econ 87:104736. https://doi.org/10.1016/j.eneco.2020.104736
Mohan G (2022) The impact of household energy poverty on the mental health of parents of young children. J Public Health (Bangkok) 44(1):121–128. https://doi.org/10.1093/pubmed/fdaa260
Moore R (2012) Definitions of fuel poverty: implications for policy. Energy Policy 49:19–26. https://doi.org/10.1016/j.enpol.2012.01.057
Mould R, Baker KJ (2017) Documenting fuel poverty from the householders’ perspective. Energy Res Soc Sci 31:21–31. https://doi.org/10.1016/j.erss.2017.06.004
NBSC (2021) Press conference on the main data results of the Seventh National Population Census. http://www.stats.gov.cn/ztjc/zdtjgz/zgrkpc/dqcrkpc/ggl/202105/t20210519_1817702.html. Accessed 2 Oct 2021
Nie P, Li Q, Sousa-Poza A (2021) Energy poverty and subjective well-being in China: New evidence from the China Family Panel Studies. Energy Econ 103:105548. https://doi.org/10.1016/j.eneco.2021.105548
Okbay A, Baselmans B, De Neve JE et al. (2016) Genetic variants associated with subjective well-being, depressive symptoms, and neuroticism identified through genome-wide analyses. Nat Genet 48(6):624–633. https://doi.org/10.1038/ng.3552
Oliveras L, Artazcoz L, Borrell C et al. (2020) The association of energy poverty with health, health care utilisation and medication use in southern Europe. SSM Popul Heal 12:100665. https://doi.org/10.1016/j.ssmph.2020.100665
Oum S (2019) Energy poverty in the Lao PDR and its impacts on education and health. Energy Policy 132:247–253. https://doi.org/10.1016/j.enpol.2019.05.030
Pan L, Biru A, Lettu S (2021) Energy poverty and public health: Global evidence. Energy Econ 101:105423. https://doi.org/10.1016/j.eneco.2021.105423
Pascoe L, Burnett AC, Anderson PJ (2021) Cognitive and academic outcomes of children born extremely preterm. Semin Perinatol 45(8):151480. https://doi.org/10.1016/j.semperi.2021.151480
Pénard T, Poussing N, Suire R (2013) Does the Internet make people happier? J Socio Econ 46:105–116. https://doi.org/10.1016/j.socec.2013.08.004
Phoumin H, Kimura F (2019) Cambodia’s energy poverty and its effects on social wellbeing: Empirical evidence and policy implications. Energy Policy 132:283–289. https://doi.org/10.1016/j.enpol.2019.05.032
Poblete-Cazenave M, Pachauri S (2021) A model of energy poverty and access: Estimating household electricity demand and appliance ownership. Energy Econ 98:105266. https://doi.org/10.1016/j.eneco.2021.105266
Porto Valente C, Morris A, Wilkinson SJ (2021) Energy poverty, housing and health: the lived experience of older low-income Australians. Build Res Inf 50(1–2):6–18. https://doi.org/10.1080/09613218.2021.1968293
Prakash K, Munyanyi ME (2021) Energy poverty and obesity. Energy Econ 101:105428. https://doi.org/10.1016/j.eneco.2021.105428
Rafi M, Naseef M, Prasad S (2021) Multidimensional energy poverty and human capital development: empirical evidence from India. Energy Econ 101:105427. https://doi.org/10.1016/j.eneco.2021.105427
Reddy A (2000) Energy and social issues. Energy and the Challenge of Sustainability, New York
Ren YS, Jiang Y, Narayan S et al. (2022) Marketisation and rural energy poverty: Evidence from provincial panel data in China. Energy Econ 111:106073. https://doi.org/10.1016/j.eneco.2022.106073
Sen A (1995) Inequality Reexamined. Oxford University Press, Oxford https://doi.org/10.1093/0198289286.001.0001
Sen A (1999) Development as Freedom. Oxford University Press, Oxford
Sharpe RA, Bearman N, Thornton CR et al. (2015) Indoor fungal diversity and asthma: a meta-analysis and systematic review of risk factors. J Allergy Clin Immunol 135(1):110–122. https://doi.org/10.1016/j.jaci.2014.07.002
Shin SH (2021) Objective and subjective memory: impact on the financial behavior of older adults in the United States. J Econ Ageing 19:100327. https://doi.org/10.1016/j.jeoa.2021.100327
Shupler M, Baame M, Nix E et al. (2022) Multiple aspects of energy poverty are associated with lower mental health-related quality of life: a modelling study in three peri-urban African communities. SSM Ment Heal 2:100103. https://doi.org/10.1016/j.ssmmh.2022.100103
Smith JP, Strauss J, Zhao Y (2014) Healthy aging in China. J Econ Ageing 4:37–43. https://doi.org/10.1016/j.jeoa.2014.08.006
Stock J, Yogo M (2005) Testing for Weak Instruments in Linear IV Regression. In: Andrews D, Stock J (eds.) Identification and inference for econometric models: essays in honor of Thomas Rothenberg. Cambridge University Press, Cambridge, pp 80–108
Sun N, Yang F (2021) Impacts of internal migration experience on health among middle-aged and older adults—Evidence from China. Soc Sci Med 284:114236. https://doi.org/10.1016/j.socscimed.2021.114236
Walston J, Hadley EC, Ferrucci L et al. (2006) Research agenda for frailty in older adults: toward a better understanding of physiology and etiology: summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J Am Geriatr Soc 54(6):991–1001. https://doi.org/10.1111/j.1532-5415.2006.00745.x
Weesie J (2000) Seemlingly unrelated estimation and the cluster-adjusted sandwich estimator. Stata Tech Bull 9(52):34–47
World Bank (2020) Tracking SDG 7: The energy progress report. https://data.worldbank.org/indicator/EG.ELC.ACCS.ZS?locations=CN. Accessed 3 Oct 2021
Xue T, Zhu T, Zheng Y et al. (2019) Declines in mental health associated with air pollution and temperature variability in China. Nat Commun 10(1):2165. https://doi.org/10.1038/s41467-019-10196-y
Yang G, D’Arcy C (2022) Physical activity and social support mediate the relationship between chronic diseases and positive mental health in a national sample of community-dwelling Canadians 65+: A structural equation analysis. J Affect Disord 298:142–150. https://doi.org/10.1016/j.jad.2021.10.055
Zeng Y (2012) Toward deeper research and better policy for healthy aging–using the unique data of Chinese longitudinal healthy longevity survey. China Econ J 5(2–3):131–149. https://doi.org/10.1080/17538963.2013.764677
Zhang D, Li J, Han P (2019) A multidimensional measure of energy poverty in China and its impacts on health: an empirical study based on the China family panel studies. Energy Policy 131:72–81. https://doi.org/10.1016/j.enpol.2019.04.037
Zhang X, Chen X, Zhang XB (2018) The impact of exposure to air pollution on cognitive performance. Proc Natl Acad Sci USA 115(37):9193–9197. https://doi.org/10.1073/pnas.1809474115
Zhang Q, Appau S, Kodom PL (2021a) Energy poverty children’s wellbeing and the mediating role of academic performance: evidence from China. Energy Econ 97:105206. https://doi.org/10.1016/j.eneco.2021.105206
Zhang Z, Shu H, Yi H et al. (2021b) Household multidimensional energy poverty and its impacts on physical and mental health. Energy Policy 156:112381. https://doi.org/10.1016/j.enpol.2021.112381
Zhao Y, Inder B, Kim JS (2021) Spousal bereavement and the cognitive health of older adults in the US: new insights on channels, single items, and subjective evidence. Econ Hum Biol 43:101055. https://doi.org/10.1016/j.ehb.2021.101055
Acknowledgements
The authors sincerely appreciate the Institute of Social Science Survey of Peking University for the data they provided. The authors would also like to thank Zheng SC for his help in the image processing of this paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors.
Informed consent
This article does not contain any studies with human participants performed by any of the authors.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, X., Yang, H. & Jia, J. Impact of energy poverty on cognitive and mental health among middle-aged and older adults in China. Humanit Soc Sci Commun 9, 253 (2022). https://doi.org/10.1057/s41599-022-01276-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1057/s41599-022-01276-4
This article is cited by
-
Multidimensional Energy Poverty in West Africa: Implication for Women’s Subjective Well-being and Cognitive Health
Applied Research in Quality of Life (2024)
-
Household Multidimensional Energy Poverty: Impact on Health, Education, and Cognitive Skills of Children in Ghana
Child Indicators Research (2023)
