
Abstract
Evaluating decision-making during youth is a complex area of research. Multiple factors influence the young person’s subjective decision-making at this stage of development. Sub-optimal decision-making can have lifelong consequences. Longer adolescence, life stressors, drugs and alcohol and adverse events impact the young person, making them vulnerable to emerging mood disorders, such as anxiety and depression. Behavioural economics with its cognitive and multidisciplinary approach examines decision-making in youth with emerging mood disorders, but few empirical studies exist outside of a laboratory setting. Of the few that apply a multidisciplinary approach, most focus on other mental disorders. This review qualitatively evaluates the decision science literature to firstly, investigate complex factors influencing decision-making between adolescence and young adulthood. Secondly, it investigates studies that have applied either a cognitive or multidisciplinary approach to evaluate how young people choose. With respect to the studies identified, this review found that as opposed to depression, clinical anxiety (trait) and its relationship to youth decision-making has not been well researched using the multidisciplinary approach. Studies that did apply this approach found that mood disordered young individuals overall performed worse than healthy controls. This review argues that applying the multidisciplinary approach to study subjective decision-making can provide an alternative measure to empirically evaluate early stages of psychopathology in a youth population. Investigating the critical time points where the decision process itself impacts affective states in individuals could further elucidate some of the challenges currently faced in decision-making studies.
Similar content being viewed by others

Introduction
Cognitive choice paradigms are increasingly being applied to models of psychopathology with the aim of evaluating and predicting behavioural outcomes. The two main approaches which are most effective at evaluating decision-making in human beings are the strictly cognitive approach, which has its foundation in classical economics, and the multidisciplinary approach. Classical economic theories examine aspects of decision-making that deal with an individual’s choices in financial situations (microeconomics) and the world as a whole (macroeconomics). Such a theoretical or cognitive approach measures attitudes towards risk, ambiguity, and inter-temporal decisions, and makes predictions of what decisions ought to be made by individuals. The sub-branch of economics, referred to as behavioural economics, applies the multidisciplinary approach. It goes one step further than the cognitive approach and examines the influence of psychological and sociological factors on decision-making, accepting that these are additional influences on the subjective decision-maker (Kahneman and Tversky, 1982). This approach considers that humans make choices largely based on dispositions, that are mostly unconscious and not amenable to change or prediction.
For decision scientists, these factors have an impact on decision-making, in addition to those mechanisms independently described by the purely cognitive approach. In other words, as Damasio argues, “the comprehensive understanding of the human mind requires an organismic perspective” because emotion and reason cannot be separated (Damasio, 1994, p. 252). Both approaches offer practical insights into general decision-making processes, with the multidisciplinary approach particularly sensitive to evaluating the impact of dysregulated emotions such as those experienced with mood disorders. This article reviews the decision science literature as a whole and argues that the multidisciplinary approach is a more effective way with which to evaluate youth decision-making, especially where clinical anxiety is present. We compare the cognitive and multidisciplinary approaches to help answer our research question, which is, why are the consequences of decision-making different for some young people? To answer this, we suggest how one approach might be more effective in some situations and/or work to complement the other approach when evaluating youth decision-making.
We then present a detailed account of the decision process itself, in a general sense and more specifically, adolescent, and young adult decision-making, where neurodevelopmental factors are an additional influence on this process. By neurodevelopment, we refer to critical neural processes developing at this age, such as attention, memory and mainly learning, all part of the brain’s executive functioning. Factors that adversely influence and affect neurodevelopment broadly include innate, environmental, and inflammatory conditions leading to mood and other disorders (Theoharides et al., 2019). Critically, because of such factors, it is estimated that over 75% of mental health symptoms present themselves before the young person turns 25 years old (Kessler et al., 2005). In the final section of this review, we outline and differentiate the changes in the decision processes in youth mental illness as compared to those processes in healthy development. We aim to show how multiple factors that influence neurodevelopment in this age group possibly conflate empirical findings in the decision sciences. Our overall aim with this review is to present those studies that empirically study clinical populations using the multidisciplinary approach, to suggest alternative measures with which to evaluate how young people choose in a clinical setting.
Method
Theoretical evaluation of decision-making
Although originating from classical economics, the cognitive and the multidisciplinary approach vary in their aims and their methodological evaluation of decision-making. In what follows, we outline the two approaches, as well as describe their points of differentiation (Glimcher, 2011; Kahneman and Slovic, 1982). Table 1 summarises how each approach describes subjective decision-making from an economic perspective.
The cognitive approach
Economic theorists run experiments with the aim of evaluating preferences given to monetary values and how subjective preferences impact the decision-making process itself (Glimcher, 2011; Van Gaal et al., 2012). These are referred to as ‘rational’ economic models. Glimcher (Glimcher, 2011) gives us the narrative of the beggar influenced by external world variables. The story begins with a beggar who finds a 20,000 florins lottery ticket, where he has a 50–50 chance of winning. The beggar has an expected value of 10,000 florins, whereas before he was worth one penny. A wealthy merchant passes by and offers the beggar 7000 florins for his ticket. The question is: Should the beggar accept the merchant’s offer or face a 50–50 chance of increasing his wealth three times over? Glimcher argues that the way to evaluate this question comes from the mathematician Blaise Pascal, who can assess the beggar’s attitude towards gains, losses, and probabilities (Glimcher, 2011).
To evaluate the expected value of each possible choice, Pascal’s theory multiplies the chances of winning by the amount to be won. In doing so, Pascal comes up with a measure of the expected value of each possible outcome; that is of the ‘for sure’ amount of 7000 florins versus the chance of winning the lottery (Glimcher, 2011). Here Pascal believes we can work out the beggar’s aversion to risk and his probability of winning. By such calculations, we can help people make decisions when they are faced with uncertain choices. We can therefore assume that in the beggar’s case, choosing an immediate payout offers the highest value, whereas, in the merchant’s case, the highest value would be gained by purchasing the lottery ticket from the beggar. But is this the best choice for these individuals?
The scientist Daniel Bernoulli (1738) goes beyond Pascal’s probability theory and explains that there are other variables that may be influencing choices involving risk (both the beggar’s and the merchant’s) and that these can also be measured (Glimcher, 2011). Bernoulli’s proposition is that we should measure the best outcome for the beggar and the merchant in a way that moves beyond simply multiplying value and probability. When we work out what the hidden value for each of the possible outcomes of the choices are, we come up with a new variable, referred to as utility. This is because in economics it is theorized that a person has some internal representation of the utility of each feasible alternative and should choose the alternative with the highest utility (Glimcher and Fehr, 2014).
In the beggar’s case, we would compare two choices: one where the beggar takes the immediate payout (as stated above), or a choice based on the calculation referred to as ‘expected utility theory’ (Tversky and Kahneman, 2000). We begin by multiplying the utility of the 20,000-florin ticket, or “4.3 utils” (Glimcher, 2011, p. 45). We multiply the utility amount (4.3) by the probability (50% chance of winning the lottery) and this calculation equates to an estimated amount, in the beggar’s case 2.15 utils. We then compare this to the merchant’s offer (3.8 utils) “where the gain is certain” (Glimcher, 2011, p. 45). The beggar would see there is a higher “expected” utility associated with taking the immediate amount. Because there is a 50% likelihood of gaining the bigger win, it is far less than twice the subjective value of the merchant’s offer. A lower utility rate suggests that the beggar would be well advised to take the merchant’s offer of 7000 florins.
Expected utility theory is the process of assessing decision-making where risk is involved (Tversky and Kahneman, 2000). It works when trying to assess hypothetical decisions, but what happens when we are faced with a real-life choice where the outcome is uncertain? This kind of uncertainty is referred to as ambiguity, where the person is more likely to make a risky choice where the probabilities for each choice are known, than an ambiguous choice where the probabilities for each choice are unknown (Ellsberg, 1961). Technically, the key difference between risk and ambiguity stems from how much information is available at the time of the decision being made (Camerer and Weber, 1992; Levy et al., 2012).
Another argument is that a person can never be fully rational in their decision-making; they can only be, what is referred to as minimally rational, mainly because there are costs associated with cognition, information, and computation of that information (Cherniak, 1986, p. 3). It is from these more realistic theories of economics that the multidisciplinary approach emerges.
The multidisciplinary approach
Economic theory is useful in that it can explain decision-making at one level, as people will choose in a certain way most of the time. However, such theories are generally based on how people ‘should’ behave, with their focus being on optimal decision-making strategies. This kind of approach can only go so far. Tversky famously pointed out that human beings are not necessarily consistent with their choices and will change their preferences at any given time (Tversky, 1969). It is therefore important to consider, where possible, other factors that may be impacting the decision-maker. Kahneman and Tversky (1982) famously extended economic theory to include a multidisciplinary approach, which aims to capture psychological and neuroscientific evidence. Here humans make choices largely based on dispositions, which are mostly unconscious and not amenable to change. In laboratory experiments, where choice is captured, the authors found that in humans certain biases and heuristics explained how the person’s choices were made. Some of the biases and heuristics uncovered included framing, anchoring, availability, and representativeness.
The framing bias occurs when a person decides based on couching an event in either a positive or sub-optimal way. Kahneman et al. argue that up to three types of framing exist: goal framing, risky choice framing, and attribute framing (Kahneman, 2013). Goal framing regards how a person’s choices will be motivated by a particular goal they have in mind. The anchoring bias occurs when a person bases their decision on a particular starting point. For example, a person may heavily rely on certain information they have to make their decision. Kahneman argues that this will affect and thus yield biases of the actual value of something.
Two key examples of heuristics exist (Kahneman, 2013). The availability heuristic is used when decisions are made based on the last thing that a person thought about. The representativeness heuristic regards a decision being made because it reminds the agent of a similar experience that is accessible and easy to recall.
Kahneman remarks how easily we stereotype people using the representativeness heuristic. He gives the example of a woman on the New York subway reading The New York Times (Kahneman, 2013). If asked whether the woman is a Ph.D. student or someone without a college degree, Kahneman says that most people would say the woman reading the newspaper is college-educated based on the example’s representativeness. However, he argues that more non graduates ride the New York subway than graduates and so it is unlikely that the woman has a college degree. Kahneman points out that our choices and judgements are based on probabilities and estimates that arise from not having the full picture in front of us.
We can therefore conclude from their work alone that decision-making cannot be ‘rational’ in the traditional sense. Then how does one apply the multidisciplinary approach to evaluate the impact of these additional factors, such as Kahneman’s heuristics and biases? This with the aim to better grasp decision-making within a laboratory setting, especially in youth with emerging mood disorders such as anxiety and depression.
Sub-branch of the multi-disciplinary approach
Neuroeconomics
To be able to answer our research question, we now turn to the sub-domain of behavioural economics, which is neuroeconomics. It is an established example of the multidisciplinary approach that is used in empirically validated studies. Neuroeconomics uses behavioural tasks to evaluate the cognitive decision processes such as decision-making under risk and uncertainty, intertemporal choice, social decision-making, and applies technology, such as neuroimaging techniques with which to evaluate the mechanisms associated with these decision processes (Sharp et al., 2012). Technological advances have enabled research in this area to be used more frequently and at a lower cost to the researcher. Neuroeconomics with its multidisciplinary approach aims to achieve practical results in the attempt to evaluate subjective decision-making, in both a laboratory and clinical setting. As a field neuroeconomics incorporates elements from neuroscience, psychology, economics and neuroeconomics.
Some scholars claim that neurobiological research evaluating the complex brain has helped us to better understand the processes involved in decision-making, and a variety of studies using the multidisciplinary approach have shown the role that various neural circuits play in general behaviour (Galván and Tottenham, 2016; Rangel et al., 2008a; Rangel and Hare, 2010; Rudolph et al., 2017). Neuroeconomics ambitiously aims to answer the following three questions: (1) What are the computations done by the brain in making different decisions, (2) How are these computations implemented in the brain, and (3) How do these computations map onto behavioural, subjective, and individual differences (Rangel and Montague, 2008b)? Neuroeconomics focuses on one key region in the brain, the prefrontal cortex (PFC), the area of neural networks that determine value-based decision-making (Sonuga‐Barke et al., 2016).
Using a combination of economic methods that evaluate behaviour and brain activities, one major ambition of neuroeconomics is evaluating suboptimal decision-making, such as those that occur in psychopathologies (Sharp et al., 2012). Researchers in decision studies argue that neuroeconomics may inform treatment because it is novel in its ‘multilevel’ research approach (Sharp et al., 2012). However, other researchers (Gallistel and King, 2011; Murphy, 2006), dispute the claims of neuroeconomics, stating that they might be more applicable to animal behavioural studies and that such methods cannot be mapped to human behaviour. This is mainly because in all its complexity these processes cannot be reduced to such specific levels of mechanism, especially ones that compute economic constructs such as expected utility. Other authors argue brain imaging technology shows neural changes, but that these are causally impacted by behaviour all the time (Levy, 2013; Lewis, 2017).
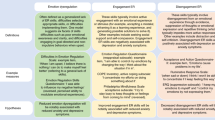
Taking this information into account, what is important in this debate is to remain open to new ways of evaluating suboptimal decision-making, especially in youth where factors that influence the decision process are already complicated at this vulnerable age, and where an emerging mood disorder may be conflated with these developmental periods. In psychopathological evaluation, impaired decision-making is not a stand-alone symptom of a disorder as such, but one of the symptoms associated with a particular disorder such as major depressive disorder (Mukherjee and Kable, 2014). Being able to identify and evaluate the neural underpinnings of these states, outside of the current medical model, is where the multidisciplinary approach can potentially be useful. Figure 1 provides a visual representation of the difference between the Cognitive and the Multidisciplinary approaches, when applied to clinical decision studies evaluating mood disorders such as anxiety and depression, especially in youth.

A visual representation of the difference between the cognitive and the multidisciplinary approaches when applied in clinical decision studies evaluating mood disorders.
In summary, the multidisciplinary approach can be useful in informing a more individualised approach to diagnosis, such as utilising neuroeconomics when mapping neuroimaging to baseline data of healthy patients, and when comparing economically measurable outcomes (Glimcher and Fehr, 2014). This approach that cuts across disciplines may be able to address the ongoing challenges that other theoretical applications face in isolation (Griffiths et al., 2010).
What is decision-making?
Human beings make decisions that derive from the output of brain mechanisms and processes that generally work in sync, and although a complex process, what is termed healthy behaviour does follow a set of decision rules, even though these rules are labelled differently in various schools of science. Decision and cognitive scientists have specific terms, ones that include molar and molecular scale concepts, that influence healthy and unhealthy decision makers alike (Ross et al., 2008, p. 109). Whether optimal or sub-optimal, the act of deciding, which produces a certain behaviour, is understood as a cognitive process (Caceda et al., 2014). Agents make simple choices on a regular basis; these include finding food or deciding when to go to sleep. A decision occurs after the agent places a higher value on one of the alternatives available to them at the time (Rangel, 2008). Value-based decision-making processes are different for everyone, and these processes can cause problems when the possible consequences or outcomes of the decisions are sub-optimal. Here lies an important question when it comes to the study of human beings: Why are the consequences of decision-making different for some people? To answer this question, one can turn to decision-making theories in neuroscience, economics, psychology, and psychiatry. Within each of these disciplines is an attempt to understand the decision-as-problem (Caceda et al., 2014).
Multiple explanatory theories have been developed to explain how healthy people (and animals) make decisions. Research suggests that decision-making is a complex process: a decision-maker must decide which options are of value to her survival or flourishing as well as be able to determine which options will allow for adaptation to the current and future environments (Alvares et al., 2014). Studies use visual paradigms to examine how the underlying neurological pathways map behaviour and to help conceptualize the decision-making process (Sonuga‐Barke et al., 2016; Wittmann and Paulus, 2009), with affective neuroscience investigating the neural processes responsible for the brain’s valuation and decision-making capacity to test hypotheses that relate to aspects of self-control, preferences, and choice (Hare et al., 2009). Three stages are associated with the decision-making process, which includes evaluation, decision management, and appraisal and accommodation (Sonuga‐Barke et al., 2016) (see Table 2).
This three-stage decision-process is governed by three brain regions or domains that inform the decision-making steps: the self-referential process, reflecting present, future, and past states, the domain that reinforces the processes that underlie learning processes; and the region of executive functioning—or areas that mediate the decision planning and implementation processes itself. The executive function of the brain is “an umbrella term that refers to a heterogeneous grouping of top-down processes that allow individuals to regulate their thoughts and behaviour to successfully engage in purposeful, goal-directed, and future-oriented actions” (Sonuga‐Barke et al., 2016, p. 326).
Executive function is distributed across multiple brain regions, initially thought to function within the prefrontal cortex, but contemporary research suggests that these processes are further connected via neural networks or connectomes (Crossley et al., 2016), to regions beyond the prefrontal cortex (Sonuga‐Barke et al., 2016, p. 326). Executive control, an important part of decision-making that relates to economic decision-making, or those more complicated or novel choices that appear, as opposed to automatic responses, is mainly governed by these top-down processes.
Disruptions to the network that allows for these decision-making stages have been identified in several mental illnesses (Sonuga‐Barke et al., 2016). For example, young patients with anxiety disorders will avoid certain decisions because of excessive hesitation (Sonuga‐Barke et al., 2016, p. 334). These patients will shy away from ambiguous choices, mainly because of the diminished capacity of their executive brain regions to determine and thus discern threatening situations. Anxious patients are known to make choices where they avoid circumstances where threats may in fact not exist. Unlike anxious patients, depressed patients are pessimistic and disengaged, mainly because they are biased in their self-referential processes and their choices will reflect such biases (Sonuga‐Barke et al., 2016, p. 334). These patients have difficulty in making decisions because the biases persist in their decision-making. Thus, depression itself has a “dual effect on the processing of reward and value: induction of excessive emotional responses and reduced willingness to reject unfair offers” (Caceda et al., 2014, p. 23).
The decision-making process is further complicated by three key valuation systems that have been identified. Individuals are required to choose what is of most value to them, before acting on that value. Table 3 presents three key valuation systems that define individualised decision-making (i) Pavlovian, (ii) habitual, and (iii) goal-directed (Alvares et al, 2014; Rangel et al., 2008a). Research suggests that all three systems are usually in agreement with one another during the decision-making process (Alvares et al., 2014; Caceda et al., 2014; Rangel et al., 2008a).
In the Pavlovian system, a person associates values with the responses of a small subset of choices they make; the choices are associated with the person’s environmental stimuli and feedback loops (Hare et al., 2009). For example, when presented with an electric shock whilst being given access to a food source, a rat may not choose the food option again as it associates the response with the stimuli and wants to avoid the shock associated with the food option.
The habitual system is slightly different, an example of which is as follows. A person would like to attend a social event and consume an alcoholic beverage. This person is also used to drinking multiple drinks, but when making their decision about the amount they are going to drink the person needs to take driving laws into consideration. In this case, the person is confronted with decisions that have multiple values, with each option compared to the other options. The decision-making process considers former experiences, usually where learning eventuates due to the consequences that either served or did not serve the decision-maker (Rangel et al., 2008b). For example, a person that is used to having an alcoholic drink with dinner every night gets into the habit of drinking every day. Here we refer to a higher-level decision-making process, unlike in the Pavlovian model where such decisions are difficult or impossible to control.
In the goal-directed system, a key criterion related to the belief must be met which states that a person must be able to have knowledge of the outcomes or consequences of their goal or desire. If no such knowledge exists, it is arguable that the person does not have a goal in the required sense. It is the discerning process that qualifies this decision model as goal-directed. This is because the goal-directed system associates values (goal values) with actions by evaluating the consequences associated with goal-directed behaviours (Rangel et al., 2008b). In the section that follows, we present how healthy young people make decisions. Thereafter we discuss the influence of prolonged mood states such as anxiety and depression on the decision-making process itself in youth populations.
Adolescent decision-making
Considering the theoretical and practical understanding of how complicated the decision process is, the study of adolescent behaviour is problematic for multiple reasons. To begin with, the study population itself is not clearly defined (Sawyer et al., 2018, p. 223). Research evaluating decision-making during adolescence (between childhood and early adulthood) can range between 13 and 19 years, at other times up to 24 years old (Sawyer et al., 2018). Reasons to study adolescence, as compared with early adulthood, is because this period is a time when risk-taking behaviour has severely problematic consequences for the individual as well as for society (Blakemore, 2018; Katon et al., 1999; Levy et al., 2012). Adolescent attitudes towards risk, reward, and learning must be considered to evaluate the personal and social impact these factors have on the young person’s life. Although not all adolescents make decisions that are sub-optimal, research suggests that neurodevelopmental and many other factors influence the young person’s capacity for reasonable decision-making. This is mainly because developmental brain regions, associated with risk-taking and sensation-seeking behaviours, namely the amygdala, nucleus accumbens (NAcc) and prefrontal cortex (PFC) are still developing (Mills et al., 2014). This point immediately raises questions regarding whether such developmental factors can in some cases be conflated with prolonged mood states, such as those that present in emerging mood disorders such as anxiety and depression.
In what follows, we attempt to outline the research challenges that arise in studying this developmentally vulnerable age group. Importantly, we flag the complexity of the decision process in the healthy young person’s psychological states, especially so around their late adolescence and early adulthood (Berns et al., 2008). Research suggests that risky decision-making is pervasive during adolescence aged 12–16 years, more so than in youth aged 18–22 years old, and young adults from 24 years onwards (Gardner and Steinberg, 2012). Vast changes in structural neurobiology, occurring up to the age of 30 (for males and females), as well as due to hormonal and physical changes (Blakemore, 2018) impact how the young person chooses and further complicates the study of this population.
Risk, reward, and learning during adolescence
It is important to understand the role of adolescent reward and risk-taking behaviour in the context of today’s society as compared with previous historical periods. Regarding the naturally occurring developmental changes around the time of puberty (and so prior to complete neurological growth), adolescents historically partook in activities (physical and social) aimed at achieving independence and maximizing survival and reproduction (Galván and Tottenham, 2016; Jordan and Andersen, 2017). Unlike adults, adolescents made decisions that were risky, and the outcomes of such risky and impulsive behaviour enabled learning and increased rewards (Van Duijvenvoorde et al., 2016). Risky behaviour persists in adolescents, but survival and reproduction, as we previously knew them, have been replaced by other behavioural outcomes that are not necessarily useful to the individual. Studies suggest that developmental differences in neurobiology and the impact that stimuli, especially emotional stimuli have on the developing young person’s brain, influences how risk plays out, making it difficult to pinpoint why some are more (or less) prone to risky decision-making (Rudolph et al., 2017, p. 94).
The dual system’s approach (Casey et al., 2008; Steinberg, 2010) and the limbic loop theory (Alexander et al., 1990), are two theories that describe adolescent brain development, specifically the impact that brain circuitry and processes have in relation to reward processing and risk-taking. These are critical aspects of decision-making during adolescence, a vulnerable stage of brain development (see Table 4).
Famously, the Dual System Theory is the dynamic account that provides evidence of why young people, especially adolescents, seem more prone to risk-taking behaviour (Casey et al., 2008; Steinberg, 2010). Contemporary studies suggest that although heterogeneity exists within this age group, in comparison with adults, adolescents are more prone to risk due to the phenomenon referred to as the ‘peer effect’ (Gardner and Steinberg, 2012; Steinberg, 2010). This phenomenon occurs due to changes happening between the adolescent’s socio-emotional system and the cognitive control system around the time of puberty (Cohen, 2005; Steinberg, 2008) The temporal disconnects between these two systems impact the adolescent’s ability to self-regulate and control reward-seeking behaviour, the latter gradually developing as the brain matures (Gogtay et al., 2004; Steinberg and Cauffman, 1996). This makes the study of this population’s decision-making more challenging.
Another key decision-making theory is Alexander and Crutcher’s (1990) ‘Limbic-loop’ Theory, which describes the neuropsychological correlates of decision-making, this specifically ambiguous and risky situation. According to this account, the brain is organized into several structurally and functionally distinct ‘circuits’ that link the cortex, basal ganglia, and thalamus, with each circuit focused on a different portion of the frontal lobe (Alexander et al. 1990). It is important to note that there is an interplay between all brain regions, what is referred to as a “parallel functional architecture” that is present within each individual circuit (Alexander et al., 1990, p. 226). In other words, no specific region or circuit works in isolation (Damasio, 2003).
However, when an executive function or working memory is impaired, decision-making becomes impaired, more so where ambiguous choices are presented (Brand et al., 2006; Camille et al., 2011; Schiebener and Brand, 2015). Research shows that brain pathology can occur more frequently in brain regions where there is the high activity or increased metabolic demand (Crossley et al., 2016, 2014). Brain regions made up of intricately connected networks defined as ‘connectomes’ or ‘hubs’, are more affected because of ongoing metabolic demands at certain stages of brain development. In later adolescence, hub connectivity increases over time as the brain develops and matures (Crossley et al., 2016).
From this, it follows that the processing of information and the subsequent behaviour depends on the finely tuned interaction between cognition, emotion, and the subject’s direct environment (Loewenstein et al., 2001; Schiebener and Brand, 2015; Weber et al., 2002). Any interference in these processes has an immediate impact on the outcome of the decisions, especially so during puberty (Stringaris et al., 2014, 2015). Some authors argue that puberty takes place up to 3 years earlier now as compared with 100 years ago and that this is mainly due to environmental changes such as improved diet, hormonal exposure in food products, reduced childhood disease, and increases in childhood obesity (Jordan and Andersen, 2017). Studies suggest earlier puberty (which means longer adolescence) further impacts a young person’s socio-cognitive development or maturity and its manifestation has mainly problematic consequences such as sub-optimal decision-making in general (Harrell et al., 1998). Drug addiction, social neglect, and other adverse events such as trauma, further impact the already ‘critical period’ of brain development, leading to behavioural changes in young adulthood (Casey et al., 2015, 2014; Jordan and Andersen, 2017; Lockhart et al., 2018).
It is therefore the consequences of the risky behaviour that in some cases lead to the emergence of mood and more severe disorders, which in turn can lead to other comorbidities later in the young people’s lives (Katon et al., 1999). Adolescents require much support in their decision-making if they are to successfully manage these multiple challenges.
Risk factors impacting developing neurobiology
In the section that follows we draw attention to the important and close interdependence between physical and mental wellbeing of individuals, especially between adolescents and early adulthood. In a comprehensive model, three known risk factors exist that impact the development of depression: genetic vulnerability, childhood adversity (abuse or neglect), and stressful life events (Katon et al., 1999). Once chronic illness develops, it can cause deterioration in health, inability to exercise, poorer quality of life, job loss and financial insecurity, increased worry, family strain, maladaptive health behaviours, and brain changes (both early and late). Each of these factors, separately or in combination, can increase the risk of depression and other mental health disorders (Katon et al., 1999), and because of this, non-somatic and somatic symptoms should not be seen as being separate.
What is somatic should not be confused with “somatomisation”, which is classified as medically unexplained somatic symptoms that are coupled with psychological distress and help-seeking behaviour. The somatic may be presenting as a psychological illness (such as depression) and vice versa. Stressful conditions and mainly stress itself, all of which have an impact should be taken seriously, because they lead to disturbances in the developing brain’s biological processes and can have dire consequences to the adult brain (Galván and Tottenham, 2016). Moreover, research suggests that these are almost as dire as the onset of mental disorders affected by other environmental and/or genetic factors (Casey et al., 2015).
Neuropsychological research on impulsivity, sensation seeking, and prolonged negative affect indicate that some individuals will have greater difficulty learning from sub-optimal outcomes, especially outcomes that are mixed (that is, those that have some benefits or pleasures associated with them) (Critchley and Harrison, 2013; Herman et al., 2018). Valid and reliable measures of some of these individual differences exist today and can be used to make predictions regarding how they will affect young people. Impulsivity, sensation seeking, thrill seeking, anxiety and depression, and other individual differences contribute to risk-taking that resists standard risk-reduction interventions (Herman et al., 2018; Rudolph et al., 2017). Thus, it is the context in which decision-making takes place that matters (Shulman et al., 2016).
Impact of emotion and its dysregulation
Neurodevelopmental shifts that take place during youth, but especially during adolescence, present outwardly as highly emotional mood states, where behaviour is often driven by these emotions (Guyer et al., 2016; Silk et al., 2012). Studies on the neural substrates of affective behaviour during adolescence are providing much insight into how changes in brain function impact decision-making and how this impact, in turn, is affected by external factors in the individual’s life (Guyer et al., 2016). Neurodevelopmental work on adolescents and young adults outlines the key role that the brain itself plays not only in the critical time of learning and development but also in its important role in emotional self-regulation (Blakemore, 2018; Casey et al. 2008, 2015). The young person’s neurobiology is fast developing (Blakemore, 2018), and at the same time experiencing a demanding social environment with many changing factors. These factors combined are known to make the young person, especially during adolescence, vulnerable and thus more prone to mood disorders, such as anxiety and depression (Silk et al., 2012).
In the research on adolescent decision-making, the study of emotion and its impact on decision-making is a central topic and has been for some time (Brand et al., 2006; George andand Dane, 2016; Loewenstein et al., 2001; Phelps et al., 2014; Schmaal et al., 2016; Sonuga‐Barke et al., 2016). In order to grasp the dysregulation of emotion, we first provide a brief overview of the complicated nature of emotion itself. The definition of affect and emotion is controversial and complex, laden with ambiguous labels and cultural challenges (Damasio, 1994; Guttenplan, 1994; Scherer, 2005, 2011). Affect is described as the pre-embodied, non-linear experience of sensation (‘out of mind’) before becoming conscious (‘in the mind’) (Dunn et al., 2006; Massumi, 1995). Studies suggest affect is the biological sensory state that occurs moments prior to any action and expression (such as decision-making) (Damasio, 2000; Harrison et al., 2010; Massumi, 1995). Some researchers suggest that only when aided by volition and cognition does affect give rise to a discrete reaction or emotion (Massumi, 1995).
Emotions are hypothesized to enable us to actively discern stimuli and events that have an impact on guiding our behaviour and mainly to move us away from threat and protect us from harm (Frijda, 2017). Evolving in the human brain over many years, emotions play an important positive part in our overall decision-making (LeDoux, 2000, 2003). Although there are differences between bio-regulatory affect and the subjectively experienced emotion triggered by many objects or events (rather than one object or event), they are also interdependent (Griffiths, 1997). For example, it has been suggested that defects in our biological system, such as difficulty processing affective visual stimuli, underlie prolonged mood disorders and phobias (Adolphs and Pessoa, 2010). Here, the subject has difficulty processing social and emotional cues that arise automatically from environmental stimuli, which leads to variability in how the information is understood. Impairments of this nature affectively disable the subject, their environment becoming a permanently threatening place to live in and having a mainly negative impact on their mood.
The delicate nature of grasping affect, emotion, and associated states, dysregulated or not, makes their evaluation in a scientific setting highly problematic (Damasio, 2003; Power, 2010). To complicate matters even further, research suggests that it is not so much the aetiology of affect and emotion that matters, but rather how emotions are expressed, or how aware a person is of their reactions (Kuhnen and Knutson, 2005, 2011). Importantly, prolonged mood should not be confused with mood in general or incidental mood, the latter described as a person’s state associated with an immediate choice or task. Research has found that memory of past experiences or future glimpses of an experience are enough to induce mood states and bias decision-making, influencing it in problematic ways (George and Dane, 2016).
Anxiety and depression in decision-making
Negative emotional states do not impact decision-making in the same way as prolonged mood states—such as trait anxiety and depression. Trait anxiety, a serious influencer for stress-induced depression is known to negatively influence a young person, leading to sub-optimal behaviour, as well as problematic physiological changes later in life (Galván and Tottenham, 2016; Heim and Nemeroff, 2001; Weger and Sandi, 2018). Unlike negative affect that may only be present for a period, anxiety in the absence of threats, may continue to persist and lead to mood disorders such as anxiety and depression. In such cases, negative biases toward threats continue to persist and impact a person’s decision-making in a very problematic way, mainly because threats become exaggerated (Caceda et al., 2014). The empirical literature demonstrates that people of all ages who are influenced by dysregulated emotion (Brand et al., 2006), such as those presented in mood disorders, may be unaware that the way in which they make decisions leads to sub-optimal consequences (Chang and Sanfey, 2008; Harle et al., 2010; Weiss et al., 2015). For example, older economic studies empirically evaluating risk attitudes in early adulthood found that risk avoidance was prominent in the anxious clinical population—as compared to the healthy population where researchers had stimulated negative affect for experimental purposes (Maner et al., 2007).
It is well known that anxiety is a response to ever-present factors of uncertainty in daily life, which is associated with helping mitigate any kind of threat (Caceda et al., 2014). In such cases, anxiety can be understood as a positive response under certain conditions in that it helps the subject avoid what could be a disaster (George and Dane, 2016; Kuhnen and Knutson, 2011). One study assessing the impact of anxiety (termed ‘utility anxiety’) on gambling decisions in young adults identified that such conditions allowed a subject to be more ‘psychologically prepared’ and thus gave the subject more time to be more informed (Wu, 1999). This is also known as the ‘risk as feeling’ hypothesis (Loewenstein et al., 2001, p. 270). Emotion here is referred to as an ‘anticipated’ emotion, and not to be confused with ‘anticipatory’ emotion (Loewenstein et al., 2001, p. 267). The latter is the immediate or felt state, or the fear of the risk at hand, whereas the former refers to the state of being afraid of what could be.
Multidisciplinary studies evaluating the impact of depression on decision-making in youth aged 18–25 years using economic tasks and functional magnetic resonance imaging, found that suboptimal behaviour persisted, with a decrease in sensitivity to risky decision-making (Gao et al., 2021). When evaluating risk attitudes in a clinical population with major depressive disorder this study found that as compared to the healthy cohort, the depressed group had decreased sensitivity to risk levels (Gao et al., 2021). Another economic decision-making study in university undergraduates assessing the effects of dopamine D2 receptor density using spontaneous eye blink rates found that healthy subjects who rated as depressive performed better than those subjects with lower depressive scores, where these decision-makers were averse to losses, and therefore took less risk (Byrne et al., 2016). A critical review evaluating the impact of depression comparing adolescents to adults, found that reward function might be especially disrupted in response to social rewards, in both the youth and ageing population (Forbes and Dahl, 2012). These and other larger reviews (Sonuga‐Barke et al., 2016) of the depression literature and its impact on decision-making in youth, demonstrate that the role of dysregulated emotion can be underestimated.
Discussion
To clearly identify the impact of prolonged mood, such as anxiety and depression and its influence on how young people choose, we now turn to the application of decision paradigms used in research practices, as demonstrated by the cognitive and multidisciplinary approaches.
Sub-optimal decision-making
What is clear across the body of research evaluating emotion and its dysregulation is the pervasive aberrant and overall sub-optimal decision-making trend in youth in general (Brand et al., 2006). This review identified several key studies that use both the cognitive and the multidisciplinary approach to evaluate mood disorders—anxiety and depression between childhood, adolescence, and young adulthood. Peer-reviewed empirical papers for inclusion in this quantitative part of the review were obtained by searching Science Direct, PubMed and PsycInfo. Table 5 provides a summary of studies that met our inclusion criteria.
The studies using both the cognitive and multidisciplinary approach applying economic measures, identified that mood disordered individuals, across all ages in youth overall performed worse than healthy controls, but that no performance differences were found based on the disorders specifically (Mukherjee and Kable, 2014; Sonuga‐Barke et al., 2016). As opposed to depression, clinical trait anxiety and its relationship to decision-making have not been well researched in the field of behavioural economics with its multidisciplinary capability (Hartley and Phelps, 2012). Overall, only one study (Weinrabe et al., 2020) evaluated youth with emerging mood disorders, with the emphasis on trait anxiety on choice preferences.
Scholars in the field have made it clear that complex factors, such as pre, during- and post-disease characteristics, including multiple non-disease-related factors, severely influence whether a link exists between anxiety and sub-optimal decision outcomes (Paulus and Yu, 2012). Moreover, our quantitative review revealed that methods used to describe these decision-making trends arrive at varying results (Alvares et al., 2014; Berns et al., 2008; Caceda et al., 2014; Han et al., 2012; Harle et al., 2017; Kishida et al., 2010; Mukherjee and Kable, 2014; Murphy et al., 2001, 1999). Recent robust studies have been conducted that aim to provide insight into the degree to which decision-making is impaired across multiple disorders and using modern technologies (Gao et al., 2021; Ji et al., 2021). In a metanalysis evaluating the impact that anxiety and depression have on adolescent and youth decision-making using the multidisciplinary approach, it was found that poor decision-making would remain the overall outcome (Sonuga‐Barke et al., 2016). The studies showed that young people suffering from depression were more disengaged and pessimistic in how they engaged in decision-making than in healthy controls (Sonuga‐Barke et al., 2016).
Most authors in the studies we reviewed from the affective neurosciences agree that prolonged anxiety, such as trait anxiety alters neural circuitry in such a way that it influences beliefs, motivation, and importantly the way in which the person learns how to discern what is or is no longer a threat (Hartley and Phelps, 2012). Clinical anxiety impacts the computation of value and choice, and in this way, it generates a negative bias, one that alters the decision process in the short and long term, and which leads to sub-optimal choices (Harle et al., 2017; Murphy et al., 1999; Swann and Snyder, 1980). These studies included information to reveal that over many generations, natural selection has sculpted a sophisticated system in the brain purposed for monitoring the environment, attending to multiple stimuli which may ‘help or harm’, and informing behaviour to avoid the threat and seek sustenance. While useful, this attentional system may veer into maladaptive and pathological functioning (or dysfunction), with dysregulation biasing attention toward threatening stimuli and leading to psychopathological mental states. This provides evidence of anxiety and biased attentional processes, especially so in major mood disorders (Murphy et al., 1999). A more recent empirical study, evaluating an Australian clinical youth population aged 18–25, found that economic decision-making was significantly impaired for young people suffering from anxiety (Weinrabe et al., 2020).
However, from all the studies we reviewed, no studies show the problematic influence of the decision process itself on the decision-maker. This was a main concern raised by another scholar evaluating decision-making in healthy populations (Berns et al., 2008). For example, we could ask what are the reverse effects of sub-optimal decision-making on mood, as opposed to prolonged mood states—such as those experienced in youth with mood disorders, influencing decision-making? Does impaired decision-making leading to adolescents avoiding risk, mean they avoid learning, a necessary part of their overall neurodevelopment, which could, in turn, impact their resilience in adulthood? More empirical evidence is required to understand the influence that external world pressures, and importantly, the role of anxiety and/or have on the young person’s decision processes and overall health.
Limitations
This review is limited to the studies evaluating mood disorders and its impact on youth decision-making. It did not evaluate studies that investigate additional risk factors during adolescence and early adulthood, such as drug and alcohol misuse, or the influence of stressful life events. Our conclusions demonstrate that further clinical empirical studies are necessary to better understand the detrimental consequences on decision-making, especially so in vulnerable youth who we argued, are prone to emerging mood disorders at this stage of neurodevelopment (Berns et al., 2008; Sonuga‐Barke et al., 2016). Very little empirical evidence exists within a developmental psychopathology framework (Blakemore, 2018), because most studies are focused on either adults, and/or youth who suffer from mainly Major Depressive Disorders, and other severe mental illnesses. However, it is estimated that over 75% of mental health symptoms, such as mood disorders present themselves before the young person turns 25 years old (Kessler et al., 2005). Large studies in children and adolescents clearly show the problematic impact that severe anxiety and chronic distress have on the young person’s long-term health (Katz et al., 2012; Merikangas, 2010).
Publication bias is likely to exist due to so few studies that use the multidisciplinary approach to study early stage, or emerging mood disorders on subjective decision-making. Furthermore, most studies were conducted in a laboratory setting where the emotional states were induced, as opposed to in a clinical setting; this is a major further limitation. In addition, small sample sizes, possibly due to the challenges associated with pinpointing mood disorders in a clinical youth population, and the high cost of working with technologies in the affective neurosciences are also a limitation.
Early-stage diagnoses and interventions are critical. Results taken from a large study (N = 1483 subjects) using the clinical staging model to evaluate young people seeking mental healthcare found that most young people already presented with ‘attenuated’ symptoms, a stage worse than ‘help-seeking’, leading to the severe disorders (Hickie (Hickie et al., 2013a, 2013b). Importantly, in Australia, anxiety and depression rates are at an all-time high in youth. 6.9% of young people up to the age of 17 years suffer from anxiety disorders as compared with their younger peers, and major depressive disorders are 5% higher in young people aged 12–17, as compared with the 1.1% in children aged 4–11 years of age (Lawrence et al., 2016). Contemporary studies have identified that early-stage intervention for youth with depression is critical, as opposed to addressing depression in its chronic stage (Kaur et al., 2019; Sivertsen et al., 2015). Studies that can assist to support clinicians evaluate critical time points where the decision process itself impacts affective states in individuals are therefore of tremendous value.
Concluding remarks
This review presents evidence that demonstrates how robust decision studies that apply the multidisciplinary approach in clinical settings can be utilized to further evaluate early stages of psychopathology in a youth population, as well as over the lifespan of the young patient. It suggests that the interplay of cognition and emotion on the decision-making process in unhealthy and healthy young people is equally important to investigate. Future research could compare both populations to evaluate the influence of the developing brain on decision-making. Investigating the critical time points where the decision process itself impacts affective states in individuals could further elucidate some of the challenges currently faced in decision-making studies. Researchers have urgently called for the qualitative evaluation of the impact of sub-optimal decision-making, starting in adolescence and observed into adulthood for two key reasons (Harbaugh et al., 2001). Firstly, to better understand youth’s risk preferences to model policies to improve decision-making; and secondly, by clarifying how such risk preferences change over time, policymakers can have better insights into adult behaviour.
References
Adolphs R, Pessoa L (2010) Emotion processing and the amygdala: from a ‘low road’ to ‘many roads’ of evaluating biological significance. Nat Rev Neurosci 11(11):773–783. https://doi.org/10.1038/nrn2920
Alexander GE, Crutcher MD, DeLong MR (1990) Basal ganglia-thalamocortical circuits: parallel substrates for motor, oculomotor, “prefrontal” and “limbic” functions. Prog Brain Res 85:119
Alvares GA, Balleine BW, Guastella AJ (2014) Impairments in goal-directed actions predict treatment response to cognitive-behavioral therapy in social anxiety disorder. PLoS ONE 9(4):e94778. https://doi.org/10.1371/journal.pone.0094778
Berns GS, Capra CM, Moore S, Noussair C (2008) Three studies on the neuroeconomics of decision-making when payoffs are real and negative. Adv Health Econ Health Serv Res 20:1–29
Blakemore SJ (2018) Development of the adolescent brain: implications for executive function and social cognition. Eur Neuropsychopharmacol 28:S1. https://doi.org/10.1016/j.euroneuro.2017.12.017
Brand M, Labudda K, Markowitsch HJ (2006) Neuropsychological correlates of decision-making in ambiguous and risky situations. Neural Networks 19(8):1266–1276. https://doi.org/10.1016/j.neunet.2006.03.001
Byrne KA, Norris DD, Worthy DA (2016) Dopamine, depressive symptoms, and decision-making: the relationship between spontaneous eye blink rate and depressive symptoms predicts Iowa Gambling Task performance. Cogn Affect Behav Neurosci 16(1):23–36. https://doi.org/10.3758/s13415-015-0377-0
Caceda R, Nemeroff CB, Harvey PD (2014) Toward an understanding of decision making in severe mental illness. J Neuropsychiatry Clin Neurosci 26(3):196–213. https://doi.org/10.1176/appi.neuropsych.12110268
Camerer C, Weber M (1992) Recent developments in modeling preferences: uncertainty and ambiguity. J Risk Uncertain 5(4):325–370. https://doi.org/10.1007/BF00122575
Camille N, Griffiths CA, Vo K, Fellows LK, Kable JW (2011) Ventromedial frontal lobe damage disrupts value maximization in humans. J Neurosci 31(20):7527–7532. https://doi.org/10.1523/JNEUROSCI.6527-10.2011
Casey BJ, Getz S, Galvan A (2008) The adolescent brain. Dev Rev 28(1):62–77. https://doi.org/10.1016/j.dr.2007.08.003
Casey BJ, Glatt CE, Lee FS (2015) Treating the developing versus developed brain: translating preclinical mouse and human studies. Neuron 86(6):1358–1368. https://doi.org/10.1016/j.neuron.2015.05.020
Casey BJ, Oliveri ME, Insel T (2014) A neurodevelopmental perspective on the research domain criteria (RDoC) framework. Biol Psychiatry 76(5):350–353. https://doi.org/10.1016/j.biopsych.2014.01.006
Chang LJ, Sanfey AG (2008) Emotion, decision-making and the brain. Adv Health Econ Health Serv Res 20:31–53
Cherniak C (1986). Minimal rationality. MIT Press.
Cohen JD (2005) The vulcanization of the human brain: a neural perspective on interactions between cognition and emotion. Jf Econ Perspect 19(4):3–24. https://doi.org/10.1257/089533005775196750
Critchley HD, Harrison NA (2013) Visceral influences on brain and behavior. Neuron 77(4):624–638. https://doi.org/10.1016/j.neuron.2013.02.008
Crossley, Fox PT, Bullmore ET (2016) Meta-connectomics: human brain network and connectivity meta-analyses. Psychol Med 46(5):897. https://doi.org/10.1017/S0033291715002895
Crossley, Mechelli A, Scott J, Carletti F, Fox PT, McGuire P, Bullmore ET (2014) The hubs of the human connectome are generally implicated in the anatomy of brain disorders. Brain 137(Pt 8):2382. https://doi.org/10.1093/brain/awu132
Damasio AR (1994) Descartes’ error: emotion, reason, and the human brain. G.P. Putnam, New York
Damasio AR (2000) The feeling of what happens: body, emotion and the making of consciousness. Vintage, London
Damasio AR (2003) Looking for Spinoza: joy, sorrow, and the feeling brain (Vol. 1st). Harcourt, Orlando
Dunn BD, Dalgleish T, Lawrence AD (2006) The somatic marker hypothesis: a critical evaluation. Neurosci Biobehav Rev 30(2):239–271. https://doi.org/10.1016/j.neubiorev.2005.07.001
Ellsberg D (1961) Risk, ambiguity, and the savage axioms. Q J Econ 75(4):643–669
Forbes EE, Dahl RE(2012) Research Review: altered reward function in adolescent depression: what, when and how? J Child Psychol Psychiatry 53(1):3–15. https://doi.org/10.1111/j.1469-7610.2011.02477.x
Frijda NH (2017) The laws of emotion. Psychology Press
Gallistel CR, King AP (2011) Memory and the computational brain: why cognitive science will transform neuroscience, vol. 6. John Wiley & Sons
Galván A, Tottenham N (2016) Adolescent brain development. In: Cicchetti D (ed) Developmental psychopathology: developmental neuroscience. John Wiley & Sons, Inc., pp. 684–719
Gao F, Fan J, Xia J, Soondrum T, Liu W, Du H, Zhu X (2021) Decreased sensitivity to risk levels in ventral stratum in major depressive disorder during risky decision-making. J Affect Disord 282:187–193. https://doi.org/10.1016/j.jad.2020.12.131
Gardner M, Steinberg L (2012) “Peer influence on risk taking, risk preference, and risk decision making in adolescence and adulthood: an experimental study”: Correction to Gardner and Steinberg (2005). Dev Psychol 48(2):589–589. https://doi.org/10.1037/a0026993
George JM, Dane E (2016) Affect, emotion, and decision making. Organ Behav Hum Decision Process 136:47–55
Glimcher PW (2011) Foundations of neuroeconomic analysis. Oxford University Press, Oxford; New York
Glimcher PW, Fehr E (2014) Neuroeconomics: decision making and the brain (Vol. Second). Elsevier/AP, Academic Press is an imprint of Elsevier, Amsterdam, London, Boston
Gogtay N, Giedd JN, Lusk L, Hayashi KM, Greenstein D, Vaituzis AC, Ungerleider LG (2004) Dynamic mapping of human cortical development during childhood through early adulthood. Proc Natl Acad Sci USA 101(21):8174–8179. https://doi.org/10.1073/pnas.0402680101
Griffiths (1997) What emotions really are: the problem of psychological categories. University of Chicago Press, Chicago, IL
Griffiths, Chater N, Kemp C, Perfors A, Tenenbaum JB (2010) Probabilistic models of cognition: exploring representations and inductive biases. Trends Cogn Sci 14(8):357–364
Guttenplan SD (1994) A Companion to the philosophy of mind. Blackell Reference, Cambridge, Oxford
Guyer AE, Silk JS, Nelson EE (2016) The neurobiology of the emotional adolescent: from the inside out. Neurosci Biobehav Rev 70:74–85. https://doi.org/10.1016/j.neubiorev.2016.07.037
Han G, Klimes-Dougan B, Jepsen S, Ballard K, Nelson M, Houri A, Cullen K (2012) Selective neurocognitive impairments in adolescents with major depressive disorder. J Aadolesc 35(1):11. https://doi.org/10.1016/j.adolescence.2011.06.009
Harbaugh WT, Krause K, Berry TR (2001) GARP for kids: on the development of rational choice behavior. Am Econ Rev 91(5):1539–1545
Hare TA, Camerer CF, Rangel A (2009) Self-control in decision-making involves modulation of the vmPFC valuation system. Science 324(5927):646–648. https://doi.org/10.1126/science.1168450
Harle, Guo DL, Zhang SA, Paulus MP, Yu AJ (2017) Anhedonia and anxiety underlying depressive symptomatology have distinct effects on reward-based decision-making. PLoS ONE 12(10):e0186473. https://doi.org/10.1371/journal.pone.0186473
Harle KM, Allen JJ, Sanfey AG (2010) The impact of depression on social economic decision making. [Article]. J Abnormal Psychol 119(2):440–446
Harrell JS, Bangdiwala SI, Deng S, Webb JP, Bradley C (1998) Smoking initiation in youth: the roles of gender, race, socioeconomics, and developmental status. J Adolesc Health 23(5):271–279
Harrison NA, Gray MA, Gianaros PJ, Critchley HD (2010) The embodiment of emotional feelings in the brain. J Neurosci 30(38):12878–12884. https://doi.org/10.1523/JNEUROSCI.1725-10.2010
Hartley CA, Phelps EA (2012) Anxiety and decision-making. Biol Psychiatry 72(2):113. https://doi.org/10.1016/j.biopsych.2011.12.027
Heim C, Nemeroff CB (2001) The role of childhood trauma in the neurobiology of mood and anxiety disorders: preclinical and clinical studies. Biol Psychiatry 49(12):1023–1039. https://doi.org/10.1016/S0006-3223(01)01157-X
Herman AM, Critchley HD, Duka T (2018). Risk-taking and impulsivity: the role of mood states and interoception. Front Psychol 9(1625). https://doi.org/10.3389/fpsyg.2018.01625
Hickie IB, Hermens DF, Naismith SL, Guastella AJ, Glozier N, Scott J, Scott EM (2013) Evaluating differential developmental trajectories to adolescent-onset mood and psychotic disorders. BMC Psychiatry 13(1):303–303. https://doi.org/10.1186/1471-244X-13-303
Hickie IB, Scott EM, Hermens DF, Naismith SL, Guastella AJ, Kaur M, McGorry PD (2013) Applying clinical staging to young people who present for mental health care. Early Interv Psychiatry 7(1):31–43. https://doi.org/10.1111/j.1751-7893.2012.00366.x
Ji X, Zhao J, Li H, Pizzagalli DA, Law S, Lin P, Wang X (2021) From motivation, decision-making to action: an fMRI study on suicidal behavior in patients with major depressive disorder. J Psychiatr Res 139:14–24
Jordan CJ, Andersen SL (2017) Sensitive periods of substance abuse: early risk for the transition to dependence. Dev Cogn Neurosci 25:29–44
Kahneman (2013) Thinking, fast and slow. Farrar, Straus and Giroux, New York
Kahneman T, Slovic (1982) Judgment under uncertainty: heuristics and biases. Cambridge University Press, Cambridge
Katon W, Von Korff M, Lin E, Simon G, Walker E, Unützer J, Ludman E (1999) Stepped collaborative care for primary care patients with persistent symptoms of depression: a randomized trial. Arch Gen Psychiatry 56(12):1109–1115. https://doi.org/10.1001/archpsyc.56.12.1109
Katz DA, Sprang G, Cooke C (2012) The cost of chronic stress in childhood: understanding and applying the concept of allostatic load. Psychodyn Psychiatry 40(3):469
Kaur M, Naismith SL, Lagopoulos J, Hermens DF, Lee RSC, Carpenter JS, Hickie IB (2019) Sleep-wake, cognitive and clinical correlates of treatment outcome with repetitive transcranial magnetic stimulation for young adults with depression. Psychiatry Res 271:335–342. https://doi.org/10.1016/j.psychres.2018.12.002
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE (2005) Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 62(6):593–602
Kishida KT, King-Casas B, Montague PR (2010) Neuroeconomic approaches to mental disorders. Neuron 67(4):543–554. https://doi.org/10.1016/j.neuron.2010.07.021
Kuhnen CM, Knutson B (2005) The neural basis of financial risk taking. Neuron 47(5):763–770. https://doi.org/10.1016/j.neuron.2005.08.008
Kuhnen CM, Knutson B (2011) The influence of affect on beliefs, preferences, and financial decisions. J Financ Quant Anal 46(3):605–626. https://doi.org/10.1017/S0022109011000123
Lawrence D, Hafekost J, Johnson SE, Saw S, Buckingham WJ, Sawyer MG, Zubrick SR (2016) Key findings from the second Australian Child and Adolescent Survey of Mental Health and Wellbeing. Austral N Z J Psychiatry 50(9):876–886. https://doi.org/10.1177/0004867415617836
LeDoux (2000) Emotion circuits in the brain. Annu Rev Neurosci 23(1):155–184. https://doi.org/10.1146/annurev.neuro.23.1.155
LeDoux (2003) The emotional brain, fear, and the amygdala. Cell Mol Neurobiol 23(4-5):727–738
Levy I, Rosenberg Belmaker L, Manson K, Tymula A, Glimcher PW (2012) Measuring the subjective value of risky and ambiguous options using experimental economics and functional MRI methods. J. Vis. Exp. 67: e3724. https://doi.org/10.3791/3724
Levy N (2013) Addiction is not a brain disease (and it matters). Front Psychiatry 4:24
Lewis M (2017) Addiction and the brain: development, not disease. Neuroethics 10(1):7–18
Lockhart S, Sawa A, Niwa M (2018) Developmental trajectories of brain maturation and behavior: relevance to major mental illnesses. J Pharmacol Sci 137(1):1–4. https://doi.org/10.1016/j.jphs.2018.04.008. Epub 2018 May 3
Loewenstein GF, Weber EU, Hsee CK, Welch N (2001) Risk as feelings. Psychol Bull 127(2):267–286. https://doi.org/10.1037//0033-2909.127.2.267
Maner JK, Richey JA, Cromer K, Mallott M, Lejuez CW, Joiner TE, Schmidt NB (2007) Dispositional anxiety and risk-avoidant decision-making. Personal Individ Differ 42(4):665–675
Massumi B (1995) The autonomy of affect. Cult Critique 31(31):83–109
Merikangas KR (2010) Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry 49(10):980–989. https://doi.org/10.1016/j.jaac.2010.05.017
Mills KL, Goddings A-L, Clasen LS, Giedd JN, Blakemore S-J (2014) The developmental mismatch in structural brain maturation during adolescence. Dev Neurosci 36(3-4):147–160
Mukherjee D, Kable JW (2014) Value-based decision making in mental illness: a meta-analysis. Clin Psychol Sci 2(6):767–782. https://doi.org/10.1177/2167702614531580
Murphy. (2006). Review of Paul Glimcher, decisions, uncertainty and the brain: the science of neuroeconomics. Philos Psychol 19(1). https://mechanism.ucsd.edu/~pp/back%20issues/volume19%20issue1.html
Murphy, Rubinsztein JS, Michael A, Rogers RD, Robbins TW, Paykel ES, Sahakian BJ (2001) Decision-making cognition in mania and depression. Psychol Med 31(4):679–693. https://doi.org/10.1017/S0033291701003804
Murphy, Sahakian BJ, Rubinsztein JS, Michael A, Rogers RD, Robbins TW, Paykel ES (1999) Emotional bias and inhibitory control processes in mania and depression. Psychol Med 29(6):1307–1321. https://doi.org/10.1017/S0033291799001233
Paulus MP, Yu AJ (2012) Emotion and decision-making: affect-driven belief systems in anxiety and depression. Trends Cogn Sci 16(9):476–483. https://doi.org/10.1016/j.tics.2012.07.009
Phelps EA, Lempert KM, Sokol-Hessner P (2014) Emotion and decision making: multiple modulatory neural circuits. Annu Rev Neurosci 37:263–287
Power M (2010) Emotion-focused cognitive therapy. John Wiley & Sons.
Rangel (2008) Consciousness meets neuroeconomics: what is the value of stimulus awareness in decision making? Neuron 59(4):525–527. https://doi.org/10.1016/j.neuron.2008.08.003
Rangel, Camerer, Montague R (2008a) A framework for studying the neurobiology of value-based decision making. Nat Rev Neurosci 9(7):545–556. https://doi.org/10.1038/nrn2357
Rangel, Camerer C, Montague R (2008b) Neuroeconomics: The neurobiology of value-based decision-making. Nat Rev Neurosci 9(7):545
Rangel, Hare T (2010) Neural computations associated with goal-directed choice. Curr Opinion Neurobiol 20(2):262–270. https://doi.org/10.1016/j.conb.2010.03.001
Ross D, Sharp C, Vuchinich R, Spurrett D (2008) Midbrain mutiny: the picoeconomics and neuroeconomics of disordered gambling. MIT Press, Cambridge
Rudolph MD, Miranda-Domínguez O, Cohen AO, Breiner K, Steinberg L, Bonnie RJ, Fair DA (2017) At risk of being risky: the relationship between “brain age” under emotional states and risk preference. Dev Cogn Neurosci 24:93–106. https://doi.org/10.1016/j.dcn.2017.01.010
Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC (2018) The age of adolescence. Lancet Child Adolesc Health 2(3):223–228
Scherer KR (2005) What are emotions? And how can they be measured? Soc Sci Inf 44(4):695–729. https://doi.org/10.1177/0539018405058216
Scherer KR (2011) On the rationality of emotions: or, When are emotions rational? Soc Sci Inf 50(3–4):330–350. https://doi.org/10.1177/0539018411411018
Schiebener J, Brand M (2015) Decision making under objective risk conditions—a review of cognitive and emotional correlates, strategies, feedback processing, and external influences. Neuropsychol Rev 25(2):171–198. https://doi.org/10.1007/s11065-015-9285-x
Schmaal L, Hibar DP, Sämann PG, Hall GB, Baune BT, Jahanshad N… Veltman DJ (2016). Cortical abnormalities in adults and adolescents with major depression based on brain scans from 20 cohorts worldwide in the ENIGMA Major Depressive Disorder Working Group. Mol Psychiatry https://doi.org/10.1038/mp.2016.60
Sharp C, Monterosso J, Montague PR (2012) Neuroeconomics: a bridge for translational research. Biol Psychiatry 72(2):87–92. https://doi.org/10.1016/j.biopsych.2012.02.029
Shulman EP, Smith AR, Silva K, Icenogle G, Duell N, Chein J, Steinberg L (2016) The dual systems model: Review, reappraisal, and reaffirmation. Dev Cogn Neurosci 17:103–117
Silk JS, Davis S, McMakin DL, Dahl RE, Forbes EE (2012) Why do anxious children become depressed teenagers? The role of social evaluative threat and reward processing. Psychol Med 42(10):2095–2107. https://doi.org/10.1017/S0033291712000207
Sivertsen B, Harvey AG, Pallesen S, Hysing M (2015) Mental health problems in adolescents with delayed sleep phase: results from a large population‐based study in N orway. J Sleep Res 24(1):11–18
Sonuga‐Barke EJS, Cortese S, Fairchild G, Stringaris A (2016) Annual Research Review: transdiagnostic neuroscience of child and adolescent mental disorders–differentiating decision making in attention‐deficit/hyperactivity disorder, conduct disorder, depression, and anxiety. J Child Psychol Psychiatry 57(3):321–349
Steinberg (2008) A social neuroscience perspective on adolescent risk-taking. Dev Rev 28(1):78–106
Steinberg (2010) A dual systems model of adolescent risk‐taking. Dev Psychobiol 52(3):216–224
Steinberg, Cauffman E (1996) Maturity of judgment in adolescence: psychosocial factors in adolescent decision making. Law Hum Behav 20(3):249–272
Stringaris A, Lewis G, Maughan B (2014) Developmental pathways from childhood conduct problems to early adult depression: findings from the ALSPAC cohort. Br J Psychiatry 205(1):17–23
Stringaris A, Vidal-Ribas Belil P, Artiges E, Lemaitre H, Gollier-Briant F, Wolke S, …, Struve M (2015) The brain’s response to reward anticipation and depression in adolescence: dimensionality, specificity, and longitudinal predictions in a community-based sample. Am J Psychiatry 172(12):1215–1223
Swann WB, Snyder M (1980) On translating beliefs into action: theories of ability and their application in an instructional setting. J Personal Soc Psychol 38(6):879–888. https://doi.org/10.1037/0022-3514.38.6.879
Theoharides T, Kavalioti M, Martinotti R (2019) Factors adversely influencing neurodevelopment. J Biol Regul Homeost Agents 33(6):1663–1667
Tversky A (1969) Intransitivity of preferences. Psychol Rev 76(1):31–48. https://doi.org/10.1037/h0026750
Tversky A, Kahneman D (2000) Choices, values, and frames. Cambridge University Press, Cambridge
Van Duijvenvoorde ACK, Peters S, Braams BR, Crone EA (2016) What motivates adolescents? Neural responses to rewards and their influence on adolescents’ risk taking, learning, and cognitive control. Neurosci Biobehav Rev 70:135–147
Van Gaal S, De Lange FP, Cohen MX (2012) The role of consciousness in cognitive control and decision making. Front Hum Neurosci 6:121
Weber EU, Blais AR, Betz NE (2002) A domain‐specific risk‐attitude scale: measuring risk perceptions and risk behaviors. J Behav Decision Making 15(4):263–290. https://doi.org/10.1002/bdm.414
Weger M, Sandi C (2018) High anxiety trait: a vulnerable phenotype for stress-induced depression. Neurosci Biobehav Rev 87:27–37. https://doi.org/10.1016/j.neubiorev.2018.01.012
Weinrabe A, Chung H-K, Tymula A, Tran J, Hickie IB (2020) Economic rationality in youth with emerging mood disorders J Neurosci Psychol Econ 3:164–177. https://doi.org/10.1037/npe0000129
Weiss NH, Sullivan TP, Tull MT (2015) Explicating the role of emotion dysregulation in risky behaviors: a review and synthesis of the literature with directions for future research and clinical practice. Curr Opin Psychol 3:22–29. https://doi.org/10.1016/j.copsyc.2015.01.013
Wittmann M, Paulus MP (2009) Intertemporal choice: neuronal and psychological determinants of economic decisions. J Neurosci Psychol Econ 2(2):71–74. https://doi.org/10.1037/a0017695
Wu G (1999) Anxiety and decision making with delayed resolution of uncertainty. Theory Decision 46(2):159–199. https://doi.org/10.1023/A:1004990410083
Acknowledgements
This work was supported by The National Health and Medical Research Council (NHMRC) Optimizing Personalized Care, at scale, for Young People with Emerging Mood Disorders (APP1136259) awarded to Ian B. Hickie. We wish to thank Dominic Murphy and Agnieszka Tymula for interest in our research, as well as Eran Asoulin for his valuable suggestions in the initial planning stages of this paper. I am very grateful to Siena Bordignon for proofreading the final submission of this paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Angé holds 100% shares in and is the Founder of GEM Connect Pty Ltd, a social enterprise in Australia and internationally supporting youth to enhance their decision-making. She is the Co-Director of Giving Education Meaning Ltd, a registered non-profit Australian charity that delivers arts and wellbeing programs to young adults globally. Angé holds 33% shares in and is the Co-Director of My Sound Technology Pty Ltd, delivering patent-pending music technology as mental health products internationally. Angé does not draw a salary from these organisations. Author Ian B. Hickie declares no financial interests in Angé’s companies. Angé is a Ph.D. candidate and receives a Research Training (RTP) Scholarship from the University of Sydney. Ian B. Hickie was an inaugural Commissioner on Australia’s National Mental Health Commission (2012–2018). He is the Co-Director, Health and Policy at the Brain and Mind Centre (BMC) University of Sydney, Australia. The BMC operates an early-intervention youth services at Camperdown under contract to headspace. He has previously led community-based and pharmaceutical industry-supported (Wyeth, Eli Lily, Servier, Pfizer, AstraZeneca) projects focused on the identification and better management of anxiety and depression. He was a member of the Medical Advisory Panel for Medibank Private until October 2017, a Board Member of Psychosis Australia Trust, and a member of Veterans Mental Health Clinical Reference group. He is the Chief Scientific Advisor to, and a 5% equity shareholder in, InnoWell Pty Ltd. InnoWell was formed by the University of Sydney (45% equity) and PwC (Australia; 45% equity) to deliver the $30M Australian Government-funded Project Synergy (2017–2020); a 3-year programme for the transformation of mental health services) and to lead transformation of mental health services internationally using innovative technologies.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Weinrabe, A., Hickie, I.B. A multidisciplinary approach to evaluate the impact of emotional dysregulation on adolescent decision making. Humanit Soc Sci Commun 8, 332 (2021). https://doi.org/10.1057/s41599-021-01013-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1057/s41599-021-01013-3
