
Abstract
Optical coherence tomography angiography measurements are influenced by a range of environmental factors as blood pressure and physical fitness. The present study aimed to evaluate the effects of light and dark exposure in eyes with neutral and mydriatic pupils on vessel density in the macular and optic nerve head regions, as measured using optical coherence tomography angiography (OCTA). 55 eyes of 55 healthy volunteers (28 patients with neutral pupils; 27.18 ± 4.33 years) were examined using a high-speed and high-resolution spectral-domain OCT XR Avanti system with a split-spectrum amplitude de-correlation angiography algorithm. OCTA imaging was performed after dark adaptation and after exposure to light. The vessel density data of the superficial and deep retinal macular and optic nerve head region OCT-angiogram were analyzed for these two light conditions. Through Bonferroni correction for multiple testing, the p- value was adapted from 0.05 to 0.017. In eyes with neutral pupils, a significant increase was found in the capillary region of the optic nerve head region (p = 0.002), comparing dark- and light-adaptation. In the macular region of eyes with neutral (p = 0.718) and mydriatic pupils (p = 0.043), no significant differences were observed, as were any in the optic nerve head region of the mydriatic eyes (p = 0.797). This observation suggests that light conditions could be a possible factor influencing OCTA measurements. After dark exposure, vessel density data were significantly different between eyes with neutral and mydriatic pupils (nerve head region: p < 0.0001, superficial macula: p < 0.0001, deep macula: p = 0.0025). These data warn for the effect of mydriatic drops on vessel density measurements.
Similar content being viewed by others

Introduction
The influence of light conditions on the retina is well documented. Electrophysiological tests as full-field electroretinogram describe this response as a retinal depolarization after light stimulation1. Retinal polarization changes lead to differences in energy demands and blood flow adaptation2. This complex process is called neurovascular coupling3,4,5,6. Distinct influences, e.g. flicker vs. continuous light, and lighting conditions such as scotopic and photopic illumination require a change in blood flow. This is accomplished by a group of cells of both vascular and neural origin, referred to as the neurovascular unit7.
Neurovascular coupling is not exclusively found in the retina. The brain, using 20% of the body’s energy at rest, has extensive neurovascular coupling mechanisms, which are needed to adapt to changing stimuli3,8. Neurovascular coupling is known to be disrupted in different conditions such as ischemic stroke, Alzheimer’s disease, or hypertension. Therapeutic strategies aiming to improve retinal or cerebral blood flow in diseases like ischemic stroke or hypertension require a precise understanding of this mechanism3,9.
As the retina is the most accessible part of the brain and the retinal vasculature can be visualized with non-invasive techniques, the eye is well suited to study neurovascular coupling10,11. Despite this, there have been few studies to date investigating neurovascular coupling in the eye12. Most of the published data draw conclusions about flow changes based on vascular caliber variations13,14.
OCT angiography (OCTA) is a non-invasive imaging technique that enables visualization and quantification of blood flow in the retina and in the optic nerve head (ONH). The technology has proven to be very valuable for the diagnosis and follow up of various ocular and systemic vascular diseases. As OCTA is fast and easily repeatable, it is well accepted by patients and clinicians. Since the introduction of OCTA research interest in the quantification of blood flow in the optic nerve and macular region is growing steadily15,16,17.
The present study evaluates the effects of light and dark exposure on vessel density (VD) in the retina and ONH using OCTA. The aim was to determine the feasibility of monitoring neurovascular coupling. The results were obtained in eyes with neutral pupils as well as in mydriasis in two different cohorts to exclude bias induced by post-dark adaptation pupillary constriction.
Materials and methods
Subjects
Fifty-five healthy subjects were included in this study. All investigations were performed in accordance with the declaration of Helsinki and written informed consent was obtained from all participants before imaging. The study was approved by the local ethics committee of the medical association of Westfalen-Lippe and the Westphalian Wilhelms-University of Muenster. Before imaging, a complete ophthalmic examination was performed including best corrected visual acuity, measurement of intraocular pressure (IOP), slit lamp biomicroscopy and funduscopy of the macula and ONH.
Inclusion criteria were age > 18 years and in good health, defined as the absence of cardiovascular diseases, high blood pressure, diabetes, sleep apnea and other systemic diseases18,19,20. Exclusion criteria were ocular pathologies on examination or in the patient’s history, and spherical equivalents outside the range of − 3.5 and + 3.5. Patients with any history of ophthalmic surgery or treatment, lens opacities, corneal opacities or refractive surgery were also excluded.
Study protocol
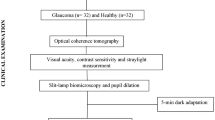
Subjects were randomly assigned to one of two groups (neutral or mydriatic pupils). Patients were not asked to undergo the cycles of dark and light adaptation with both neutral and mydriatic pupils to improve compliance (Fig. 1).

Flow chart of the study protocol.
Before OCTA imaging of the ONH and macular regions, the subjects were put at ease. Immediately after performing each OCTA measurement, systemic blood pressure and the pulse rate were determined at the left brachial artery at the height of the heart with the subject in an upright sitting position.
After dark adaptation for 25 min OCTA measurements were performed in mesopic light conditions (indirect surrounding light, 50 lx)21. The participants remained in dark adaptation during transport from the darkened room to the OCTA device by way of blindfold goggles. Subsequently, the subjects were light adapted using a 250-lx light box for 10 min followed by OCT-A measurements in mesopic light conditions. All images were recorded in the right eye by an experienced operator under the same standardized mesopic lighting conditions in the same location. Measurements of the macular and ONH region were performed in separate cycles of dark and light adaptation. The group of subjects with neutral pupils did not receive eye drops. The group of subjects with pupils in mydriasis underwent pupil dilation using 1 single drop of a tropicamide 0,5% and neosynephrin 2.5% mixture. 20 min after instillation dark adaptation was initiated.
OCT angiography
OCTA technology has been described in detail previously17,22,23,24. Imaging was conducted with a spectral domain OCT-system (AngioVue, RTVue XR Avanti SD-OCT, Optovue, Fremont, CA, USA). The device delivered volumetric scans of 304 × 304 A-scans at 70,000 A-scans per second using a light source at 840 nm. Two consecutive B-scans covering the central 3 × 3 mm2 field of the macula and the 4.5 × 4.5 mm2 ONH field were performed to compute inter-B-scan decorrelation with the SSADA algorithm. The software version used in this study included the eye tracking function (DualTrac Motion Correction, Optovue, Fremont, CA, USA).
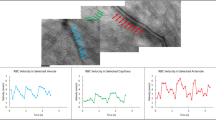
VD was then calculated by first extracting a binary image of the vessels from the grayscale OCTA en-face image, and then computing the percentage of pixels of vessels in the defined sectors or in the entire en-face image based on the binary image23. After checking for proper segmentation, VD data were evaluated in the superficial plexus (VDsM) and the deep plexus (VDdM) of the central macula and in the radial peripapillary capillary layer of the peripapillary region (VDrpcPP) (Fig. 2). For the VDprcPP, two options are available in the analysis menu: “capillary” and “all”. We opted for the capillary values, thus excluding the large vessels. These analyses were performed with proprietary software of Optovue (ReVue 2017.1.0.151). Images were excluded, when quality index was below 6 or when uncorrectable segmentation errors were present in the quantifiable region24.

Exemplary angiograms from one participant. Left column shows angiograms of optic nerve head region (a), macular superficial plexus (c) and macular deep plexus (e) after dark adaptation. The right column shows angiograms of optic nerve head region (b), macular superficial plexus (d) and macular deep plexus (f) after light adaptation.
Statistical analysis
Microsoft Excel 2010 was used for data management. Statistical analyses were performed using Prism 7.02 (GraphPad Software nc., La Jolla, USA). The sample size was calculated based on a previous study with a detected effect size (ES) = 0.73, revealing that a sample size of 23 would yield a statistical power of (1-beta) = 0.96 at alpha = 0.0514,25. OCTA data were tested for normal distribution using the D'Agostino-Pearson normality test (omnibus K2 test). Data presented as mean ± SD and median [interquartile range]. Differences between measurements were determined using the two-sided paired t-test for normal distributed data or Wilcoxon paired t-test in the case of non-normal distributed data. To compare baseline OCTA data between eyes with neutral and mydriatic pupils, the two-sided unpaired t-test for normal distributed data or Mann–Whitney t-test in the case of non-normal distributed data were instrumented. To compare the distribution of baseline OCTA data between eyes with neutral and mydriatic pupils, the two-sample Kolmogorov–Smirnov-test. For the t-tests, p-value was adapted through Bonferroni correction for multiple testing from 0.05 to 0.017. For the correlation analysis, p- value was adapted through Bonferroni correction for multiple testing from 0.05 to 0.01.
Results
55 healthy volunteers (neutral group [n = 28]: 26.88 years ± 4.91; mydriasis group [n = 27]: 27.48 years ± 3.69) were included prospectively in this study. Systemic, cardiovascular parameters (heart rate and blood pressure) and image quality index were not significantly different between eyes with neutral and mydriatic pupils. Further characteristics of the study population are summarized in Table 1.
In the group with neutral pupils, after dark adaptation, 1 optic disc image and 1 macular image, and after light adaptation, 3 optic disc images were excluded due to a low quality index. In the group with mydriatic pupils, after dark adaptation, 1 macular image, after light adaptation, 1 optic disc images and 1 macular image were excluded due to a low quality index. No projection artefacts were observed in the deep retinal plexus.
In eyes with neutral pupils, a significant increase in VD was found in the RPC layer of the peripapillary region between dark- and light-adapted states. (Fig. 3) In the macular region of eyes with neutral and mydriatic pupils, no significant differences in VD were observed, as were any in the RPC layer of the peripapillary region of the mydriatic eyes. (Table 2). Comparing baseline OCTA data between eyes with neutral and mydriatic pupils, statistically significant differences were found: VDrpcPP: p < 0.0001, VDsM: p < 0.0001, VDdM: p = 0.0025. Comparing differences in distribution of OCTA baseline data between eyes with neutral and mydriatic pupils, statistical differences were found: VDrpcPP: < 0.0001, VDsM: < 0.0001, VDdM: 0.0017.

Tukey plot of vessel density of radial peripapillary capillary layer of peripapillary area after dark and light adaptation in patient with neutral and mydriatic pupils. *Statistically significant.
A correlation analysis was performed between baseline OCTA data and several other parameters: age, intraocular tension, spherical equivalent, mean arterial pressure and heart rate. This did not reveal significant correlations. The correlation between spherical equivalent and VDdM in eyes with neutral pupils almost reached statistical significance (spearman r = 0.481, p = 0.011). The correlation between the macular quality index and VDsM in eyes with mydriatic pupils almost reached statistical significance (spearman r = 0.487, p = 0.0116).
Discussion
In this study, macular and ONH region vessel density data were analyzed in eyes with neutral and mydriatic pupils and in two light conditions: dark-adapted and light-adapted states. In eyes with neutral pupils, a significant change was found in the RPC layer of the peripapillary region between light- and dark-adapted states. In the macular region of eyes with neutral and mydriatic pupils, no significant differences were observed, as were any in the RPC layer of the peripapillary region of the mydriatic eyes. After dark exposure, vessel density data were significantly different between eyes with neutral and mydriatic pupils.
OCT-A is a much used but still relatively novel non-contact imaging technique, which can be performed easily and fast. It enables the visualization of retinal and choroidal vessels and vessels in the ONH region without the need for intravenously injected dye. OCTA therefore attracted considerable ophthalmological clinical research interest over the last 5 years17. Moreover, OCTA enables quantitative analysis of ocular flow: the repeatability of vessel density data using OCT-A has been analyzed in healthy subjects and in patients with various ocular and systemic diseases as well as in different animal models15,16,17,22,23,26,27. Consequently, an increasing amount of systemic and environmental factors have been shown to influence OCTA measurements. Neurovascular coupling effects, like light and dark adaptation, on OCTA have been studied only in eyes with neutral pupils28. Since pupil diameter is known to influence optic nerve OCT measurement, a parallel evaluation in eyes with neutral and mydriatic pupils seems reasonable29. This pilot study evaluates changes in vessel density, measured by OCTA, in response to dark and light exposure in both eyes with neutral and mydriatic pupils.
The retina is supplied by the central retinal artery and the short posterior ciliary arteries. The macular retinal circulation can be divided into four layers: radial peripapillary capillary plexus, the superficial vascular plexus, the intermediate capillary plexus and the deep capillary plexus30. The last two layers have a spider-like appearance with small feeding vessels31,32. In the peripapillary region, the radial peripapillary capillary network supplies the unmyelinated nerve fibres33,34. Roy and Sherrington hypothesized more than 100 years ago that the brain could vary the vascular supply in response to variations in functional activity35. About a century later different studies demonstrated similar phenomena for the ONH region and major retinal vessels12,36. To compensate for elevated oxygen consumption of photoreceptors in the dark, ocular perfusion increases7,10. Experiments on neurovascular coupling revealed two possible mechanisms which might act in synergy. (i) Local metabolic feedback systems, in which neural activity leads to energy demand and vasodilation, are the most traditional way to explain NVC9. (ii) Neurons are postulated to increase local blood flow directly or via astrocytes releasing vasoactive agents. This glutamate-mediated process is called functional hyperemia5,37,38.
Literature on the effects of dark adaptation on flow is not conclusive. In 1983 Feke et al. used laser Doppler techniques to demonstrate a retinal blood flow increase after the transition from light to dark39. Using bidirectional laser doppler velocimetry, Riva et al. showed an increase in diameter and blood flow velocity in major veins, taking place 5 min into dark adaptation40. However, newer studies using static registration methods as scanning laser ophthalmoscopy and retinal vessel analyzers did not find any significant increase in retinal branch diameter during dark adaptation41,42. Even more, a more recent study of Riva et al. using laser Doppler flow measurements found no change in blood flow during dark adaptation43. The present results of the peripapillary region in eyes with neutral pupils contradict the findings of Feke et al. and the earlier results of Riva et al. Of note, Riva et al. and Feke et al. measure blood flow of large vessels directly around the optic nerve, whereas our study only analyses the capillaries of the peripapillary region, disregarding the larger vessels39,40.
Dark and light stimulation has often been combined with flicker stimuli. Flicker-induced arterial and venular vasodilation have been more consistently reported in literature, especially in the inner retina, more susceptible to these stimuli. Due to technological limitations, these studies focused on the larger vessels. OCTA provides a higher axial resolution, enabling the visualization of capillaries, in combination with a depth-resolution. Instrumenting these OCTA features, Nesper et al. aimed to include light and dark adaptation, as well as flicker-stimuli. Nesper et al. reported a statistically significant increase, resp. decrease in the superficial and intermediate layers following the transition from dark to ambient light. In the deep layer they did not find a significant difference (p < 0.05)28. Additionally, they also found a significant increase in superficial layer during flicker stimulation compared to dark adaptation. They attributed this to constriction of the deep and intermediate layers and a large vessel dilation response in the superficial layer. In the macular region of eyes with neutral pupils, we do not find similar results as in Nesper et al. This incongruence might be explained by the different segmentation strategies used: Nesper and colleagues used a three-slab segmentation, whereas we used the more widespread 2-slab segmentation. The possible advantage of the latter is the arguably fewer segmentation errors since only one segmentation border must be checked. A major disadvantage is a lower sensitivity to layer-specific reactions to stimuli44,45. The three plexuses are differentially regulated. Kornfield and Newman have showed that even between the superficial, intermediate, and deep layers divergence in effects is possible. Duan et al. even found different effects to stimuli between arterioles and venules46.
The results of Nesper et al. for the superficial plexus (increase from dark to light) and the present results in the radial peripapillary capillaries (increase from dark to light) seem to be in agreement. A similar effect of a stimulus on the superficial plexus and the radial peripapillary capillaries would be plausible since the activity of the retinal nerve fiber layer is downstream of the inner retina. However, this gives nuance to the basal principle of NVC, metabolic need leading to vascular adaptation.
In general, we have to be aware of the limitation of the OCTA technique itself and the long acquisition times of OCTA in comparison with e.g., laser Doppler techniques or retinal vessel analyzer, which give an instant measurement.
Furthermore, OCTA determines for every pixel a binary response of flow and non-flow, without a clear indication of velocity or increase in perfusion47. Thus, the minute increase in perfusion by neurovascular coupling might not result in a morphological change, large enough to be observed with OCTA. This, together with the vasoconstrictive effects of mydriasis induction, could explain the absence of similar effects in eyes in mydriasis.
Of note, the comparison of macular and optic disc vessel density data of eyes with neutral and mydriatic pupils after dark exposure reveals a highly significant difference in this population. Thus, mydriasis induction by tropicamide 0.5% and phenylephrine 2.5% seems to decrease vessel density at the macula and the optic nerve. Topical phenylephrine, through α1-adrenoreceptors, has been shown by laser doppler flowmetry to induce a decrease in blood velocity in retinal arteries48. Similarly, tropicamide, through the muscarinic acetylcholine receptors, decreases retinal capillary perfusion in healthy individuals49. Literature is not conclusive on this important issue. An earlier study by Brücher et al. found no difference in OCTA parameters (macula) between neutral pupils and mydriasis in an older patient cohort with macular degeneration (induced by a tropicamide 0,5% and neosynephrin 2,5% mixture), as did Hohberger in a young population (30 persons, macula and optic disc, 0,5% tropicamide, 5% phenylephrine)29,50. However, Cheng et al. found in a small cohort (8 young subjects, 0.5% tropicamide/0.5% phenylephrine mixture) a reduced vessel density in the peripapillary region, but not in the macular region, as did Villatoro et al. (26 participants, 2.5% phenylephrine/0.5% tropicamide)51,52. These studies seem to suggest, that the capillaries at the optic nerve are more susceptible to vasoconstrictive medication than those at the macula. Cheng et al. proposes this as an evolutionary advantage, where the central vision must be protected from vasoconstriction in a fight or flight response, whereas the peripheral vision is less of important in these moments. Villatoro et al. suggests that these findings are mere aberrations induced by changes in pupil size or, alternatively, proposes that these findings are within boundaries of intra-session variation of vessel density. An important limitation for our findings is that the population with neutral pupils is not the same as the population with mydriatic pupils. For future studies, caution is warranted not to mix vessel density data acquired in different pharmacologically induced pupil conditions.
This study has several limitations. Our study population consisted of healthy subjects of a relatively young and narrow age range. Not all factors known to influence OCTA measurements were recorded and considered. Blood pressure, heart rate, eye pressure and refraction were measured and found to be in acceptable ranges, other parameters as physical fitness and hematocrit were not assessed53,54.
Pupil dilation affects OCTA measurements. The present study did not find a significant difference in quality index scores between the groups with neutral and mydriatic pupils. A near-significant correlation between the macular quality index and VDsM in eyes with mydriatic pupils was observed. This suggests an interaction between quality index and OCTA measurements. The present study was not blinded. Both the OCTA operator and the image analyst were aware of whether a test person was dark- or light-adapted before the OCTA measurement and whether pupils were neutral or in mydriasis. The OCTA operator was highly experienced in both neutral and mydriatic pupils. The analyst was not blinded since no qualitative assessment of his part was asked outside of artefact control and segmentation check/correction.
No direct conclusions should be drawn for subjects with systemic or ocular pathologies, subjects of other age groups or OCTA systems using an alternative segmentation system. Aditionally, these results are only applicable on subjects with neutral pupils and pupils dilated with a single drop of a tropicamide 0.5% and neosynephrin 2.5% mixture. Other protocols for mydriasis induction may have different effects on the retinal vasculature and influence OCTA measurements55.
Rather than submitting the subjects to 4 cycles of dark and light adaptation (2 with neutral pupils, 2 in mydriasis), we opted, to improve compliance, thus for 2 groups (neutral and mydriatic pupils), undergoing each 2 cyles of dark and light adapation.
Also, the data distribution in the two groups was different. For this reason, the comparison of OCTA data between the two groups (neutral and mydriatic pupils) must be handled with care.
Pupil size can have an impact on vessel density measurements. In this study, we did not measure the pupil size to prioritize OCTA measurements and to be able to measure a maximal effect of early dark and light adaptation. Furthermore, we did not record the pupil size in neutral pupils and in mydriasis at baseline. Considering this parameter in future studies would be valuable51.
In conclusion, this study reveals significant changes in optic nerve OCTA parameters in eyes with neutral pupils. This was not found in macular OCTA parameters in eyes with neutral and mydriatic pupils, neither in optic disc OCTA parameters in eyes in mydriasis. This observation suggests that light conditions could be a possible factor influencing OCTA measurements. The basis of neurovascular coupling, metabolic need leading to vascular adaptation, does not seem consistent with our current findings. Our results lay emphasis on the complexity of regulation mechanisms in the different regions and layers of the macula and optic nerve. Additionally, these data warn for the effect of mydriatic drops on vessel density measurements. Further studies are needed to evaluate effects of alternative stimuli protocols, concentration, and compositions of mydriasis-inducing agents.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Robson, A. G. et al. ISCEV guide to visual electrodiagnostic procedures. Doc. Ophthalmol. 136, 1–26 (2018).
Masland, R. H. Processing and encoding of visual information in the retina. Curr. Opin. Neurobiol. 6, 467–474 (1996).
Muoio, V., Persson, P. B. & Sendeski, M. M. The neurovascular unit: Concept review. Acta Physiol. 210, 790–798 (2014).
Marc, R. E. et al. Heterocellular coupling between amacrine cells and ganglion cells. Front. Neural Circuits 12, 90 (2018).
Prada, D. et al. Autoregulation and neurovascular coupling in the optic nerve head. Surv. Ophthalmol. 61, 164–186 (2016).
Son, T. et al. Functional optical coherence tomography of neurovascular coupling interactions in the retina. J. Biophoton. 11, e201800089 (2018).
Linsenmeier, R. A. Effects of light and darkness on oxygen distribution and consumption in the cat retina. J. Gen. Physiol. 88, 521–542 (1986).
Iadecola, C. The neurovascular unit coming of age: A journey through neurovascular coupling in health and disease. Neuron 96, 17–42 (2017).
Attwell, D. et al. Glial and neuronal control of brain blood flow. Nature 468, 232–243 (2010).
Kur, J., Newman, E. A. & Chan-Ling, T. Cellular and physiological mechanisms underlying blood flow regulation in the retina and choroid in health and disease. Prog. Retin. Eye Res. 31, 377–406 (2012).
Newman, E. A. Functional hyperemia and mechanisms of neurovascular coupling in the retinal vasculature. J. Cereb. Blood Flow Metab. 33, 1685–1695 (2013).
Riva, C. E., Logean, E. & Falsini, B. Visually evoked hemodynamical response and assessment of neurovascular coupling in the optic nerve and retina. Prog. Retin. Eye Res. 24, 183–215 (2005).
Nagel, E. Flicker observation light induces diameter response in retinal arterioles: A clinical methodological study. Br. J. Ophthalmol. 88, 54–56 (2004).
Kotliar, K. E., Vilser, W., Nagel, E. & Lanzl, I. M. Retinal vessel reaction in response to chromatic flickering light. Graefes Arch. Clin. Exp. Ophthalmol. 242, 377–392 (2004).
Alnawaiseh, M., Schubert, F., Heiduschka, P. & Eter, N. Optical coherence tomography angiography in patients with retinitis pigmentosa. Retina https://doi.org/10.1097/IAE.0000000000001904 (2017).
Alnawaiseh, M., Lahme, L., Müller, V., Rosentreter, A. & Eter, N. Correlation of flow density, as measured using optical coherence tomography angiography, with structural and functional parameters in glaucoma patients. Graefes Arch. Clin. Exp. Ophthalmol. 256, 589–597 (2018).
Kashani, A. H. et al. Optical coherence tomography angiography: A comprehensive review of current methods and clinical applications. Prog. Retin. Eye Res. 60, 66–100 (2017).
Shi, W.-Q. et al. Retinal microvasculature and conjunctival vessel alterations in patients with systemic lupus erythematosus: An optical coherence tomography angiography study. Front. Med. 8, 724283 (2021).
Monteiro-Henriques, I., Rocha-Sousa, A. & Barbosa-Breda, J. Optical coherence tomography angiography changes in cardiovascular systemic diseases and risk factors: A review. Acta Ophthalmol. 100, e1–e15 (2022).
Alnawaiseh, M. Optical coherence tomography angiography for evaluation of the microcirculation in systemic diseases. Ophthalmol. Z. Dtsch. Ophthalmol. Ges. 116, 712–713 (2019).
Robson, A. G. et al. ISCEV guide to visual electrodiagnostic procedures. Doc. Ophthalmol. Adv. Ophthalmol. 136, 1–26 (2018).
Jia, Y. et al. Quantitative optical coherence tomography angiography of choroidal neovascularization in age-related macular degeneration. Ophthalmology 121, 1435–1444 (2014).
Coscas, F. et al. Normative data for vascular density in superficial and deep capillary plexuses of healthy adults assessed by optical coherence tomography angiography. Investig. Opthalmol. Vis. Sci. 57, 211 (2016).
Lauermann, J. L. et al. Impact of eye-tracking technology on OCT-angiography imaging quality in age-related macular degeneration. Graefes Arch. Clin. Exp. Ophthalmol. 255, 1535–1542 (2017).
Zinn, S. et al. Effect of high-intensity interval training in patients with type 1 diabetes on physical fitness and retinal microvascular perfusion determined by optical coherence tomography angiography. Microvasc. Res. 132, 104057 (2020).
Brand, C. et al. Aberrant ocular architecture and function in patients with Klinefelter syndrome. Sci. Rep. 7, 13528 (2017).
Alnawaiseh, M. et al. Quantitative analysis of retinal perfusion in mice using optical coherence tomography angiography. Exp. Eye Res. 164, 151–156 (2017).
Nesper, P. L. et al. Hemodynamic response of the three macular capillary plexuses in dark adaptation and flicker stimulation using optical coherence tomography angiography. Investig. Opthalmol. Vis. Sci. 60, 694 (2019).
Brücher, V. C. et al. Influence of mydriasis on optical coherence tomography angiography imaging in patients with age-related macular degeneration. PLoS ONE 14, e0223452 (2019).
Zhang, M. et al. Projection-resolved optical coherence tomographic angiography. Biomed. Opt. Express 7, 816 (2016).
Yu, P. K. et al. Microstructure and network organization of the microvasculature in the human macula. Investig. Opthalmol. Vis. Sci. 51, 6735 (2010).
Weinhaus, R. S., Burke, J. M., Delori, F. C. & Snodderly, D. M. Comparison of fluorescein angiography with microvascular anatomy of macaque retinas. Exp. Eye Res. 61, 1–16 (1995).
Snodderly, D., Weinhaus, R. & Choi, J. Neural-vascular relationships in central retina of macaque monkeys (Macaca fascicularis). J. Neurosci. 12, 1169–1193 (1992).
Henkind, P. Radial peripapillary capillaries of the retina. I. Anatomy: Human and comparative. Br. J. Ophthalmol. 51, 115–123 (1967).
Roy, C. S. & Sherrington, C. S. On the regulation of the blood-supply of the brain. J. Physiol. 11, 85–158 (1890).
Garhöfer, G. et al. Diffuse luminance flicker increases blood flow in major retinal arteries and veins. Vis. Res. 44, 833–838 (2004).
Offenhauser, N., Thomsen, K., Caesar, K. & Lauritzen, M. Activity-induced tissue oxygenation changes in rat cerebellar cortex: Interplay of postsynaptic activation and blood flow: Oxygen consumption in rat cerebellum. J. Physiol. 565, 279–294 (2005).
StLawrence, K. S., Ye, F. Q., Lewis, B. K., Frank, J. A. & McLaughlin, A. C. Measuring the effects of indomethacin on changes in cerebral oxidative metabolism and cerebral blood flow during sensorimotor activation. Magn. Reson. Med. 50, 99–106 (2003).
Feke, G. T., Zuckerman, R., Green, G. J. & Weiter, J. J. Response of human retinal blood flow to light and dark. Invest. Ophthalmol. Vis. Sci. 24, 136–141 (1983).
Riva, C. E., Grunwald, J. E. & Petrig, B. L. Reactivity of the human retinal circulation to darkness: A laser Doppler velocimetry study. Invest. Ophthalmol. Vis. Sci. 24, 737–740 (1983).
Von Hanno, T., Sjølie, A. K. & Mathiesen, E. B. Retinal vascular calibre and response to light exposure and serial imaging. Acta Ophthalmol. 92, 444–448 (2014).
Barcsay, G., Seres, A. & Nemeth, J. The diameters of the human retinal branch vessels do not change in darkness. Investig. Opthalmol. Vis. Sci. 44, 3115 (2003).
Riva, C. E., Logean, E., Petrig, B. L. & Falsini, B. Effet de l’adaptation à l’obscurité sur le flux rétinien1. Klin. Monatsblätter Augenheilkd. 216, 309–310 (2000).
Kornfield, T. E. & Newman, E. A. Regulation of blood flow in the retinal trilaminar vascular network. J. Neurosci. 34, 11504–11513 (2014).
Leahy, C., Radhakrishnan, H., Weiner, G., Goldberg, J. L. & Srinivasan, V. J. Mapping the 3D connectivity of the rat inner retinal vascular network using OCT angiography. Investig. Opthalmol. Vis. Sci. 56, 5785 (2015).
Duan, A., Bedggood, P. A., Bui, B. V. & Metha, A. B. Evidence of flicker-induced functional hyperaemia in the smallest vessels of the human retinal blood supply. PLoS ONE 11, e0162621 (2016).
Jia, Y. et al. Split-spectrum amplitude-decorrelation angiography with optical coherence tomography. Opt. Express 20, 4710–4725 (2012).
Takayama, J. et al. Topical phenylephrine decreases blood velocity in the optic nerve head and increases resistive index in the retinal arteries. Eye 23, 827–834 (2009).
Harazny, J. M., Schmieder, R. E., Welzenbach, J. & Michelson, G. Local application of tropicamide 0.5% reduces retinal capillary blood flow. Blood Press. 22, 371–376 (2013).
Hohberger, B., Müller, M., Hosari, S. & Mardin, C. Y. OCT-angiography: Mydriatic phenylephrine and tropicamide do not influence retinal microvasculature in macula and peripapillary region. PLoS ONE 14, e0221395 (2019).
Villatoro, G. et al. Impact of pupil dilation on optical coherence tomography angiography retinal microvasculature in healthy eyes. J. Glaucoma 29, 1025–1029 (2020).
Cheng, J., Yu, J., Jiang, C. & Sun, X. Phenylephrine affects peripapillary retinal vasculature: An optic coherence tomography angiography study. Front. Physiol. 8, 996 (2017).
Yang, J. et al. Hematocrit dependence of flow signal in optical coherence tomography angiography. Biomed. Opt. Express 8, 776 (2017).
Nelis, P. et al. Correlation analysis of physical fitness and retinal microvasculature by OCT angiography in healthy adults. PLoS ONE 14, e0225769 (2019).
Elbeyli, A. & Kurtul, B. E. The influence of topical cyclopentolate instillation on peripapillary and macular microvasculature measured by optical coherence tomography angiography in healthy individuals. J. Curr. Ophthalmol. 33, 437–443 (2021).
Acknowledgements
We acknowledge support by Open Access Publication Fund of University of Muenster.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
P.N. and A.N. designed and supervised the study, enrolled participants, and performed examinations. P.N. and A.N. interpreted data. P.N. and V.B. wrote the manuscript. N.E. and M.A. provided resources. All authors critically reviewed the manuscript and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nelis, P., Nieweler, A., Brücher, V. et al. Light conditions influence optic nerve OCT angiography parameter in healthy subjects with neutral pupils. Sci Rep 13, 9154 (2023). https://doi.org/10.1038/s41598-023-36069-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-36069-5
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
