
Abstract
The aim of the present study was to explore the influence of anxiety and fear of COVID-19 on vaccination hesitancy among Slovenian postsecondary students. A cross-sectional study using a set of previously tested instruments and ad hoc questions created by the authors was chosen as the method to gain insight into various health and sociodemographic aspects of Slovenian postsecondary students affected by the COVID-19-induced closures and suspensions of educational activities at tertiary educational institutions (N = 5999). Overall, 39.7% of participating students expressed an intention to get vaccinated at the first possible opportunity, whereas 29.2% expressed no intent to do so. The highest vaccine hesitancy was observed among prospective teachers (50.3%) and the lowest among prospective physicians (5,7%). When examining the role of anxiety and fear of COVID-19 on the Slovenian postsecondary students’ intentions to get vaccinated the results of logistic regression showed that only fear of COVID-19 played a mild and significant role.
Similar content being viewed by others

Introduction
Vaccination and vaccination campaigns are widely recognized as the greatest public health achievements in human history1,2. Yet, despite solid evidence that the benefits of vaccination far outweigh any potential harms, there is a worldwide hesitancy to vaccinate3,4,5 resulting in unnecessary health problems and morbidity from preventable diseases. The problem is so severe that vaccine hesitancy has been named one of the top ten global health problems by the World Health Organisation6. In addition to existing surveys on vaccines, such as the measles vaccine, vaccine hesitancy and even resistance to vaccines and vaccination was again demonstrated in the COVID-19 pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)7.
According to the official data, the first infection with a novel coronavirus was registered in Slovenia on the 4th of March 2020 and the vaccination campaign started on the 27th of December 2020 for the vaccination of people older than 80 years, health care workers and residents of nursing homes. At the time of questionnaire submission (February–March 2021), the first doses of vaccine were available to the most vulnerable population groups aged from 18 to 65 years, which included vulnerable postsecondary students as a target population. However, the decision to get vaccinated was a voluntary decision of each citizen in Slovenia8,9,10. While there are parts of the world where vaccines against COVID-19 are still not fully available, there are also parts of the world, especially in rich countries like Slovenia, where people can choose to get vaccinated and the availability of vaccines is not a reason not to get vaccinated11. This raises the questions: why do so many people refuse vaccination, and secondly, what are the reasons for the refusal.
As postsecondary students are of legal age, they are fully responsible for their own decisions, including the decision to get vaccinated or not. Research shows that the prevalence of vaccination hesitancy among postsecondary students ranges between 13 and 19.3%12,13. Lower levels of vaccination hesitancy were observed among medical students—10.6% in India14. On the other hand, the global prevalence of COVID-19 vaccination hesitancy among students/trainees in healthcare were reported to be 18.9%15. Even higher levels of COVID-19 vaccination rejection was found among dental students in a global study involving 22 countries—22.5% were hesitant and 13.9% rejected the vaccine16. However, the refusal to be vaccinated raises additional questions as higher levels of fear relating to the infection with SARS-CoV-2 are reported among postsecondary students compared to other age groups17. Moreover, a positive correlation between fear of COVID-19 and anxiety was also observed, especially among female students17,18. Thus, an argument can be made that given their higher levels of fear of COVID-19 and anxiety they would be more inclined to get vaccinated for COVID-19, which was also found by various studies19,20,21.
Yet many factors can negatively influence the intentions and implementation of vaccination campaigns, which can have devastating effects not only on the health of individuals but also on society as a whole. Therefore, an understanding of the factors that contribute to vaccination hesitancy is essential. The majority of postsecondary students’ physical health may not be as affected by COVID-19 as more vulnerable groups are (e.g., elderly, immunocompromised, chronically ill), but they are an active part of the community and potentially active spreaders of the virus. Moreover, they will act as gatekeepers or promoters of maladaptive behaviours in the future, as many of them will act as influencers and decision makers. This applies, for example, to the use of other vaccines against life-threatening diseases for their children or future behaviours in response to new outbreaks.
Therefore, the aim of the present study is to examine the influence of fear of COVID-19 and anxiety on Slovenian postsecondary students’ intentions to get vaccinated when the vaccine would be available. To the best of our knowledge is the first study that examined the entire post-secondary student population in Slovenia.
The results may serve as a basis for a better understanding of vaccination hesitancy among students and enable the development of targeted interventions and campaigns against it. The research questions that guided our study were as follows:
- RQ 1:
-
How great are anxiety and fear among the students?
- RQ2:
-
Are students a one-dimensional population in terms of intent to get vaccinated against COVID-19?
- RQ 3:
-
Can anxiety and fear of COVID-19 be used as predictors of willingness to get vaccinated or not?
- RQ 4:
-
Is there a difference between medicine and healthcare students in terms of their intentions relating to vaccination against COVID-19?
Methodology
Participants and procedure
The present study is part of the research titled “Students’ experience of COVID-19 epidemic” aimed to assess and understand the impact of COVID-19 and related measures on the postsecondary students’ mental health22,23. A cross-sectional study was designed comprising psychological instruments, sociodemographic questions and ad hoc questions created by authors. All methods were carried out in accordance with relevant guidelines and regulations.
The participants were postsecondary students enrolled in Slovenian’ higher education institutions. Thus, for the present study participants that were at the time of the study enrolled as full-time students were assessed as eligible. At the time of the present study that included approximately 60.600 students24. They were recruited online via a web-based survey platform (https://www.1ka.si/); the data collection took place between the 9th of February and the 8th of March 8 2021, on the whole territory of Slovenia. Simple random sampling was used—invitation letters to participate in the study were sent to all universities, private faculties, and student organisations with a request to forward the invitation to all their students. To get as much feedback as possible a reminder letter with the invitation to participate was sent to all addressees after one week and after another week to those from whom we had not received any feedback.
At the beginning of the questionnaire, the participants were informed about various aspects of the study, including their rights to voluntarily participate or withdraw from the study and that the data will be processed in accordance with EU and Slovenian legislation. Thereafter the participants were asked to give consent to participate in the research and state that they have read the information regarding the research they intend to participate in. Therefore, informed consent was obtained from all the participants before they filled out the questionnaire in the present study. The sample structure is presented in Table 1.
Ethical approval to conduct the study was obtained from the National Medical Ethics Committee of the Republic of Slovenia (NMEC), Ministry of Health (No. 0120-48/2021/3). The entire methodology—from creating the questionnaire to delivery and processing of the data was conducted in accordance with ethical and professional guidelines and regulations.
Instruments and questions
The Fear of COVID-19 Scale (FCV-19S)25 is a seven-item scale assessing fear of COVID-19 (hereafter: FCOV). The seven items (see Table 4) are scored on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), with scores ranging from 7 to 35. The higher the score, the greater the fear of COVID-19. According to references25,26 the scale is unidimensional with strong psychometric characteristics and reliability expressed by Cronbach’s alpha above 0.80 in the general population as well in the population of postsecondary students in the interest of the study27,28. In some studies, a different factorial structure was found. For example, Reznik and colleagues28 reported two components based on Principal Component Analysis with Varimax rotation.
The Generalized Anxiety Disorder Questionnaire (GAD-7)29 is a 7-item self-report measure to assess the severity of anxiety and its symptoms according to DSM-IV criteria. Participants rated how often they experienced anxiety symptoms in the past 2 weeks on a 4-point Likert scale from 0 (not at all) to 3 (almost every day). Total scores range from 0 to 21, with a cut-off score of 10 identifying instances of generalized anxiety disorder. The following cut-offs correlate with the level of anxiety severity and scores ≥ 5, ≥ 10, and ≥ 15 are representing mild, moderate and severe anxiety symptom levels.
Intention to be vaccinated against COVID-19 was examined by asking the participants “Do you intend to get vaccinated?”. Three responses were offered, and they should tick one of them:
Yes, I will vaccinate at the first opportunity.
Yes, I will vaccinate, but later.
No, I do not intend to be vaccinated.
The responses were scored 2, 1, and 0, respectively. At the time of the data collection (February–March 2021) and in line with the vaccination plans communicated by the Slovenian authorities, postsecondary level students were not being vaccinated. The exception to the rule was a minority of students with a chronic disease with the risk of severe complications caused by the infection, for all the others vaccination was only foreseen in some uncertain future. Therefore, it was not possible to measure their actual behaviour (to opt, opt-out or postpone decision) based on the actual offer of vaccination but their behavioural intention30 toward something that was an option to happen in an uncertain future.
Sociodemographic data examined in the present study included gender, field of study and educational level.
Statistical analyses
Constructs anxiety (ANX) measured by GAD-7 and fear of Covid-19 (FCOV) assessed by FCV-19S, were handled in a similar way. Because the sums of items in the constructs were of interest after an initial data screening, data sets of respondents with missing data were listwise deleted from the poll. Each variable was screened for measures of central tendencies, skewness, and kurtosis. Cronbach’s alphas were calculated as a measure of reliability. Before proceeding to Exploratory Factorial Analysis (EFA) the data matrices were inspected by use of KMO and Barlett’s test. With the application of Principal Component Analysis (PCA) with Direct Oblimin Rotation component (factor) structure of the constructs was explored.
A complete case analysis approach was applied, which resulted in a difference in the reported number of respondents in different analyses31. Cases with missing data were excluded from the poll by use of listwise deletion in correlational, regression, and exploratory factor analyses. Effect sizes were calculated as Eta square (η2) with cut-off values of 0.01 for small, 0.06 for medium, and 0.14 for large effect.
To the best of our knowledge, the FCV-19S was used in Slovenia for the first time and therefore, the initial validation was conducted. The choice was Principal Component Analysis (PCA) with a Direct Oblimin Rotation. The cut-off value of the Kaiser–Meyer–Olkin (KMO) measure of ≥ 0.8 was taken as empirical evidence of the suitability of the data matrix. Because items were conceptual similar even in the case of multiple factors, it was assumed they would be correlated27. For the FCV-19S assessment, Cronbach's alpha of 0.80, minimum inter-item correlations ranging from 0.15 to 0.50, and minimum corrected item-total correlations of 0.30 were used as indicators of internal consistency reliability.
Because we were not so much interested in the predictive role of each of the items forming scales the sum of items was used as a predictor of intention to be vaccinated. Binary logistic regression was a choice and the Spearman correlation coefficient was used to assess the connections between variables.
IBM SPSS® Version 28 was used to perform calculations. Additionally, we believed an EFA was more appropriate than a confirmatory factor analysis (CFA) because previous studies did not all find the same, one-factor solution across samples from different nations and languages. Furthermore, this is the recommended approach when conducting the first psychometric evaluation of a newly translated measure, regardless of the rigour of the translation method32. Given the conceptual similarity among items, we assumed that if there were multiple factors, they would be correlated. Thus, we conducted a PCA with a Direct Oblimin rotation. Based on recommendations by Clark and Watson33, we considered our sample size sufficiently large to conduct an PCA on the seven-item Fear of COVID-19 Scale. As recommended by Field34, we used a cut-off of the Kaiser–Meyer–Olkin (KMO) measure of ≥ 0.8 as empirical evidence of a sufficiently large sample size for factor analysis.
Results
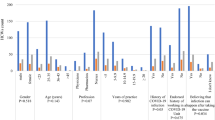
In Table 2, the results of postsecondary students’ intentions to be vaccinated are presented.
Results are by no means encouraging because only approximately 40% of participants expressed intentions to be vaccinated at the first opportunity and about 30% reported not having any such intentions.
At the first glance at Table 3, it can be recognized that the highest proportion of students that have expressed the intention to be vaccinated are medical students. The result could be interpreted in the light of better health information and attitudes; however, the gap in the intentions to get vaccinated at the first opportunity between the medical students (82.9%) and students of healthcare (34.7%) is not easily commented in terms of misinformation. The highest number of students that expressed no intention to get vaccinated (50.3%) are prospective teachers.
Validation of the Slovenian version of the Fear of COVID scale
In the analysis were included data provided by 4691 students for whom we collected all data of interest. Even, if possible, we do not apply data imputation but use listwise deletion instead. Cronbach’s alpha of the scale was 0.83, and deletion of any item will result in a lower value.
The value of Kaiser–Meyer–Olkin Measure of Sampling Adequacy (KMO) was 0.84 and the results of Bartlett's Test of Sphericity were: Chi-square = 13,425.03; df = 21; p < 0.001, which allows the intended factor analysis.
Even if it is supposed that the scale is unidimensional, the two components were extracted explaining about 58% of the variance (Table 4). Both components correlate (r = 0.561; p < 0.001). In the first component items are grouped to reflect physical harm or even death, where students generally disagree with such fears. In the second component items reflect psychological conditions, where numbers are much higher.
Validation of the Slovenian version of the Generalized Anxiety Disorder questionnaire (GAD-7) scale
The value of Kaiser–Meyer–Olkin Measure of Sampling Adequacy (KMO) was 0.94 and the results of Bartlett's Test of Sphericity were as follows: Chi-square = 32,412.33; df = 21; p < 0.001, which allows intended factor analysis. Cronbach’s alpha of the GAD-7 within the present study is 0.940. The PCA was conducted and according to the results GAD-7 is a unidimensional tool, which confirms the findings of their authors, and the first component (Eigenvalue = 5.176) explains 73.94% of the variance. Due to the proprietary restrictions, analysis of individual items is not provided.
Correlation between constructs ANX and FCOV
Spearman’s correlation coefficient rho between GAD-7 and FCV-19S (N = 4665) was 0.301 (CI95% 0.274–0.328) at the p < 0.001 level. Additionally, correlations between GAD-7 and both components emerging from FCV-19S, as a result of PCA (see Table 4) were calculated. It appears that sums calculated from items of both components (F1 = sum of FCOVcdeg; F 2 = sum of FCOVabe) correlate positively with GAD-7 (Rho = 0.301 (CI 0.273–0.327). More specifically, correlation between F2 and GAD-7 was a little bit higher (Rho = 0.301 (CI 0.273–0.327) than between F1 and GAD-7 (Rho = 0.235 (CI 0.206–0.262). All correlations were statistically significant at the p < 0.001 levels.
Results of the logistic regression
The answer to the question about the intention to vaccinate (still postponed in the uncertain future at the time of the survey) was exclusive for each respondent. Consequently, the choice of one option excludes the other two options, so the binary logistic regression was chosen. Based on previous correlation analysis results, the independent variables in the equations were the sums of GAD-7 (ANX) and FCV-19S (FCOV) and each of the three options offered as outcome variables.
From the results of regression analyses (Betas), presented in Table 5, it can be concluded that Anxiety (ANX) and Fear of Covid-19 (FCOV) are most probably not major causes of vaccination hesitancy. Differences between the three groups are minor and statistically significant at p < 0.001 levels only for FCOV as positive predictor of intention to be vaccinated immediately, and negative in intentions not to get a vaccine. ANX is very weak predictor (p < 0.01) of rejection of vaccination.
It can be revealed that differences in anxiety (F (N = 5392, df = 2) = 2.092, p = 0.123) are minor. Differences in FCOV scale (F (N = 4684, df = 2) = 60.343, p < 0.001) shows a decreasing trend, what can lead to a conclusion that fear is a mild driver toward vaccination. The finding is supported by the value of Eta squared (0.025, CI 0.017–0.034), which indicates a small effect.
We continued with the analysis of data from two subgroups, namely prospective physicians (medical students) and prospective healthcare workers, which in our opinion will be most influential on the general public’s intentions to be vaccinated.
Upon examining the results of logistic regression (Table 6), it can be observed that ANX and FCOV have a statistically significant (p < 0.05) influence on their decision to get vaccinated as soon as possible but not them who decided to postpone it. Additionally, FCOV is a significant (p < 0.05) negative predictor for reporting no intentions to get vaccinated.
Similar to the results of the entire test population, there were small and statistically not significant differences in terms of levels of ANX (Eta squared: 0.004, CI 0.00–0.020; p = 0.404) and FCOV (Eta squared: 0.018, CI 0.00–0.048; p = 0.029) among medical students as well (Table 6).
As evident in Table 7, FCOV had a statistically significant effect at p < 0.001 on healthcare students’ intent not to get vaccinated, but not on their intentions to obtain the vaccination. ANX once again did not play a statistically significant (p > 0.001) role in students’ expressed intentions to get vaccinated or to decline the vaccination.
By examining the results of ANOVA test, it can be observed in Table 8 that differences in anxiety levels (F (N = 5392, df = 2) = 0.234, p = 0.791) were small (Eta squared: 0.001, CI 0.00–0.008, p = 0.404). However, the differences in FCOV scale (F (N = 5392, df = 2) = 9.501) were statistically significant (p < 0.001) with a small to medium effect. The finding is supported by the value of Eta squared (0.036, CI 0.009–0.070).
Discussion
The aim of the present study was to explore the influence of anxiety and fear of COVID-19 on vaccination hesitancy among Slovenian postsecondary students. The data collection used in the present study was conducted in February 2021 when the vaccine was not fully accessible to the general population, but was distributed in line with the governmental priority plan. Thus, in the present study, the postsecondary students’ intentions for future behaviour were measured. More specifically, their intentions to get vaccinated at the first opportunity, to get vaccinated at a later point or not get vaccinated.
Overall, 39.7% of participating students expressed an intention to get vaccinated at the first possible opportunity, whereas 29.2% expressed no intent to do so. These results are not encouraging as the level of vaccine hesitancy among postsecondary students reported by other researchers rage between 13% and 19.3%12,13 Although in the present study the highest vaccine hesitancy was observed among prospective teachers (50.3%), the levels of vaccine hesitancy among participating healthcare students were almost twice as high compared to the results of the review that involved studies from 39 countries—34% vs. 18.9% respectively15. On the other hand, only 5.7% of participating medical students (which involved also dental medicine students) reported no intentions to get vaccinated. This percentage was much lower compared to the Indian medical students where 10.6% expressed vaccine hesitancy and dental students where 13.9% rejected the vaccine and 22.5% expressed hesitancy16.
When examining the role of anxiety and fear of COVID-19 on the Slovenian postsecondary students’ intentions to get vaccinated the results showed that only fear of COVID-19 played a mild and significant role. More specifically, when students reported higher levels of fear of COVID-19 they expressed less vaccine hesitancy intentions. Similar results were observed upon inspection of intentions to get vaccinated among healthcare students and medical students.
Moreover, anxiety was found to have a significant role in expressed intentions to get vaccinated at the first possible opportunity only among the medical students, and played a weak statistically significant role among tertiary students’ group that reported no intentions to obtain the vaccination when it will become accessible. However, these weak statistically significant effects could also have emerged due to the large sample size, which could potentially cause small differences to become statistically significant. Indeed other researchers also reported fear of COVID-19 to have a role in the vaccination hesitancy among postsecondary students, but they have found anxiety to have a significant role as well17,18,19,21.The difference in the reported influence of anxiety on vaccination hesitancy could be due to the different psychometric tools used for measuring anxiety. In the present study, GAD-7 was used to assess anxiety, while Bendau and colleagues19 used the COVID-19-Anxiety Questionnaire, which measures phobic anxiety symptoms related to the COVID-19 pandemic35, and Nazli and colleagues21 used COVID-19 Phobia Scale36 for measuring fear, anxiety and related behavioural changes during the COVID-19 pandemic. However, Kassim and colleagues17 used The Depression Anxiety Stress Scale (DASS37), and Alici and Copur18 used the Beck Anxiety Inventory (BAI38)—both scales were found to yield similar results as GAD-739,40. Therefore, a conclusion as to why anxiety appears not to have played a strong role in the Slovenian postsecondary students’ in their intentions regarding the COVID-19 vaccination cannot be easily made.
An argument could be made that medical students have more vaccine-related knowledge and can therefore make more educated decisions compared to most of the other student groups. This could potentially explain why the fear of COVID-19 and anxiety played a role in the medical students’ intentions to obtain vaccination as soon as it becomes available to them in the future. However, despite healthcare students also having more knowledge relating to vaccinations compared to non-healthcare students, the results in the present study showed high levels of vaccination hesitancy among them. In their review, Mustapha and colleagues15 identified various reasons for the healthcare students’ hesitancy, which among others involved the following: vaccination safety concerns (effectiveness, side effects, the rapidness of the vaccine development, etc.), mistrust in the government and their agencies, anti-vaccination beliefs/attitudes. Likewise, Riad and colleagues16 identified insufficient knowledge regarding the COVID-19 vaccine safety and government and pharmaceutical industry mistrust as having a significant impact on vaccination hesitancy. Moreover, they found that the availability of vaccines in their local health centre promoted students’ acceptance of COVID-19 vaccination and that the gradual increase in the levels of vaccine acceptance in the USA might be positively associated with the actual availability of vaccination which is proven to be effective and safe16.
Considering all of the aforementioned vaccination deterring factors identified by researchers, there are several possible explanations why anxiety did not play a greater role in Slovenian postsecondary students’ expressed intentions to get vaccinated or not. The first potential explanation could be derived from the theory of planned behaviour30. The theory proposes that behaviour results from behavioural intentions that stem from attitudes towards the behaviour (i.e. beliefs about the outcome having positive or negative consequences), subjective norms (i.e. perceived social pressure to engage or not) and perceived behavioural control (i.e. one’s ability to carry out the targeted behaviour). The polarisation of the Slovenian public regarding the question of vaccination for COVID-19 (subjective norms), together with postsecondary students being considered as a low-risk group for COVID-19-related complications (attitudes) could have had a greater deterring effect to get vaccinated than anxiety promoting effect to do so. Fear of COVID-19, on the other hand, could have increased the participants’ belief that the cost of not getting vaccinated would be greater than getting vaccinated (attitudes) and thus reduce their vaccination hesitancy.
Secondly, at the time of the present study, the vaccination was not yet available in the local healthcare centres; research on side effects, vaccine effectiveness and potential different outcomes across various groups was still scarce. More specifically, affective forecasting bias, e.g. expectations bias, could have led them to believe that the negative consequences of vaccination for their well-being would be greater than what they really are and thus decide against vaccination. Indeed, the results of the present study showed that anxiety was a positive predictor for the tertiary student group reporting no intentions to get vaccinated in the future, while having no significant impact on the intentions to get vaccinated. Moreover, fear of COVID-19 was found to be a significant negative predictor for having no intentions to get vaccinated and was a significant positive predictor for intending to be vaccinated as soon as possible. Therefore, it appears that some of the students’ anxiety could reflect the mistrust of vaccination as, at the time of the present research, it was not yet available to students at the local health centres16 and thus, had a deterring effect on students’ intentions to get vaccinated in the future, especially if the fear of COVID-19 was low at the same time.
Lastly, the anxiety symptoms reported by the participants could be the result of other factors not related to the COVID-19 vaccination. For example, history of anxiety and/or depressive disorder41, governmental measurements aimed at reducing the spread of COVID-19, change in studying format (i.e. forced distant online learning)42, worries relating to the health of their family members43 and worry about social support44 have been linked to increased levels of anxiety during the COVID-19 pandemic among postsecondary students.
However, this study had limitations as well. Firstly, it did not explore the influence of various factors on vaccination hesitancy. For example, gender, year of study, urban vs rural living environment, level of COVID-19-related knowledge, financial status and history of mental health difficulties13,45,46,47,48. All of these factors would offer a better insight into the vaccination hesitancy among Slovenian postsecondary students. Moreover, a psychometric tool designed to measure anxiety particularly related to COVID-19 (e.g., the COVID-19-Anxiety Questionnaire) would enable a better distinction between postsecondary students whose anxiety stems from COVID-19 factors and those whose anxiety emerged as a result of other factors. As this study had a cross-sectional design, a follow-up on the realisation of the expressed intentions by the participants regarding the vaccination was not possible.
Future research should explore more in-depth the influence of various factors on vaccination hesitancy. Furthermore, additional research is needed to determine the effects of the vaccine and COVID-19 knowledge on the vaccination hesitancy as the results of different research are inconsistent13,46. Addressing this question would also provide a better insight into why healthcare students express high levels of vaccination hesitancy and medical students do not, while both are considered to have a great amount of knowledge regarding the aforementioned topics. Additionally, as the social norms affect our behaviour, participants’ perception of social norms relating to vaccination hesitancy should be assessed as well when exploring the topic of vaccination hesitancy.
Not only did the COVID-19 pandemic bring numerous changes into our everyday life, but also opened a social dilemma—to get vaccinated or not to get vaccinated for COVID-19. The Slovenian postsecondary students overall reported low intentions to get vaccinated when the vaccine would be available to them and only fear of COVID-19 appeared to have had a small to mild influence on their decision. Even more worrying is the fact that high vaccination hesitancy was observed among prospective healthcare workers as they represent the future gatekeepers and/or promotors of maladaptive behaviours by influencing the health-related decisions of many people. As the numbers are well below the percentages recommended by authorities to allow community (herd) immunity, the decision makers should support further explorations to determine the exact causes for high vaccination hesitancy among Slovenian postsecondary students and subsequent development of targeted interventions and campaigns against it. Moreover, it should specifically explore the reasons behind significantly different levels of vaccination hesitancy among medical students and healthcare students, as the present results might call for a review of the healthcare study programmes in order to ensure a better understanding of the vaccines among future healthcare workers. Not only would these interventions reduce the negative consequences of the potential future outbreaks of a health crisis like COVID-19, but also ensure that the postsecondary students will be the first in line to promote positive health behaviours.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Change history
06 January 2023
A Correction to this paper has been published: https://doi.org/10.1038/s41598-022-27000-5
References
Ammar, A. et al. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: Insights from the ECLB-COVID19 multicentre study. Biol. Sport 38, 9–21 (2021).
Poland, G. A. & Jacobson, R. M. Understanding those who do not understand: A brief review of the anti-vaccine movement. Vaccine 19, 2440–2445 (2001).
Dubé, E. et al. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 9, 1763–1773. https://doi.org/10.4161/hv.24657 (2013).
Loomba, S., de Figueiredo, A., Piatek, S. J., de Graaf, K. & Larson, H. J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 5, 337–348 (2021).
MacDonald, N. E. et al. Vaccine hesitancy: Definition, scope and determinants. Vaccine 33, 4161–4164 (2015).
Thomas, N. Vaccines Immun. https://doi.org/10.1016/j.cnur.2015.10.005 (2022).
Dror, A. A. et al. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 35, 775–779 (2020).
Nacionalni Inštitut Za Javno Zdravje. Spremljanje neželenih učinkov po cepljenju proti covid -19 v Sloveniji. (2022).
Eržen, I., Kamenšek, T., Fošnarič, M. & Žibert, J. Key challenges in modelling an epidemic-what have we learned from the COVID-19 epidemic so far. Zdravstveno Varstvo 59, 117–119 (2020).
Velikonja, N. K., Erjavec, K., Verdenik, I., Hussein, M. & Velikonja, V. G. Association between preventive behaviour and anxiety at the start of the COVID-19 pandemic in Slovenia. Zdravstveno Varstvo 60, 17–24 (2020).
Tatar, M., Shoorekchali, J. M., Faraji, M. R. & Wilson, F. A. International COVID-19 vaccine inequality amid the pandemic: Perpetuating a global crisis?. J. Glob. Health 11, 1–3 (2021).
Barello, S., Nania, T., Dellafiore, F., Graffigna, G. & Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 35, 781–783 (2020).
Bou Hamdan, M., Singh, S., Polavarapu, M., Jordan, T. R. & Melhem, N. M. COVID-19 vaccine hesitancy among university students in Lebanon. Epidemiol. Infect. https://doi.org/10.1017/S0950268821002314 (2021).
Jain, J. et al. COVID-19 vaccine hesitancy among medical students in India. Epidemiol. Infect. 149, 1–10 (2021).
Mustapha, T., Khubchandani, J. & Biswas, N. COVID-19 vaccination hesitancy in students and trainees of healthcare professions: A global assessment and call for action. Brain Behav. Immunity Health 16, 100289 (2021).
Riad, A. et al. Prevalence and drivers of COVID-19 vaccine hesitancy among Czech university students: National cross-sectional study. Vaccines 9, 1–25 (2021).
Kassim, M. A. M. et al. Relationship between fear of COVID-19, psychopathology and sociodemographic variables in Malaysian population. Int. J. Ment. Heal. Addict. 20, 1303–1310 (2022).
Kuru Alici, N. & Ozturk Copur, E. Anxiety and fear of COVID-19 among nursing students during the COVID-19 pandemic: A descriptive correlation study. Perspect. Psychiatr. Care 58, 141–148 (2022).
Bendau, A., Plag, J., Petzold, M. B. & Ströhle, A. COVID-19 vaccine hesitancy and related fears and anxiety. Int. Immunopharmacol. 97, 107724 (2021).
Lo Moro, G., Cugudda, E., Bert, F., Raco, I. & Siliquini, R. Vaccine hesitancy and fear of COVID-19 among Italian medical students: A cross-sectional study. J. Community Health 47, 475–483 (2022).
Nazlı, ŞB., Yığman, F., Sevindik, M. & Deniz Özturan, D. Psychological factors affecting COVID-19 vaccine hesitancy. Ir. J. Med. Sci. 191, 71–80 (2022).
Gabrovec, B., Selak, Š, Crnkovič, N., Cesar, K. & Šorgo, A. Perceived satisfaction with online study during COVID-19 lockdown correlates positively with resilience and negatively with anxiety, depression, and stress among slovenian postsecondary students. Int. J. Environ. Res. Public Health 19, 7024 (2022).
Gabrovec, B. et al. Compliance with preventive measures and COVID-19 vaccination intention among medical and other healthcare students. Int. J. Environ. Res. Public Health 19, 11656 (2022).
Ministrstvo za izobraževanje, znanost in šport. Študijsko leto 2020/2021 v številkah. https://www.gov.si/novice/2020-09-29-studijsko-leto-20202021-v-stevilkah/ (2020).
Ahorsu, D. K. et al. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 20, 1537–1545 (2020).
Soraci, P. et al. Validation and psychometric evaluation of the italian version of the fear of COVID-19 scale. Int. J. Ment. Health Addict. https://doi.org/10.1007/s11469-020-00277-1 (2020).
Perz, C. A., Lang, B. A. & Harrington, R. Validation of the fear of COVID-19 scale in a US college sample. Int. J. Ment. Health Addict. 20, 273–283 (2022).
Reznik, A., Gritsenko, V., Konstantinov, V., Khamenka, N. & Isralowitz, R. COVID-19 fear in Eastern Europe: Validation of the fear of COVID-19 Scale. Int. J. Ment. Health Addict. 19, 1903–1908. https://doi.org/10.1007/s11469-020-00283-3 (2021).
Spitzer, R. L., Kroenke, K., Williams, J. B. W. & Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 166, 1092–1097 (2006).
Ajzen, I. From intentions to actions: A theory of planned behavior. Action Control https://doi.org/10.1007/978-3-642-69746-3_2 (1985).
Aristovnik, A., Keržič, D., Ravšelj, D., Tomaževič, N. & Umek, L. Impacts of the COVID-19 pandemic on life of higher education students: A global perspective. Sustainability (Switzerland) 12, 1–34 (2020).
Swami, V. & Barron, D. Translation and validation of body image instruments: Challenges, good practice guidelines, and reporting recommendations for test adaptation. Body Image 31, 204–220 (2019).
Clark, L. A. & Watson, D. Constructing validity: Basic issues in objective scale development. Psychol. Assess. 7, 309–319 (1995).
Field, A. Discovering Statistics Using IBM SPSS Statistics (Sage Publications, 2013).
Bruno Petzold, M. et al. Development of the COVID-19-Anxiety Questionnaire and first psychometric testing. BJPsych Open https://doi.org/10.1192/bjo.2020.82 (2020).
Dilbaz, N., Noyan, O. C., Alpar, G. & Kazan, O. K. Development of the COVID-19 phobia scale: Validity and reliability study. J. Neurobehav. Sci. 7, 142 (2020).
Lovibond, P. F. & Lovibond, S. H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 33, 335–343 (1995).
Beck, A. T., Epstein, N., Brown, G. & Steer, R. A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 56, 893–897 (1988).
Peters, L. et al. Comparison of DASS-21, PHQ-8, and GAD-7 in a virtual behavioral health care setting. Heliyon 7, e06473 (2021).
Seo, J. G. & Park, S. P. Validation of the Generalized Anxiety Disorder-7 (GAD-7) and GAD-2 in patients with migraine. J. Headache Pain 16, 1–7 (2015).
Sy-CherngWoon, L. et al. Depression, anxiety, and the COVID-19 pandemic: Severity of symptoms and associated factors among university students after the end of the movement lockdown. PLoS ONE 16, e0252481 (2021).
Sazakli, E. et al. Prevalence and associated factors of anxiety and depression in students at a Greek university during COVID-19 lockdown. J. Public Health Res. 10, 2089 (2021).
Patwary, M. et al. Mental health status of university students and working professionals during the early stage of COVID-19 in Bangladesh. Int. J. Environ. Res. Public Health 19, 6834 (2022).
Kumar Dhar, B., Ayittey, F. K., Sarkar, S. M., Dhar, B. K. & Ayittey, F. K. Impact of COVID-19 on psychology among the university students. Glob. Chall. 4, 2000038 (2020).
Bai, W. et al. Attitudes toward COVID-19 vaccines in Chinese college students. Int. J. Biol. Sci. 17, 1469 (2021).
Gao, X., Li, H., He, W. & Zeng, W. COVID-19 vaccine hesitancy among medical students: The next COVID-19 challenge in Wuhan, China. Disaster Med. Public Health Prep. https://doi.org/10.1017/DMP.2021.291 (2021).
Mose, A., Haile, K. & Timerga, A. COVID-19 vaccine hesitancy among medical and health science students attending Wolkite University in Ethiopia. PLoS ONE 17, e0263081 (2022).
Willis, D. E. et al. COVID-19 vaccine hesitancy: Race/ethnicity, trust, and fear. Clin. Transl. Sci. 14, 2200–2207 (2021).
Acknowledgements
This publication arises from the “Measures in the Field of COVID-19 Spread Management with a Focus on Vulnerable Populations” project, funded by Slovenia and the European Social Fund, of the European Structural and Investment Funds, covered by Regulation (EU) No. 1303/2013 of the European Parliament and of the Council (the Common Provisions Regulation). The content of this paper represents the views of the authors only and is their sole responsibility; it cannot be considered to reflect the views of the European Commission or any other body of the European Union. The European Commission does not accept any responsibility for the use that may be made of the information it contains.
Funding
The study was conducted in Slovenia as part of a NIJZ project. The project title is “Measures to manage the spread of COVID-19 with a focus on vulnerable groups of population”. This research is co-financed by the Republic of Slovenia and the European Union under the European Social Fund in the framework of the EU response to the COVID-19 pandemic (Grant No. C2711-20-054101). The content of this article represents the views of the authors only and is their sole responsibility; it cannot be considered to reflect the views of the European Commission or any other body of the European Union. The European Commission does not accept any responsibility for the use that may be made of the information it contains.
Author information
Authors and Affiliations
Contributions
A.Š., B.G., N.C., M.V., K.C. and Š.S. conceived this study. All authors commented on the paper, B.G. and Š.S. oversaw the analysis, and N.C., M.V., K.C. edited the final manuscript. B.G. and Š.S. led the writing of the paper. Š.S., N.C. and K.C. cleaned, analysed, and verified the underlying data. All authors contributed to the study design. All authors contributed to drafting the paper and revised the manuscript for important intellectual content. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained an error in the Funding section. Full information regarding the corrections made can be found in the correction notice for this Article.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Šorgo, A., Crnkovič, N., Cesar, K. et al. The influence of anxiety and fear of COVID-19 on vaccination hesitancy among postsecondary students. Sci Rep 12, 20564 (2022). https://doi.org/10.1038/s41598-022-25221-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-25221-2
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
