
Abstract
Today, individual prognosis in patients with adenocarcinoma of the esophagus (EAC) is based on post-surgical TNM staging and valid biomarkers are still not implemented. Integrin beta1 (ITGB1) is widely expressed in epithelial cells and promotes cell adhesion and growth. Its impact on tumor progression was described for different tumor entities before, data on its function as a potential biomarker in EAC is not available. Aim of the study is to evaluate the expression level of ITGB1 in a large collective of EAC and its impact on patients´ prognosis. 640 patients with esophageal adenocarcinoma were analyzed immunohistochemically for ITGB1. The data was correlated with long term outcome, clinical, pathological and molecular data (TP53, HER2/neu, c-myc, GATA6, PIK3CA and KRAS). Of 640 patients to be analyzed, 127 (19.8%) showed expression of ITGB1. ITGB1 expression was associated with lymph node metastasis, expression of integrin alphaV and KRAS mutation status. Patients with high ITGB1 expression showed impaired overall survival (22.5 months (95% CI 15.3–29.7 months), vs. 34.1 months (95% CI 25.3–42.4 months), P = 0.024). This effect was particularly evident in the group of patients undergoing primary surgery without prior neoadjuvant therapy (10.2 months (95% CI 1.9–41.7 months) vs. 31.4 months (95% CI 21.1–144.2 months, P = 0.008). ITGB1 was also an independent prognostic marker in multivariable analysis (HR 1.696 (95% CI 1.084–2.653, P = 0.021) in patients that underwent primary surgery. We demonstrate for the first time the prognostic significance of ITGB1 expression in a large EAC patient population.
Similar content being viewed by others


Introduction
Esophageal cancer ranks seventh in terms of incidence and sixth in mortality worldwide1. A rising incidence of esophageal adenocarcinoma (EAC) is described in high-income western countries and is expected to rise even further2. Establishing multimodal treatment protocols shows promising results in the treatment of EAC. However, overall-survival of patients with EAC remains limited3,4 Excluding clinical parameters like age and histopathological grading there are barely any prognostic factors established for risk stratification in patients with EAC. To individualize the current treatment protocols the use of prognostic biomarkers should be implied to identify patients benefiting from multimodal therapy including chemotherapy, radiotherapy, surgery and immunotherapy5,6.
Integrins are heterodimeric transmembrane proteins which regulate cell–cell and cell-extracellular matrix (ECM) interactions7. There are 24 known Integrins which are structurally made from a combination of a beta and an alpha subunit8. Today 18 alpha and 8 beta integrin subunits are described. Integrins play a major part in organizing cytoskeleton, activating intracellular signal pathways thereby promoting cell survival as well as mediating cell responses to growth factors and cytokines8,9. Due to these functions it is that an increasing interest has risen in the role integrins play in malignant diseases. Several integrins have been found to be involved in tumorigenesis, tumor progression and in the metastatic cascade for different tumor entities. Our group was able to show the impact of integrin alpha V expression on patients’ prognosis in esophageal cancer10.
In the present study, we are focusing on Integrin beta1 (ITGB1), which has been described as tumor progressor in various tumor entities like lung cancer, colon cancer11 and prostate cancer12.
To date, there is no analysis of ITGB1 expression in esophageal adenocarcinoma. The aim of this study was to analyze the expression of ITGB1 in esophageal adenocarcinoma and possibly correlate the expression profile with clinico-pathological, molecular and survival data.
Patients and Methods
Patients and tumor samples
Formalin-fixed and paraffin embedded tumor tissue of 685 patients with esophageal adenocarcinomas that underwent primary surgical resection or resection after neoadjuvant therapy between 1999 and 2014 at the Department of General, Visceral and Cancer Surgery, University of Cologne, Germany was analyzed as previously described10,13,14. The standard surgical procedure consisted of a transthoracic en-bloc esophagectomy with two-field lymphadenectomy (abdominal and mediastinal lymph nodes), reconstruction by formation of a gastric tube with intrathoracic esophagogastrostomy (Ivor-Lewis esophagectomy)15. The abdominal phase was predominantly performed as a laparoscopic procedure (hybrid Ivor-Lewis esophagectomy). Technical details of this operation are described elsewhere16,17,18. Patients with locally advanced esophageal cancer (cT3) or evidence for loco regional lymph node metastasis in clinical staging received preoperative chemoradiation (5-Fluouracil, cisplatin, 40 Gy) or chemotherapy alone. Follow-up data were available for all patients (Table 1).
Single spot tissue micro arrays (TMA) were built for immunohistochemical analyses. TMA construction was performed as previously described19,20. In brief, tissue cylinders with a diameter of 1.2 mm each were punched from selected tumor tissue blocks using a self-constructed semi-automated precision instrument and embedded in empty recipient paraffin blocks. 4 μm sections of the resulting TMA blocks were transferred to an adhesive coated slide system (Instrumedics Inc., Hackensack, NJ) for immunohistochemistry. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The present study was ethically approved by the University of Cologne Ethics Committee (Reference No. 13-091) and written informed consent was obtained from all patients.
Immunohistochemistry for Integrin beta1 (ITGB1)
Immunohistochemistry (IHC) was performed on TMA slides using the Integrin beta1 rabbit monoclonal antibody (A-4; dilution 1:100; Santa Cruz, USA). Staining and scoring procedures were conducted as previously described20,21,22,23. All immunohistochemical stainings were performed using the Leica BOND-MAX stainer (Leica Biosystems, Germany) according to the protocol of the manufacturer.
The membraneous staining pattern was scored manually and independently by two pathologists (A.Q. and H.L.) according to a 4-tier-scoring system (Fig. 1). Score 3 + was defined as a strong staining of ≥ 30% of tumor cells or moderate staining ≥ 70%. A weak staining in > 70% or moderate staining in > 30 and ≤ 70%, or a strong staining in ≤ 30% of tumor cells was considered as Score 2 + . Score 1 + was assigned when ≤ 70% of tumor cells were weakly positive or ≤ 30% were moderately stained. Less staining was defined as negative (Score 0). Discrepant results were resolved by consensus review.

Immunohistochemistry staining for integrin beta1 (ITGB1). Negative tumor sample for ITGB1 (A), weak (B), moderate (C) and strong staining intensity (D).
Expression of ITGB1 was correlated with molecular markers including analysis of TP53, Her2/neu, c-myc, GATA6, PIK3CA mutations and KRAS amplification.
Statistical analysis
Clinical data were collected prospectively and analyzed according to a standardized protocol as previously described13,14,20. SPSS Statistics for Mac (Version 21, SPSS) was used for statistical analysis. Interdependence between staining results and clinical data were calculated using the chi-squared and Fisher’s exact tests, and displayed by cross-tables. Survival curves were plotted using the Kaplan–Meier method and analyzed using the log-rank test. All tests were two-sided. P values < 0.05 were considered statistically significant.
Results
Patients’ baseline characteristics
On the TMA a total of 640 patients of 685 (93.2%) were immunohistochemically interpretable for ITGB1. Reasons for the non-informative cases were missing tissue samples or the absence of distinct cancer tissue in the TMA spot. Patients were predominantly males (n = 564, 88.1%), females n = 76, 11.9%. The median age of the entire patient cohort at the time of diagnosis was 65.2 years (range 33.6–85.6 years). In 333 patients (56.0%) a neoadjuvant treatment (chemo- or radiochemotherapy) was performed before surgery.
Expression of ITGB1 in esophageal adenocarcinoma
Expression of ITGB1 was detected in 127 patients (19.9%) (Fig. 2). ITGB1 expression was associated with presence of lymph node metastasis (P = 0.039) and Integrin alpha V (ITGAV) expression (P < 0.001). A correlation of ITGB1 expression with molecular marker could only be seen for KRAS mutation status (P = 0.044) (Table 1).

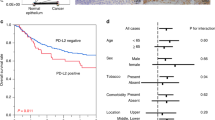
Kaplan–Meier survival analysis for overall survival of the entire patient cohort Kaplan–Meier survival analysis for overall survival of the entire patient cohort (A). Median OS in patients with presence of ITGB1 was 22.5 months (95% confidence interval (95% CI) 15.3–29.7 months), and 34.1 months (95% CI 25.3–42.4 months, P = 0.024) without ITGB1 expression. Median OS in patients after primary surgery (B) with ITGB1 expression in the tumor was 10.2 months (95% CI 1.9–41.7 months) compared to 31.4 months (95% CI 21.1–144.2 months, P = 0.008) in the group without ITGB1 expression. Patients that received neoadjuvant treatment before surgery (C) showed a median OS with ITGB1 expression of 22.7 months (95%CI 15.3–30.2 months) vs. 25.9 months without ITGB1 expression (95% CI 20.6–31.2 months), P = 0.423).
ITGB1 expression marks poor outcome in patients without neoadjuvant treatment
Patients with expression of ITGB1 (score 1 +, 2 +, 3 +) in the primary tumor showed an impaired overall survival compared to patients without ITGB1 expression (score 0). Median OS in patients with presence of ITGB1 was 22.5 months (95% confidence interval (95% CI) 15.3–29.7 months), median OS in patients without ITGB1 expression was 34.1 months (95% CI 25.3–42.4 months, P = 0.024). Stratification in patients with and without any kind of neoadjuvant treatment revealed that the survival difference is mainly driven by the group of patients that underwent primary surgery without neoadjuvant treatment. In this group, patients with ITGB1 expression in the tumor showed a median OS of 10.2 months (95% CI 1.9–41.7 months) compared to a median OS of 31.4 months (95% CI 21.1–144.2 months, P = 0.008) in the group without ITGB1 expression (Fig. 2).
In the patient cohort after neoadjuvant treatment, an ITGB1 associated survival difference could not be observed. The median overall survival did not differ significantly between the two groups (median OS in patients with ITGB1 expression 22.7 months (95% CI 15.3–30.2 months) vs. 25.9 months without ITGB1 expression (95% CI 20.6–31.2 months), P = 0.423).
A multivariate cox-regression model showed that ITGB1 is an independent prognostic factor in the group of patients without neoadjuvant treatment (hazard ratio (HR) 1.171 (95% CI 1.089–2.707), P = 0.020) but failed to serve as prognostic marker in the patients group after neoadjuvant treatment (HR 1.121 (95% CI 0.806–1.557), P = 0.498) (Tables 2 and 3).
Discussion
To date, the impact of ITGB1 on survival in esophageal adenocarcinoma has not been studied. In our analysis, we were able to examine 640 primary tumors regarding ITGB1 expression. Approximately 20% of the tumors were positive for ITGB1 and were associated with a significantly worse prognosis than ITGB1 negative tumors. This effect is stronger in the group of patients without neoadjuvant therapy than in the group of patients who received (radio) chemotherapy prior to esophagectomy.
The role of integrins in tumor progression has received more and more attention in recent years. In the past, integrins were primarily described as interaction partners of epithelial cells to the extracellular matrix, but recent data show a direct influence on tumor progression of different integrin subtypes in a variety of tumor entities7,8. In our preliminary work, we have already demonstrated that expression of integrin alpha V has an impact on overall survival of patients with adenocarcinoma of the esophagus10. In the present study, we focused on the most common beta subunit of integrines. Integrin beta 1 is the most physiologically abundant beta subunit and together with a variety of alpha subunits forms a multitude of heterodimer combinations. The physiologically mediated functions in humans are diverse: for example, ITGB1 forms a so-called RGD (Arg-Gly-Asp) receptor binding domain in the combination of alpha5 and alpha8. The combination alpha4/beta1 enables specific leukocyte binding as well as binding to laminin and various collagens24,25. The role of ITGB1 in tumor progression has been demonstrated for several tumor entities, including lung, prostate, breast, and colorectal cancer26.
The mechanisms described via which ITGB1 induces tumor progression are diverse. In the past, the focus was on the analysis of an altered extracellular matrix within the tumor and thus a modified signal transduction after bidding of ITGB1 expressing tumor cells to the ECM26.
In addition to the direct interaction of integrins with the ECM, the influence of TGFbeta signaling in dependence of integrin expression on the remodeling of tumor microenvironment could be shown27. In this context, TGF beta mediates remodeling of the ECM which mediates tumor progression. In addition to local effects of integrin expression on tumor cells, detection of ITGB1 in tumor exosomes was shown to provide a premetastatic niche for lung metastases in pancreatic cancer. The effect was demonstrated via gene upregulation of S100 in lung fibroblasts which subsequently promoted the formation of pulmonary metastases28.
In prostate cancer, interactions between the transmembrane molecule Trop-2 and beta1 integrins results in re-localization of integrin beta 1 at the leading edges and can promote prostate cancer cell migration on fibronectin12. Metastatic and migratory capabilities of prostate cancer cells are in part integrin beta 1 dependent and rely on the Trop-2 promotion29. Trop-2 has recently gained attention as a clinical study in patients with triple-negative breast cancer treated with the drug Savituzumab govitecan (SG), a combination of anti-Trop-2 antibody and SN-38 (active metabolite of Irinotecan) could show significant positive effects on progression free and overall survival30. In a phase I/II study for SG’s use in metastatic epithelial cancers, 19 esophageal cancer patients were included of which 10 (52.6%) showed stable disease for at least 3.4 months31. The link between ITGB1 and Trop-2 mediated tumor progression could be of interest for the future as ITGB1 expression may be a potential biomarker of response prediction for SG therapy. However, future research should study the role of Trop-2 and its interactions with integrin beta 1 in EAC.
There are no data concerning the effect of neoadjuvant therapy on protein expression of ITBG1 in esophageal cancer. In our data, we find more pronounced effects on overall survival in the group of patients who did not receive preoperative (radio)-chemotherapy. One hypothesis is that neoadjuvant therapy leads to a variety of epigenetic changes within the tumor and thus integrin mediated effects on natural tumor progression are no longer detectable. We could detect similar effects for a variety of biomarkers in our collective13,21,22,23. For example, we demonstrated this for integrin alphaV, dickkopf-2, VISTA, and other biomarkers where prognostic relevance was not present after administration of neoadjuvant therapy.
Findings in other studies had proposed that up-regulation of ITGB1 would contribute to cell survival after radiation exposure in various cancers, thus facilitating resistance32. Our collective includes solely patients with esophageal adenocarcinoma. A recent publication by Xie and colleagues revealed very similar results in esophageal squamous cell carcinoma (ESCC) in 278 patients33. Only 6 (2.1%) patients had received any form of pretreatment in their ESCC cohort. They report high expression of ITGB1 in 179 patients (64%), whereas ITGB1 positivity in our cohort of patients after primary surgery was 19.6%. Their findings regarding the effect on survival are in line with our findings, considering the pronounced effects in our primary surgery cohort, and the fact that their collective almost entirely consists of patients that underwent primary surgery. This finding is even more interesting, as genomic data reveals that esophageal squamous carcinoma and esophageal adenocarcinoma can likely be considered two different diseases34. In our collective, ITGB1 positivity was not associated with a difference in survival after neoadjuvant therapy. It could be hypothesized that neoadjuvant therapies’ positive anti-tumor effect levelled the survival disadvantage of the ITGB1 positive patients compared to the ITGB1 negative patients. The median OS between the ITGB1 positive group after neoadjuvant therapy was 22.7 months and the untreated ITGB1 positive group had a 10.2 month median OS. Considering that patients who receive neoadjuvant therapy presented with a more progressed clinical tumor stage to receive pre-treatment in the first place, the survival difference in these two groups is notable. Especially, as no correlation of ITGB1 with the UICC stage was observed.
In conclusion, our findings support integrin beta1 as a possible prognostic biomarker in esophageal adenocarcinoma. The negative effect on survival is particularly evident in the group of primary resected patients in our cohort. The extent to which individual patient prognosis can be predicted in pretherapeutic biopsies is currently under investigation and could potentially influence treatment decisions for and against neoadjuvant therapy in the future. Association of integrin beta expression with other targetable molecules such as Trop-2 should be the object of further studies in EAC.
Data availability
Data available on request to the corresponding author due to privacy/ethical restrictions.
References
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71(3), 209–249 (2021).
Arnold, M., Laversanne, M., Brown, L. M., Devesa, S. S. & Bray, F. Predicting the future burden of esophageal cancer by histological subtype: International trends in incidence up to 2030. Am. J. Gastroenterol. 112(8), 1247–1255 (2017).
van Hagen, P. et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N. Engl. J. Med. 366(22), 2074–2084 (2012).
Al-Batran, S. E. et al. Histopathological regression after neoadjuvant docetaxel, oxaliplatin, fluorouracil, and leucovorin versus epirubicin, cisplatin, and fluorouracil or capecitabine in patients with resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4-AIO): Results from the phase 2 part of a multicentre, open-label, randomised phase 2/3 trial. Lancet Oncol. 17(12), 1697–1708 (2016).
Kato, K. et al. KEYNOTE-590: Phase III study of first-line chemotherapy with or without pembrolizumab for advanced esophageal cancer. Future Oncol. 15(10), 1057–1066 (2019).
Janjigian, Y. Y. et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): A randomised, open-label, phase 3 trial. Lancet 398(10294), 27–40 (2021).
Desgrosellier, J. S. & Cheresh, D. A. Integrins in cancer: Biological implications and therapeutic opportunities. Nat. Rev. Cancer 10(1), 9–22 (2010).
Hamidi, H. & Ivaska, J. Every step of the way: Integrins in cancer progression and metastasis. Nat. Rev. Cancer 18(9), 533–548 (2018).
Guo, W. & Giancotti, F. G. Integrin signalling during tumour progression. Nat. Rev. Mol. Cell. Biol. 5(10), 816–826 (2004).
Loeser, H. et al. Integrin alpha V (ITGAV) expression in esophageal adenocarcinoma is associated with shortened overall-survival. Sci. Rep. 10(1), 18411 (2020).
Fujita, S., Watanabe, M., Kubota, T., Teramoto, T. & Kitajima, M. Alteration of expression in integrin beta 1-subunit correlates with invasion and metastasis in colorectal cancer. Cancer Lett. 91(1), 145–149 (1995).
Trerotola, M. et al. Trop-2 promotes prostate cancer metastasis by modulating beta(1) integrin functions. Cancer Res. 73(10), 3155–3167 (2013).
Schiffmann, L. M. et al. Elevated X-linked inhibitor of apoptosis protein (XIAP) expression uncovers detrimental prognosis in subgroups of neoadjuvant treated and T-cell rich esophageal adenocarcinoma. BMC Cancer 19(1), 531 (2019).
Plum, P. S. et al. HER2/neu (ERBB2) expression and gene amplification correlates with better survival in esophageal adenocarcinoma. BMC Cancer 19(1), 38 (2019).
Schroder, W. et al. Ivor-Lewis esophagectomy with and without laparoscopic conditioning of the gastric conduit. World J. Surg. 34(4), 738–743 (2010).
Holscher, A. H., Schneider, P. M., Gutschow, C. & Schroder, W. Laparoscopic ischemic conditioning of the stomach for esophageal replacement. Ann. Surg. 245(2), 241–246 (2007).
Messager, M. et al. Laparoscopic gastric mobilization reduces postoperative mortality after esophageal cancer surgery: A French nationwide study. Ann. Surg. 262(5), 817–822 (2015).
Mariette, C. et al. Hybrid minimally invasive esophagectomy for esophageal cancer. N. Engl. J. Med. 380(2), 152–162 (2019).
Simon, R., Mirlacher, M. & Sauter, G. Tissue microarrays. Methods Mol. Med. 114, 257–268 (2005).
Essakly, A. et al. PIK3CA and KRAS amplification in esophageal adenocarcinoma and their impact on the inflammatory tumor microenvironment and prognosis. Transl. Oncol. 13(2), 157–164 (2020).
Schiffmann, L. M. et al. Dickkopf-2 (DKK2) as context dependent factor in patients with esophageal adenocarcinoma. Cancers (Basel) 12(2), 451 (2020).
Schallenberg, S. et al. Loss of the SWI/SNF-ATPase subunit members SMARCF1 (ARID1A), SMARCA2 (BRM), SMARCA4 (BRG1) and SMARCB1 (INI1) in oesophageal adenocarcinoma. BMC Cancer 20(1), 12 (2020).
Loeser, H. et al. The expression of the immune checkpoint regulator VISTA correlates with improved overall survival in pT1/2 tumor stages in esophageal adenocarcinoma. Oncoimmunology 8(5), e1581546 (2019).
Jahangiri, A., Aghi, M. K. & Carbonell, W. S. beta1 integrin: Critical path to antiangiogenic therapy resistance and beyond. Cancer Res. 74(1), 3–7 (2014).
Al-Jamal, R. & Harrison, D. J. Beta1 integrin in tissue remodelling and repair: From phenomena to concepts. Pharmacol. Ther. 120(2), 81–101 (2008).
Kato, H. et al. The primacy of beta1 integrin activation in the metastatic cascade. PLoS ONE 7(10), e46576 (2012).
Schober, M. & Fuchs, E. Tumor-initiating stem cells of squamous cell carcinomas and their control by TGF-beta and integrin/focal adhesion kinase (FAK) signaling. Proc. Natl. Acad. Sci. U. S. A. 108(26), 10544–10549 (2011).
Hoshino, A. et al. Tumour exosome integrins determine organotropic metastasis. Nature 527(7578), 329–335 (2015).
Trerotola, M. et al. Trop-2 is up-regulated in invasive prostate cancer and displaces FAK from focal contacts. Oncotarget 6(16), 14318–14328 (2015).
Bardia, A. et al. Sacituzumab govitecan in metastatic triple-negative breast cancer. N. Engl. J. Med. 384(16), 1529–1541 (2021).
Bardia, A. et al. Sacituzumab govitecan, a Trop-2-directed antibody-drug conjugate, for patients with epithelial cancer: Final safety and efficacy results from the phase I/II IMMU-132-01 basket trial. Ann. Oncol. 32, 746–756. https://doi.org/10.1016/j.annonc.2021.03.005 (2021).
Nam, J. M., Chung, Y., Hsu, H. C. & Park, C. C. Beta1 integrin targeting to enhance radiation therapy. Int. J. Radiat. Biol. 85(11), 923–928 (2009).
Xie, Y.-H. et al. Role of integrin beta1 in the progression and chemoresistance of of esophageal squamous cell carcinoma. J. Cancer 13, 2074–2085. https://doi.org/10.7150/jca.68647 (2022).
Salem, M. E. et al. Comparative molecular analyses of esophageal squamous cell carcinoma, esophageal adenocarcinoma, and gastric adenocarcinoma. Oncologist 23, 1319–1327. https://doi.org/10.1634/theoncologist.2018-0143 (2018).
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
A.D., I.W., F.G. wrote the main manuscript, conceptualized the project and performed the formal analysis, as well as prepared the tables. H.L, A.Q. prepared the figures, performed the TMA analysis and contributed to the methodology. H.F., S.C., C.B., T.Z., W.S. reviewed and edited the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Damanakis, A.I., Wahler, I., Fuchs, H. et al. Integrin beta1 (ITGB1) as a prognostic marker in esophageal adenocarcinoma. Sci Rep 12, 20745 (2022). https://doi.org/10.1038/s41598-022-25071-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-25071-y
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
