
Abstract
Biochemical recurrence (BCR) of prostate cancer (PCa) occurs in about 25% of patients treated with radical prostatectomy (RP) and up to 45% in patients who receive external beam radiotherapy (RT). Early diagnosis of PCa recurrence is of high importance for successful salvage therapy. The aim of the present study is to analyze the efficacy of 68 Ga-PSMA PET/CT in detecting the presence of local and/or systemic disease in patients with a history of PCa who have BCR. A total of 52 PCa patients with BCR referred for 68 Ga-PSMA PET/CT were recruited from the American University of Beirut Medical Center between November 2017 and December 2019. We compared the performance of PSMA PET/CT to the results and clinical factors based on follow up: PSA, PSA kinetics, primary treatment, and Gleason score. The relationship between the PET/CT findings and clinical indicators of disease were assessed by univariate and multivariate logistic regression. From a total of 52 patients, 34 (65.4%) had positive PSMA-PET/CT scans. Among those, 8/34 (23.5%) received primary RT. For all patients with a positive PSMA-PET: the detection rate was 2/4 (50%) for PSA < 0.2, 5/10 (50%) for PSA 0.2–0.49, 3/6 (50%) for PSA 0.5–0.99, 6/12 (50%) for PSA 1–1.99, 8/9 (88.9%) for PSA 2–3.99, and 10/11 (90.9%) for PSA 4–10.
PSMA-PET/CT positivity was significantly associated with PSA level at time of PET scan, PSA doubling time, Gleason score and TNM staging. However, it did not show a significant correlation with radiotherapy as primary treatment, ongoing androgen deprivation therapy (ADT), time to relapse, and initial PSA before therapy. In our single center prospective trial, 68 Ga-PSMA PET/CT successfully detected the recurrence of PCa in patients with BCR. Scan positivity was significantly associated with PSA level at time of PET scan, PSA doubling time, Gleason score, and TNM staging. PSMA- PET/CT is a highly promising modality in the work up of patients with PCa in the setting of BCR for earlier detection of disease recurrence.
Similar content being viewed by others

Introduction
Prostate cancer (PCa) is the most common solid malignancy in men and the third leading cause of cancer-related death in western Europe and the United States1,2. Prostate Specific Antigen (PSA) is a widely used test for PCa screening. Biochemical Recurrence (BCR) is common across all modes of intervention, with a 10-year cumulative incidence of approximately 24% in patients who underwent radical prostatectomy (RP) and 43% in patients who received external beam radiotherapy3. In accordance with the nomograms, local recurrence in prostate bed after RP can be predicted with an accuracy of about 80% in patients with a BCR more than 3 years after RP, a PSA doubling time (PSAdt) > 11 months, Gleason Score (GS) < 7 and a pT3aN0 and pTxN1. In contrast, systemic recurrence can be predicted with an accuracy of about 80% in patients with a BCR distance of less than 1 year after RP, PSAdt of about 4–6 months, GS > 7 and stage of pT3b and pTxN14,5. Despite a good sensitivity in distinguishing between local and distant recurrence, the nomograms do not provide information about either the real site of recurrence (lymph node vs. bone; pelvic vs. extra-pelvic) or the actual number of metastatic lesions. Moreover, most patients have features that can be compatible, in agreement with the nomograms, with both local and systemic recurrence. As such, targeted rescue therapies cannot be organized taking into consideration the possibility of risk supplied by only nomograms. Patients are therefore generally directed to a salvage radiotherapy (S-RT) of the prostate bed (suspicion of local recurrence) or to a systemic treatment with Androgen Deprivation Therapy (ADT) in case of suspicion of systemic recurrence. ADT + RT combination has also been used as standard treatment of BCR for locally advanced high-risk PCa6,7.
Conventional imaging methods, including computed tomography (CT), bone scintigraphy (BS) and magnetic resonance (MR), showed low accuracy values for restaging patients with BCR. During the last decade, nuclear medicine techniques such as positron emission tomography (PET), with 11C-choline and 18F-choline, were found to be more accurate than conventional diagnostic modalities for restaging patients with PCa showing BCR8, allowing the differentiation between a local recurrence confined to the pelvis from a systemic recurrence9. However, PET/CT with choline showed a suboptimal sensitivity when performed in patients with early BCR, i.e. patients with low serum PSA (< 0.2 ng/mL) after radical therapy9.
The optimal timing to implement rescue treatments (such as S-RT) for the best prognosis is when the extension of the disease is low, which is when serum PSA levels are first detectable after radical therapy10. In this context, there is a necessity for a diagnostic test potentially able to differentiate between initial or loco-regional from a systemic recurrence only manageable with palliative approaches.
One molecule used to target PCa is Prostate Specific Membrane Antigen (PSMA)11. PSMA is a membrane enzyme that is markedly expressed in PCa cells when compared with healthy prostate tissue12. The bond at the catalytic site of PSMA in its extracellular domain allows for the development of small-specific inhibitors that are internalized after ligand binding13. The use of 68 Ga-PSMA (Glu-NH-CO–NH-Lys- (Ahx)—[68 Ga (HBED-CC as a radiopharmaceutical for PET/CT imaging has proven to be more accurate in the diagnosis of early disease recurrence when compared to 18F-choline PET/CT14,15. These studies have also demonstrated a better tumor to background ratio (TBR) with 68 Ga-PSMA PET/CT compared to 18F-choline PET/CT in identifying suspicious lesions for relapse13. Further studies conducted on larger patient populations with BCR after radical therapy have shown an excellent diagnostic ability of 68 Ga-PSMA PET/CT in restaging patients with BCR, even when serum PSA values were very low16,17,18.
In recent months, the use of this tracer has been a subject of growing interest in the scientific community16,17,18,19,20,21. This radiopharmaceutical had also shown high specificity (> 90%) in studies using histological analysis as a reference standard for validation of PET results16,19,21. Finally, none of the studies in the literature had reported adverse events or clinically detectable pharmacological effects occurring concurrently or after executing the PET/CT 68 Ga-PSMA. For the reasons explained above, PSMA can be an excellent molecular target for the development of radiotracers for PET/CT imaging that can detect early disease relapse.
Objectives
The primary aim of this study was to evaluate the detection rate, accuracy, and positivity rate of 68 Ga-PSMA PET/CT in detecting the presence of local and/ or systemic disease in patients with treated PCa and evidence of BCR. In addition, we aim to compare the performance of PSMA PET/CT to the results and clinical factors (GS, PSA levels, PSA kinetics, TNM staging) used in the normal care pathway.
Materials and methods
Study design
This study was done prospectively in patients with PCa at the American University of Beirut Medical Center, Lebanon. All patients had detectable serum PSA post primary therapy of PCa with either RP or RT. Fifty-two patients have been recruited into this study based on well-defined inclusion and exclusion criteria (Table 1).
All patients that were undergoing drug-use cures in the normal care pathway were evaluated. Eligible patients who participated in the study signed the informed consent before undergoing the 68 Ga-PSMA PET/CT scans.
Based on the European Association of Urology guidelines, patients were assigned to either local and/or systemic therapy4. Patients were then followed longitudinally with collection of clinical and biochemical data in 3-month intervals during the first year (T5-T6-T7-T8) and six months during the second year of follow-up (T9-T10). The duration of the enrollment of samples was twenty-four months. The duration of follow-up and clinical data collection for each individual patient was twenty-four months. This study was approved by the Institutional Review Board of American University of Beirut, and we confirm that all research was performed in accordance with relevant guidelines/regulations.
68 Ga-PSMA PET/CT imaging
Since this is a non-randomized study, all patients had a PET/CT scan with 68 Ga-PSMA. The radiopharmaceutical study of the tracer 68 Ga-PSMA are synthesized at the radiology pharmaceutical laboratory of AUBMC. The PET/CT scans were conducted with the following technical standards:
Good Manufacturing Practice (GMP) certified 68 Ga Radiolabelling Kit by Isotope Technologies Garching (Munich, Germany) and single-use sterile cassette by ABX Advanced Biochemical Compounds (ABX) (Radeberg, Germany) were labeled to 10 mg PSMA-11. Each patient received 65 to 178 megabecquerel (MBq) (mean 113.3 ± 21.2 MBq) (1.76–4.81 millicurie [mCi]; mean 3.06 ± 0.57 mCi) of 68 Ga-PSMA 11 intravenously. Sixty minutes post-injection of the radiotracer, whole-body images were acquired in supine position using a Philips Gemini TF 16 PET/CT scanner. Adverse reactions to the radiotracer were not experienced in any patient.
Two board-certified specialists with 23 years of experience in nuclear medicine and 7 years of experience in reporting 68 Ga PSMA PET/CT scans, reviewed all scans. The viewing and the processing of the images were made using a semi- quantitative workstation.
Images were interpreted with the dedicated commercially available software IntelliSpace Portal 8.0 by Philips Healthcare, which were displayed simultaneously as PET, CT, and PET/CT fusion series in axial cuts, sagittal and coronal, and 3D MIP (maximum intensity projection) reconstructions. Semi-quantitative SUVmax were measured in the lesions with higher uptake in the prostate bed, nodal, and extra-nodal metastasis.
All suspicious lesions with tracer uptake above the surrounding background activity and not conforming to benign or known pitfalls of 68 Ga-PSMA PET/CT findings were considered as sites of disease recurrence. Indeterminate PSMA findings were analyzed in light of clinical follow up, including PSA, imaging and response to therapy. The gold standard was PSA, imaging, and response to therapy.
Statistical analysis
The demographic and clinical variables were arranged using descriptive analysis. The comparison between patients with positive and negative PSMA PET/CT results was performed using the t-test. The relationship between the PET/CT results and clinical indicators of disease status were assessed by univariate and multivariate logistic regression methods. The data was analyzed using statistical package SPSS version 21 for Windows.
Consent to participate
Took approval from Institutional Review Board (IRB) of American University of Beirut. irb@aub.edu.lb.
Results
Patients’ characteristics
A total of 52 PCa patients with BCR referred for PSMA PET/CT between November 2017 and December 2019 were enrolled: 42 (80.8%) patients were treated initially with RP while 10 (19.2%) were managed with RT. The median time from PCa diagnosis to BCR was 41 months. At the time of PET/CT, 21 (40.3%) patients were ongoing ADT and 26 (50%) presented with a PSAdt ≤ 10 months. Table 2 shows the patients’ characteristics based on PSMA PET/CT results.
The median age of the patients was 71.3 years: 41 (78.8%) men fulfilled eligibility based on having PSA < 4 ng/mL while 11 (21.2%) presented PSA concentration between 4 and 10 ng/mL with negative conventional imaging.
68 Ga-PSMA PET/CT imaging
At least one malignant focus was found in 34/52 patients (65.4%) (Fig. 1), while 18 (34.6%) patients had a negative PSMA-PET/CT scan with no detectable disease (Fig. 2). We found a significant correlation between lesion identification and PSA mean at the time of imaging (p = 0.006). The detection rate was 2/4 (50%) for PSA < 0.2, 5/10 (50%) for PSA 0.2–0.49, 3/6 (50%) for PSA 0.5–0.99, 6/12 (50%) for PSA 1–1.99, 8/9 (88.9%) for PSA 2–3.99, and 10/11 (90.9%) for PSA 4–10. However, there was no statistically significant correlation between the imaging positivity and different PSA values at time of PSMA/PET (p = 0.09).

A 71-year-old patient on ADT and status post EBRT 60 Gray in 20 fractions. PSA at time of acquisition = 9.5 ng/mL. Axial CT (a) image of the prostate bed is shown. Fused PET/CT (b) shows focus of increased radiotracer uptake in the right peripheral zone of the prostate gland at mid-gland (black arrow) in keeping with disease recurrence. PET image is shown (c). Sagittal fused PET/CT (d) shows the described lesion (black arrow).

A 80-year-old patient status post radical prostatectomy. PSA level at time of acquisition: 1.38 ng/mL. Whole body 68 Ga-PSMAPET/CT was performed: axial cuts of PET (a), fused PET/CT (b, c), and CT images (d) showing no evidence of radiotracer avid disease in the whole body notably in the prostate bed.
PSMA-PET/CT scans were positive in 32/45 patients (71.11%) whose PSAdt was ≤ 10 months versus 2/7 (28.6%) patients whose PSAdt was above 10 months.
PSA imaging results were significantly associated with PSAdt means (p = 0.006). However, it was not significantly associated with PSAdt when comparing ≤ 10 months to > 10 months (p = 0.08).
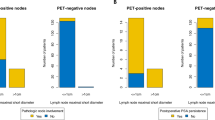
Moreover, PSMA PET/CT was significantly associated with TNM stage (p = 0.03) (Fig. 3).

A 68-year-old patient status post radical prostatectomy. PSA level at time of acquisition: 9 ng/mL. Whole body 68 Ga-PSMAPET/CT was performed. Maximal intensity projection image (a) showing metastatic disease. Axial CT (b) showing disease in the right common iliac lymph node (red arrow). PET/CT (c) showing focal areas of radiotracer uptake in the apical region of the prostatic bed associated with pre-sacral radiotracer avid lymph node as well as multiple radiotracer avid bone lesions. PET image (d) shows focal uptake at the right common iliac node (black arrow). Axial thoracic CT (e) fused with PET (f) shows focal uptake in the left scapula. PET image (g) demonstrates this lesion.
To note, GS was not reported in two out of 34 patients with positive PSMA PET/CT scans, as these patients performed their biopsies in other hospitals. Statistical analysis of 32 patients with positive imaging findings showed a significant correlation between PSMA PET/CT scan positivity and GS (p = 0.02). Furthermore, the detection rate was 1/3 (33.33%) in patients with GS 6, 17/29 (58.6%) in GS 7, 8/10 (80%) in GS 8 and 6/6 (100%) in GS 9. However, there was no statistically significant correlation between the positivity of the PSMA PET/CT scans and the different categories of GS (p = 0.09) (Table 3).
In Table 4, multivariate logistic regression showed that GS was significantly associated with positive PSMA-PET/CT scans (OR: 5.94; 95% CI 1.25–28.38; p = 0.03).
Similarly, PSA values at the time of PSMA-PET/CT scans was also positively associated with imaging positivity (OR2.54; 95% CI 1.15–5.63; p = 0.02).
There was no significant association between PSMA PET/CT status and time to relapse (p = 0.21), ADT treatment (p = 0.08), or primary therapy (p = 0.46).
Discussion
In our study, the positivity rate of PSMA PET/CT with at least one malignant focus was 65.4%, with similar rates ranging between 60–75% in other studies22,23,24,25. High PSA levels at the time of the PET/CT examinations were associated with higher PSMA PET/CT positivity, where a mean difference in PSA between positive and negative PSMA PET was found to be 4.5 ng/mL in one meta-analysis26. This is most likely due to the higher burden of disease with higher PSA levels2.
When it comes to positivity rates stratified by PSA levels, our study revealed equal or slightly higher overall PSMA PET/CT positivity per group when compared to the known literature: (PSA < 0.2: 50% vs 36.8%, PSA 0.2–0.49: 50% vs 43.3%, PSA 1–1.99: 50% vs 58.9%)27.
Features of aggressive or advanced disease were correlated with higher positivity rates, including shorter PSAdt (p = 0.006) and higher GS (p = 0.02). These findings were in concordance with the current literature, with PSAdt found to be an independent predictor of bone metastases and high GS associated with pelvic lymph node metastases27,28. This was predictable because shorter PSAdt and higher GS correlate with greater tumor extent and higher tumoral cells turnover, providing more sites for PSMA ligand binding.
The findings obtained from the logistic regression showed that the positivity of the PSMA-PET scans was associated with four main factors: PSA at the time of the PET/CT examination, PSAdt, GS, and TNM stage29,30. These findings were in concordance with the available literature on the value of PSMA PET/CT in evaluating patients with PCa with BCR22,23,31,32,33,34.
In our study, no significant association was detected between PSMA PET positivity and time to relapse. Previous literature has shown higher positivity of PSMA PET in shorter time to relapse when the time period was less than 29.5 months35. This may be explained by the relatively shorter follow up time in this prospective study (24 months), compared to the longer times in the abovementioned retrospective cohort35.
The use of ADT was not found to be associated with PSMA PET positivity, while some previous literature has shown a significant increase in the rates of positive PSMA PET in patients undergoing ADT36. In this study, 17/21 (80.9%) of patients who were on ADT had a positive PSMA PET/CT, while only 17/31 (54.8%) of patients who did not receive ADT had a positive PSMA PET/CT. No significance was detected (p = 0.08), which may be explained by our sample size.
This study showed no significant association between PSMA PET positivity and primary therapy in the setting of BCR (p = 0.46), such that 8/10 (80%) of patients who were on RT had a positive PSMA PET/CT, while only 26/42 (61.9%) of patients who underwent RP had a positive PSMA PET/CT. This is most likely due to the higher number of patients who received RP relative to RT in this cohort.
Limitations
Three limitations were encountered in this study, the first being the use of histopathologic confirmation as a gold standard. This method of confirmation was not always feasible from an ethical and a practical point of view. Consequently, the constellation of known standard references were used, such as clinical and laboratory values, and drop in PSA levels after therapy. This is also the reason why the negative predictive value of 68GA PSMA PET/CT was not assessed.
The second major limitation encountered was the monocentric approach of the study, which is the cause of the relatively small sample size, bearing in mind that AUBMC is one of the biggest institutions and reference centers in the Middle East. The third limitation burdening this study is the inclusion of 4 patients with a PSA < 0.2 ng/mL. These patients were included due to the proximity of their PSA levels (0.18, 0.19 ng/mL) to the lower limit for inclusion, while also keeping note of the small sample size at our single center study. Nonetheless, this small study design was a minor step in confirming the capability of PSMA PET/CT in detection of local and metastatic recurrence in patients with BCR. Overall survival was not calculated due to the short follow up time (24 months) and the generally protracted course of disease in PCa, with all 52 patients surviving beyond the 24-month mark in this study. Larger multicenter studies with longer follow-up periods are needed for better investigation of subsequent changes in management.
Conclusion
This single center prospective study on PSMA-PET/CT confirmed its ability and strength in detection of PCa recurrence in the setting of BCR. Our study with a limited number of patients showed promising results. The positivity of PSMA-PET/CT imaging was significantly associated with PSA at PET imaging time, PSAdt, GS, and TNM staging. PSMA- PET/CT is a highly promising modality in the work up of patients with PCa in the setting of BCR for earlier detection of disease recurrence.
Data availability
The datasets generated during and analysed during the current study are available from the corresponding author Dr. Mohamad Haidar on request.
References
Bray, F. et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer J. Clin. 68, 394–424 (2018).
NCCN Guidelines Prostate Cancer V.1.2022. (2022).
Suárez, J. F. et al. Mortality and biochemical recurrence after surgery, brachytherapy, or external radiotherapy for localized prostate cancer: A 10-year follow-up cohort study. Sci. Rep. 12, 12589. https://doi.org/10.1038/s41598-022-16395-w (2022).
Heidenreich, A. et al. EAU guidelines on prostate cancer. part ii: treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur. Urol. 65, 467–479 (2014).
Stephenson, A. J. et al. Postoperative nomogram predicting the 10-year probability of prostate cancer recurrence after radical prostatectomy. J. Clin. Oncol. 23, 7005–7012 (2005).
Yoo, S. et al. Combination of androgen deprivation therapy and salvage radiotherapy versus salvage radiotherapy alone for recurrent prostate cancer after radical prostatectomy. Urol. Int. 99, 406–413 (2017).
Pilepich, M. V. et al. Phase III radiation therapy oncology group (RTOG) trial 86–10 of androgen deprivation adjuvant to definitive radiotherapy in locally advanced carcinoma of the prostate. Int. J. Radiat. Oncol. Biol. Phys. 50, 1243–1252 (2001).
Choueiri, T. K., Dreicer, R., Paciorek, A., Carroll, P. R. & Konety, B. A Model That predicts the probability of positive imaging in prostate cancer cases with biochemical failure after initial definitive local therapy. J. Urol. 179, 906–910 (2008).
Castellucci, P. et al. Early biochemical relapse after radical prostatectomy: Which prostate cancer patients may benefit from a restaging 11 C-Choline PET/CT scan before salvage radiation therapy?. J. Nucl. Med. 55, 1424–1429 (2014).
Ceci, F. et al. Impact of 11C-choline PET/CT on clinical decision making in recurrent prostate cancer: results from a retrospective two-centre trial. Eur. J. Nucl. Med. Mol. Imaging 41, 2222–2231 (2014).
Hupe, M. C. et al. Expression of prostate-specific membrane antigen (PSMA) on biopsies is an independent risk stratifier of prostate cancer patients at time of initial diagnosis. Front. Oncol. 8, (2018).
Kinoshita, Y. et al. Expression of prostate-specific membrane antigen in normal and malignant human tissues. World J. Surg. 30, 628–636 (2006).
Ghosh, A. & Heston, W. D. W. Tumor target prostate specific membrane antigen (PSMA) and its regulation in prostate cancer. J. Cell. Biochem. 91, 528–539 (2004).
Afshar-Oromieh, A. et al. Comparison of PET imaging with a 68Ga-labelled PSMA ligand and 18F-choline-based PET/CT for the diagnosis of recurrent prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 41, 11–20 (2014).
Morigi, J. J. et al. Prospective comparison of 18 F-fluoromethylcholine versus 68 Ga-PSMA PET/CT in prostate cancer patients who have rising PSA after curative treatment and are being considered for targeted therapy. J. Nucl. Med. 56, 1185–1190 (2015).
Afshar-Oromieh, A. et al. The diagnostic value of PET/CT imaging with the 68Ga-labelled PSMA ligand HBED-CC in the diagnosis of recurrent prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 42, 197–209 (2015).
Eiber, M. et al. Evaluation of hybrid 68 Ga-PSMA ligand PET/CT in 248 patients with biochemical recurrence after radical prostatectomy. J. Nucl. Med. 56, 668–674 (2015).
Ceci, F. et al. 68Ga-PSMA PET/CT for restaging recurrent prostate cancer: Which factors are associated with PET/CT detection rate?. Eur. J. Nucl. Med. Mol. Imaging 42, 1284–1294 (2015).
Sterzing, F. et al. 68Ga-PSMA-11 PET/CT: A new technique with high potential for the radiotherapeutic management of prostate cancer patients. Eur. J. Nucl. Med. Mol. Imaging 43, 34–41 (2016).
Budäus, L. et al. Initial experience of 68Ga-PSMA PET/CT imaging in high-risk prostate cancer patients prior to radical prostatectomy. Eur. Urol. 69, 393–396 (2016).
Hijazi, S. et al. Pelvic lymph node dissection for nodal oligometastatic prostate cancer detected by 68 Ga-PSMA-positron emission tomography/computerized tomography. Prostate 75, 1934–1940 (2015).
Hope, T. A. et al. Impact of 68 Ga-PSMA-11 PET on management in patients with biochemically recurrent prostate cancer. J. Nucl. Med. 58, 1956–1961 (2017).
Fendler, W. P. et al. Assessment of 68 Ga-PSMA-11 PET accuracy in localizing recurrent prostate cancer. JAMA Oncol. 5, 856 (2019).
Mattiolli, A. B. et al. Impact of 68GA-PSMA PET / CT on treatment of patients with recurrent / metastatic high risk prostate cancer - a multicenter study. Int. Braz J Urol 44, 892–899 (2018).
Tan, N. et al. Imaging of prostate specific membrane antigen targeted radiotracers for the detection of prostate cancer biochemical recurrence after definitive therapy: A systematic review and meta-analysis. J. Urol. 202, 231–240 (2019).
Treglia, G. et al. Detection Rate of 18F-Labeled PSMA PET/CT in Biochemical Recurrent Prostate Cancer: A Systematic Review and a Meta-Analysis. Cancers (Basel) 11, 710 (2019).
Morris, M. J. et al. Diagnostic performance of 18F-DCFPyL-PET/CT in men with biochemically recurrent prostate cancer: Results from the CONDOR phase III Multicenter Study. Clin. Cancer Res. 27, 3674–3682 (2021).
Verburg, F. A. et al. Extent of disease in recurrent prostate cancer determined by [68Ga]PSMA-HBED-CC PET/CT in relation to PSA levels, PSA doubling time and Gleason score. Eur. J. Nucl. Med. Mol. Imaging 43, 397–403 (2016).
Perera, M. et al. Sensitivity, specificity, and predictors of positive 68 Ga–prostate-specific membrane antigen positron emission tomography in advanced prostate cancer: A systematic review and meta-analysis. Eur. Urol. 70, 926–937 (2016).
Jadvar, H. et al. Appropriate use criteria for prostate-specific membrane antigen PET imaging. J. Nucl. Med. 63, 59–68 (2022).
Gupta, S. K. et al. Prostate-Specific Membrane Antigen Positron Emission Tomography–Computed Tomography for Prostate Cancer: Distribution of Disease and Implications for Radiation Therapy Planning. Int. J. Radiat. Oncol.*Biol,*Phys. 99, 701–709 (2017).
Dietlein, F. et al. PSA-stratified performance of 18 F- and 68 Ga-PSMA PET in patients with biochemical recurrence of prostate cancer. J. Nucl. Med. 58, 947–952 (2017).
Sachpekidis, C. et al. 68Ga-PSMA-11 dynamic PET/CT imaging in biochemical relapse of prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 43, 1288–1299 (2016).
Schmuck, S. et al. Comparison of standard and delayed imaging to improve the detection rate of [68Ga]PSMA I&T PET/CT in patients with biochemical recurrence or prostate-specific antigen persistence after primary therapy for prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 44, 960–968 (2017).
Francolini, G. et al. Detection rate, pattern of relapse and influence on therapeutic decision of PSMA PET/CT in patients affected by biochemical recurrence after radical prostatectomy, a retrospective case series. Clin. Transl. Oncol. 23, 364–371 (2021).
Cerci, J. et al. Diagnostic performance and clinical impact of 68Ga-PSMA-11 PET/CT imaging in early relapsed prostate cancer after radical therapy: A prospective multicenter study (IAEA-PSMA Study). J. Nucl. Med. 63, 240–247 (2022).
Funding
Partially funded by the IAEA.
Author information
Authors and Affiliations
Contributions
M.H. H.M and A.A.G conceived and designed the analysis; M.E., S.A and A.R.A collected the data; S.A and H.T did the analysis tool; A.E., M.O., A.S and E.E.L. performed the analysis; M.K. substantially revised the abstract, introduction, methods, results, and discussion; All of the authors contributed in writing the paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Haidar, M., Abi-Ghanem, A.S., Moukaddam, H. et al. 68Ga-PSMA PET/CT in early relapsed prostate cancer patients after radical therapy. Sci Rep 12, 20500 (2022). https://doi.org/10.1038/s41598-022-24688-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-24688-3
This article is cited by
-
Whole-body tumour burden on [18F]DCFPyL PET/CT in biochemical recurrence of prostate cancer: association with tumour biology and PSA kinetics
European Journal of Nuclear Medicine and Molecular Imaging (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
