
Abstract
This study sought to evaluate the roles of and interactions between cognitive processes that have been shown to exhibit impact from socioeconomic status (SES) and living conditions in predicting social adaptation (SA) in a population of adults living in socially vulnerable conditions. Participants included 226 people between the ages of 18 and 60 who have been living in vulnerable contexts throughout life in Santiago, Chile. Data was collected through a battery of psychological assessments. A structural equation model (SEM) was implemented to examine the interrelationships among cognitive and social variables. Results indicate a significant relationship between executive function (EF) and SA through both social cognition (SC) and intelligence. Theory of Mind (ToM), a component of SC, was shown to exhibit a significant relationship with affective empathy; interestingly, this was negatively related to SA. Moreover, fluid intelligence (FI) was found to exhibit a positive, indirect relationship with SA through crystallized intelligence (CI). Evaluation of these results in the context of research on the impacts of SES and vulnerable living conditions on psychological function may allow for the development of more effective clinical, political, and social interventions to support psychosocial health among socially vulnerable populations.
Similar content being viewed by others


Introduction
Social adaptation (SA) encompasses an ability to interact with others in a manner that aligns with sociocultural norms1. Socially vulnerable populations represent individuals living in contexts with reduced access to economic resources due to their low-income range. This population lives in social risk neighborhoods and lacks the social resources necessary to withstand the impacts of external stressors2,3,4,5; this thwarts SA. The number and magnitude of stressors experienced by these persons combined with their insufficient access to resources to manage stress create conditions for poor mental health and chronic stress6,7. Furthermore, living in vulnerable conditions, particularly as a child, may be a driver for a reduction in the performance of functions or processes associated with the prefrontal cortex—that have been independently associated with SA—such as social cognition (SC) (includes decision-making, emotional processing, Theory of Mind (ToM), and empathy), fluid intelligence (FI), crystallized intelligence (CI), and executive functions (EF)7,8,9,10,11,12. Given the behavioral control exerted by these cognitive functions, it has been suggested that adolescents living in poverty who exhibit deficits in these functions may partake in resultant maladaptive behaviors that thwart SA13,14,15,16,17,18,19,20. The dynamics, precedents, and interactions of these cognitive functions in the context of SA and social vulnerability, however, are not yet fully understood. By elucidating the ways in which these cognitive constructs work together and separately in predicting social outcomes, we might better understand the role of specific variables in predicting SA. This information may allow for the design of more effective intervention programs to support psychosocial health among vulnerable populations.
Existing studies have investigated EF in relation to ToM (a component of SC) and FI against the context of SA to build models that more accurately reflect the synergies and determinants of these processes. In addition to the role of EF impairments in yielding maladaptive behavior15,16,18,19,20, these impairments are also related to reduced functioning in ToM21,22. In the sample investigated by Colvert et al.21, subjects exhibiting cognitive dysfunction related to EF and ToM were significantly more likely to have been subjected to deprived environmental conditions earlier in life21. This provides further indication of the role of socioeconomic status (SES) and early living conditions in determining cognitive capacities that affect SA.
Similar to EF, intelligence develops in childhood and exhibits environmental effects related to SES and early living conditions23,24. Poverty in childhood is associated with reduced literacy levels that exhibit a negative impact on FI11. Additionally, concerns related to poverty consume mental resources, leaving fewer to allocate toward other tasks17. Brydges et al.25 found a single factor model of EF—whose capacity seems to be similarly influenced by SES—that robustly predicted FI and CI capacity25. Though FI has not been shown to determine the expression of social cognitive abilities (including ToM), there exists evidence to suggest that this expression may be mediated by CI26. Given this background, intelligence seems to relate to SA both directly and indirectly. Directly, FI seems to support analysis and adaptation to changing social situations. Indirectly, CI seems to aid in perspective-taking abilities, experience, and expression which support SA.
Empathy, a component of SC, must also be considered in this context. EF has been shown to exhibit regulatory control over empathy while also serving as its developmental foundation27,28,29. While EF ability is positively correlated with empathic capacity, this relationship is specifically stronger with cognitive empathy (i.e., understanding what another is feeling) than affective empathy (i.e., feeling what another is feeling)30,31,32,33,34. Cognitive empathy recruits inhibitory control, working memory, and cognitive flexibility while affective empathy only recruits inhibitory control34. Despite its siloed and less significant relationship with EF, affective empathy seems to list cognitive empathy as a prerequisite to its function31. In keeping with its putative position as a higher-level outcome of its precedents in cognitive empathy, affective empathy has been shown to be directly related to the selection of adaptive social strategies among poor individuals. This has not been shown to be the case for wealthy individuals35. Given this context, it is of critical importance to consider EF and empathy in evaluating SA in individuals of low SES.
Prior studies have investigated interactions between the aforementioned cognitive functions (e.g., EF, FI, SC) in isolation and in populations temporarily experiencing low SES. However, to our knowledge, no previous studies have investigated the relationships between these constructs and the predicting roles played by these functions to better understand SA in populations longitudinally impacted by low SES. Based on the literature overview presented previously, we proposed a model in which the relationships between EF, SC, and intelligence are tested simultaneously to investigate their role in predicting SA (see Fig. 1). We expect that EF serves as a cornerstone variable that predicts, on the one hand, aspects of intelligence, and on the other, components of SC. Both factors—intelligence and SC—might contribute to the effect of EF on SA. Based on this structural model and the reviewed literature, we evaluated the following additional hypotheses: (i) a higher-order factor reflecting the common variance of EF subdomains (i.e., verbal inhibitory control, motor inhibitory control, abstraction, and working memory capacity) is directly related to latent variables reflecting ToM, FI, and affective empathy; (ii) ToM is directly related to affective empathy and the latter is directly related to SA [we did not hypothesize a direct path between ToM and FI because there is limited evidence for adults in Latin America living in long-term vulnerable contexts—however, we contrast this model with an alternative one including this path in the Supplementary Materials]; (iii) FI is directly related to CI and the latter is directly related to SA (i.e., direct effect); (iv) FI is indirectly related to SA through CI (i.e., indirect effect). Taken together, this paper aims to determine the potential of the above-mentioned cognitive features in predicting SA in adults living in socially vulnerable contexts since childhood.

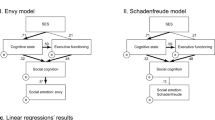
Structural equation modelling social adaptation of vulnerable populations. Main results. (A) Structural equation model 1; (B) Model fit, values in brackets denote 90% confidence intervals; (C) Monte Carlo simulations of the distribution of the unstandardized indirect effect of fluid intelligence (FI) on social adaptation (SA) through crystallized intelligence (CI), values in brackets denote 95% confidence intervals. Variables in circles are unobserved (latent) factors explaining observed (manifest) variables (not shown). Arrows indicate the hypothesized pathways with numbers as the standardized regression estimates. Dashed lines indicate that the effects were not statistically significant. WMC working memory capacity, Abstr. Abstraction, V.Inh verbal inhibitory control, M.Inh motor inhibitory control, EF executive function, ToM theory of mind, FI fluid intelligence, AE affective empathy, SA social adaptation, M marginal effect.
Methods
The data presented in this paper were part of a multidimensional study in which social adaptation in vulnerable populations was studied in different waves. The data presented here corresponded to the 2014–15 wave and they have not been published before.
Participants
A total of 226 adults (51.3% female) between ages 18 to 60 took part in this study (M = 42.00, SD = 14.80). The mean years of education were around nine (M = 9.44, SD = 3.24, Range = 0–18). This equates to incomplete secondary studies. All participants have lived most of their lives in vulnerable socioeconomic contexts according to the Social Protection Sheet of the Ministry of Social Development and Family of the Chilean government36. All participants were qualified as a part of the 40th percentile of the lowest income range (stretch 1 of 7) of the Chilean Welfare Program36. This socioeconomic qualification depends on: (i) the sum of labor, pension, and capital income of all members of the household; (ii) the number of household members; (iii) characteristics of the household members: age, disability, or dependency; (iv) evaluation of goods and services to which a household has access or owns and which allow for inference of its socioeconomic status when compared to the actual income received by the household. Furthermore, most of the participants lived in neighborhoods in Santiago, Chile that have a high social risk index and participated in a social program of the Ministry of Social Development and Family.
According to the above-mentioned criteria, before starting the study, we performed a brief semi-structured interview to establish the degree of each individual’s exposure to a long-term socially vulnerable context. Only participants who met this criterion participated in the study. Participation was voluntary and data were anonymized. We excluded individuals with a visual or hearing impairment who told us they would be unable to complete our assessment battery (e.g., to read or respond to verbal information or to follow the evaluator’s oral instruction). Persons with psychiatric or neurological conditions did not participate. All participants provided a signature as proof of their informed consent. The study received prior approval from the ethics committee of the Adolfo Ibañez University (Santiago, Chile) and followed the protocol of the Declaration of Helsinki.
Procedure
All neuropsychological tests, socio-demographic and psychological questionnaires used in this study were administered by licensed clinical social workers and clinical psychologists. Each evaluator made sure that each participant understood the informed consent before administering the tests. Participants were informed that they retained the right to clarify any confusion at any time by asking the examiner directly. The battery of assessments was randomly sequenced for each participant to reduce order bias. Participants took approximately 90 min to complete the protocol, including a 15-min break. Most of the interviews were conducted in the neighborhoods in which the participants lived—typically, in the community meeting house. The field study was carried out between 2014 and 2015.
Instruments
The study protocol included the following measures. Estimates of reliability were calculated with the split-half methods (Spearman-Brown coefficient) for dichotomic scales and Cronbach’s α from Likert scales.
-
(a) EF measurement with INECO Frontal Screening (IFS)37,38. This tool evaluates EF through a diversity of domains: motor programming, conflicting instructions, Go-No Go testing (to measure motor inhibition; M.Inh.), and verbal inhibitory control testing (to measure verbal inhibitory control: V.Inh.); proverb interpretation (to measure abstraction: Abstr.); and backwards digit span, phonological loop, and visuospatial sketchpad testing (to measure working memory capacity: WMC). IFS is a sensitive instrument and has been tested in patients with frontal lobe injuries and neuropsychiatric disorders against healthy controls38,39. It has been used in current populations37. The reliability of the Chilean version of IFS was α = 0.90537. The reliability of the sample was α = 0.76.
-
(b) FI and CI measurement through the Wechsler Adult Intelligence Scale III (WAIS-III)40 and two subtests: progressive matrices, using raw (not standardized) scores (to measure FI; consists of 26 trials, so 26 is the maximum direct score) and vocabulary (to measure CI; consists of 33 words for which meaning must be explained). WAIS-III has been validated in its assessment of both SC-specific factors41 as well as intelligence in healthy controls and patients with frontal lobe lesions and neuropsychiatric disorders42. Note that we applied this version of the assessment and not WAIS-IV because their norms were published while data of the present investigation were being collected. Estimates of reliability ranged from α = 0.86 to 0.95 across different ages for vocabulary subscale, and α = 0.76 to 0.94 across ages for matrices subscale43. In the present study, both subscales showed high reliability for this sample—α = 0.79 and α = 0.75, respectively.
-
(c) ToM measurement through the Reading the Mind in the Eyes Test and Mini-Sea. The Reading the Mind in the Eyes Test evaluates ToM through the presentation of 17 pictures of human faces44 in which only the area around the eyes is visible45,46; emotional state must be interpreted by the participant based on the image. It has been validated for its use in evaluating ToM in healthy populations47 as well as those who have been shown to exhibit deficits in SC (e.g., people living with schizophrenia, autism, anorexia)45,48,49. In complement, emotional recognition was tested with the Mini-Sea50. This instrument includes two subtests: (i) a facial emotion recognition test (from Ekman pictures; scored from 0 to 15) in which participants are instructed to categorize the emotion that is being expressed; and (ii) a shortened version of the Faux Pas recognition test51 used to evaluate ToM based on stories that describe everyday social situations. The reliability of Reading the Mind Test test was 0.5644. In the present study, α = 0.51 was obtained for the Reading the Mind Eyes and α = 0.78 for the Mini Sea. Although the reliability of the Reading the Mind in the Eyes Test was not good, it must be considered that calculating Cronbach’s alfa would not be suitable for this test —as is the case with other similar tests designed to measure emotion recognition, such as MiniPONS52. In these cases, only correct responses between individuals can be compared and thus, calculating this parameter is not straightforward53. However, recent studies have reported acceptable test–retest reliability for the adult version of the test in very different samples, which contributes to solving this gap47,53,54,55. Test–retest reliability for the Spanish version was 0.63 based on the interclass correlation53].
-
(d) Affective empathy measurement through the Empathy Quotient—a 60-item questionnaire in which 40 questions explore empathy and 20 serve as fillers to avoid an excessive and conspicuous focus on empathy that might trigger biased response56. The affective dimension was calculated through a parcel analysis of affective items of empathy57. The use of the Empathy Quotient has been validated in healthy populations as well as those with depersonalization symptoms and autism spectrum disorders58,59,60. Item reliability for the EQ was 0.9959. In this sample, α = 0.75 was obtained.
-
(e) SA measurement using the Social Adaptation Self-evaluation Scale (SASS). This instrument was developed as a quick and straightforward evaluation that specifically targets the measurement of social motivation and behavior of the examinee61,62. It contains 21 questions that explore job interest, homework interest, work enjoyment, interest in hobbies, quality of spare time, relationship-seeking behavior (familiar, romantic, and platonic), relationship quality and appreciation, sociability, social attractiveness, social compliance, community involvement, intellectual interest, communication difficulties, rejection sensitivity, vainness, difficulty in coping with resources, and control of surroundings. The use of SASS in evaluating SA has been validated in both healthy populations as well as in patients with Major Depressive Disorder and Bipolar Disorder63. The reliability is 0.7861,62. In this study, α = 0.90 was obtained.
Statistical analysis
Structural Equation Modeling (SEM) analysis was used to estimate the proposed model, provide a detailed accounting of measurement errors, and accurately estimate the structural relations between latent factors64. Data preparation, analyses, and plotting were conducted with R in RStudio65 using the following packages: tidyverse66, lavaan67,68 semTools69 and semPlot70.
Since the data were not normally distributed, we used maximum likelihood estimation with robust (Huber-White) standard errors; a chi-square (χ2) statistic was scaled by the Yuan-Bentler correction factor71. A full information maximum likelihood estimation method was implemented to account for missing data72. For identification and scaling of the model, the variance of each latent variable was fixed to one. Structural equation modelling adequacy fit indices were used to assess model goodness of fit: the YB χ2 statistic, the robust comparative fit index (CFI)73, and the root mean square error approximation (RMSEA)73. The YB χ2 statistic is used as a fit index and it is expected to be as close to zero as possible, thus it is not expected to be significant (i.e., p-value should be > 0.05). The CFI is an index with values from 0 to 1 assessing the extent to which the specified model improves fit over the null model (values > 0.90 considered as adequate fit, values in the range of 0.95–0.99 considered as excellent fit, and a value of one considered as exact fit)74. The RMSEA indicates the discrepancies between the sample variance-covariance matrix and the model-implied variance-covariance matrix (values > 0.08 considered as poor fit, values in the range of 0.05–0.08 considered as adequate fit, and values ≤ 0.05 considered as good fit)64. Finally, Monte Carlo simulations were used to construct confidence intervals for the indirect effects75.
Results
The fit of the model to data was excellent (see Panel B of Fig. 1) [Supplementary material presents a comparison of this model with two alternative models. Data analysis indicates that this model offers the best approximation to the data]. The structural model and standardized model parameters are shown in Fig. 1 (factor loadings are shown in Table 1). The descriptive statistics of the model variables are shown in Table 2. The EF factor was specified as a second-order factor in which seemingly distinct but related factors (i.e., WMC, Abstr.: V.Inh., and M.Inh.) are accounted for by one common underlying higher-order factor76,77. The factor loadings for all first-order factors (i.e., WMC, Abstr. V.Inh, and M.Inh) were statistically significant (p < 0.01, see Table 1). As expected, the influence of EF on ToM and FI was statistically significant (p < 0.01; hypothesis 1). However, EF exhibited a strong negative correlation to affective empathy (β = − 0.71, p = 0.094; hypothesis 1, see Fig. 1). Concerning the second hypothesis, ToM was moderately related to affective empathy (β = 0.64, p = 0.051). Contrary to our prediction, affective empathy was negatively related to SA (p < 0.05). Additionally, FI was strongly related to CI (p < 0.001) and the latter was related to SA (p < 0.01; hypothesis 3). In this model we also tested the hypothesis that the prediction of FI to SA may be accounted for by CI. To this aim, we estimate the direct and indirect effects of FI on SA. The direct effect is the influence of FI on SA controlling for CI. The indirect effect is the influence of FI on SA through CI. As panel A of Fig. 1 displays, the direct effect was weak and nonsignificant (direct effect β = 0.02, p = 0.867, see the value of the dashed black line in Fig. 1). The standardized indirect effect was small (β = 0.28) and reliable. Monte Carlo simulations for constructing confidence intervals of the unstandardized indirect effect revealed that they did not include zero (see panel C of Fig. 1). This finding suggests that the effect of FI on SA is accounted for by CI (hypothesis 4). That is, persons with better FI exhibited higher scores in CI, which in turn predicted higher levels of SA.
Finally, in accordance with the reviewer’s request, we have conducted an additional analysis to test the SEM model proposed (Model 1) against rival models. We presented two alternative models in the Supplementary Materials section, including an additional path from FI to ToM (Model 2), and an additional path from EF to ToM (Model 3). The fit of models 1 and 2 were identical, but the path from FI to ToM was non-significant, suggesting that it is unnecessary to include it in the model. This could be indicating that, in the presence of an effect of EF to ToM, the influence of FI on ToM was not important. Thus, Model 1 was preferable. The comparison between models 1 and 3 showed similar goodness-of-fit and similar parameter estimates, but Model 1 presents the smallest AIC and ΔAIC indicates no support for Model 3. Taken together, the model proposed in this paper (Model 1) was the best representation of the data.
Discussion
This study was conducted to evaluate the dynamics of specific cognitive features—EF, SC, and intelligence—in predicting SA among a population that has sustained low SES over their lifetime. Our main hypothesis was that EF serves as a cornerstone variable that predicts components of SC and aspects of intelligence and that both factors—SC and intelligence—might contribute to the effect of EF on SA. In evaluating our SEM according to our first hypothesis, EF was found to be positively related to both ToM and FI. Unexpectedly, it was negatively related to affective empathy. Moreover, according to our second hypothesis, ToM was positively related to affective empathy, but again unexpectedly, affective empathy was negatively linked to SA. Concerning the relationship of FI to SA, our results confirm the indirect relationship (hypothesis 4) of FI to SA through CI, while disproving the proposed direct relationship (hypothesis 3). In summary, FI is directly related to CI and indirectly related to SA; FI was directly related to CI and indirectly related SA. That is to say, the role of FI in predicting SA is through CI. We will discuss and further interpret these results in the following sections.
Executive functioning, social cognition, and social adaptation
Concerning the influence of EF on SA, we identified a positive relationship between EF and ToM (a component of SC), which was moderately associated with affective empathy (statistically, it was marginally significant). However, affective empathy was negatively related to SA.
This first relationship was expected: SC (ToM) together with EF have been shown to play a crucial role in the regulation of social interaction80,81. Impairment in SC has also been observed among individuals who show social adaptation impairments such as those with mental health disorders82 and neurodegenerative diseases83 as well as in delinquents84 and ex-combatants85,86. Impairments in socio-affective variables—specifically, low internal locus of control, self-esteem, and high stress—have been also described among individuals living in vulnerable environments87.
Paradoxically, EF exhibited a strong negative correlation with affective empathy—a component of SC that was inversely related to SA in this population (although this was statistically marginally significant). This runs contrary to the findings of Sun et al. whose data suggest that poor individuals who exhibit greater affective empathy also exhibit greater coping strategies that support SA35. The non-replication of these results may stem from differences in the sample populations. This study focused on adults living in socially vulnerable conditions since childhood. This seems relevant given that certain areas with disproportionately low SES can be perceived as territorial traps for the most disadvantaged. In these areas, financial and professional opportunities can be scarce and resources to progress are inaccessible to most. The population recruited in this study exhibits low social mobility. Typically, several generations of their families have remained in the same place. According to an OECD report in 2019, the high levels of inequality in Chile tend to hamper income and social mobility88. For instance, it could take six generations for descendants of a family located in the lowest 10% of the income distribution to reach the average income compared to only four to five generations on average in all OECD countries88. This is also reinforced by Delaunay89 who states, “in Chile, the propensity to move, whether it is migration or daily mobility, increases in general with the socioeconomic level of the people, from which it follows that those of the lower strata have few options to use migration as a resource to get out of poverty” [89; p.1]. Sun et al. focused on people with low SES at the time the study was conducted with no control for maintenance or duration of SES35. Extended duration of impoverishment with origins in childhood may play a role in reversing the socially protective effects provided by affective empathy in populations living in poverty whose SES has sustained over their life course.
Our results align with other studies that pointed out that empathy is cognitively taxing, and thus, people tend to avoid it. Across 11 studies and a meta-analytic review, a strong preference to avoid empathy and as well as a tendency to feature conceptions of empathy as being more effortful and aversive and less efficacious than an alternative course of action have been identified90. We speculate that this could explain the negative relationship that we found between EF and affective empathy. Better EF abilities in adults living in poverty could assist them in better self-regulating responses to potential vicarious distress that could trigger a high empathic concern with other people. This empathy regulation—the inhibition of empathy-related behaviors and the avoidance of empathy-involved situations—to avoid distress, could, in turn, thwart SA. This theory should be addressed in future research among controlled populations of varying SES for validation.
Executive functioning, intelligence and social adaptation
Our results showed a positive correlation between EF and FI, which was indirectly associated with SA through CI. Previous research has supported a positive reciprocal relationship between EF and FI91 suggesting that changes in both domains might operate bidirectionally. Among the various EFs, it is WM that has been most strongly associated with both FI and CI92,93,94,95,96. Executive functions are critical for activating, maintaining, and selecting appropriate actions or thoughts to achieve goals; they are central to self-control and self-regulation97 which aids mental, social, and physical long-term adaptation in “normalized” environments98,99. On the contrary, disadvantaged social environments promote low executive functioning (EF)13,17,100. Individuals that have to deal with a high amount of life stress and unpredictability may have deficits both in working memory capacity100—due to the added burden of chronic inhibition of unwanted thoughts about adverse life events—and in the inhibition of prepotent responses101.
Additionally, the finding that EF predicts FI and CI and that FI predicts SA through CI was expected as the relationship between intelligence and SA has been tested previously10. Recently, Huepe and Salas suggested that the elucidation of prefrontal cortex functions such as FI and perspective changing is crucial for understanding psychosocial adaptation mechanisms102. We did not find a direct effect of FI, but the comparison with other previous studies is not straightforward. In our model, the direct effect indicates the influence of FI on SA controlling for CI, whereas other studies have only tested the linear relationship between FI and SA without controlling for CI10,87. While it has been suggested that lower levels of education and overall socioeconomic deprivation could limit the use of FI10, other lines of research have suggested that intelligence itself is a predictor of poverty and health inequalities103,104. The combined role of this domain remains elusive; whether intelligence can be considered as a driver or an outcome of living in vulnerable conditions is unclear. Our results suggest that FI is more strongly associated with SA given its relationship to CI. These results corroborate those of a previous study105 that found that FI and CI could act as cognitive reserve that could have potential protective effects for people living in vulnerable contexts. Further research on the function and interaction of intelligence as it relates to SA may help to support the position of intelligence as a target for therapeutic exercise to improve psychosocial wellbeing in vulnerable populations. Systematic work in vulnerable contexts suggests that despite the limited capacity for improvement exhibited by cognitive functions such as intelligence and EF in childhood, developing therapeutic programs that favor empathy, the use of intelligence and some cognitive functions (such as self-regulation and decision-making control) allow for greater SA106,107.
The methods and findings described above present several limitations. First, the Social Adaptation Self-evaluation Scale (SASS) used to measure SA in participants incorporates issues related to social desirability bias into our results. Despite the above, the instrument showed good psychometric indicators and the results were consistent with what was expected (predictive validity). Notwithstanding, future research on this topic should employ SA measurement methods that encompass aspects of peer evaluation to provide comparison and reduce this bias. Second, we are aware that the WAIS-III assessment used in this study was normed in 1998. However, taking that and the date of publication of the norms of WAIS-IV for the Chilean population (2014) into account, we deemed appropriate the omission of standardized scores for IQ and rather used the direct scores of two subscales with good reliability estimates. We think that this guarantees the accuracy of the measure.
Additionally, participants recruited for this study did not include individuals of higher SES. Though conclusions were made based on the data set presented by our study, putative explanations provided by comparison to previous peer-reviewed research of populations with differing SES and living conditions require further research to substantiate. In future research, a more exhaustive and diverse sample population should be recruited to include those who have sustained high SES over their lifetime, those who lived with low SES in childhood and later lived with high SES, and those who lived with high SES in childhood and later lived with low SES. Research of this kind might yield more accurate comparisons, claims, and explanations of etiology in controlling for factors not directly isolated in this study that may impact cognition and SA.
Conclusions
The results presented by this study support the validity and significance of EF, SC, and intelligence in predicting SA among adults living in vulnerable conditions since childhood. Specifically, the findings suggest that EF plays a fundamental role in the manifestation of SA in this population. Further longitudinal research among populations of varying SES—in both level and duration sustained—is required to validate the potential explanations suggested by the findings of this study and to inform effective intervention methods to promote psychosocial health among people living in vulnerable conditions across life stages.
Data availability
For requesting access to the full database that support the manuscript, please write to the corresponding authors.
References
Miao, H., Li, Z., Yang, Y. & Guo, C. Social comparison orientation and social adaptation among young Chinese adolescents: The mediating role of academic self-concept. Front. Psychol. https://doi.org/10.3389/fpsyg.2018.01067 (2022).
Chaudhuri, S. Assessing Vulnerability to Poverty: Concepts, Empirical Methods and Illustrative Examples (Columbia University, 2003).
Evans, G. W. & English, K. The environment of poverty: Multiple stressor exposure, psychophysiological stress and socioemotional adjustment. Child Dev. 73(4), 1238–1248 (2002).
Evans, G. W., Gonnella, C., Marcynyszyn, L. A., Gentile, L. & Salpekar, N. The role of chaos in poverty and children’s socioemotional adjustment. Psychol. Sci. 16(7), 560–565 (2005).
Henoch, P. Vulnerabilidad social Más allá de la pobreza. Serie Informe Social, 128(7) 1–24 (2010).
Evans, G. W. & Kim, P. Early childhood poverty and adult chronic physiological stress: The mediating role of childhood cumulative risk exposure. Psychol. Sci. 23(9), 979–983 (2012).
Evans, G. W. & Kim, P. Multiple risk exposure as a potential explanatory mechanism for the socioeconomic status-health gradient. Ann. N. Y. Acad. Sci. 1186, 174–189. https://doi.org/10.1111/j.1749-6632.2009.05336.x (2010).
Amadó, A., Serrat, E. & Vallès-Majoral, E. The role of executive functions in social cognition among children with down syndrome: Relationship patterns. Front. Psychol. 7, 1363. https://doi.org/10.3389/fpsyg.2016.01363 (2016).
Evans, G. W. & Schamberg, Ma. Childhood poverty, chronic stress, and adult working memory. Proc. Natl. Acad. Sci. 106(16), 6545–6549. https://doi.org/10.1073/pnas.0811910106 (2009).
Huepe, D. et al. Fluid intelligence and psychosocial outcome: from logical problem solving to social adaptation. PLoS ONE 6(9), e24858. https://doi.org/10.1371/journal.pone.0024858 (2011).
Lipina, S. et al. Linking childhood poverty and cognition: Environmental mediators of non-verbal executive control in an Argentine sample. Dev. Sci. 16(5), 697–707 (2013).
Wade, M. et al. On the relation between theory of mind and executive functioning: A developmental cognitive neuroscience perspective. Psychon. Bull. Rev. 25, 2119–2140. https://doi.org/10.3758/s13423-018-1459-0 (2018).
Blair, C. et al. Salivary cortisol mediates effects of poverty and parenting on executive functions in early childhood. Child Dev. 82(6), 1970–1984 (2011).
Brieant, A., Peviani, K. M., Lee, J. E., King-Casas, B. & Kim-Spoon, J. Socioeconomic risk for adolescent cognitive control and emerging risk-taking behaviors. J. Res. Adolesc. 31(1), 71–84. https://doi.org/10.1111/jora.12583 (2020).
Corvo, K. The role of executive function deficits in domestic violence perpetration. Partn. Abus. 5(3), 342–356 (2014).
Dolan, S. L., Bechara, A. & Nathan, P. E. Executive dysfunction as a risk marker for substance abuse: The role of impulsive personality traits. Behav. Sci. Law 26(6), 799–822 (2008).
Mani, A., Mullainathan, S., Shafir, E. & Zhao, J. Poverty impedes cognitive function. Science 341(6149), 976–980. https://doi.org/10.1126/science.1238041 (2013).
Marazziti, D. et al. Executive function abnormalities in pathological gamblers. Clin. Pract. Epidemiol. Ment. Health 4(1), 1–6 (2008).
Reynolds, B. W., Basso, M. R., Miller, A. K., Whiteside, D. M. & Combs, D. Executive function, impulsivity and risky behaviors in young adults. Neuropsychology 33(2), 212 (2019).
Verdejo-García, A. et al. Impulsivity and executive functions in polysubstance-using rave attenders. Psychopharmacology 210(3), 377–392 (2010).
Colvert, E. et al. Do theory of mind and executive function deficits underlie the adverse outcomes associated with profound early deprivation?: Findings from the English and Romanian adoptees study. J. Abnorm. Child Psychol. 36(7), 1057–1068. https://doi.org/10.1007/s10802-008-9232-x (2008).
Yeh, Z.-T., Tsai, M.-C., Tsai, M.-D., Lo, C.-Y. & Wang, K.-C. The relationship between theory of mind and the executive functions: Evidence from patients with frontal lobe damage. Appl. Neuropsychol. Adult 24(4), 342–349. https://doi.org/10.1080/23279095.2016.1185425 (2016).
Estes, D. & Bartsch, K. Theory of mind: A foundational component of human general intelligence. Behav. Brain Sci. https://doi.org/10.1017/S0140525X16001618 (2017).
Osterhaus, C. et al. Theory of mind and diverse intelligences in 4-year-olds: Modelling associations of false beliefs with children’s numerate-spatial, verbal and social intelligence. Br. J. Dev. Psychol. 38(4), 580–593 (2020).
Brydges, C. R., Reid, C. L., Fox, A. M. & Anderson, M. A unitary executive function predicts intelligence in children. Intelligence 40(5), 458–469 (2012).
Yirmiya, N., Solomonica-Levi, D., Shulman, C. & Pilowsky, T. Theory of mind abilities in individuals with autism, down syndrome, and mental retardation of unknown etiology: The role of age and intelligence. J. Child Psychol. Psychiatry 37(8), 1003–1014 (1996).
Decety, J. & Meyer, M. From emotion resonance to empathic understanding: A social developmental neuroscience account. Dev. Psychopathol. 20(4), 1053–1080 (2008).
de Waal, F. B. M. & Preston, S. D. Mammalian empathy: Behavioural manifestations and neural basis. Nat. Rev. Neurosci. 18(8), 498 (2017).
Heyes, C. Empathy is not in our genes. Neurosci. Biobehav. Rev. 95, 499–507 (2018).
Decety, J. The neurodevelopment of empathy in humans. Dev. Neurosci. 32(4), 257–267 (2010).
Healey, M. L. & Grossman, M. Cognitive and affective perspective-taking: Evidence for shared and dissociable anatomical substrates. Front. Neurol. https://doi.org/10.3389/fneur.2018.00491 (2018).
Pfeifer, J. H., Iacoboni, M., Mazziotta, J. C. & Dapretto, M. Mirroring others’ emotions relates to empathy and interpersonal competence in children. Neuroimage 39(4), 2076–2085. https://doi.org/10.1016/j.neuroimage.2007.10.032 (2008).
Warrier, V. et al. Genome-wide analyses of self-reported empathy: correlations with autism, schizophrenia, and anorexia nervosa. Trans. Psychiatry 8(1), 35. https://doi.org/10.1038/s41398-017-0082-6 (2018).
Yan, Z., Hong, S., Liu, F. & Su, Y. A meta-analysis of the relationship between empathy and executive function. PsyCh J. 9(1), 34–43 (2020).
Sun, R., Vuillier, L., Hui, B. P. H. & Kogan, A. Caring helps: Trait empathy is related to better coping strategies and differs in the poor versus the rich. PLoS ONE 14(3), e0213142 (2019).
Ministerio de Desarollo Social y Familia - Gobierno de Chile. (2020). Caracterización Socioeconómica. Data Social: Registro Social de Hogares. Retrieved March 14, 2022, from http://www.registrosocial.gob.cl/que-es#top. Accessed 14 March 2022
Ihnen, J., Antivilo, A., Muñoz-Neira, C. & Slachevsky, A. Chilean version of the INECO Frontal Screening (IFS-Ch): Psychometric properties and diagnostic accuracy. Dement. Neuropsychol. 7(1), 40–47 (2013).
Torralva, T., Roca, M., Gleichgerrcht, E., Bekinschtein, T. & Manes, F. A neuropsychological battery to detect specific executive and social cognitive impairments in early frontotemporal dementia. Brain 132(Pt 5), 1299–1309. https://doi.org/10.1093/brain/awp041 (2009).
Torralva ,T., Roca, M., Gleichgerrcht, E., López, P. & Manes F. INECO Frontal Screening (IFS): a brief, sensitive, and specific tool to assess executive functions in dementia. J Int Neuropsychol Soc. 15(5), 777–786. https://doi.org/10.1017/S1355617709990415 (2009).
Wechsler, D. (1997). WAIS-III: Wechsler adult intelligence scale (3rd ed.). San Antonio, TX: Psychological Corporation (Spanish adaptation: WAIS-III: Escala Wechsler para adultos. Madrid: TEA, 1998).
Allen, D. N. & Barchard, K. A. Identification of a social cognition construct for the WAIS-III. Appl. Neuropsychol. 16(4), 262–274. https://doi.org/10.1080/09084280903297727 (2009).
Cockcroft, K., Alloway, T., Copello, E. & Milligan, R. A cross-cultural comparison between South African and British students on the wechsler adult intelligence scales third edition (WAIS-III). Front. Psychol. 6, 297. https://doi.org/10.3389/fpsyg.2015.00297 (2015).
García, L. F., Ruiz, M. Á. & Abad, F. J. Factor structure of the Spanish WAIS-III. Psicothema 15(1), 155–160 (2003).
Redondo, I. & Herrero-Fernández, D. Validation of the reading the mind in the eyes test in a healthy Spanish sample and women with anorexia nervosa. Cognit. Neuropsychiatry 23(4), 201–217. https://doi.org/10.1080/13546805.2018.1461618 (2018).
Baron-Cohen, S., Wheelwright, S., Hill, J., Raste, Y. & Plumb, I. The “Reading the Mind in the Eyes” Test revised version: A study with normal adults, and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry 42(2), 241–251. https://doi.org/10.1111/1469-7610.00715 (2001).
Brüne, M. & Brüne-Cohrs, U. Theory of mind—evolution, ontogeny, brain mechanisms and psychopathology. Neurosci. Biobehav. Rev. 30(4), 437–455 (2006).
Vellante, M. et al. The “reading the mind in THE Eyes” test: Systematic review of psychometric properties and a validation study in Italy. Cogn. Neuropsychiatry 18(4), 326–354. https://doi.org/10.1080/13546805.2012.721728 (2013).
Harrison, A., Tchanturia, K. & Treasure, J. Attentional bias, emotion recognition and emotiosn regulation in anorexia: State or trait?. Biol. Psychiat. 68(8), 755–761. https://doi.org/10.1016/j.biopsych.2010.04.037 (2010).
Kettle, J. W., O’Brien-Simpson, L. & Allen, N. B. Impaired theory of mind in first-episode schizophrenia: Comparison with community, university and depressed controls. Schizophr. Res. 99(1–3), 96–102. https://doi.org/10.1016/j.schres.2007.11.011 (2008).
Bertoux, M. et al. Social Cognition and emotional assessment differentiates frontotemporal dementia from depression. J. Neurol. Neurosurg. Psychiatry 83(4), 411–416. https://doi.org/10.1136/jnnp-2011-301849 (2012).
Stone, V. E., Baron-Cohen, S. & Knight, R. T. Frontal lobe contributions to theory of mind. J. Cogn. Neurosci. 10(5), 640–656. https://doi.org/10.1162/089892998562942 (1998).
Bänziger, T., Scherer, K., Hall, J. & Rosenthal, R. Introducing the MiniPONS: A short multichannel version of the profile of nonverbal sensitivity (PONS). J. Nonverbal Behav. 35, 189–204. https://doi.org/10.1007/s10919-011-0108-3 (2011).
Fernández-Abascal, E. G. et al. Test-retest reliability of the ‘reading the mind in the eyes’ test: A one-year follow-up study. Mol. Autism 4, 33. https://doi.org/10.1186/2040-2392-4-33 (2013).
Yıldırım, E. A. et al. Investigation of the reliability of the “reading the mind in the eyes test” in a Turkish population. Turk psikiyatri dergisi = Turkish J. Psychiatry 22(3), 177–186 (2011).
Hallerbäck, M. U., Lugnegård, T., Hjärthag, F. & Gillberg, C. The reading the mind in the eyes test: Test-retest reliability of a Swedish version. Cogn. Neuropsychiatry 14(2), 127–143. https://doi.org/10.1080/13546800902901518 (2009).
Baron-Cohen, S. & Wheelwright, S. The empathy quotient: An investigation of adults with asperger syndrome or high functioning autism, and normal sex differences. J. Autism Dev. Disord. 34(2), 163–175. https://doi.org/10.1023/B:JADD.0000022607.19833.00 (2004).
Little, T. D., Cunningham, W. A., Shahar, G. & Widaman, K. F. To parcel or not to parcel: Exploring the question, weighing the merits. Struct. Equ. Model. 9(2), 151–173 (2002).
Lawrence, E., Shaw, P., Baker, D., Baron-Cohen, S. & David, A. Measuring empathy: Reliability and validity of the empathy quotient. Psychol. Med. 34(5), 911–920. https://doi.org/10.1017/S0033291703001624 (2004).
Allison, C., Baron-Cohen, S., Wheelwright, S. J., Stone, M. H. & Muncer, S. J. Psychometric analysis of the empathy QUOTIENT (EQ). Personality Individ. Differ. 51(7), 829–835. https://doi.org/10.1016/j.paid.2011.07.005 (2011).
Fernández, A., Baeza, C., Pavez, P. & Aldunate, N. Chilean version of the empathy quotient (EQ) scale: Adaptation and psychometric properties. Span. J. Psychol. 24, E24. https://doi.org/10.1017/SJP.2021.2 (2021).
Bobes, J. et al. Validation of the Spanish version of the social adaptation scale in depressive patients. Actas Espanolas de Psiquiatria 27(2), 71–80 (1999).
Bosc, M., Dubini, A. & Polin, V. Development and validation of a social functioning scale, the social adaptation self-evaluation scale. Eur. Neuropsychopharmacol. 7(1), S57–S70 (1997).
Ohtani, T. et al. Association between longitudinal changes in prefrontal hemodynamic responses and social adaptation in patients with bipolar disorder and major depressive disorder. J. Affect. Disord. 176, 78–86. https://doi.org/10.1016/j.jad.2015.01.042 (2015).
Bollen, K. A., Long, J. S., Browne, M. W., & Cudeck, R. (1993). Alternative Ways of Assessing Model Fit. In Testing structural equation models (pp. 136–162). essay, Sage.
RStudio Team. (2022). Open source & professional software for data science teams. RStudio. Retrieved from https://www.rstudio.com/. Accessed 14 March 2022
Wickham, H. et al. Welcome to the Tidyverse. J. Open Source Softw. 4(43), 1686 (2019).
Rosseel, Y. lavaan: An R package for structural equation modeling. J. Stat. Softw. 48(2), 1–36 (2012).
Rosseel, Y. et al. Package ‘lavaan’. Retriev. June 17(2017), 1 (2017).
Jorgensen, T. D., Pornprasertmanit, S., Schoemann, A. M., Rosseel, Y., Miller, P., & Quick, C. & Mansolf, M. semTools: Useful tools for structural equation modeling. R Package Version 0.5–2.Computer Software https://CRAN.R-project.org/package=semTools. (2018) Accessed 14 March 2022
Epskamp, S. semPlot: Path Diagrams and Visual Analysis of Various SEM Packages’ Output. R Package Version 1.1.2. Computer Software https://CRAN.R-project.org/package=semPlot (2019). Accessed 14 March 2022
Yuan, K. H. & Bentler, P. M. Three likelihood-based methods for mean and covariance structure analysis with nonnormal missing data. Sociol. Methodol. 30(1), 165–200. https://doi.org/10.1111/0081-1750.00078 (2000).
Baraldi, A. N. & Enders, C. K. An introduction to modern missing data analyses. J. Sch. Psychol. 48, 5–37 (2010).
Savalei, V. On the computation of the RMSEA and CFI from the mean-and-variance corrected test statistic with nonnormal data in SEM on the computation of the RMSEA and CFI from the mean-and-variance corrected test statistic with nonnormal data in SEM. Multivar. Behav. Res. 53, 419–429. https://doi.org/10.1080/00273171.2018.1455142 (2018).
Little, T. D. Model fit, simple size and power. In Longitudinal Structural Equation Modeling (ed. Little, T. D.) 106–136 (Guildford Press, 2013).
Preacher, K. J. & Selig, J. P. Advantages of Monte Carlo confidence intervals for indirect effects. Commun. Method. Meas. 6(2), 77–98 (2012).
Chen, F. F., Sousa, K. H. & West, S. G. Teacher’s corner: Testing measurement invariance of second-order factor models. Struct. Equ. Modeling 12(3), 471–492. https://doi.org/10.1207/s15328007sem1203_7 (2005).
Kline, R. B. Principles and Practice of Structural Equation Modeling 134–134 (The Guilford Press, 2016).
Little, T. D., Rhemtulla, M., Gibson, K. & Schoemann, A. M. Why the items versus parcels controversy needn’t be one. Psychol. Method. 18(3), 285–300. https://doi.org/10.1037/a0033266 (2013).
Field, A. Discovering statistics using IBM SPSS statistics 4th edition. J. Adv. Nurs. https://doi.org/10.1111/j.1365-2648.2007.04270_1.x (2013).
De Jaegher, H., Di Paolo, E. & Gallagher, S. Can social interaction constitute social cognition?. Trends Cogn. Sci. 14(10), 441–447. https://doi.org/10.1016/j.tics.2010.06.009 (2010).
Meyer, M. L., Taylor, S. E. & Lieberman, M. D. Social working memory and its distinctive link to social cognitive ability: An fmri study. Social Cognit. Affect. Neurosci. 10(10), 1338–1347. https://doi.org/10.1093/scan/nsv065 (2015).
Uekermann, J. et al. Social cognition in attention-deficit hyperactivity disorder (ADHD). Neurosci. Biobehav. Rev. 34(5), 734–743. https://doi.org/10.1016/j.neubiorev.2009.10.009 (2010).
Christidi, F., Migliaccio, R., Santamaría-García, H., Santangelo, G. & Trojsi, F. Social cognition dysfunctions in neurodegenerative diseases: Neuroanatomical correlates and clinical implications. Behav. Neurol. 2018, 1–18. https://doi.org/10.1155/2018/1849794 (2018).
Nas, C. N., Orobio De Castro, B. & Koops, W. Social information processing in delinquent adolescents. Psychol. Crime Law 11(4), 363–375. https://doi.org/10.1080/10683160500255307 (2005).
Tobón, C. et al. Emotional processing in Colombian ex-combatants and its relationship with empathy and executive functions. Soc. Neurosci. 10(2), 153–165 (2015).
Trujillo, S. P. et al. Atypical modulations of N170 component during emotional processing and their links to social behaviors in ex-combatants. Front. Hum. Neurosci. 11, 244 (2017).
Neely-prado, A., Navarrete, G. & Huepe, D. Socio-affective and cognitive predictors of social adaptation in vulnerable contexts. PLoS ONE 14(6), e0218236. https://doi.org/10.1371/journal.pone.0218236 (2019).
OECD. (2019). How does Chile compare? - OECD. OECD. Retrieved March 7, 2022, from https://www.oecd.org/chile/sag2019-chile-en.pdf. Accessed 7 March 2022
Delaunay, D. et al. Relaciones entre pobreza, migración y movilidad: Dimensiones territorial y contextual [Relationship between poverty, migration, and mobility: Territorial and contextual dimensions]. In Notas de Población: CEPAL (ed. Bravo, J.) (Naciones Unidas, 2007).
Cameron, C. D. et al. Empathy is hard work: People choose to avoid empathy because of its cognitive costs. J. Exp. Psychol. Gen. 148(6), 962 (2019).
Uka, F., Gunzenhauser, C., Larsen, R. A. & von Suchodoletz, A. Exploring a bidirectional model of executive functions and fluid intelligence across early development. Intelligence 75, 111–121. https://doi.org/10.1016/j.intell.2019.05.002 (2019).
Engle, R. W., Kane, M. J. & Tuholski, S. W. Individual Differences in Working Memory Capacity and what they tell us About Controlled Attention, General Fluid Intelligence, and Functions of the Prefrontal Cortex (Cambridge University Press, 1999).
Redick, T. S. et al. Measuring working memory capacity with automated complex span tasks. Eur. J. Psychol. Assess. 28(3), 164–171. https://doi.org/10.1027/1015-5759/a000123 (2012).
Ackerman, P. L., Beier, M. E. & Boyle, M. O. Working memory and intelligence: The same or different constructs?. Psychol. Bull. 131(1), 30–60. https://doi.org/10.1037/0033-2909.131.1.30 (2005).
Kane, M. J., Hambrick, D. Z. & Conway, A. R. A. Working memory capacity and fluid intelligence are strongly related constructs: Comment on Ackerman, Beier, and Boyle (2005). Psychol. Bull. 131(1), 66–71. https://doi.org/10.1037/0033-2909.131.1.66 (2005).
Oberauer, K., Wilhelm, O., Schulze, R. & Süß, H. M. Working memory and intelligence–Their correlation and their relation: Comment on Ackerman, Beier, and Boyle (2005). Psychol. Bull. 131(1), 61–65. https://doi.org/10.1037/0033-2909.131.1.61 (2005).
Miyake, A. & Friedman, N. P. The nature and organization of individual differences in executive functions: Four general conclusions. Curr. Dir. Psychol. Sci. 21(1), 8–14 (2012).
Mischel, W. et al. “Willpower” over the life span: Decomposing self-regulation. Social Cognit. Affect. Neurosci. 6(2), 252–256. https://doi.org/10.1093/scan/nsq081 (2011).
Moffitt, T. E. et al. A gradient of childhood self-control predicts health, wealth and public safety. Proc. Natl. Acad. Sci. U.S.A. 108(7), 2693–2698. https://doi.org/10.1073/pnas.1010076108 (2011).
Klein, K. & Boals, A. The relationship of life event stress and working memory capacity. Appl. Cogn. Psychol. 15(5), 565–579. https://doi.org/10.1002/acp.727 (2001).
Mittal, C., Griskevicius, V., Simpson, J. A., Sung, S. & Young, E. S. Cognitive adaptations to stressful environments: When childhood adversity enhances adult executive function. J. Pers. Soc. Psychol. 109(4), 604–621. https://doi.org/10.1037/pspi0000028 (2015).
Huepe, D. & Salas, N. Fluid intelligence, social cognition and perspective changing abilities as pointers of psychosocial adaptation. Front. Hum. Neurosci. 7(June), 287. https://doi.org/10.3389/fnhum.2013.00287 (2013).
Gottfredson, L. S. Intelligence: is it the epidemiologists’ elusive “fundamental cause” of social class inequalities in health?. J. Pers. Soc. Psychol. 86(1), 174 (2004).
Strenze, T. Intelligence and socioeconomic success: A meta-analytic review of longitudinal research. Intelligence 35(5), 401–426. https://doi.org/10.1016/j.intell.2006.09.004 (2007).
Salas, N., Escobar, J. & Huepe, D. Two sides of the same coin: fluid intelligence and crystallized intelligence as cognitive reserve predictors of social cognition and executive functions among vulnerable elderly people. Front. Neurol. https://doi.org/10.3389/fneur.2021.599378 (2021).
Marchant Orrego, T., Milicic, N., & Álamos Valenzuela, P. (2013). Impacto en los niños de un programa de desarrollo socio-emocional en dos colegios vulnerables en Chile.
Rosado, P. P., Cruces, A. G., Negrillo, E. A. & Ordás, R. P. Efectos de un programa de Responsabilidad Personal y Social sobre la empatía y la inteligencia emocional en educación física. Retos 44, 504–514 (2022).
Acknowledgements
This work was supported by grants from Comisión Nacional de Investigación Científica y Tecnológica (CONICYT/FONDECYT Regular N 1201486 to David Huepe). Agustin Ibanez is supported by grants from ANID/FONDECYT Regular (1210195 and 1210176); FONCYT-PICT 2017-1820; ANID/FONDAP/15150012; Sistema General de Regalías (BPIN2018000100059), Universidad del Valle (CI 5316); and the MULTI-PARTNER CONSORTIUM TO EXPAND DEMENTIA RESEARCH IN LATIN AMERICA [ReDLat, supported by National Institutes of Health, National Institutes of Aging (R01 AG057234), Alzheimer’s Association (SG-20-725707), Rainwater Charitable foundation—Tau Consortium, and Global Brain Health Institute)]. Natalia Trujillo was supported by Minciencias contracts 777-111577757638, 844-11158446727, 20201680192400001E and 80740-495-2020. Nuria Carriedo was supported by a grant from La Secretaría de Estado de Universidades, Investigación, Desarrollo e Innovación de España. Subvención Modalidad A Estancias de profesores e investigadores Sénior en centros extranjeros, incluido el programa Salvador de Madariaga (PRX19/00147). The contents of this publication are solely the responsibility of the authors and do not represent the official views of these Institutions.
Author information
Authors and Affiliations
Contributions
N.S. and D.H. designed the study; N.S. and D.H. coordinated clinical and neuropsychological assessment; D.H., N.T., O.R-V. and A.I. analyzed the data; D.H., N.T., O.R-V., A.I. and M.S. wrote the manuscript; N.C. revised and wrote the manuscript. All authors contributed to revising the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schulte, M., Trujillo, N., Rodríguez-Villagra, O.A. et al. The role of executive functions, social cognition and intelligence in predicting social adaptation of vulnerable populations. Sci Rep 12, 18693 (2022). https://doi.org/10.1038/s41598-022-21985-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-21985-9
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
