
Abstract
Previous studies have reported adverse effects of short and long sleep duration on cardiovascular health. However, how sleep time and sleep efficiency affect angina have not been studied in hypertensive individuals. This study aimed to assess the relationship of sleep with angina. Using a cross-sectional design, data from 1563 hypertensive individuals were collected from the parent Sleep Heart Health Study (SHHS). Age, alcohol use, average diastolic blood pressure (ADBP), average systolic blood pressure (ASBP), cigarette use, sleep time, sleep efficiency, percent time in stage N3 of sleep, and body mass index (BMI) were used as covariates. Multiple linear regression, the Chi-Square test, and Pearson’s correlation coefficient were used for data analysis. Unadjusted sleep efficiency, sleep time, ADBP, and age were significant (p < 0.05) predictors of the number of angina episodes (Anginan). When the covariates were adjusted, only ADBP and ASBP were significant (p < 0.05) predictors of Anginan. Sleep efficiency, BMI, ADBP, sleep time, and age had a significant (p < 0.05) correlation with Anginan. In hypertensive individuals, sleep time and sleep efficiency did not affect Anginan when adjusted for covariates. ADBP and ASBP were found to be significant predictors of Anginan when the covariates were adjusted.
Similar content being viewed by others


Introduction
To maintain good emotional, mental, and physical health, individuals are required to have good sleep1. Several advantages of good sleep are reported. Normal sleep reduces the workload on the cardiovascular system, therefore, it may enhance cardiovascular longevity, and insufficient sleep may cause adverse consequences2.
Reduction in blood pressure (BP) is reported during normal sleep, where systemic BP decreases by an average of 5–10% in stages N1 and N2 of non-rapid eye movement (NREM) sleep and by 10–15% in stage N33,4. The reduction in heart rate is also observed by 5–10% during NREM sleep. During rapid eye movement (REM) sleep, greater variability is observed in both BP and heart rate. Cardiac output also decreases during NREM sleep4,5,6.
Therefore, there are several benefits of nocturnal sleep on the cardiovascular system, especially through the reduction in systemic BP. Thus, if total sleep time is reduced due to any disorder then the cardiovascular system will be deprived of several benefits it accrues from good nocturnal sleep. The prevalence of sleep problems has been reported from 1.6 to 56% in several studies conducted in different countries throughout the world7,8,9. It’s reported that the ability to perform daily activities of living is directly affected in individuals having sleep disturbances10, which in turn induces a sedentary lifestyle11 that ultimately affects the health and quality of life of such individuals12,13. Sleep for less than 7 h duration is reported to be a significant risk factor for disorders of the nervous system, immune system, endocrine system, and cardiovascular systems, and may result in substance abuse, mood disorders, anxiety disorders, hypertension, cardiovascular diseases, impaired glucose tolerance, diabetes, and obesity in children and adults, thereby increasing the rate of mortality14,15,16,17,18,19. Asplund20 in a large epidemiological study of elderly people in Sweden reported that poor sleep was associated with cardiac dysrhythmias and angina pectoris.
Therefore, several studies have reported how sleep problems are related to cardiovascular system problems, however, to our knowledge, no previous study has been performed to test the association of the number of angina episodes (Anginan) with sleep in hypertensive individuals. The present study used data from the Sleep Heart Health Study (SHHS), which was initiated in 1994 as a multicenter prospective cohort study. The SHHS was a community-based longitudinal study that consisted of several ongoing cohort studies of the respiratory and cardiovascular systems21. Therefore, this study aimed to assess the association of Anginan with sleep time and sleep efficiency in hypertensive individuals.
Materials and methods
A cross-sectional design was used. The demographic characteristics (gender, age, body mass index (BMI), cigarette smoking, alcohol use), cardiovascular variables [average diastolic blood pressure (ADBP), average systolic blood pressure (ASBP), presence of angina, Anginan] and sleep variables (sleep time, percent time in stage N3 of sleep, percentage of time in bed that was spent sleeping) were obtained from the data collected by the parent study Sleep Heart Health Study (SHHS). Only participants of age 40 years or older at the time of the sleep study participated.
The specific aims, designs, and protocols of the SHHS have been previously described21,22. The SHHS Manual of Operations contains a comprehensive description of the methods used in study23. The primary aim of SHHS was to study the cardiovascular consequences of sleep-disordered breathing. The baseline data for SHHS were obtained from nine ongoing epidemiologic studies of cardiovascular and respiratory disease from December 1995 to January 1998 in diverse populations in the United States.
Only the data of hypertensive individuals were used from the SHHS. In SHHS, hypertension was defined as a resting BP of at least 140/90 mmHg or the use of antihypertensive medication24. The parent study (SHHS) included a baseline examination of 5804 participants, of which 3326 were not qualified as hypertensive and a total of 2478 participants qualified as hypertensive. However, out of 2478 participants, 915 participants’ data were missing for one or more variables. These participants were excluded from data analysis. Therefore, ultimately 1563 participants were used for data analysis (Tables 1 and 2). All methods were performed in accordance with the relevant guidelines and regulations.
In SHHS, information related to covariates such as medical history and health-related characteristics was obtained using a standardized questionnaire through an interview by the study technician while visiting participants’ homes. The information regarding cardiovascular health was obtained by asking questions such as if the doctor ever told the participant that he had angina, etc. The responses of the participants were obtained in the form of ‘yes’, ‘no’, or ‘unsure’. Other related information like alcohol use or cigarette packs per year, was also obtained through interviews. Bodyweight, height, and BP were measured during the home visits of the participants using standard protocols. Bodyweight was measured by a portable scale. A manual of operation of SHHS contains detailed information regarding the protocols for these measurements23.
BP measurement
The participants were asked to rest for 5 min, then in a sitting position, 3 BP readings were taken with a 5-min interval in between each reading, with the use of a mercury gauge sphygmomanometer. Systolic and diastolic BPs were measured to the nearest 2 mmHg24.
Measurement of sleep variables
Sleep variables were measured using a single overnight EEG-based polysomnography at the participant’s home and in some cases where the home environment was not conducive to polysomnography, a non-home environment (e.g. a motel) was used21. The Compumedics P Series System (Abbotsford, Victoria, Australia) was used for polysomnography. During the evening home visit, this equipment was calibrated and sensors were placed on the participants21.
The institutional review board of each participating center approved the study. The signed informed consent was obtained from each participant. Data on smoking were also obtained through a questionnaire. Data regarding cardiovascular disease was also obtained through a questionnaire.
Data analysis
SPSS statistical software version 26 (SPSS Inc., Chicago, IL, USA) was used for data analysis. A total of 1563 participants’ data was analyzed. The descriptive statistics of the outcome variable (Anginan) and predictors (age, alcohol use, ADBP, ASBP, cigarette smoking, sleep time, sleep N3, BMI, sleep efficiency) are shown in Table 1. Multiple linear regression analysis was performed to predict the relationship of the dependent variable, i.e. Anginan, with predictors. Pearson’s correlation coefficient was used for correlational analysis between Anginan and other covariates. A Chi-square test was performed to test the relationship between categorical variables (presence of angina and gender). The confidence interval was established at 95%, p < 0.05 considered significant.
Variables:
-
Alcohol use: number of alcoholic drinks per day.
-
Cigarette smoking: Cigarette packs smoked per year.
-
Sleep time: sleep time when the entire sleep was captured.
-
Sleep N3: percent time in stage N3 (stages 3 and 4 according to traditional terminology25) of sleep.
-
Sleep efficiency: percentage of time in bed that was spent sleeping, or the ratio of total sleep time to total time in bed, expressed as a percentage.
Results
Multiple linear regression revealed that unadjusted sleep efficiency, sleep time, ADBP, and age were significant (p < 0.05) predictors of Anginan and were responsible for 0.3%, 0.8%, 0.2%, and 0.9% variance in Anginan, respectively, in the hypertensive population (Table 3). When all the covariates (age, alcohol, ADBP, ASBP, cigarette smoking, sleep efficiency, sleep time, sleep N3, and BMI) were adjusted then only ADBP and ASBP were found to be significant predictors of Anginan (p < 0.05). The adjusted covariates had a significant impact (p < 0.01) on Anginan and were responsible for 2.3% of the variance (Table 4). Pearson’s correlation coefficients between Anginan and other predictors are presented in Table 5. Sleep efficiency, BMI, ADBP, sleep time, and age were found to have a significant (p < 0.05) correlation with Anginan. Among these significant correlations, only age had a positive correlation, otherwise, the rest of the covariates had a negative correlation. Pearson correlation coefficient values are presented in Table 5. The Chi-square test revealed a significant difference (p = 0.01, Cramer’s V = 0.066) in the presence of angina with gender differences (male and female) (Table 6). The presence of angina was found to be significantly (p < 0.05) greater in the male hypertensive population than in the female hypertensive population.
Discussion
The results of the present study revealed that unadjusted sleep efficiency, sleep time, ADBP, and age were significant predictors of Anginan in hypertensive individuals. When all covariates (age, BMI, alcohol use, ADBP, ASBP, cigarette smoking, sleep time, sleep N3, and sleep efficiency) were adjusted, then only ADBP and ASBP were found to be significant predictors of Anginan. Adjusted covariates were found to be responsible for only 2.3% of the variance in Anginan. This indicates that there will be several factors other than the above-mentioned covariates that can predict more variation in the Anginan. The present study aimed to know the association of sleep time and sleep efficiency with Anginan, which has not been found when sleep time and efficiency were adjusted to other covariates. Therefore, in the present study, hypertension played a major role in predicting the Anginan rather than sleep time and efficiency.
Previous epidemiological studies have shown that impaired sleep patterns like long and short sleep duration are related to several cardiometabolic impairments such as hypertension, diabetes, obesity, hypercholesterolemia, stroke, and myocardial infarction26,27.
In the present study, it should be noted that the mean sleep efficiency was 48.33%, which is quite low. Several factors could be responsible for low sleep efficiencies, such as participants belonging to the older age group (mean age 72.03 years), the presence of hypertension, and other cardiovascular diseases in the study cohort. A study performed by Didikoglu et al. showed a relationship between old age and reduced sleep efficiency. They reported an 18.6% decrease in sleep efficiency in older adults between the age of 40 and 100 years28.
Sleep duration is associated with cardiovascular risks29, and in particular, with an increased risk of myocardial infarction30 and it is the combination of poor sleep quality and short sleep duration that causes maximum risks31. A study by Buxton and Marcelli32 reported that both short and long durations of sleep were predictors of cardiovascular disease.
Reduced sleep duration has been reported to result in a general increase in inflammatory markers, reduced variability in heart rate, increased BP, disrupted hypothalamic axis, glucose intolerance, hyper-activation of the sympathetic nervous system, and increased cortisol levels33,34,35,36,37. Other studies found that the risk of obesity and weight gain is more in individuals with poor sleep quality or short sleep duration38,39. However, no study in our knowledge reported the effects of sleep duration and efficiency on angina in hypertensive individuals. Therefore, the comparison of the findings of the present study with other studies is difficult.
However, a systemic review and meta-analysis performed by Cappuccio et al. found that sleep of short duration was not associated with an increased risk of developing cardiovascular diseases or dying from it however they reported that sleep of long duration was associated with an increased risk of developing cardiovascular disease or dying from it40. The reason for the association of long duration of sleep with CVD could be because other factors such as subclinical diseases, physical inactivity, low socioeconomic status, and depression are associated with long duration of sleep and thus may confound the associations of long duration of sleep with CVD41,42. Thus long sleep durations may even be the consequence of comorbidities40,41.
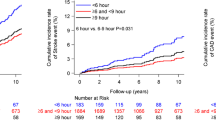
The findings of the present study are also supported by the study of Qureshi et al.43 which reported that sleep durations of fewer than 6 h and more than 8 h were not associated with an increased risk of coronary artery disease.
The results of the present study indicated that the presence of angina is greater in men compared to women. According to the study by Maas et al.44, women develop cardiovascular diseases 7–10 years later than men. Before menopause, women have a low coronary heart disease event rate45. The reason for this may be that women have premenopausal protection against ischemic heart diseases46. Endogenous estrogen hormone released before menopause is assumed to delay the manifestation of atherosclerotic diseases in women44. Similar findings were reported by Hemingway et al. who reported that the age-standardized annual incidence per 100 population of all cases of angina was higher in men than in women47. Additionally, a study by Murphy et al. reported that angina is more common in men than in women48.
The present study revealed that, when unadjusted, age is a significant predictor of Anginan and was responsible for 0.9% variance. Age was also found to have a significant positive correlation, although small (r = 0.097), with Anginan. But when adjusted for other covariates, no significant impact of age was found on Anginan. However contrary findings were reported by the study of Fisher et al., which reported that older people were more likely to have angina and more severe symptoms when compared with people with a similar extent of disease49. They reported that age is an independent and significant predictor of the presence and severity of angina, even after adjusting for covariates. Several factors may explain the association of aging with the presence of angina, such as deconditioning due to a sedentary lifestyle, physiological factors related to aging, and the disease process49.
An interesting finding from the present study is that no association was found between the number of cigarette packs used in a year and Anginan. Similar findings were reported by Pujades-Rodriguez50 who reported no differences in lifetime risks for stable angina according to the smoking status. However, a study by Merry et al.51 reported that smoking increased the risk of unstable angina. Also, the study by Wilmink et al.52 found a relative risk of 1.3 for angina for current smokers compared to non-smokers.
This study used gold standard measurements for sleep parameters and cardiovascular health. However, some limitations are needed to be mentioned for future studies. Cardiovascular medication adherence was not controlled, which has an impact on BP and cardiovascular health. Depression and anxiety symptoms increase during aging which has an impact on overall sleep quality. Future studies are needed to assess the impact of sleep on cardiovascular health with controlled psychological symptoms. Future studies should control extraneous variables like physical activity and sedentary lifestyle because they affect cardiovascular health.
Conclusion
In hypertensive individuals, sleep time and sleep efficiency did not affect Anginan when adjusted for covariates. Average diastolic and systolic BP were found to be significant predictors of Anginan when covariates were adjusted.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due but are available from the corresponding author on reasonable request.
Abbreviations
- Anginan :
-
Number of angina episodes
- BMI:
-
Body mass index
- REM:
-
Rapid eye movement
- NREM:
-
Non-rapid eye movement
- BP:
-
Blood pressure
- ADBP:
-
Average diastolic blood pressure
- ASBP:
-
Average systolic blood pressure
- SHHS:
-
Sleep heart health study
References
Altevogt, B. M. & Colten, H. R. Sleep disorders and sleep deprivation: an unmet public health problem. (2006).
Parish, J. M. & Shepard, J. W. Jr. Cardiovascular effects of sleep disorders. Chest 97, 1220–1226 (1990).
Coccagna, G., Mantovani, M., Brignani, F., Manzini, A. & Lugaresi, E. Arterial pressure changes during spontaneous sleep in man. Electroencephalogr. Clin. Neurophysiol. 31, 277–281 (1971).
Khatri, I. M. & Freis, E. D. Hemodynamic changes during sleep. J. Appl. Physiol. 22, 867–873 (1967).
Bristow, J., Honour, A., Pickering, T. & Sleight, P. Cardiovascular and respiratory changes during sleep in normal and hypertensive subjects. Cardiovasc. Res. 3, 476–485 (1969).
Miller, J. & Horvath, S. Cordioc output during humon sleep. Nature 73, 2455 (1976).
Koyanagi, A. & Stickley, A. The association between sleep problems and psychotic symptoms in the general population: A global perspective. Sleep 38, 1875–1885 (2015).
Léger, D., Poursain, B., Neubauer, D. & Uchiyama, M. An international survey of sleeping problems in the general population. Curr. Med. Res. Opin. 24, 307–317 (2008).
Stranges, S., Tigbe, W., Gómez-Olivé, F. X., Thorogood, M. & Kandala, N.-B. Sleep problems: An emerging global epidemic? Findings from the INDEPTH WHO-SAGE study among more than 40,000 older adults from 8 countries across Africa and Asia. Sleep 35, 1173–1181 (2012).
Lemma, S. et al. The epidemiology of sleep quality, sleep patterns, consumption of caffeinated beverages, and khat use among ethiopian college students. Sleep Disord. 2012, 11 https://doi.org/10.1155/2012/583510 (2012).
Lie, I., Arnesen, H., Sandvik, L., Hamilton, G. & Bunch, E. H. Predictors for physical and mental health 6 months after coronary artery bypass grafting a cohort study. Eur. J. Cardiovasc. Nurs. 9, 238–243 (2010).
Redeker, N. S., Ruggiero, J. & Hedges, C. Patterns and predictors of sleep pattern disturbance after cardiac surgery. Res. Nurs. Health 27, 217–224 (2004).
Redeker, N. S., Ruggiero, J. S. & Hedges, C. Sleep is related to physical function and emotional well-being after cardiac surgery. Nurs. Res. 53, 154–162 (2004).
Chaput, J. P., Després, J. P., Bouchard, C. & Tremblay, A. Short sleep duration is associated with reduced leptin levels and increased adiposity: Results from the Quebec family study. Obesity 15, 253–261 (2007).
Forquer, L. M., Camden, A. E., Gabriau, K. M. & Johnson, C. M. Sleep patterns of college students at a public university. J. Am. Coll. Health 56, 563–565 (2008).
Knutson, K. L. et al. Association between sleep and blood pressure in midlife: The CARDIA sleep study. Arch. Intern. Med. 169, 1055–1061 (2009).
Koren, D., Arnon, I., Lavie, P. & Klein, E. Sleep complaints as early predictors of posttraumatic stress disorder: A 1-year prospective study of injured survivors of motor vehicle accidents. Am. J. Psychiatry 159, 855–857 (2002).
Kripke, D. F., Garfinkel, L., Wingard, D. L., Klauber, M. R. & Marler, M. R. Mortality associated with sleep duration and insomnia. Arch. Gen. Psychiatry 59, 131–136 (2002).
Meerlo, P., Sgoifo, A. & Suchecki, D. Restricted and disrupted sleep: effects on autonomic function, neuroendocrine stress systems and stress responsivity. Sleep Med. Rev. 12, 197–210 (2008).
Asplund, R. Sleep and cardiac diseases amongst elderly people. J. Intern. Med. 236, 65–71 (1994).
Quan, S. F. et al. The sleep heart health study: Design, rationale, and methods. Sleep 20, 1077–1085 (1997).
H. Rapoport David M. Smith Philip L. Kiley James P., S. H. H. R. G. R. S. s. p. c. e. S. M. H. L. B. K. Q. S. F. I. C. G. D. J. B. W. Methods for obtaining and analyzing unattended polysomnography data for a multicenter study. Sleep 21, 759–767 (1998).
Group, S. H. H. S. R. Sleep Heart Health Study Manual of Operation (SHHS Coordinating Center, 1996).
Nieto, F. J. et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. JAMA 283, 1829–1836 (2000).
Carskadon, M. A. & Dement, W. C. Normal human sleep: An overview. Princ. Pract. Sleep Med. 4, 13–23 (2005).
Grandner, M. A., Jackson, N. J., Pak, V. M. & Gehrman, P. R. Sleep disturbance is associated with cardiovascular and metabolic disorders. J. Sleep Res. 21, 427–433 (2012).
Gangwisch, J. Epidemiological evidence for the links between sleep, circadian rhythms and metabolism. Obes. Rev. 10, 37–45 (2009).
Didikoglu, A. et al. Longitudinal sleep efficiency in the elderly and its association with health. J. Sleep Res. 29, e12898 (2020).
Grandner, M. A., Patel, N. P., Gehrman, P. R., Perlis, M. L. & Pack, A. I. Problems associated with short sleep: Bridging the gap between laboratory and epidemiological studies. Sleep Med. Rev. 14, 239–247 (2010).
Sabanayagam, C. & Shankar, A. Sleep duration and cardiovascular disease: Results from the National Health Interview Survey. Sleep 33, 1037–1042 (2010).
Chandola, T., Ferrie, J. E., Perski, A., Akbaraly, T. & Marmot, M. G. The effect of short sleep duration on coronary heart disease risk is greatest among those with sleep disturbance: A prospective study from the Whitehall II cohort. Sleep 33, 739–744 (2010).
Buxton, O. M. & Marcelli, E. Short and long sleep are positively associated with obesity, diabetes, hypertension, and cardiovascular disease among adults in the United States. Soc. Sci. Med. 71, 1027–1036 (2010).
Tochikubo, O., Ikeda, A., Miyajima, E. & Ishii, M. Effects of insufficient sleep on blood pressure monitored by a new multibiomedical recorder. Hypertension 27, 1318–1324 (1996).
Spiegel, K., Leproult, R. & Van Cauter, E. Impact of sleep debt on metabolic and endocrine function. Lancet 354, 1435–1439 (1999).
Kato, M. et al. Effects of sleep deprivation on neural circulatory control. Hypertension 35, 1173–1175 (2000).
Meier-Ewert, H. K. et al. Effect of sleep loss on C-reactive protein, an inflammatory marker of cardiovascular risk. J. Am. Coll. Cardiol. 43, 678–683 (2004).
Shearer, W. T. et al. Soluble TNF-α receptor 1 and IL-6 plasma levels in humans subjected to the sleep deprivation model of spaceflight. J. Allergy Clin. Immunol. 107, 165–170 (2001).
Magee, C. A., Caputi, P. & Iverson, D. C. Short sleep mediates the association between long work hours and increased body mass index. J. Behav. Med. 34, 83–91 (2011).
Watanabe, M., Kikuchi, H., Tanaka, K. & Takahashi, M. Association of short sleep duration with weight gain and obesity at 1-year follow-up: A large-scale prospective study. Sleep 33, 161–167 (2010).
Cappuccio, F. P., Cooper, D., D’Elia, L., Strazzullo, P. & Miller, M. A. Sleep duration predicts cardiovascular outcomes: A systematic review and meta-analysis of prospective studies. Eur. Heart J. 32, 1484–1492 (2011).
Stranges, S. et al. Correlates of short and long sleep duration: A cross-cultural comparison between the United Kingdom and the United States: The Whitehall II Study and the Western New York Health Study. Am. J. Epidemiol. 168, 1353–1364 (2008).
Krueger, P. M. & Friedman, E. M. Sleep duration in the United States: A cross-sectional population-based study. Am. J. Epidemiol. 169, 1052–1063 (2009).
Qureshi, A. I., Giles, W. H., Croft, J. B. & Bliwise, D. L. Habitual sleep patterns and risk for stroke and coronary heart disease: A 10-year follow-up from NHANES I. Neurology 48, 904–910 (1997).
Maas, A. H. & Appelman, Y. E. Gender differences in coronary heart disease. Neth. Heart. J. 18, 598–603 (2010).
Prescott, E., Hippe, M., Schnohr, P., Hein, H. O. & Vestbo, J. Smoking and risk of myocardial infarction in women and men: Longitudinal population study. BMJ 316, 1043 (1998).
Kones, R. Recent advances in the management of chronic stable angina I: Approach to the patient, diagnosis, pathophysiology, risk stratification, and gender disparities. Vasc. Health Risk Manag. 6, 635 (2010).
Hemingway, H. et al. Incidence and prognostic implications of stable angina pectoris among women and men. JAMA 295, 1404–1411 (2006).
Murphy, N. F. et al. Prevalence, incidence, primary care burden and medical treatment of angina in Scotland: Age, sex and socioeconomic disparities: A population-based study. Heart 92, 1047–1054 (2006).
Fisher, L. D., Maynard, C., Rademaker, A. W., Alderman, E. L. & Mock, M. Age variation in the association between angiographic coronary disease and angina from the Coronary Artery Surgery Study (CASS). Int. J. Cardiol. 24, 317–326 (1989).
Pujades-Rodriguez, M. et al. Heterogeneous associations between smoking and a wide range of initial presentations of cardiovascular disease in 1 937 360 people in England: lifetime risks and implications for risk prediction. Int. J. Epidemiol. 44, 129–141 (2015).
Merry, A. H. et al. Smoking, alcohol consumption, physical activity, and family history and the risks of acute myocardial infarction and unstable angina pectoris: A prospective cohort study. BMC Cardiovasc. Disord. 11, 1–14 (2011).
Wilmink, T. B., Quick, C. R. & Day, N. E. The association between cigarette smoking and abdominal aortic aneurysms. J. Vasc. Surg. 30, 1099–1105 (1999).
Acknowledgements
The authors are grateful to the Researchers Supporting Project number (RSP-2021/382), King Saud University, Riyadh, Saudi Arabia for funding this research. This work was supported by National Heart, Lung and Blood Institute cooperative agreements U01HL53940 (University of Washington), U01HL53941 (Boston University), U01HL53938 (University of Arizona), U01HL53916 (University of California, Davis), U01HL53934 (University of Minnesota), U01HL53931 (New York University), U01HL53937 and U01HL64360 (Johns Hopkins University), U01HL63463 (Case Western Reserve University), and U01HL63429 (Missouri Breaks Research). The opinions expressed in this paper are those of the authors and do not necessarily reflect the views of the Indian Health Service. SHHS acknowledges the Atherosclerosis Risk in Communities Study, the Cardiovascular Health Study, the Framingham Heart Study, the Cornell/Mt. Sinai Worksite and Hypertension Studies, the SHHS, the Tucson Epidemiologic Study of Airways Obstructive Diseases, and the Tucson Health and Environment Study for allowing their cohort members to be part of the SHHS and for permitting data acquired by them to be used in the study. SHHS is particularly grateful to the members of these cohorts who agreed to participate in SHHS as well. SHHS further recognizes all of the investigators and staff who have contributed to its success. A list of SHHS investigators, staff, and their participating institutions is available on the SHHS website, http://iws1.jhsph.edu/Research/Centers/CCT/shhs/.
Funding
Researchers Supporting Project number (RSP-2021/382), King Saud University, Riyadh, Saudi Arabia.
Author information
Authors and Affiliations
Contributions
A.H.A., M.K., M.M.A., A.S.A., and M.A. conceptualized the study and its methodology. A.H.A. and M.M.A. were involved in supervision. M.K., A.S.A., and M.M.A. did data analysis and interpretation. M.K. and M.A. wrote, reviewed, and edited the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alghadir, A.H., Khan, M., Alshehri, M.M. et al. In hypertensive individuals, sleep time and sleep efficiency did not affect the number of angina episodes: a cross-sectional study. Sci Rep 12, 16290 (2022). https://doi.org/10.1038/s41598-022-20255-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-20255-y
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
