
Abstract
Surgical process modelling is an innovative approach that aims to simplify the challenges involved in improving surgeries through quantitative analysis of a well-established model of surgical activities. In this paper, surgical process model strategies are applied for the analysis of different Minimally Invasive Liver Treatments (MILTs), including ablation and surgical resection of the liver lesions. Moreover, a generic surgical process model for these differences in MILTs is introduced. The generic surgical process model was established at three different granularity levels. The generic process model, encompassing thirteen phases, was verified against videos of MILT procedures and interviews with surgeons. The established model covers all the surgical and interventional activities and the connections between them and provides a foundation for extensive quantitative analysis and simulations of MILT procedures for improving computer-assisted surgery systems, surgeon training and evaluation, surgeon guidance and planning systems and evaluation of new technologies.
Similar content being viewed by others

Introduction
For many years, surgery has been considered an art, treating surgery as an artist-driven process. This agrees with the fact that many of the processes during surgery are processed mentally inside the artist’s/surgeon’s brain. To better expose this process, expert consensus meetings, national and international guidelines provide generalized recommendations on a high abstraction level based on the pillars of evidence-based medicine. In recent years, with the introduction of new technologies, tools and hybrid operating rooms (ORs), surgeries became increasingly convoluted1. Improving these highly complex surgical procedures is a shared concern of experts with different backgrounds. However, without a solid knowledge of these treatment processes, they can hardly be improved2.
In surgical process modelling, surgeries are treated not as an artist-driven process but as a sequence of tasks and steps that are followed by the clinical team3, which can support analysis and predicting surgical actions. Analysis of surgical process models can reveal the bottlenecks and potential improvements to the surgeries, aiding further advances4,5,6,7,8,9. Such process models are a great means for finding the structural coherence of complex surgical procedures and for obtaining a profound qualitative and quantitative understanding of the relations within the surgical procedure, its variation parameters and its output parameters10,11,12,13. Hence, these are great tools for training surgical teams and educating young surgeons.
Minimally Invasive Liver Treatment (MILT) is an example of a procedure were different clinicians use different methods and techniques to treat liver lesions through surgical/interventional liver manipulations when non-surgical methods (non-invasive and chemotherapy treatments) are not adequate. After the introduction in the previous century, minimally invasive approach for liver surgery has only in recent years changed the way how benign and malignant lesions are treated14,15. Although the less invasive nature of MILT compared to open surgeries benefits the patient16,17, various challenges that can increase the risk of surgical errors remain, including inadequate visualization of the patient’s internal structure, lack of tactile feedback and complex navigation towards target treatment lesions18,19. Moreover, the continuous change of the liver shape and location due to, e.g., pneumoperitoneum, patient respiration and manipulation of the liver during an intervention, add to these challenges1. Over the last three decades, a broad range of MILT techniques has been introduced. These techniques can be categorized into three methods: laparoscopic liver resection (LLR)20,21,22,23,24, laparoscopic liver ablation (LLA)25,26,27,28,29 and percutaneous ablation (PA)30,31,32,33,34 and robot-assisted resection35. This paper focuses on the first three categories. As a result, different surgeons and interventionists use different methods and techniques, which can all be executed with large process variations. Furthermore, procedures are further dependent on factors such as:
-
medical team skills, experience and preferences
-
patient-specific properties, such as patient’s body topography, patient health condition and clinical history
-
type, size, and location of the treatment areas.
These all add to the inherent complexity of MILT procedures. A detailed generic process model of MILT is crucial for assessing these complexities, educating new surgeons and improving MILT procedures. Yet, to the best of our knowledge, such model has not yet been established. The sole study available on modeling the MILT process is a qualitative study describing radiofrequency percutaneous ablation36. Therefore, the aim of this study is to establish a generic surgical process model (or surgical workflow) of MILT that covers the entire procedure for a variety of MILT methods and their corresponding techniques. The proposed generic process model provides the relation between entities and allows quantitative and qualitative studies of surgical procedure. The process model was developed in a modular way to increase its usability and efficiency and to facilitate aspects of data acquisition, analysis and procedure improvement10,37,38,39.
Methods
This study focuses on three commonly distinguished MILT methods. Within each method several variations, referred to as types, can be distinguished:
-
Laparoscopic Liver Resection (LLR): Resecting the necessary region of the liver parenchyma using the minimally invasive approach. Depending on the size and location of the resection region, three types of operations can be applied: formal resection40,41, anatomical resection42,43,44 and atypical resection, also known as parenchyma sparing45,46,47.
-
Laparoscopic Liver Ablation (LLA): Laparoscopic ablation of the tumor by placing one or several needles inside or around the target lesion, aiming to destroy target cells by means of burning, electrifying, freezing, or chemicals. The clinician manipulates the internal structures through small incisions to make the treatment region accessible and to ensure that the treatment is performed on the right location. LLA has four different types: Radiofrequency Ablation (RFA)32,33,34,48, Microwave Ablation (MWA)48,49,50,51, Irreversible Electroporation (IRE)52, Cryoablation (CA)53,54,55 and Ethanol Injection (EI)56,57,58.
-
Percutaneous Ablation (PA): Similar to LLA, but without laparoscopic manipulations and ablation needles are inserted directly through the skin into the treatment area. PA has the same treatment types as LLA.
Modeling strategies
To establish a generic process model of MILT, the modeling strategies proposed in our previous work10 were applied as described below.
Granularity level
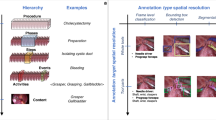
The generic process model of MILT was established at three levels of abstraction and granularity, see Fig. 1:
-
Procedure Considering the entire procedure as a single process, starting from patient intake until the end of the intervention. Highest abstraction level, lowest granularity.
-
Phase (P) Contains groups of modules and decisions that all share a goal or purpose. Intermediate abstraction level, intermediate granularity.
-
Module (M) A chain of actions and decisions aiming to fulfil a specific goal within a phase. Low abstraction level, high granularity.

Different levels of granularity embodied in the developed surgical process model.
Data acquisition method
Model design data
Data of the MILT procedures were collected through live observations and offline video observations, literature study and interviews.
The data were acquired from:
-
Sixteen live observations at Oslo University Hospital (OUH), Oslo, Norway and Erasmus Medical Center, Rotterdam, Netherlands (Erasmus MC), performed by experienced teams. The live observations were composed of twelve laparoscopic and four ablation treatments.
-
Eight interviews with clinical experts at Erasmus MC and OUH.
-
Nine offline observations using endoscopic video recordings of laparoscopic liver surgeries and OR recordings of ablation procedures.
The process model was primarily designed based on the live observations in the OR. Interviews with the surgical team members were conducted to verify that the observed procedures were representative for MILT methods in general. To obtain a thorough understanding of surgical methods and to let the teams get used to the observer, the observer also attended several laparoscopic resection procedures of other organs in the aforementioned hospitals. Furthermore, the procedure description of MILT procedures in Refs.19,24,34,40,56,58,59,60,61,62,63,64,65 has been investigated.
Model verification data
After establishing the MILT process model, endoscopic video recordings of laparoscopic liver surgeries of fifteen extra procedures were used for verification. In addition, the author (MG) has attended six intervention sessions in Erasmus MC and Bern University Hospital (BUH).
For final verification, the proposed process model the process model was presented to clinicians and the validity and correctness of the generic process model for different techniques of performing MILT were discussed with the participating clinicians in OUH and Erasmus MC. Example surgical videos were used to discuss how the process model mimics every activities in performing different technics of MILT in clinical practice. Video Marker Software was used to discuss the registered surgical data for the entire duration of sample surgeries over the endoscopic videos.
Ethical approval was obtained from each of the clinical centers in which the data were collected and observations were done for design and verification of the process model (OUH: Regional Ethical Committee of South Eastern Norway- REK Sør-Øst B 2011/1285 and the Data Protection Officer of OUH) and Erasmus MC and BUH with following the hospitals ethical rules). Based on these hospitals rules, informed consents were obtained from patients for further investigation on their surgical procedure. All methods for data acquisition and verification were performed in accordance with the relevant guidelines and regulations of the hospitals.
Modelling approach
A combination of top-down and bottom-up approaches was used to benefit from the advantages of both approaches (see10). Based on the data from OR observations, interviews and literature studies, a top-down approach was first used to establish a global overview of the surgical workflow. Next, the endoscopic videos were used as low-level data to model the details of the process model and to improve the initially established general overview bottom-up. This modelling process was iterated until no process model changes resulted from new iterations anymore.
Generalization
Generalization of the MILT process model to LLR, LLA, PA and their different types and techniques should ensure agreement with divergences and differences of the MILT procedures in clinical practice. Therefore, the data for analysis and modelling was acquired in procedures using various MILT types and techniques, with a variety of patient conditions (age, gender, build, clinical history, tumour specification and number, etc.). The individual procedures were merged in the generalization process, covering all events of the treatments and not only the most probable events.
Model representation
The generic MILT process model was concretized by using workflow and process model diagrams. The process model was made to have a modular structure to increase model usability and efficiency10.
Verification
Qualitative and quantitative verifications were done to confirm that the proposed generic process model of MILT reflects the procedure in clinical practice:
-
Qualitative verification was performed to confirm that the path options in the established process model fit any observed order of possible actions and decisions occurring during MILT in clinical practice. This was done by registering the sequence of the encountered process model elements (phases and modules) throughout the entire treatment procedure of fifteen offline observation of MILT procedures from OUH. In addition, the author (MG) has attended four intervention sessions at Bern University Hospital and two at Erasmus MC. Furthermore, interviews with clinical teams were done and the process model was discussed with highly experienced surgeons with at least 10 years of surgical experience in OUH and Erasmus MC.
-
Quantitative verification was performed to confirm that the sum of the encountered workflow elements (phases, modules) duration was equivalent to the total procedure times of fifteen offline MILT procedures from OUH.
As each treatment procedure can be composed of thousands of steps, in-house process model data registration software was developed to facilitate registration of data on the videos of the endoscopic camera (Fig. 2).

A snapshot of the developed process model data registration software (DOI: https://doi.org/10.4121/20163926). The software comprises three main sections: (a) endoscopic video player, (b) data registration panel to register data at the desired granularity level, locally or in the data-base and (c) registered data management.
Results
Workflow phases
Within the MILT treatment procedure, including its preparations, three hierarchical sub-phases are distinguished clinically:
-
Operation: the entire process in the OR, from when OR and patient are being prepared, until when the patient is moved out of the OR to the recovery room.
-
Intervention: starts with the first ablation needle manipulation or first incision in the abdomen by the interventionist/surgeon and ends when the last incision is closed.
-
Surgery: starts with the first incision in the abdomen by the surgeon and ends when the last incision has been closed.
-
Treatment: the actual physical treatment (resection or ablation) of the target region.
The generic process model of MILT procedures at the lowest granularity level (highest abstraction) is displayed in Fig. 3, showing all phases. The individual phases are explained below:

Generic process model of MILT at the phase level. Most of the phases are colored blue with solid-line rectangles; these phases are common between ablation and resection procedures. The gray phase, “needle manipulation”, is designated only for the ablation procedures. The blue and gray phases are connected by black solid and red dashed arrows showing the flow of activities. The black solid arrows are common between ablation and resection procedures, whereas the red dashed arrows are only used for ablation procedures. The green dashed rectangles show the phases that can happen anytime during the operation. These phases are connected to all other phases, but for the sake of readability, these arrows were left out of the figure. The black dotted-dashed arrows show the transfer of data such as medical images and patient medical history.
Phase 01: Intake—The patient is admitted to the hospital and complete anamnesis is collected.
Phase 02: re-operative Imaging—Medical images of the abdominal region are made for planning the MILT procedure prior to a possible operation. Phase 02 can take place right before operation up to a few months prior.
Phase 03: Pre-operative Planning—Planning includes all decisions about things like treatment approach, incision locations and resection paths or possible needle placements, size of the target region, etc. prior to the possible operation. The planning is based on the patient anamnesis (from Phase 01), medical images (from Phase 02), available equipment and technical resources and experiences.
Phase 04: Intra-operative Preparation—On the day of operation, prior to the intervention, the patient, OR equipment and surgical instruments are prepared for the operation.
Phase 05: Intra-operative Imaging—Medical images can be acquired in the OR, before and during the intervention.
Phase 06: Intra-operative Planning—The treatment plan can be generated or updated in the OR just before and during the intervention. Any pre-operative data and new images were taken in the OR (from Phase 05) aid in making decisions in this phase. The MILT method and type might also be changed during the operation. The MILT procedure is considered aborted if it is converted to a non-MILT procedure, such as open surgery.
Phase 07: Operative field Access—If LLR or LLA is the preferred method, the surgeon first makes the operative field accessible.
Phase 08a/b: Isolation of the treatment area consists of activities to separate the target region from surrounding structures and prepares the target region for the treatment. Based on the nature of these activities and how they affect the patient’s anatomy, isolation can be performed in two ways:
Phase 08a: Treatment Area Isolation: Destructive—Isolation by destructive (permanent) dissection or closure of surrounding structures. Only applies to LLR and LLA.
Phase 08b: Treatment Area Isolation: Non-destructive—Isolation with temporary effects, using actions such as temporarily closure of vessels or hydro dissection.
Phase 09: Needle Manipulation—Maneuvering ablation needle(s) to the desired position.
Phase 10: Treatment—The actual treatment of the target region by either resection or ablation.
Phase 11: Intra-operative Complications—Handling any complications that might occur during the operation. Such actions may include, for example, blood transfusion and hemostasis (e.g. bleeding vessel ligation) or surgical drainage.
Phase 12: Miscellaneous—Other clinical activities that do not directly serve the MILT procedure might take place, such as biopsy and catheter placement.
Phase 13: Intra-operative Wrap-up—All activities aimed at wrapping up, such as removal of un-absorbable materials, closing the incisions, etc.
The generic process model of MILT procedures at the module level, including the phases, modules and decisions linking the modules, is provided in Fig. 4 (DOI:https://doi.org/10.4121/20163968). A legend explaining the different symbols used in Figs. 3 and 4 is provided in Fig. 5. All activities in the entire procedure of MILT including sequential and parallel activities are covered in the presented generic process model. Parallel activities are represented using  symbols. Apart from the continuous support of nurses and anaesthesiologist in the entire intra-operative phases and the act of blood suctioning in parallel to other treatment activities during surgery, based on the current data, the parallel activities are associated with two phases: intra-operative preparation phase (Phase 4) and intra-operative imaging (Phase 2) activities. In intra-operative phases, we plotted the connections associated with the imaging phase, where there was a high chance of performing imaging routines. In other places where this is less likely to happen, we used a symbol
symbols. Apart from the continuous support of nurses and anaesthesiologist in the entire intra-operative phases and the act of blood suctioning in parallel to other treatment activities during surgery, based on the current data, the parallel activities are associated with two phases: intra-operative preparation phase (Phase 4) and intra-operative imaging (Phase 2) activities. In intra-operative phases, we plotted the connections associated with the imaging phase, where there was a high chance of performing imaging routines. In other places where this is less likely to happen, we used a symbol  to show the possibility for imaging. A brief walkthrough of the module-level MILT process model including the contents of the modules in the process model is provided in Supplementary material-part S1. A brief description of the Modules is provided in Table 1.
to show the possibility for imaging. A brief walkthrough of the module-level MILT process model including the contents of the modules in the process model is provided in Supplementary material-part S1. A brief description of the Modules is provided in Table 1.

Generic process model for MILT procedures at the module granularity level. See Fig. 5 for explanation of the used symbols and line styles. DOI: https://doi.org/10.4121/20163968.

Model verification
The result of the quantitative and qualitative verifications of the process model confirmed that the process model provides a pathway for all encountered sequences of actions and decisions that were observed to occur during MILT procedures in clinical practice. Supplementary material-part S2 lists all the registered sequence of actions and decisions in the entire duration of endoscopic videos from different surgical procedures for parenchyma sparing of a tumor located in Segments 5&6, 7&8 and 5, performed in OUH. Durations of all entities in the procedure are presented in the Supplementary material-part S2. Table 2 shows the duration and occurrence frequencies of every action extracted from the endoscopic video on which the Supplementary material-part S2 data is based, at the module as well as the phase granularity level. Figure 6 provides a process model view at the phase level for duration and occurrence frequency of different phases for the typical example of a surgical procedure. Note that during the entire course of a surgery, some timings are out of the view of endoscopic camera or associated with activities other than surgical actions, e.g. the surgeon might need to take out the camera and clean it. The timing of such activities are also extracted and labeled as Idle. Phases 1 to 3 are pre-operative phases and are not captured by the endoscopic videos. These pre-operative phases were verified through attendance to pre-operative imaging and planning sessions and discussions with clinical teams. The result of the verification process shows that there were no activities in any of the observed MILT procedures that were not covered by the proposed process model.

Generic surgical process model view at the phase level for duration and occurrence frequency of different phases for a sample surgery presented in Supplementary material-part S2 (type: parenchyma sparing of a tumor in Segments 5 and 6).
In sessions with two highly experienced surgeons and two assistant surgeons in OUH and Erasmus MC, discussing the validity and correctness of the generic process model for different techniques of performing MILT, it was confirmed that the proposed process model mimics the activities in the clinical practice.
Discussion
Surgical process models bring several advantages and pave the way for further improvement of operations. The presented generic process model covers a broad range of MILT procedures and associated techniques. No deviations from the proposed process model were found in the treatment procedures that were analysed in the verification process. The proposed process model provides relationships between different entities of MILT procedures at the proposed levels of details. Thus, the process model provides the possibility for extensive quantitative as well as qualitative analysis of the procedures at the desired level of detail.
In intra-operative phases, distinguishing between planning and other treatment activities is a complicated task. Planning during operation is an ongoing mental activity and can be considered as an element inside all intra-operative phases. Modelling planning activities in a separate phase in the generic process model provides the foundation for further analysis and improvement of planning. Recognizing the points where planning occurs in the surgical process model and deriving the sequential relationships between planning and other intra-operative activities, show how and to what extent planning is associated with different activities and reveals the possible bottlenecks of planning.
Imaging activities can occur at any moment in the intraoperative phases. Although imaging activities could be defined as a green phase in the proposed generic surgical process model, it was decided to model sequential and parallel dependencies between entities as it highly benefits further analysis of process model and performing possible simulations. Live observations and interviews with experts in two institutions (OUH and Erasmus MC) were performed to determine the low granularity level structure of the process model. The process model was initially established based on the data from endoscopic video analysis and live observations in aforementioned institutions. The data was complimented with literature studies and analysis of videos of procedures available on the web from different institutes (Institute of Medical Education of Novgorod State University in Russia and Unité Hepatobiliopancreatique in Strasbourg, France- Videos can be found at Dr Sergey Baydo (https://www.youtube.com/c/DrSergeyBaydo/videos) and Dr Riccardo Memeo (https://www.youtube.com/channel/UCdhB0tuE3EC_iNipn1A3ltg/videos) YouTube Channels.) to make the process model as generally applicable as possible. Moreover, in verification process, the endoscopic videos of fifteen additional surgeries performed in OUH were analysed and six live observations of MILT procedures were performed in Erasmus MC and BUH. For these reasons, process model should conform to the procedures in other institutions as well. In this study, we did not take videos from the OR. These recording would make further quantitative validation of the model possible, but also requires special ethical approval, since sensitive information is recorded. In an earlier study, we investigated the consequence of recording in the OR66. In this study the pre-operative and not the post-operative phase was included in the generic process model, because the former has a direct influence on performing the treatment, which is the focus of this work. All concepts associated with different techniques of MILT are defined and categorized as different phases and modules. Thus, we expect that variations of performing actions in different institutions by using different techniques/instrument, will hardly cause any deviations from the proposed process model. However, lack of instruments, equipment or knowledge might change the course of actions or introduce innovative ways to tackle problems (that might happen especially in underdeveloped countries), which may not be considered in the presented process model. Recognizing and registration of surgical activities are crucial for performing analysis on surgical procedures, generating and verifying surgical process models and training machine learning methods to develop AI systems for the future hybrid ORs67. The in-house developed Video Marker Software in this work aided efficient registration and verification of data over the endoscopic video. The extracted data using the Video Marker Software from surgical videos that are acquired from OUH has been presented in Supplementary material-part S2. The statistical analysis of the extracted data reveals the bottlenecks in different surgeries. Based on the analysis, the surgeons spent most of their time on the treatment phase (P10); approximately 25 min (40% of total surgery time), and almost 85% of the treatment phase duration was allocated to the resection. This result emphasises the importance of treatment phase on the total surgery duration. Development of automated workflow recognition systems that can (semi)automatically analyse the endoscopic videos with appropriate image processing and/or machine learning methods are currently under attention of researchers, especially for analysis of minimally invasive treatments68,69. Such systems can be of great use to aid gathering surgical data for different purposes of process model analysis and verifications67,70,71.
The presented process model aids different aims of analysis for improvement of surgeries/interventions in follow-up studies. Analysis of process models and providing connections between every entities of the surgical procedures, identify the points where AI and software/platform systems can be beneficial, predicts how big the benefits are and determines how these systems can be designed and developed to be employed in clinical practice, see e.g. Ref.4,72. Development phase of the desired technologies and tools for hybrid ORs can also benefit from analysis of such surgical process models. Nowadays, Agile methods (SCRUM, XP, etc.)73,74 are being widely used in the process of the development of technologies. These methods aid smooth adaptation to changing requirements throughout the development process by using iterative planning and feedbacks from developers and the end users73,75. With the process model and computer simulations, analysis of the effect of possible changes and their eligibility aids making right decisions and adaptations during the agile sessions.
The process model can widely contribute in the training and skill evaluation of surgeons76,77,78. The optimal treatment option for each surgery with specific conditions can be derived and novice surgeons can be trained based on the probable sequence of events and the possible deviations for each operation. The experienced surgeons can review the steps and possible deviations before or during an operation as a roadmap. For this purpose, real-time recognition of surgical steps over the endoscopic videos is required, a topic which has attracted wide attentions in recent years79,80. The process model benefits analysis of surgeons’ learning curves81,82. Durations and occurrence frequencies of surgical steps and deviations from nominal surgery paths can be used as criteria for learning curve analysis, as well as surgeons’ skills evaluations. In recent years navigation platforms for guiding surgeons in performing MILT attracted broad attention83,84,85,86,87,88. Analysis of the proposed surgical process model can reveal the optimal treatment options to guide surgical teams using navigation systems by suggesting/predicting next surgical steps and the time required for performing each surgical action5,13,89,90. Currently, prior to operation the lead surgeon/interventionist goes into the details of the patient’s organ-specific anatomy and mentally pre-visualizes the whole procedure and all its key steps. The complexities of such pre-operative planning activity, can be reduced by the process model which brings the possibility to propose the treatment options for individual procedures. Analysis of surgical process model can prevent extra costs of trial and error in the development phase of technologies and introduction of new technologies into clinical practice. With the process model, it is possible to provide scientific evidence for the possible enhancement of surgeries by the proposed technology for specific methods/types/techniques of performing surgeries. The effects and eligibility of any adjustment in the new technologies can be analysed on the surgical procedure, prior to actual implementation of technologies, resulting in a more efficient business model.
Conclusion
A generic surgical process model for MILT was established by applying the modelling strategies developed in prior work. The presented model covers MILT methods for laparoscopic liver resection, laparoscopic liver ablation and percutaneous ablation, with their types, techniques and variations as observed in data obtained from various sources. As the presented model was established using a numerical model representation, it can be used for extensive quantitative and qualitative analysis and improvement of MILT procedures through various ways, such as the introduction of new technologies in the OR, training of clinical teams, analysis of learning curves and skills evaluations, optimization of OR management and medical team activities in the OR.
Data availability
All data generated or analysed during this study are included in this published article and its supplementary information files. The datasets generated and/or analysed during the current study are also available in the DOI: https://doi.org/10.4121/20163968.
References
Kenngott, H. G. et al. Effects of laparoscopy, laparotomy, and respiratory phase on liver volume in a live porcine model for liver resection. Surg. Endosc. 35(12), 7049–7057 (2021).
Maier-Hein, L. et al. Surgical data science–from concepts toward clinical translation. Med. Image Anal. 76, 102306 (2022).
MacKenzie, C. L. et al. Hierarchical decomposition of laparoscopic surgery: A human factors approach to investigating the operating room environment. Minim. Invasive Ther. Allied Technol. 10(3), 121–127 (2001).
Loeve, A. J. et al. Workflow and intervention times of MR-guided focused ultrasound—Predicting the impact of new techniques. J. Biomed. Inform. 60, 38–48 (2016).
Franke, S., Meixensberger, J. & Neumuth, T. Intervention time prediction from surgical low-level tasks. J. Biomed. Inform. 46(1), 152–159 (2013).
Burgert, O. et al. Requirement specification for surgical simulation systems with surgical workflows. In 15th Annual Conference on Medicine Meets Virtual Reality, MMVR 2007 58–63 (IOS Press, 2007).
Ebrahimi, H., Yee, A. & Whyne, C. Surgical process analysis identifies lack of connectivity between sequential fluoroscopic 2D alignment as a critical impediment in femoral intramedullary nailing. Int. J. Comput. Assist. Radiol. Surg. 11(2), 297–305 (2016).
Neumann, J., et al., Perioperative workflow simulation and optimization in orthopedic surgery, in 1st International Workshop on OR 2.0 Context-Aware Operating Theaters, OR 2.0 2018, 5th International Workshop on Computer Assisted Robotic Endoscopy, CARE 2018, 7th International Workshop on Clinical Image-Based Procedures, CLIP 2018, and 1st International Workshop on Skin Image Analysis, ISIC 2018, held in conjunction with the 21st International Conference on Medical Imaging and Computer-Assisted Intervention, MICCAI 2018. 2018. p. 3–11.
Fernández-Gutiérrez, F. et al. Workflow optimisation for multimodal imaging procedures: A case of combined X-ray and MRI-guided TACE. Minim. Invasive Ther. Allied Technol. 26(1), 31–38 (2017).
Gholinejad, M., Loeve, A. J. & Dankelman, J. Surgical process modelling strategies: Which method to choose for determining workflow?. Minim. Invasive Ther. Allied Technol. 28(2), 91–104 (2019).
Neumuth, T. Surgical process modeling. Innov. Surg. Sci. 2(3), 123–137 (2020).
Lalys, F. & Jannin, P. Surgical process modelling: A review. Int. J. Comput. Assist. Radiol. Surg. 9(3), 495–511 (2014).
Forestier, G. et al. Finding discriminative and interpretable patterns in sequences of surgical activities. Artif. Intell. Med. 82, 11–19 (2017).
Gouda, B. et al. Minimally-invasive surgery for liver metastases. Minerva Chir. 70(6), 429–436 (2015).
Felli, E., Baumert, T. & Pessaux, P. Is minimally invasive true anatomical HCC resection a future way to improve results in bridge or salvage liver transplantation?. Clin. Res. Hepatol. Gastroenterol. 1, 1 (2020).
Kang, S. H. et al. Laparoscopic liver resection versus open liver resection for intrahepatic cholangiocarcinoma: 3-year outcomes of a cohort study with propensity score matching. Surg. Oncol. 33, 63–69 (2020).
Guerrini, G. P. et al. Laparoscopic versus open liver resection for intrahepatic cholangiocarcinoma: The first meta-analysis. Langenbecks Arch. Surg. 405(3), 265–275 (2020).
Aghayan, D. L. et al. Laparoscopic versus open liver resection in the posterosuperior segments: A sub-group analysis from the OSLO-COMET randomized controlled trial. HPB 21(11), 1485–1490 (2019).
Abbaszadeh-Kasbi, A., & Reza Keramati, M. An Invited Commentary on “Perioperative outcomes comparing laparoscopic with open repeat liver resection for post-hepatectomy recurrent liver cancer: A systematic review and meta-analysis” (Int J Surg 2020; Epub ahead of print): Laparoscopic versus Open Repeat Liver Resection for Recurrent Liver Cancer. Int. J. Surg. 78, 70 (2020).
Buell, J. F. et al. Laparoscopic liver resection. J. Am. Coll. Surg. 200(3), 472–480 (2005).
Mala, T. et al. Laparoscopic liver resection: Experience of 53 procedures at a single center. J. Hepatobiliary Pancreat. Surg. 12(4), 298–303 (2005).
Are, C., Fong, Y., & Geller, D.A. Laparoscopic liver resections, in Advances in Surgery. 2005, Academic Press Inc. p. 57–75.
Fretland, Å. A. et al. Open versus laparoscopic liver resection for colorectal liver metastases (the Oslo-CoMet study): Study protocol for a randomized controlled trial. Trials 16, 1 (2015).
Fretland, A. A. et al. Laparoscopic versus open resection for colorectal liver metastases. Ann. Surg. 267(2), 199–207 (2018).
Chopra, S. S. et al. Laparoscopic radiofrequency ablation of liver tumors: Comparison of MR guidance versus conventional laparoscopic ultrasound for needle positioning in a phantom model. Minim. Invasive Ther. Allied Technol. 20(4), 212–217 (2011).
Siperstein, A. et al. Laparoscopic radiofrequency ablation of primary and metastatic liver tumors: Technical considerations. Surg. Endosc. 14(4), 400–405 (2000).
Topal, B., Aerts, R. & Penninckx, F. Laparoscopic radiofrequency ablation of unresectable liver malignancies: Feasibility and clinical outcome. Surg. Laparosc. Endosc. Percutaneous Tech. 13(1), 11–15 (2003).
Alemi, F. et al. Laparoscopic treatment of liver tumours using a two-needle probe bipolar radiofrequency ablation device. HPB 13(9), 656–664 (2011).
Sheka, A. C. et al. Tumor lysis syndrome after laparoscopic microwave ablation of colorectal liver metastases. J. Gastrointest. Cancer 51(2), 631–635 (2020).
Lee, S. J. et al. Percutaneous radiofrequency ablation for metachronous hepatic metastases after curative resection of pancreatic adenocarcinoma. Korean J. Radiol. 21(3), 316–324 (2020).
Mertyna, P. et al. Thermal ablation: A comparison of thermal dose required for radiofrequency-, microwave-, and laser-induced coagulation in an ex vivo bovine liver model. Acad. Radiol. 16(12), 1539–1548 (2009).
Mulier, S. et al. Radiofrequency ablation with four electrodes as a building block for matrix radiofrequency ablation: Ex vivo liver experiments and finite element method modelling—Influence of electric and activation mode on coagulation size and geometry. Surg. Oncol. 33, 145–157 (2020).
Melekhina, O. et al. Percutaneous radiofrequency-assisted liver partition versus portal vein embolization before hepatectomy for perihilar cholangiocarcinoma. BJS Open 4(1), 101–108 (2020).
Schullian, P. et al. Simultaneous stereotactic radiofrequency ablation of multiple (≥ 4) liver tumors: Feasibility, safety, and efficacy. J. Vasc. Interv. Radiol. 31(6), 943–952 (2020).
Giulianotti, P. C. et al. Robotic liver surgery: Technical aspects and review of the literature. Hepatobiliary Surg. Nutr. 5(4), 311 (2016).
Liebmann, P., & Neumuth, T. Model driven design of workflow schemata for the operating room of the future. in 40th Jahrestagung der Gesellschaft fur Informatik e.V. (GI): Service Science - Neue Perspektiven fur die Informatik, INFORMATIK 2010. 2010. Leipzig.
Kiran Kumar, P. & Khanna, V. Modular views on software architecture systems. Int. J. Civ. Eng. Technol. 8(2), 503–510 (2017).
Vidal-Silva, C. L. et al. Looking for a modular software development methodology: Blending of feature-oriented programming and aspect-oriented programming JPI. Inf. Technol. 30(3), 95–104 (2019).
Wang, Y. M. & Liu, H. W. The modularity condition for overlap and grouping functions. Fuzzy Sets Syst. 372, 97–110 (2019).
Sheen, A. J., Jamdar, S. & Siriwardena, A. K. Laparoscopic hepatectomy for colorectal liver metastases: The current state of the art. Front. Oncol. 9, 1 (2019).
Cipriani, F. et al. Pure laparoscopic versus open hemihepatectomy: A critical assessment and realistic expectations—a propensity score-based analysis of right and left hemihepatectomies from nine European tertiary referral centers. J. Hepatobiliary Pancreat. Sci. 27(1), 3–15 (2020).
Kim, J. H. Laparoscopic anatomical segmentectomy using the transfissural Glissonean approach. Langenbecks Arch. Surg. 405(3), 365–372 (2020).
She, W. H. et al. Anatomical versus nonanatomical resection for colorectal liver metastasis. World J. Surg. 1, 1 (2020).
Qi, L. N. et al. Outcomes of anatomical versus non-anatomical resection for hepatocellular carcinoma according to circulating tumour-cell status. Ann. Med. 52(1–2), 21–31 (2020).
Kalil, J. A. et al. Laparoscopic parenchymal-sparing hepatectomy: The new maximally minimal invasive surgery of the liver—a systematic review and meta-analysis. J. Gastrointest. Surg. 23(4), 860–869 (2019).
Deng, G. et al. Parenchymal-sparing versus extended hepatectomy for colorectal liver metastases: A systematic review and meta-analysis. Cancer Med. 8(14), 6165–6175 (2019).
Aghayan, D. L. et al. Laparoscopic parenchyma-sparing liver resection for colorectal metastases. Radiol. Oncol. 52(1), 36–41 (2018).
da Costa, A. C. et al. Radiofrequency combined with immunomodulation for hepatocellular carcinoma: State of the art and innovations. World J. Gastroenterol. 26(17), 2040–2048 (2020).
Bressem, K. K. et al. Exploring patterns of dynamic size changes of lesions after hepatic microwave ablation in an in vivo porcine model. Sci. Rep. 10, 1 (2020).
Ajao, M. O. et al. Two-dimensional (2D) versus three-dimensional (3D) laparoscopy for vaginal cuff closure by surgeons-in-training: A randomized controlled trial. Surg. Endosc. 1, 1 (2019).
Aarts, B. M. et al. Percutaneous microwave ablation of histologically proven T1 renal cell carcinoma. Cardiovasc. Intervent. Radiol. 43(7), 1025–1033 (2020).
Zimmerman, A., Grand, D. & Charpentier, K. P. Irreversible electroporation of hepatocellular carcinoma: Patient selection and perspectives. J. Hepatocell. Carcinoma 4, 49 (2017).
Kim, D. K. et al. Percutaneous cryoablation in early stage hepatocellular carcinoma: Analysis of local tumor progression factors. Diagn. Interv. Radiol. 26(2), 111–117 (2020).
Cha, S. Y. et al. RF ablation versus cryoablation for small perivascular hepatocellular carcinoma: Propensity Score analyses of mid-term outcomes. Cardiovasc. Intervent. Radiol. 43(3), 434–444 (2020).
Mala, T. et al. Cryoablation of colorectal liver metastases: Minimally invasive tumour control. Scand. J. Gastroenterol. 39(6), 571–578 (2004).
Swierz, M. J. et al. Percutaneous ethanol injection for liver metastases. Cochrane Database Syst. Rev. 1, 2 (2020).
Chedid, M. F. et al. Transarterial embolization and percutaneous ethanol injection as an effective bridge therapy before liver transplantation for hepatitis c-related hepatocellular carcinoma. Gastroenterol. Res. Pract. 1, 1 (2016).
Riemsma, R. P. et al. Percutaneous ethanol injection for liver metastases. Cochrane Database Syst. Rev. 1(5), 1 (2013).
Fretland, Å. A. et al. Open versus laparoscopic liver resection for colorectal liver metastases (the Oslo-CoMet Study): Study protocol for a randomized controlled trial. Trials 16(1), 1–10 (2015).
Simon, C.J., D.E. Dupuy, and W.W. Mayo-Smith, Microwave ablation: principles and applications. Radiographics, 2005. 25(suppl_1): p. S69-S83.
Lencioni, R. & Crocetti, L. Image-guided thermal ablation of hepatocellular carcinoma. Crit. Rev. Oncol. Hematol. 66(3), 200–207 (2008).
Ryan, M. J. et al. Ablation techniques for primary and metastatic liver tumors. World J. Hepatol. 8(3), 191 (2016).
Glazer, D. I. et al. Percutaneous image-guided cryoablation of hepatic tumors: single-center experience with intermediate to long-term outcomes. AJR Am. J. Roentgenol. 209(6), 1381 (2017).
Spinczyk, D. et al. Supporting diagnostics and therapy planning for percutaneous ablation of liver and abdominal tumors and pre-clinical evaluation. Comput. Med. Imaging Graph. 78, 101664 (2019).
Troisi, R. I. et al. Risk factors and management of conversions to an open approach in laparoscopic liver resection: analysis of 265 consecutive cases. HPB 16(1), 75–82 (2014).
Henken, K. R. et al. Implications of the law on video recording in clinical practice. Surg. Endosc. 26(10), 2909–2916 (2012).
Lecuyer, G. et al. Assisted phase and step annotation for surgical videos. Int. J. Comput. Assist. Radiol. Surg. 15(4), 673–680 (2020).
Twinanda, A. P. et al. Endonet: A deep architecture for recognition tasks on laparoscopic videos. IEEE Trans. Med. Imaging 36(1), 86–97 (2016).
Garrow, C. R. et al. Machine learning for surgical phase recognition: A systematic review. Ann. Surg. 273(4), 684–693 (2021).
Dergachyova, O. et al. Automatic data-driven real-time segmentation and recognition of surgical workflow. Int. J. Comput. Assist. Radiol. Surg. 11(6), 1081–1089 (2016).
Loukas, C. Video content analysis of surgical procedures. Surg. Endosc. 32(2), 553–568 (2018).
Jannin, P. & Morandi, X. Surgical models for computer-assisted neurosurgery. Neuroimage 37(3), 783–791 (2007).
Ahmad, M.O., & Raulamo-Jurvanen, P. Scientific Collaboration, Citation and Topic Analysis of International Conference on Agile Software Development Papers, in 3rd International Conference on Lean and Agile Software Development, LASD 2019, and the 7th Conference on Multimedia, Interaction, Design and Innovation, MIDI 2019, A. Przybylek and M.E. Morales-Trujillo, Editors. 2020, Springer. p. 108–132.
Vallon, R. et al. Systematic literature review on agile practices in global software development. Inf. Softw. Technol. 96, 161–180 (2018).
Dingsoeyr, T., Falessi, D. & Power, K. Agile development at scale: The Next Frontier. IEEE Softw. 36(2), 30–38 (2019).
Uemura, M. et al. Procedural surgical skill assessment in laparoscopic training environments. Int. J. Comput. Assist. Radiol. Surg. 11(4), 543–552 (2016).
Nakawala, H., Ferrigno, G. & De Momi, E. Development of an intelligent surgical training system for Thoracentesis. Artif. Intell. Med. 84, 50–63 (2018).
Schumann, S., Bühligen, U. & Neumuth, T. Outcome quality assessment by surgical process compliance measures in laparoscopic surgery. Artif. Intell. Med. 63(2), 85–90 (2015).
Volkov, M., et al. Machine learning and coresets for automated real-time video segmentation of laparoscopic and robot-assisted surgery. in 2017 IEEE international conference on robotics and automation (ICRA). 2017. IEEE.
Padoy, N. Machine and deep learning for workflow recognition during surgery. Minim. Invasive Ther. Allied Technol. 28(2), 82–90 (2019).
Forestier, G. et al. Surgical motion analysis using discriminative interpretable patterns. Artif. Intell. Med. 91, 3–11 (2018).
Forestier, G. et al. Surgical skills: Can learning curves be computed from recordings of surgical activities?. Int. J. Comput. Assist. Radiol. Surg. 13(5), 629–636 (2018).
Palomar, R. et al. Surface reconstruction for planning and navigation of liver resections. Comput. Med. Imaging Graph. 53, 30–42 (2016).
Zachariadis, O. et al. Accelerating B-spline interpolation on GPUs: Application to medical image registration. Comput. Methods Prog. Biomed. 1, 193 (2020).
Riediger, C. et al. First application of intraoperative MRI of the liver during ALPPS procedure for colorectal liver metastases. Langenbecks Arch. Surg. 405(3), 373–379 (2020).
Sakata, K., Kijima, T. & Arai, O. Initial report: A novel intraoperative navigation system for laparoscopic liver resection using real-time virtual sonography. Sci. Rep. 10(1), 1 (2020).
Luo, H. et al. Augmented reality navigation for liver resection with a stereoscopic laparoscope. Comput. Methods Programs Biomed. 1, 187 (2020).
Pérez de Frutos, J. et al. Laboratory test of Single Landmark registration method for ultrasound-based navigation in laparoscopy using an open-source platform. Int. J. Comput. Assist. Radiol. Surg. 13(12), 1927–1936 (2018).
Forestier, G. et al. Automatic matching of surgeries to predict surgeons’ next actions. Artif. Intell. Med. 81, 3–11 (2017).
Dergachyova, O., Morandi, X. & Jannin, P. Knowledge transfer for surgical activity prediction. Int. J. Comput. Assist. Radiol. Surg. 13(9), 1409–1417 (2018).
Acknowledgements
This work is part of the HiPerNav project that received funding from the European Union’s Horizon 2020 Research and Innovation program under grant agreement No 722068.
Author information
Authors and Affiliations
Contributions
M.G.: conceptualization, methodology, software, data verification and validation, formal analysis, investigation, resources, data curation, writing—original draft, writing—review and editing, visualization, E.P.: data verification, resources, writing-review and editing. D.A.: data verification, resources, writing-review and editing. A.A.F.: data verification, writing-review and editing. B.E.: data verification, writing-review and editing. T.T.: data verification, writing-review and editing. O.J.E.: conceptualization, writing-review and editing, project administration, funding acquisition. A.L.: conceptualization, formal analysis, data validation, writing—original draft, writing—review and editing, supervision. J.D.: conceptualization, data validation, writing-review and editing, supervision, project administration, funding acquisition.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gholinejad, M., Pelanis, E., Aghayan, D. et al. Generic surgical process model for minimally invasive liver treatment methods. Sci Rep 12, 16684 (2022). https://doi.org/10.1038/s41598-022-19891-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-19891-1
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
