
Abstract
Estrogen can promote the acceleration of bone maturation and phthalate esters (PAEs) have estrogen-mimicking effects. We investigated whether PAEs are associated with the acceleration of bone age (BA) in girls with early onset of puberty (EOP). This case–control study enrolled 254 girls with EOP from the Endocrinology Department at Shenzhen Children’s Hospital between December 2018 and August 2019. Ultra-performance liquid chromatography and tandem mass spectrometry were used to analyze the 10 metabolites of PAEs (mPAEs) in urine samples. BA was measured using an artificial intelligence system. BA exceeding the chronological age (CA) by > 2 years (BA-CA ≥ 2 years) was referred to as significant BA advancement. Participants were divided into groups A (BA-CA ≥ 2 years; case group) and B (BA-CA < 2 years; control group). Propensity score matching (PSM) was performed for both groups in a 1:2 ratio with a caliper of 0.25. To identify potential dose–response relationships between PAEs exposure and BA advancement, we grouped the participants after PSM according to the tertiles of the mPAE concentrations. After PSM, 31 and 62 girls in groups A and B were selected. The concentration of Mono-ethyl phthalate (MEP) in group A was significantly higher than in group B (11.83 μg/g vs. 7.11 μg/g, P < 0.05); there was no significant difference in the levels of other mPAEs between the groups. The degree of BA advancement and proportion of significantly advanced BA in the lowest, middle, and highest tertiles of the MEP sequentially increased, as well as in the lowest, middle, and highest tertiles of Mono-(2-ethyl-5-carboxypentyl) phthalate; however, these were only statistically different between the highest and lowest MEP tertiles (both P < 0.05). For the remaining mPAEs, differences in the degree of BA advancement among the lowest, middle, and highest tertiles, as well as differences in the proportion of significantly advanced BA among the lowest, middle, and highest tertiles, were not significant (all P > 0.05). Our findings suggested that MEP was positively associated with BA advancement in girls with EOP. Exposure to PAEs may promote accelerated bone maturation.
Similar content being viewed by others


Introduction
Bone maturation, evaluated clinically by bone age (BA), refers to the developmental process from the emergence of ossification centers to the adult form of bones1. Acceleration of bone maturation manifests as a BA that exceeds the chronological age (CA), known as BA advancement. Significant BA advancement suggests an attenuation of the height growth potential. In other words, although children with advanced BA are taller than their peers during childhood, their growth plates fuse earlier and they may be shorter than their peers in adulthood. Shorter height may influence their physical and mental health from childhood to adulthood2; thus, significantly accelerated bone maturation, which could lead to impaired final adult height, is a social health issue that deserves attention. However, children with considerably advanced BA (BA-CA ≥ 2 years) have been observed in different populations: approximately 10% of healthy prepubescent Chinese children (unpublished observations by our research team); up to 21% of healthy children in the United States3; and 48.7% of girls with isolated premature thelarche, who should not have significantly advanced BA4,5. Moreover, a long-term trend of overall accelerated bone maturation in children has been observed in many countries3,6,7,8,9,10. Unfortunately, existing research results cannot fully explain the acceleration of bone maturation in children. Estradiol (E2) is the major factor that promotes bone maturation and growth plate fusion11,12,13,14,15. The body mass index (BMI), dehydroepiandrosterone sulfate (DHEAS), serum insulin-like growth factor-1 (IGF-1), and E2 are the most recognized independent risk factors for advanced bone maturation, explaining only 19.3–24% of all cases4,16, which indicates that more than half of the factors accelerating bone maturation remain unknown.
Phthalate esters (PAEs) are environmental endocrine-disrupting chemicals that interfere with the functioning of an organism’s endocrine system. Human exposure to PAEs is widespread and is a serious potential problem for human health, especially for children during the immature and developmental stages17. PAEs have been shown to have estrogenic effects17,18,19,20. PAEs exposure reportedly increases the incidence of precocious puberty in girls21. However, there is a lack of clinical case studies on the association between PAEs exposure and accelerated bone maturation. The impact of PAEs on accelerated bone maturation must be identified as soon as possible because PAEs are ubiquitous in the various ecosystems of the Pearl River Delta region in China, where Shenzhen is located22,23,24, indicating that children are almost continuously exposed to them.
In China, central precocious puberty (CPP)25 is defined as puberty before the age of 8 years while early puberty (EP)26 is defined as entering puberty between ages 8 and 9.5 years. Both CPP and EP present early functional initiation of the hypothalamic-pituitary–gonadal axis and BA advancement; however, definitions of the puberty onset age overlap and vary by country26. Therefore, in this study, we referred to CPP and EP together as the early onset of puberty (EOP). In this study, we investigated whether PAEs could accelerate bone maturation in girls with EOP. For our research purposes, we examined 10 urinary PAE metabolites (mPAEs) in the urine samples of girls with EOP and evaluated BA using emerging artificial intelligence (AI) technology to reduce manual evaluation errors. Propensity score matching (PSM) was used to balance confounding factors. Monoethyl phthalate (MEP) was positively associated with accelerated bone maturation.
Methods
Participants
Parents or guardians of all study participants provided written informed consent. All procedures were conducted according to the relevant guidelines and regulations. This study was approved by the Ethics Committee of the Shenzhen Children’s Hospital (201905503). We performed follow-ups with most girls aged 6–10 years with an early occurrence of secondary sexual characteristics in the outpatient department of our hospital. They were advised temporary hospitalization to complete gonadotropin-releasing hormone (GnRH) stimulation tests if they met the indications for hospitalization as follows: breast development occurring before the age of 9.5 years and persisting for at least 3 months, with a combination of at least one of the following: (1) the breast Tanner stage progressed in no more than 6 months; (2) BA exceeded CA for more than 2 years, and (3) accelerated height growth. Girls suspected of CPP or EP were verified via the GnRH stimulation test, and pathological causes, such as central nervous system tumors, were ruled out in the Department of Endocrinology at Shenzhen Children’s Hospital between December 2018 and August 2019.
The inclusion criteria were as follows: (1) breast development before 9.5 years old; (2) GnRH stimulation test results were positive: the ratio of the peak luteinizing hormone (LH) to the peak follicle-stimulating hormone (FSH) was > 0.6 while the level of the peak LH was > 5.0 IU/L; (3) pelvic ultrasound: the length of the uterus was > 3.4 cm, the volume of the ovary was > 1 mL, and there were more than two follicles with a diameter of > 4 mm; and (4) without other causes, such as a central nervous system tumor, peripheral precocious puberty, or local mammary gland hyperplasia, among others. Our study included 302 girls initially diagnosed with CPP or EP.
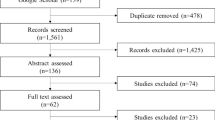
Girls with a history of hormone treatment or Chinese traditional medicine, other endocrine diseases (including atypical adrenocortical hyperplasia, abnormal thyroid function, and growth hormone deficiency), abnormal bone development, congenital dysplasia, severe obesity, infants small for their gestational age, premature birth, and lack of left-hand radiographs in our hospital were excluded. Ultimately, 254 girls were enrolled in this study (Fig. 1).

Flowchart of the population selected for the study.
This was a case–control study. The enrolled girls were divided into group A (BA-CA ≥ 2 years) as the case group and group B (BA-CA < 2 years) as the control group according to whether BA was significantly advanced. To identify potential dose–response relationships between BA advancement and mPAE concentrations, we additionally categorized the girls into groups according to the tertiles of the urinary mPAE concentration: lowest (< Q1), middle (Q1–Q2), and highest (> Q2) tertiles.
Physical and laboratory examination
Standing height (cm) and body weight (kg) were measured using the same apparatus and following the same standard procedure. The BMI was calculated as the body weight (kg)/height (m)2. Breast development was staged by well-trained pediatricians from the endocrinology department according to the Tanner criteria.
GnRH stimulation tests and venous blood samples were collected to determine serum hormone levels between 8:00 and 10:00 am in a fasting state. The gonadotropin injection volume was 2.5–3.0 µg/kg; each injection volume did not exceed 100 µg in the GnRH stimulation test. The E2, LH, and FSH levels were measured using immunochemiluminometric assays.
The BMI, DHEAS, and IGF-1 levels were standardized and expressed as standard deviation scores (SDS) according to reference data for different sexes and ages of Chinese children27,28,29, calculated as follows: (measured value − mean value for the same age and sex)/standard deviation.
Urinary phthalate metabolite analysis
Polypropylene tubes were used to collect spot urine samples (50 mL). Urine samples were collected during the hospital stay and transported to the laboratory at the Shenzhen Center of Disease Control and Prevention on ice within 4 h, stored at − 40 °C, and tested within 1 year.
A total of 10 urinary mPAEs were detected in this study: monoethyl phthalate (MEP), mono-methyl phthalate (MMP), monobutyl phthalate (MBP), mono-isobutyl phthalate (MiBP), mono-benzyl phthalate (MBzP), mono (2-ethyl-5-hydroxyhexyl) phthalate (MEHHP), mono (2-ethylhexyl) phthalate (MEHP), mono (2-ethyl-5-carboxypentyl) phthalate (MEOHP), mono -(2-ethyl-5-carboxypentyl) phthalate (MECPP), and mono -[(2-carboxymethyl)hexyl] phthalate (MCMHP). We selected the 10 mPAEs because their parent compounds have been detected at relatively high levels in the Pearl River Delta region, where Shenzhen is located23; their detection rates are high in the urine of primary school students in Shenzhen24. All urinary mPAEs were analyzed via ultra-performance liquid chromatography and tandem mass spectrometry (UHPLC-MS/MS). Details of the method, including information on the relatively isotopically labeled internal standards and reagents, have been reported previously24. Urinary creatinine concentrations were determined using UHPLC-MS/MS to correct urine dilution30.
BA assessment
BA was evaluated using an automated AI system (Yitu Healthcare, Hangzhou, China), known as the intelligent diagnosis system for child growth and development, which was developed for Chinese children using the TW3-Chinese RUS method31. The TW3-Chinese RUS method is a standard method for determining bone maturity in Chinese children based on the TW3 RUS method32.
Statistical analysis
The detection threshold of E2 at our hospital was 20 pg/mL. The concentrations of E2 and mPAEs below the limit of detection (LOD) were replaced with 1/2 LOD. PAEs are often classified as low-molecular-weight (LMW) and high-molecular-weight (HMW) phthalates during exposure analyses33,34. ΣDi(2-ethylhexyl) phthalate (DEHP) is the sum of the creatinine-corrected concentrations of the five metabolites of DEHP (MCMHP, MEHP, MEOHP, MEHHP, and MECPP). ΣLMW is the sum of creatinine-corrected concentrations of the four LMW phthalate metabolites (MBP, MMP, MiBP, and MEP). ΣHMW is the sum of the creatinine-corrected concentrations of the six HMW phthalate metabolites (ΣDEHP and MBzP). ΣmPAE is the sum of the creatinine-corrected concentrations of all mPAEs (ΣLMW and ΣHMW)35.
Differences between the two groups of continuous variable data were analyzed using the Student’s t-test or Mann–Whitney U test. The differences between multiple groups of continuous variable data were tested using the Kruskal–Wallis one-way ANOVA. Rates between multiple groups were compared using the multiple-group chi-square test with Bonferroni correction. Statistical significance was set at P < 0.05. SPSS (version 23, IBM Corporation, Armonk, NY, USA) was used for data analysis.
PSM was performed on R software (version 3.3.3; R Foundation for Statistical Computing) using the MatchIt package (version 3.0.2). Based on previous research results and clinical experience, the study included the age of onset, disease duration, BMI SDS, DHEAS SDS, and IGF-1 SDS as covariates for the PSM4,16. The matching ratio of groups A and B was 1:2 because the number of patients in group B was 3.2-fold higher than in group A. Logistic regression was used to calculate the propensity scores. The nearest neighbor matching method was used for matching in PSM. To ensure a suitable sample size and better matching balance, after setting different caliper values several times for matching, the final caliper value was set to 0.25. The baseline variables of the two matched groups were compared; standardized mean differences were calculated to assess whether the included confounding factors were balanced.
Ethics approval and consent to participate
All study participants provided written informed consent from their parents or guardians. This study was approved by the Ethics Committee of the Shenzhen Children’s Hospital (201905503).
Results
Baseline characteristics before and after PSM
After PSM, 93 girls (31 in group A and 62 in group B) were selected. Table 1 presents the baseline characteristics before and after PSM. There were no statistical differences in the baseline variables between groups A and B after PSM (P > 0.05). The standardized mean difference of the baseline variables after matching was < 0.1, indicating that the PSM balance was optimal. The median and quantile of E2 levels were 24.0 (10.0, 39.0) pg/mL in group A and 10.0 (10.0, 33.3) pg/mL in group B following PSM analysis, and no statistical differences between the two groups were found (P = 0.463).
Urinary phthalate metabolites levels
The detection rates of mPAEs in the urine of the 93 girls were as follows: MBP (100%), MMP (98.9%), MECPP (98.9%), MiBP (96.7%), MEHHP (95.7%), MEP (92.5%), MEOHP (92.5%), MEHP (89.2%), MCMHP (86.0%), and MBzP (11.8%). The highest concentration of creatinine-corrected urinary mPAE was MBP (geometric mean: 203.77 μg/g), followed by MiBP (45.07 μg/g), MEP (8.55 μg/g), MMP (7.80 μg/g), MECPP (7.17 μg/g), MEHHP (5.99 μg/g), MEHP (5.10 μg/g), MEOHP (4.32 μg/g), MCMHP (2.58 μg/g), and MBzP (0.12 μg/g). The concentration of ΣLMW (308.41 μg/g) was higher than that of ΣHMW (28.05 μg/g). The concentration of MEP in group A was significantly higher than that in group B (11.83 μg/g vs. 7.11 μg/g, P < 0.05). There were no significant differences in the levels of the other urinary mPAEs, ΣDEHP, ΣLMW, ΣHMW, and ΣmPAEs between groups A and B (all P > 0.05) (Table 2).
Potential dose–response relationship between urinary phthalate metabolites concentrations and BA advancement
The differences in the degree of BA advancement (BA-CA) among the lowest, middle, and highest tertiles of each mPAE were analyzed and compared (Fig. 2), as were the differences in the proportion of significantly advanced BA among the lowest, middle, and highest tertiles of the mPAEs (Fig. 3). The degree of BA advancement and proportion of significantly advanced BA in the lowest, middle, and highest tertiles for MEP sequentially increased, as well as in the lowest, middle, and highest tertiles for MECPP (Figs. 2 and 3). However, the degree of BA advancement and proportion of significantly advanced BA were statistically different between the highest and lowest MEP tertiles (both P < 0.05) (Figs. 2 and 3). For the remaining urinary mPAEs, differences in the degree of BA advancement among the lowest, middle, and highest tertiles, as well as the differences in the proportion of significantly advanced BA among the lowest, middle, and highest tertiles, were not significant (all P > 0.05) (Figs. 2 and 3).

Bone age (BA) advancement in tertiles of the (a) low molecular weight mPAEs, ΣLMW, ΣHMW, and ΣmPAEs; and (b) high molecular weight mPAEs and ΣDEHP. The degree of BA advancement in the highest MEP tertile was statistically higher than that in the lowest MEP tertile (P < 0.05), as indicated by the asterisk (*). ΣDEHP: sum of the creatinine-corrected concentrations of MCMHP, MEHP, MEOHP, MEHHP, and MECPP. ΣLMW: sum of the creatinine-corrected concentrations of MBP, MMP, MiBP, and MEP. ΣHMW: sum of the creatinine-corrected concentrations of ΣDEHP and MBzP. ΣmPAEs: sum of the creatinine-corrected concentrations of all of the mPAEs.

The proportion of significantly advanced bone age (BA) between the tertiles of the (a) low molecular weight mPAEs, ΣLMW, ΣHMW, and ΣmPAEs; and (b) high molecular weight mPAEs and ΣDEHP groups. The proportion of significantly advanced BA in the highest MEP tertile was statistically higher than that in the lowest MEP tertile (P < 0.05). ΣDEHP: sum of the creatinine-corrected concentrations of MCMHP, MEHP, MEOHP, MEHHP, and MECPP. ΣLMW: sum of the creatinine-corrected concentrations of MBP, MMP, MiBP, and MEP. ΣHMW: sum of the creatinine-corrected concentrations of ΣDEHP and MBzP. ΣmPAEs: sum of the creatinine-corrected concentrations of all of the mPAEs.
Discussion
Bone maturation is affected by both internal and external factors1. However, the influence of environmental factors on bone maturation remains unclear. To our knowledge, the relationship between PAEs exposure and accelerated bone maturation has not yet been examined in girls with EOP. In this study, after using PSM to balance the confounding factors (i.e., disease duration, age of onset, BMI SDS, IGF-1 SDS, and DHEAS SDS) that may affect bone maturation4,16, we found that the urinary MEP concentration of girls with significantly advanced BA was significantly higher than that in the control group. The degree of BA advancement and proportion of significantly advanced BA in the highest MEP tertile were significantly higher than those in the lowest tertile group. Urinary metabolite concentrations can serve as a valuable method for assessing phthalate exposure in humans30. Therefore, our findings indicate that MEP, a monoester metabolite of diethyl phthalate (DEP), may be positively associated with accelerated bone maturation in girls with EOP. PAEs may be an important environmental factor affecting BA.
Previous case reports and studies have shown that estrogen and estrogen receptor α (ERα) is the main determinant of bone maturation and epiphyseal fusion11,12,15. Higher estrogen concentrations can accelerate bone maturation and stimulate fusion of the epiphyseal growth plate, leading to longitudinal growth termination13,14,15. However, children are not only influenced by their estrogen production, but also by substances in the environment that have estrogenic effects, such as PAEs.
Evidence from in vivo and in vitro studies suggests that DEP may exert estrogenic activity by directly acting on the ER and/or increasing estrogen synthesis by inducing aromatase gene expression17,18,19,20. DEP-treated female mice exhibited altered estrous cycle patterns, similar to animals with an increased endogenous estrogen load and corresponding uterine histological changes18. Furthermore, DEP promoted an increase in aromatase gene expression in ovarian cells via ERα both in vivo and in vitro18. Other PAEs also had estrogenic effects; however, DEP and DEHP showed better docking efficiency with ERα and estrogen receptor β (ERβ) than other PAEs in molecular docking studies36. These findings provide a theoretical basis for our findings and may partially explain the fact that only MEP was positively associated with accelerated bone maturation in this study, despite the lower concentrations of MEP compared to MBP. In this study, we also found that MECPP, a metabolite of DEHP, showed a similar pattern as MEP, but the difference was not statistically significant. Nonetheless, we cannot categorically deny the possibility that MECPP may be associated with accelerated bone maturation as PAEs exposure may have synergistic effects36.
The effects of estrogen on longitudinal bone growth are biphasic. Low doses of estrogen promote bone elongation, while high doses induce growth plate senescence and epiphyseal fusion, resulting in the cessation of longitudinal bone growth11. The girls in this study had attained puberty and showed higher estrogen levels relative to prepubertal children. Whether DEP plays a role in accelerating bone maturation on this basis is unclear as we are currently unable to assess urinary DEP alone or all PAE levels corresponding to the amount of E2. This needs further evaluation through clinical and basic research.
DEP is as widely sourced as other PAEs; therefore, we are exposed to it almost constantly. Moreover, modern lifestyles may increase the risk of exposure to high doses of PAEs37. DEP is a colorless and odorless oily liquid that is soluble or partially miscible with organic molecules with aromatic properties38. Therefore, it is often used as a solvent, carrier, and cosmetic ingredient for fragrances and is widely used in personal care products, especially perfumes, skin care lotions, hair care products, cosmetics, and nail polishes, among others37,38,39. DEP is not chemically bound to the product; therefore, it can be released into the environment in a gas or particulate phase37. The use of perfumes is significantly associated with the concentration of DEP in indoor dust37. Skin exposure to DEP is the main route of exposure for the population, especially women who frequently use personal care products, whereas the inhalation of indoor air is the main route of exposure for children to DEP39. Additionally, DEP in the environment can enter the human body through ingestion via the digestive tract and skin directly from the air30,40.
This study found weak evidence that MEP exposure may be positively associated with accelerated bone maturation in girls with EOP. Future studies must therefore investigate the impact that PAEs exposure has on accelerated bone maturation and its underlying mechanism. At the same time, we should raise awareness about reducing exposure to PAEs, especially for children.
Study limitations
One of the major limitations of this study was that a single spot urine test for mPAEs reflects only the short-term exposure level of PAEs. Changes in lifestyle, such as dietary habits and the use of nursing products, could also affect the results. Another major limitation was the small sample size (due to limited EOP cases), which reduces the statistical power and strength of the evidence.
Conclusions
Our findings indicate that MEP could be positively associated with accelerated bone maturation in girls with EOP by detecting MEP concentrations in urine samples. We should raise awareness of the need to reduce exposure to PAEs. Future studies must examine the relationship between PAEs exposure and the acceleration of bone maturation.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AI:
-
Artificial intelligence
- BA:
-
Bone age
- BMI:
-
Body mass index
- CA:
-
Chronological age
- CPP:
-
Central precocious puberty
- DEHP:
-
Di(2-ethylhexyl) phthalate
- DEP:
-
Diethyl phthalate
- DHEAS:
-
Dehydroepiandrosterone sulfate
- E2 :
-
Estradiol
- EOP:
-
Early onset of puberty
- ERα:
-
Estrogen receptor α
- ERβ:
-
Estrogen receptor β
- FSH:
-
Follicle-stimulating hormone
- GnRH:
-
Gonadotropin-releasing hormone
- HMW:
-
High-molecular-weight
- LH:
-
Luteinizing hormone
- LMW:
-
Low-molecular-weight
- LOD:
-
Limit of detection
- MBP:
-
Monobutyl phthalate
- MBzP:
-
Mono-benzyl phthalate
- MCMHP:
-
Mono-[(2-carboxymethyl)hexyl] phthalate
- MECPP:
-
Mono-(2-ethyl-5-carboxypentyl) phthalate
- MEHHP:
-
Mono (2-ethyl-5-hydroxyhexyl) phthalate
- MEHP:
-
Mono (2-ethylhexyl) phthalate
- MEOHP:
-
Mono (2-ethyl-5-carboxypentyl) phthalate
- MEP:
-
Mono-ethyl phthalate
- MiBP:
-
Mono-isobutyl phthalate
- MMP:
-
Mono-methyl phthalate
- mPAEs:
-
Metabolites of PAEs
- PAEs:
-
Phthalate esters
- PSM:
-
Propensity score matching
- SDS:
-
Standard deviation scores
References
Creo, A. L. & Schwenk, W. F. Bone age: A handy tool for pediatric providers. Pediatrics https://doi.org/10.1542/peds.2017-1486 (2017).
Christensen, T. L., Djurhuus, C. B., Clayton, P. & Christiansen, J. S. An evaluation of the relationship between adult height and health-related quality of life in the general UK population. Clin. Endocrinol. (Oxf.) 67(3), 407–412. https://doi.org/10.1111/j.1365-2265.2007.02901.x (2007).
Calfee, R. P., Sutter, M., Steffen, J. A. & Goldfarb, C. A. Skeletal and chronological ages in American adolescents: Current findings in skeletal maturation. J. Child. Orthop. 4(5), 467–470. https://doi.org/10.1007/s11832-010-0289-z (2010).
Su, H. et al. Factors affecting bone maturation in Chinese girls aged 4–8 years with isolated premature thelarche. BMC Pediatr. 20(1), 356. https://doi.org/10.1186/s12887-020-02256-w (2020).
Huiping, S. et al. Bone maturation in girls aged 4–8 years with isolated premature thelarche in a relative progression. Chin. J. Osteoporos. Bone Miner. Res. 14, 29–34. https://doi.org/10.3969/j.issn.1674-2591.2021.01.006 (2021).
Himes, J. H. An early hand-wrist atlas and its implications for secular change in bone age. Ann. Hum. Biol. 11(1), 71–75. https://doi.org/10.1080/03014468400006911 (1984).
Hawley, N. L., Rousham, E. K., Norris, S. A., Pettifor, J. M. & Cameron, N. Secular trends in skeletal maturity in South Africa: 1962–2001. Ann. Hum. Biol. 36(5), 584–594. https://doi.org/10.1080/03014460903136822 (2009).
Duren, D. L., Nahhas, R. W. & Sherwood, R. J. Do secular trends in skeletal maturity occur equally in both sexes?. Clin. Orthop. Relat. Res. 473(8), 2559–2567. https://doi.org/10.1007/s11999-015-4213-1 (2015).
Hsieh, C. W., Liu, T. C., Jong, T. L. & Tiu, C. M. Long-term secular trend of skeletal maturation of Taiwanese children between agricultural (1960s) and contemporary (after 2000s) generations using the Tanner-Whitehouse 3 (TW3) method. J. Pediatr. Endocrinol. Metab. 26(3–4), 231–237. https://doi.org/10.1515/jpem-2012-0213 (2013).
Boeyer, M. E., Sherwood, R. J., Deroche, C. B. & Duren, D. L. Early maturity as the new normal: A century-long study of bone age. Clin. Orthop. Relat. Res. 476(11), 2112–2122. https://doi.org/10.1097/CORR.0000000000000446 (2018).
Rochira, V., Kara, E. & Carani, C. The endocrine role of estrogens on human male skeleton. Int. J. Endocrinol. 2015, 165215. https://doi.org/10.1155/2015/165215 (2015).
Zirilli, L., Rochira, V., Diazzi, C., Caffagni, G. & Carani, C. Human models of aromatase deficiency. J. Steroid Biochem. Mol. Biol. 109(3–5), 212–218. https://doi.org/10.1016/j.jsbmb.2008.03.026 (2008).
Almeida, M. et al. Estrogens and androgens in skeletal physiology and pathophysiology. Physiol. Rev. 97(1), 135–187. https://doi.org/10.1152/physrev.00033.2015 (2017).
Nilsson, O. et al. Evidence that estrogen hastens epiphyseal fusion and cessation of longitudinal bone growth by irreversibly depleting the number of resting zone progenitor cells in female rabbits. Endocrinology 155(8), 2892–2899. https://doi.org/10.1210/en.2013-2175 (2014).
Borjesson, A. E. et al. The role of estrogen receptor alpha in growth plate cartilage for longitudinal bone growth. J. Bone Miner. Res. 25(12), 2690–2700. https://doi.org/10.1002/jbmr.156 (2010).
Sopher, A. B. et al. Bone age advancement in prepubertal children with obesity and premature adrenarche: Possible potentiating factors. Obesity (Silver Spring) 19(6), 1259–1264. https://doi.org/10.1038/oby.2010.305 (2011).
Eales, J. et al. Human health impacts of exposure to phthalate plasticizers: An overview of reviews. Environ. Int. 158, 106903. https://doi.org/10.1016/j.envint.2021.1069035 (2022).
Kumar, N., Sharan, S., Srivastava, S. & Roy, P. Assessment of estrogenic potential of diethyl phthalate in female reproductive system involving both genomic and non-genomic actions. Reprod. Toxicol. 49, 12–26. https://doi.org/10.1016/j.reprotox.2014.06.008 (2014).
Guven, C. et al. Low dose monoethyl phthalate (MEP) exposure triggers proliferation by activating PDX-1 at 1.1B4 human pancreatic beta cells. Food Chem. Toxicol. 93, 41–50. https://doi.org/10.1016/j.fct.2016.04.023 (2016).
Jobling, S., Reynolds, T. & White, R. A variety of environmentally persistent chemicals, including some plasticizers, are weakly estrogenic. Environ. Health Perspect. 103, 582–587. https://doi.org/10.1289/ehp.95103582 (1995).
Hashemipour, M., Kelishadi, R., Amin, M. M. & Ebrahim, K. Is there any association between phthalate exposure and precocious puberty in girls?. Environ. Sci. Pollut. Res. Int. 25(14), 13589–13596. https://doi.org/10.1007/s11356-018-1567-4 (2018).
Gao, D., Li, Z., Wang, H. & Liang, H. An overview of phthalate acid ester pollution in China over the last decade: Environmental occurrence and human exposure. Sci. Total Environ. 645, 1400–1409. https://doi.org/10.1016/j.scitotenv.2018.07.093 (2018).
Liu, W. et al. Indoor exposure to phthalates and its burden of disease in China. Indoor Air 32(4), e13030. https://doi.org/10.1111/ina.13030 (2022).
Yao, Y. et al. Urinary phthalate metabolites in primary school starters in Pearl River Delta, China: Occurrences, risks and possible sources. Environ. Res. 179(Pt B), 108853. https://doi.org/10.1016/j.envres.2019.108853 (2019).
Bradley, S. H., Lawrence, N., Steele, C. & Mohamed, Z. Precocious puberty. BMJ 368, l6597. https://doi.org/10.1136/bmj.l6597 (2020).
Mul, D., Oostdijk, W. & Drop, S. L. S. Early puberty in girls. Best Pract. Res. Clin. Endocrinol. Metab. 16(1), 153–163. https://doi.org/10.1053/beem.2002.0187 (2002).
Zhe, S., HuaMei, M., YanHong, L. & MinLian, D. Change of serum dehydroepiandrosterone sulfate (DHEAS) level in children and adolescents. Chin. J. Lab. Med. 31, 1358–1362 (2008).
Shanshan, X., Xuefan, G., Hhui, P. & Huijuan, Z. Study on normal reference values of serum insulin growth factor-1 and insulin factor binding protein-3 in children and adolescents. J. Clin. Pediatr. 27, 1105–1110 (2009).
Hhui, L., Chengye, J., Xinnan, Z. & Yaqin, Z. Body mass index growth curves for Chinese children and adolescents aged 0 to18 years. Chin. J. Pediatr. 47, 493–498. https://doi.org/10.3760/cma.j.issn.0578-1310.2009.07.004 (2009).
Johns, L. E., Cooper, G. S., Galizia, A. & Meeker, J. D. Exposure assessment issues in epidemiology studies of phthalates. Environ. Int. 85, 27–39. https://doi.org/10.1016/j.envint.2015.08.005 (2015).
Zhou, X. L. et al. Diagnostic performance of convolutional neural network-based Tanner-Whitehouse 3 bone age assessment system. Quant. Imaging Med. Surg. 10(3), 657–667. https://doi.org/10.21037/qims.2020.02.20 (2020).
Zhang, S. Y. et al. Standards of TW3 skeletal maturity for Chinese children. Ann. Hum. Biol. 35(3), 349–354. https://doi.org/10.1080/03014460801953781 (2008).
Phthalates action plan (Information on PBT chemicals can be found on the EPA website at http://www.epa.gov/pbt/) U.S. Environmental Protection Agency (2012).
Yu, W., Hongkai, Z. & Kannan, K. A review of biomonitoring of phthalate exposures. Toxics 7(2), 21. https://doi.org/10.3390/toxics7020021 (2019).
Wolff, M. S. et al. Prenatal phenol and phthalate exposures and birth outcomes. Environ. Health Perspect. 116(8), 1092–1097. https://doi.org/10.1289/ehp.11007 (2008).
Hamid, N., Junaid, M., Manzoor, R., Jia, P. P. & Pei, D. S. Prioritizing phthalate esters (PAEs) using experimental in vitro/vivo toxicity assays and computational in silico approaches. J. Hazard. Mater. 398, 122851. https://doi.org/10.1016/j.jhazmat.2020.122851 (2020).
Zhang, Q. et al. Phthalate exposure in Chinese homes and its association with household consumer products. Sci. Total Environ. 719, 136965. https://doi.org/10.1016/j.scitotenv.2020.136965 (2020).
Api, A. M. Toxicological profile of diethyl phthalate A vehicle for fragrance and cosmetic ingredients. Food Chem. Toxicol. 39(2), 97–108. https://doi.org/10.1016/s0278-6915(00)00124-1 (2001).
Guo, Y. & Kannan, K. A survey of phthalates and parabens in personal care products from the United States and its implications for human exposure. Environ. Sci. Technol. 47, 14442–14449. https://doi.org/10.1021/es4042034 (2013).
Weschler, C. J. et al. Transdermal uptake of diethyl phthalate and di(n-butyl) phthalate directly from air: Experimental verification. Environ. Health Perspect. 123(10), 928–934. https://doi.org/10.1289/ehp.1409151 (2015).
Acknowledgements
We would like to thank Editage (www.editage.cn) for English language editing.
Funding
This study was supported by the High-level Key Clinical Specialty project of Guangdong Provincial Health Commission (Supporting construction funds of Shenzhen) (SZGSP012), and the Shenzhen Science and Technology program (JCYJ20210324123610028 and KCXFZ20201221173400002). The funders had no role in the design of the study or collection, analysis, interpretation of data, or writing the manuscript.
Author information
Authors and Affiliations
Contributions
S.H. analyzed and interpreted the data, and was a major contributor in writing the manuscript. Z.S. was a major contributor in design of the work and substantively revised the manuscript. Y.Y. and L.Z. was a major contributor in acquisition data of mPAEs concentrations. H.S., Y.J., X.Z. and X.Z. contributed to the acquisition and analysis of the data. Q.S. contributed to the design of the work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huang, S., Su, Z., Su, H. et al. Association between phthalate exposure and accelerated bone maturation in Chinese girls with early puberty onset: a propensity score-matched case–control analysis. Sci Rep 12, 15166 (2022). https://doi.org/10.1038/s41598-022-19470-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-19470-4
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
