
Abstract
We aimed to evaluate the changes in maternal and neonatal complications such as threatened preterm labor (TPL) and preterm birth before and during the coronavirus disease 2019 (COVID-19) pandemic using large-scale real-world data in Japan. We obtained data from the Japan Medical Data Center claims database and evaluated differences in maternal and neonatal complications, such as the prevalence of TPL and preterm birth before the COVID-19 pandemic (in the year 2018 or 2019) and during the COVID-19 pandemic (in 2020). We included 5533, 6257, and 5956 deliveries in the years 2018, 2019, and 2020, respectively. TPL prevalence and preterm birth had significantly decreased in 2020 (41.3%, 2.6%, respectively) compared with those reported in 2018 (45.3%, 3.9%, respectively) and 2019 (44.5%, 3.8%, respectively). Neonatal outcomes such as low-birth-weight infants and retinopathy of prematurity were also improved during the pandemic. There were no clear trends in the prevalence of maternal complications such as hypertensive disorders of pregnancy; hemolysis, elevated liver enzymes, and low platelets (HELLP) syndrome; and preeclampsia. Oral ritodrine hydrochloride usage in all participants had significantly decreased during the COVID-19 pandemic. In conclusion, our results suggest that the COVID-19 pandemic has ameliorated TPL and consequently reduced the number of preterm births.
Similar content being viewed by others


Introduction
The coronavirus disease 2019 (COVID-19) has become a great public health concern. After the World Health Organization declared the COVID-19 outbreak a pandemic, some studies reported that people’s lifestyles have become more sedentary and less active worldwide1 and also in Japan2. People tend to stay at home and avoid outdoor and excessive leisure-time activities. The resulting inactivity was observed across age groups and even among pregnant women. Such lifestyle changes due to the pandemic may affect the risk of maternal and neonatal complications, such as threatened preterm labor (TPL) and preterm birth.
The association between maternal physical activity and TPL is a controversial topic of great scientific interest. Increased participation in leisure-time physical activities was previously linked to a lower risk of preterm birth3. In contrast, participation in heavy, long, or standing occupational physical activities was also shown to be associated with an increased risk of preterm birth4,5,6,7. The influence of physical activity on TPL and preterm birth are different according to the types and intensity of activities. Bed rest is one of the most common interventions to prevent preterm birth. However, its effectiveness for TPL prevention remains unclear8,9,10. Besides heavy labor during pregnancy, previous history of TPL or preterm birth11,12,13 and infections7,11,14 are also known risk factors of TPL and preterm birth.
Although the use of ritodrine hydrochloride is generally avoided for TPL treatment in other countries due to cardiopulmonary side effects, its use is common in Japan9,10,15. However, there is no report of the impact of the use of ritodrine hydrochloride during the COVID-19 pandemic. Because TPL management may also have been influenced by the COVID-19 pandemic through maternal lifestyle changes, the correlation between the effect of COVID-19 and the use of tocolytic agents is unclear. However, it is difficult to evaluate TPL and its management in a nationwide context in Japan during the COVID-19 pandemic with a limited number of patients in a few hospitals. Therefore, we aimed to evaluate the changes in the occurrence of maternal and neonatal complications, such as TPL, in response to lifestyle changes due to the COVID-19 pandemic by assessing large-scale real-world data in Japan.
Methods
Data source and study participants
We extracted information from the Japan Medical Data Center database (JMDC, Inc., Tokyo, Japan; JMDC). This database includes the patient's health insurance claims, medical examination data, and ledger data from employee-based insurances in Japan.
We included women who delivered their babies between October and December in 2018, 2019, and 2020 in this study. As the Japanese government declared a state of emergency in April 2020 for the first time since the global COVID-19 outbreak, we defined the deliveries in 2018 and 2019 as those that occurred before the COVID-19 pandemic and the deliveries in 2020 as those that occurred during the pandemic. We limited the deliveries from October to December to set the entire pregnancy period after April 2020, when people started to adopt a sedentary lifestyle. Deliveries were defined using the year and month of birth of the participant’s newborn based on the ledger data or procedure codes and dates related to deliveries. From the JMDC database, we extracted 17,746 deliveries, which met our inclusion criteria. This study was conducted following proper guidelines, such as the Japanese Ethical Guidelines for Medical and Biological Research Involving Human Subjects. Informed consent from participants was not required as all identifying information of the participants was completely anonymized. The study protocol was approved by the Ethics Committee at the Shiga University of Medical Science (No. R2021-139).
Definition of variables
TPL and other complications were diagnosed based on the International Classification of Diseases, Tenth Revision (ICD-10) codes. Procedures, such as cesarean section, were searched by Japanese standardized procedure codes. Data on the use of medication, such as ritodrine hydrochloride and magnesium sulfate, were retrieved using Japanese individual drug codes. The amount of medication used was calculated based on the prescribed dosage for each medicine and dosing period.
TPL was defined by the ICD-10 code for TPL (O60.0) or as the usage of any type of ritodrine hydrochloride. Preterm birth was defined by the newborn’s ICD-10 code for preterm birth (P07.2, P07.3) and the birth of a very low or extremely low birth weight infant (P07.0: birth weight of less than 1000 g, P07.1: 1000–1499 g).
Complications diagnosed during pregnancy—such as hypertensive disorders of pregnancy (O10, O11, O13–O16); hemolysis, elevated liver enzymes, and low platelets (HELLP) syndrome (O14.2); and preeclampsia (O14.0, O14.1, O14.9)—were extracted using ICD-10 codes recorded for diagnoses within seven months before delivery. Data on complications diagnosed before pregnancy, such as hypertension (I10-I15), diabetes (E10-E14), and anti-phospholipid syndrome (D68.6), were extracted using ICD-10 codes diagnosed more than ten months before delivery. Data on neonatal outcomes were extracted using ICD-10 codes for respiratory distress syndrome (P22.0), low birth weight (P07.0-P07.2) and retinopathy of prematurity (H35.1), procedure codes for admission to neonatal intensive care unit and respiratory support, or drug codes for artificial pulmonary surfactant, which were recorded in the delivery month.
Statistical analysis
We evaluated differences in maternal and neonatal complications at childbirth between October and December in 2018, 2019, and 2020. Comparison analysis was performed using Pearson’s chi-square test for categorical variables and Student’s t-test or Wilcoxon’s rank sum test for continuous variables. Bonferroni-corrected p-value of less than 0.0167 was used as the statistical significance threshold due to multiple testings in 2018, 2019, and 2020. All statistical analyses were performed using SAS version 9.42 (SAS Institute Inc., Cary, NC, USA).
Results
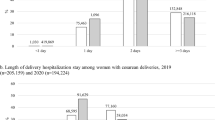
There were 5533, 6257, and 5956 deliveries in the years 2018, 2019, and 2020, respectively (Fig. 1); the corresponding number of newborns were 5597, 6339, and 6021, respectively (Fig. 1). Basic characteristics of participants, such as mother’s age at birth or complications before pregnancy, including hypertension, had not changed between periods before and during the COVID-19 pandemic (Table 1). TPL prevalence had significantly decreased in 2020 (n = 2458, 41.3%) compared with that in 2018 (n = 2507, 45.3%) and 2019 (n = 2781, 44.5%) (Table 1). Preterm birth prevalence in 2020 (n = 154, 2.6%) had declined in comparison to those in 2018 (n = 218, 3.9%) and 2019 (n = 238, 3.8%). Meanwhile, no clear trends were observed in the prevalence of hypertensive disorders of pregnancy, HELLP syndrome, preeclampsia, emergency transfer, and deliveries by cesarean section. Among the participants during the COVID-19 pandemic, we extracted seven COVID-19 cases by ICD-10 code (U07.1), which were four cases in the TPL group and three cases in the non-TPL group (data not shown). No participants got vaccinations in our study as the COVID-19 vaccinations had not been approved yet in Japan in 2020.

Flow chart of the study population. We firstly extracted delivery information from October to December between 2018 and 2020 from the database. The numbers of participants were shown based on deliveries and newborns. We defined the deliveries in 2018 and 2019 as before the COVID-19 pandemic and the deliveries in 2020 as during the COVID-19 pandemic. TPL was diagnosed by ICD-10 code and the use of tocolytic agents, which records were used to analyze each medical use and dosage. COVID-19 Coronavirus disease 2019, TPL threatened preterm labor.
In terms of neonatal complications, the prevalence of low-birth-weight infant had significantly decreased in 2020 (n = 224, 3.7%) compared with those in 2018 (n = 330, 5.9%) and 2019 (n = 353, 5.6%) (Table 2). The prevalence of retinopathy of prematurity had also decreased in 2020 (n = 14, 0.2%) compared with those in 2018 (n = 37, 0.7%) and 2019 (n = 41, 0.7%). There were no differences in admission to the neonatal intensive care unit and diagnosis of infant respiratory distress syndrome between the periods before and during the COVID-19 pandemic.
Oral ritodrine hydrochloride usage in total participants was significantly decreased in 2020 (n = 1626, 27.3%) compared to those in 2018 (n = 1720, 31.1%) and 2019 (n = 1911, 30.5%). For intravenous administration of ritodrine hydrochloride, there was no significant difference among the years of 2018 (n = 364, 6.6%), 2019 (n = 424, 6.8%), and 2020 (n = 396, 6.7%). In patients with TPL, the ritodrine hydrochloride usage rate, for both intravenous and oral administration, did not significantly change in the years 2018 (14.5% for intravenous, 68.6% for oral administration), 2019 (15.3%, 68.7%), and 2020 (16.1%, 66.2%). Usage rate of magnesium sulfate also did not show any differences among the years 2018 (3.4%), 2019 (3.0%), and 2020 (3.2%) in patients with TPL. The median intravenous dosage of ritodrine hydrochloride (50 mg of ritodrine hydrochloride per ampule) did not change in 2020 (22.0 ampoules per delivery) compared with those in 2018 (21.5 ampoules per delivery) and 2019 (20.0 ampoules per delivery) (Table 3). The median oral dosage of ritodrine hydrochloride (5 mg of ritodrine hydrochloride per tablet) also did not change in 2020 (62.5 tablets per delivery) compared with those in 2018 (63.0 tablets per delivery) and 2019 (63.0 tablets per delivery). The dosage of magnesium sulfate (10 g of magnesium sulfate per ampule) did not present any difference in 2020 (8.0 ampoules per delivery) compared with those in 2018 (8.0 ampoules per delivery) and 2019 (7.0 ampoules per delivery). The percentage of TPL treated in larger medical institutions (≥ 20 beds) did not change in the years 2018 (46.0%), 2019 (45.0%), and 2020 (43.7%).
Discussion
The present study showed that the prevalence of TPL and preterm birth during the COVID-19 pandemic significantly decreased compared with those before the COVID-19 pandemic. Neonatal outcomes, such as low-birth-weight infants and retinopathy of prematurity, were also improved during the COVID-19 pandemic. Our result is consistent with a previous report of decreased preterm birth during the pandemic in high-income countries16. Although another study also reported that the prevalence of TPL and preterm birth decreased during and after the state of emergency in Japan, we also demonstrated improved outcomes of neonatal complications based on a larger sample size compared to the previous study17. Furthermore, our study showed oral ritodrine hydrochloride usage in all the participants significantly decreased during the COVID-19 pandemic.
After the first state of emergency declaration in April 2020 by the Japanese government, people changed their lifestyles to stay and work at home in Japan2. Increases in sedentary behaviors during lockdowns in several countries were also reported1. The association between physical activity and TPL is still unclear and varies according to the types and intensity of physical activity, such as leisure-time or occupational physical activity3,4,5,6,7. Additionally, the efficacy of bed rest in TPL management remains to be determined8,9,10. Our result showed that the lifestyle change during the COVID-19 pandemic might influence TPL prevention. However, it is difficult to determine whether there is a direct impact of reduced physical activity on TPL. The types of reduced physical activity due to the COVID-19 pandemic may vary depending on personal lifestyle or occupation. In Japan, while people avoided going outside and excess physical activity during the COVID-19 pandemic, necessary activities of daily living and working were not restricted. Therefore, it is difficult to assume how much people reduced physical activity in our study.
Maternal complications such as hypertensive disorders of pregnancy can be a cause of medically indicated preterm birth11. However, there were no significant differences in the prevalences of hypertensive disorders of pregnancy, HELLP syndrome, and preeclampsia between periods before and during the COVID-19 pandemic in our study. A previous systematic review indicated that there are discrepancies with regard to the influence of sedentary behavior on hypertensive disorders18. One study showed no significant difference in the prevalence of hypertensive disorders between periods before and during the COVID-19 pandemic16. Other studies mentioned that appropriate physical activity reduced the risk of gestational hypertensive disorders19 and preeclampsia20. It is possible that reduced physical activities during the COVID-19 pandemic are not drastic enough to increase the risk of hypertensive disorders. During the pandemic, heavy labor and excess leisure-time activities are limited while necessary daily activities are not reduced. This setting might represent a favorable environment for pregnant women to reduce TPL and not increase hypertensive disorders. Nevertheless, we need to carefully consider the influence of a sedentary lifestyle on hypertensive disorders of pregnancy and other complications during pregnancy.
We did not investigate maternal mental health problems such as depression. However, the COVID-19 pandemic may adversely impact maternal mental health by reduction of physical activity and restriction on social activities, such as meeting people or utilizing social support. A previous report showed no significant influence of a sedentary lifestyle on depression18. In contrast, other studies showed that maternal depression increased during the pandemic in several countries16,21. Maternal depression during pregnancy can be a risk of preterm birth11. Therefore, maternal mental healthcare under limited social support due to COVID-19 is another important public health concern.
We also revealed that only the oral usage rate of ritodrine hydrochloride in all participants significantly decreased during the COVID-19 pandemic. TPL management by the use of ritodrine hydrochloride and magnesium sulfate did not change during the COVID-19 pandemic. This result indicates that the prevalence of mild TPL with only oral ritodrine hydrochloride treatment decreased by lifestyle change due to the COVID-19 pandemic. As a result, the total number of patients with TPL during the pandemic decreased in our study. In contrast, the prevalence of severe TPL, which requires intravenous ritodrine hydrochloride, did not decrease during the pandemic. TPL and preterm birth are induced by various causes7,11, such as a previous history of TPL or preterm birth12,13, infection7,14, heavy labor4,5,6,7, and many other maternal complications. Our results indicate that a certain amount of mild TPL could be prevented by lifestyle change, including reduction of excessive physical activity.
The strength of our study was the large sample size compared to those in previous reports, as we evaluated the nationwide situation using real-world data in Japan. We also evaluated, in detail, the use of tocolytic agents as our dataset included medication records and the prescribed dosage of each medicine. A limitation of our study was our inability to estimate the extent by which people limited their physical or social activity. However, previous reports showed that people tend to be more sedentary and less active due to the COVID-19 pandemic worldwide1 and also in Japan2. Additionally, we could not obtain the data on gestational age at birth from our database. Since data on the diagnoses of some complications were obtained based on ICD-10 codes alone, the number of cases might be overestimated. However, we excluded suspected disease codes and combined the available information on applied medicine or procedure with ICD-10 codes to improve the diagnostic accuracy of the study.
Conclusion
This study showed that the prevalence of TPL and preterm birth were significantly lower during the COVID-19 pandemic than in the pre-pandemic period. Neonatal outcomes were also improved during the pandemic than in the pre-pandemic period. Although the direct influence of a sedentary lifestyle on TPL remains controversial, our results suggest that maternal lifestyle changes due to the pandemic might have ameliorated TPL and consequently, reduced the risk of preterm birth.
Data availability
The data that support the findings of this study are available from the corresponding author (S.T.) upon reasonable request.
References
Stockwell, S. et al. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 7, e000960 (2021).
Nishijima, C., Miyagawa, N., Tsuboyama-Kasaoka, N., Chiba, Y. & Miyachim, M. Association between lifestyle changes and at-home hours during and after the state of emergency due to the COVID-19 pandemic in Japan. Nutrients 13, 2698 (2021).
Aune, D., Schlesinger, S., Henriksen, T., Saugstad, O. D. & Tonstad, S. Physical activity and the risk of preterm birth: A systematic review and meta-analysis of epidemiological studies. BJOG 124, 1816–1826 (2017).
Cai, C. et al. The impact of occupational activities during pregnancy on pregnancy outcomes: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 222, 224–238 (2020).
Lee, L. J. et al. Role of maternal occupational physical activity and psychosocial stressors on adverse birth outcomes. Occup. Environ. Med. 74, 192–199 (2017).
Mozurkewich, E. L., Luke, B., Avni, M. & Wolf, F. M. Working conditions and adverse pregnancy outcome: A meta-analysis. Obstet. Gynecol. 95, 623–635 (2000).
Goodfellow, L., Care, A. & Alfirevic, Z. Controversies in the prevention of spontaneous preterm birth in asymptomatic women: An evidence summary and expert opinion. BJOG 128, 177–194 (2021).
Sosa, C. G., Althabe, F., Belizan, J. M. & Bergel, E. Bed rest in singleton pregnancies for preventing preterm birth. Cochrane Database Syst. Rev. 3, CD003581 (2015).
Management of Preterm Labor. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. Practice Bulletin No. 171. Obstet. Gynecol. 128, e155–e164 (2016).
Goldenberg, R. L. The management of preterm labor. Obstet. Gynecol. 100, 1020–1037 (2002).
Goldenberg, R. L., Culhane, J. F., Iams, J. D. & Romero, R. Epidemiology and causes of preterm birth. Lancet 371, 75–84 (2008).
Mercer, B. M. et al. The preterm prediction study: effect of gestational age and cause of preterm birth on subsequent obstetric outcome. National Institute of Child Health and Human Development maternal-fetal Medicine Units Network. Am. J. Obstet. Gynecol. 181, 1216–1221 (1999).
Kazemier, B. M. et al. Impact of obstetric history on the risk of spontaneous preterm birth in singleton and multiple pregnancies: a systematic review. BJOG 121, 1197–1208; discussion 1209 (2014).
Goldenberg, R. L., Hauth, J. C. & Andrews, W. W. Intrauterine infection and preterm delivery. N. Engl. J. Med. 342, 1500–1507 (2000).
Nakamura, M. et al. Comparison of perinatal outcomes between long-term and short-term use of tocolytic agent: A historical cohort study in a single perinatal hospital. J. Obstet. Gynaecol. Res. 42, 1680–1685 (2016).
Chmielewska, B. et al. Effects of the COVID-19 pandemic on maternal and perinatal outcomes: A systematic review and meta-analysis. Lancet Glob. Health 9, e759–e772 (2021).
Okawa, S., Hosokawa, Y., Nanishi, K., Zaitsu, M. & Tabuchi, T. Threatened abortion, threatened premature labor, and preterm birth during the first state of emergency for COVID-19 in 2020 in Japan. J. Obstet. Gynaecol. Res. 48, 1116–1125 (2022).
Fazzi, C., Saunders, D. H., Linton, K., Norman, J. E. & Reynolds, R. M. Sedentary behaviours during pregnancy: A systematic review. Int. J. Behav. Nutr. Phys. Act. 14, 32 (2017).
Magro-Malosso, E. R., Saccone, G., Di Tommaso, M., Roman, A. & Berghella, V. Exercise during pregnancy and risk of gestational hypertensive disorders: A systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 96, 921–931 (2017).
Aune, D., Saugstad, O. D., Henriksen, T. & Tonstad, S. Physical activity and the risk of preeclampsia: A systematic review and meta-analysis. Epidemiology 25, 331–343 (2014).
Fan, S. et al. Psychological effects caused by COVID-19 pandemic on pregnant women: A systematic review with meta-analysis. Asian J. Psychiatr. 56, 102533 (2021).
Acknowledgements
The data used in this study was obtained from the Japan Medical Data Center (JMDC, Inc., Tokyo, Japan; JMDC). We appreciate their kind support. We also would like to thank Editage (www.editage.com) for English language editing.
Funding
This study was supported by the Grants-in-Aid for Scientific Research (KAKENHI; 21K09539). The grant provided financial support for the preparation of the article, such as English language editing services and Open Access Publication Fee.
Author information
Authors and Affiliations
Contributions
M.O., S.T., S.T-M., K.K., M.K., K.M., and T.M. are involved in the conception, design, and planning of the study. M.O., S.T-M., and K.K. are involved in data analysis. M.O. drafted the original manuscript. S.T., S.T-M., K.K., M.K., K.M., and T.M. are involved in review and editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ohashi, M., Tsuji, S., Tanaka-Mizuno, S. et al. Amelioration of prevalence of threatened preterm labor during the COVID-19 pandemic: nationwide database analysis in Japan. Sci Rep 12, 15345 (2022). https://doi.org/10.1038/s41598-022-19423-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-19423-x
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
