
Abstract
We estimated mortality and economic loss attributable to PM2·5 air pollution exposure in 429 counties of Iran in 2018. Ambient PM2.5-related deaths were estimated using the Global Exposure Mortality Model (GEMM). According to the ground-monitored and satellite-based PM2.5 data, the annual mean population-weighted PM2·5 concentrations for Iran were 30.1 and 38.6 μg m−3, respectively. We estimated that long-term exposure to ambient PM2.5 contributed to 49,303 (95% confidence interval (CI) 40,914–57,379) deaths in adults ≥ 25 yr. from all-natural causes based on ground monitored data and 58,873 (95% CI 49,024–68,287) deaths using satellite-based models for PM2.5. The crude death rate and the age-standardized death rate per 100,000 population for age group ≥ 25 year due to ground-monitored PM2.5 data versus satellite-based exposure estimates was 97 (95% CI 81–113) versus 116 (95% CI 97–135) and 125 (95% CI 104–145) versus 149 (95% CI 124–173), respectively. For ground-monitored and satellite-based PM2.5 data, the economic loss attributable to ambient PM2.5-total mortality was approximately 10,713 (95% CI 8890–12,467) and 12,792.1 (95% CI 10,652.0–14,837.6) million USD, equivalent to nearly 3.7% (95% CI 3.06–4.29) and 4.3% (95% CI 3.6–4.5.0) of the total gross domestic product in Iran in 2018.
Similar content being viewed by others


Introduction
PM2.5 has been recognized as the leading environmental cause of respiratory-, cardiovascular, and cancer-related deaths worldwide1,2,3,4. Based on the Global Burden of Disease (GBD) study, the number of deaths and crude death rate per 100,000 population attributable to ambient PM2.5 exposures in Iran increased from 36,379 (95% CI 32,140–40,502) and 47 (95% CI 42–53) in 2010 to 41,742 (95% CI 36,156–47,037) and 49 (95% CI 43–56) in 2019, whereas the figure for age-standardized death rate per 100,000 population declined from 74 (95% CI 65–83) to 63 (95% CI 55–71) (https://vizhub.healthdata.org/gbd-compare/). Also, exposure to ambient PM2.5 reduced the average of life expectancy at birth for Iran in the range of 0.76–1.02 years in 20165. Recent estimates predict that global PM2.5-related deaths may double by 20506. Current estimates also suggest that global economic loss attributable to health effects of ambient PM2.5 exposure is substantial and may increase until 20307,8,9. It has been reported that 99% of the global population remain exposed to annual PM2.5 levels above the updated World Health Organization Air Quality Guidelines (WHO AQGs: 5 μg m−3)10. Though ambient PM2.5 concentrations have declined in high-income countries, levels in many low- and middle-income countries (LMICs) remain unchanged or have increased due to largely the lack of strong air quality management policies11,12,13.
Ambient air pollution in Iran as a LMIC has been considered as one of the most important public health risk factor by the government, policy-makers, health authorities, national and even international public health bodies as well as environmental health researchers14,15,16,17. National investigations have been conducted to estimate the health effects of ambient PM2.5 air pollution in Iran16,17. Little, however, is known about both health effect and economic loss attributable to ambient PM2.5 in all Iranian counties. In this context, we designed this study to estimate PM2.5-related health, namely all-cause and cause-specific mortality, such as ischemic heart disease (IHD), cerebrovascular disease (stroke), chronic obstructive pulmonary disease (COPD), lung cancer (LC) and lower respiratory infection (LRI), and YLL and economic loss for 429 counties and 31 provinces of Iran in 2018.
Methods
We used two different but complementary approaches to estimate long-term exposure to ambient PM2.5 and its impact on mortality and economic loss. We initially obtained ambient PM2.5 data from all the available ground-based ambient air quality monitoring stations (AQMSs) across Iran, processed and validated the hourly PM2.5 concentrations and then estimated human exposure. We also used the high-resolution satellite-derived PM2.5 data from the GBD study to estimate human exposure. We then obtained the population data and the national baselines of all-cause mortality and cause specific deaths to estimate the health burden attributable to ambient PM2.5 exposures by using the GEMM function. After that, we estimated the crude death rate and age-standardized death rate per 100,000 population associated with PM2.5 air pollution exposure in the Iranian provinces and counties on the basis of the WHO standard population (https://www.who.int/healthinfo/paper31.pdf). We estimated the economic loss due to ambient PM2.5-related health effects by using two well-documented methods including the value of statistical life (VSL) and the value of life year (VOLY). Finally, we compared our findings that were estimated based on the ground-monitored and satellite-based PM2.5 data.
Study domain
Iran is a country located in the Eastern Mediterranean region and is characterized by diverse geo-climatic areas, ranging from arid and semi-arid to subtropical along the Caspian coast and the northern forests. With nearly 81 million inhabitants in 31 provinces and 429 counties, Iran is the world's 17th most populous country in 2018. Spanning 1,648,195 km2, it is the second largest country in the Middle East and the 17th largest in the world15 (details in Supplementary Text 1).
Estimation of human exposures based on the ground-monitored and satellite-based PM2.5 data
We obtained the real-time hourly data on ambient PM2.5 concentrations from January 1, 2018, to December 31, 2018, from all the available AQMSs provided by the Iranian Department of Environment (DoE) and Tehran Air Quality Control Company (TAQCC). There were 229 AQMSs throughout 70 Iranian counties located in 25 provinces (out of 31) of Iran (Fig. 1). Of the 229 AQMSs, 147 monitored the ambient PM2.5 levels of Iranian counties for the year 2018 (Supplementary Text 2). To remove any inconsistency which might arise owing to operation disruptions at the AQMSs (e.g. routine maintenance activities, communication failures and power outages), hourly data were pre-processed and validated by using Z scores approach (Supplementary Text 3)18,19,20. Prior to the estimation of the health effects and economic loss of PM2.5 for each of 429 counties, the missing hourly PM2.5 data for the included AQMSs were estimated by using the hourly ratio of PM2.5/PM10 according to the available hourly data during the year of study, 2018 (Supplementary Text 4). As mentioned above, we also used the high-resolution satellite-derived PM2.5 data from the GBD study 2017 and 2019 (the average of both years was used for 2018)3,21. Though full details reported elsewhere, note that he GBD study provides datasets for ambient PM2·5 concentrations at a 0·1° × 0·1° resolution (~ 11 × 11 km) that these datasets include approximately 15,800 grids for Iran. To estimate human exposures to PM2.5 for each of 429 Iranian counties, we averaged the ambient PM2·5 concentrations of grids that were within the border of each of counties. Then, we estimated the health effects and economic loss of exposure to ambient PM2·5 for each of counties using the figures averaged. We calculated the population-weighted mean (PWM) PM2·5 concentrations at national level based on both ground-monitored and satellite-based ambient PM2·5 data using the following equation20,22.
where PM2.5 is the mass concentration of ambient PM2.5. Pop is the population number. The suffixes i show each of investigated counties and n is the number of all counties within each province and country.

Spatial distribution of AQMSs across Iranian provinces in 2018 (this figure was generated by ArcGIS v10.7.0.10450).
Mortality baseline and population data
We obtained the population data within each population group for Iranian counties from the Statistical Centre of Iran (https://www.amar.org.ir/english/Population-and-Housing-Censuses). Moreover, national baselines of all-cause mortality and cause specific mortalities (stroke, IHD, COPD, LC and LRI) for each age group were obtained from the Institute for Health Metrics and Evaluation (IHME), GBD web-system (http://ghdx.healthdata.org/gbd-results-tool).
Assessing PM2.5-related burden of disease
We estimated the ambient PM2.5-related health effects (e.g., all-cause mortality and five specific causes of death including IHD, stroke, COPD, LC and LRI) using the BenMAP-CE v1.5 software based on the concentration–response function developed by Burnet et al.23,24 as follow:
-
Global Exposure Mortality Model (GEMM):
$$\mathrm{GEMM }\left(\mathrm{z}\right)=\mathrm{exp}\left\{\frac{\mathrm{\theta ln}(\frac{\mathrm{z}}{\mathrm{\alpha }}+1)}{1+\mathrm{exp}(-\frac{\mathrm{z}-\upmu }{\upnu })}\right\}$$
θ, α, μ, and ν present the shape of response function estimating all-cause mortality and cause specific deaths. Where, Z presents the annual average concentration of ambient PM2.5 for each city; Zcf known counterfactual concentration is the lowest observed concentration in any of the 41 cohorts (2.4 µg m−3) from Canada, United States, Europe and Asia below which no change in the hazard ratio is assumed. The following equation is used to estimate the health burden:
where NPM denotes the number of mortalities in age group caused by ambient PM2.5 for all-cause mortality and cause specific mortalities; BI (baseline incidence) is a certain BI for each of health endpoints within each of population groups and PAF is the population attributable fraction computed by multiplying the population (P) and the relative risks (RRs, based on the GEMM function), as shown in following equation:
YLL
In the present study, the number of YLL was limited to all-cause mortality from long-term exposure to ambient PM2.5 for adults aged ≥ 25 years. We calculated YLL for Iran in 2018 using the following equation17,25:
where LEi and NPMi are the remaining life expectancy and the number of deaths in age group i, respectively. The YLL was the sum of YLL for all age groups. In this analysis, we used life expectancy tables for Iran from the IHME, GBD study (https://vizhub.healthdata.org/gbd-compare/arrow).
Economic valuation estimates
Two approaches (including VSL and VOLY) were used to estimate the economic loss due to ambient air pollution-related health effects8,16,25,26,27. We used the VSL information reported for Co-operation and Development (OECD) countries (the mean VSL for OECD countries equal to 3.833 million USD) because of the lack of national studies on estimating VSL in Iran16,25. We, therefore, adjusted/calculated VSL for our study as follow.
Here, GDPIran and GDPOECD represent the GDP per capita for Iran and OECD countries, respectively. Also, b represents the income elasticity of the VSL for different countries, ranging from 1.0 to 1.4 for low-income and middle-income countries16,25. We used 1.2 (as average of 1.0–1.4) for b in the present study16,25 because the average transfer error is smallest when the central elasticity value of 1.2 is considered28. As reported previously19, GDP for Iran and OECD countries were 3598 and 39,339 USD in 2018, respectively. As a result, based on the aforementioned assumptions, the VSLIran was equal to 217,282 USD for the year 2018. Lastly, the economic costs of health burden was evaluated by multiplying the number of all cause and cause specific mortalities attributable to ambient PM2.5 and adjusted VSL for Iran, as shown in the following equation:
where Mortalitycounty is the number of all-cause and cause-specific deaths attributable to long-term exposure to ambient PM2.5 for each of 429 Iranian counties. Our second approach to valuing premature deaths was to calculate the economic value of YLL due to ambient PM2.5 exposures. Empirical values of VOLY have been either determined using WTP studies or approximated as a multiple of GDP per capita25. For our analysis, we used a VOLY equal to one GDP per capita as follow30:
Results
Overview of ambient PM2.5 concentration and its health and economic impacts at national level in Iran
Figure 2 shows the annual mean PM2.5 concentrations for Iran in 2018. The average (± standard deviation) of PM2.5 concentrations based on the AQMSs and satellite measurements were 31.0 (± 5.2) and 39.2 (± 10.5) μg m−3, respectively, while the PWM PM2·5 concentrations for both approaches were 30.1 (± 7.8) and 38.6 (± 4.7) μg m−3 in 2018. The average difference between both datasets was nearly 8.0 μg m−3. Table 1 provides the results on all cause and cause specific mortalities due to ambient PM2.5 exposures, estimating based on ground and satellite-based datasets. The number of all-cause mortality attributable to long-term exposure to ambient PM2.5 using ground-monitored data was 49,303 (95% CI 40,914–57,379), whereas this figure stood at 58,873 (95% CI 49,024–68,287) using satellite-based data. As shown in Table 1, the highest and lowest number of cause specific deaths due to ambient PM2.5 in Iran was found for IHD [24003 (95% CI 22,051–25,887)] and LC [1884 (95% CI 1180–2502)], respectively when applying ground-monitored data. Similar trend can be reported while using satellite data. PM2.5-related all-cause, IHD, stroke, LRI, COPD and LC deaths were responsible for about 15%, 26%, 17%, 49%, 23% and 26% of those deaths in Iran when applying ground-monitored data. Among five specific causes of death, PM2.5-related IHD and stroke caused about 61% (49% for IHD and 12% for stroke) of total PM2.5-related deaths in Iran. Considering both approaches, the number of all cause and cause specific deaths attributable to ambient PM2.5 exposures has increased with age groups (Figure S2). More than 68% of the total deaths attributable to PM2.5 were from the elderly group (aged 65 or more); nearly 31% in the age group 65–79 years and 37–38% in the age group of 80 and up. Crude death and age-standardized death rates per 100 000 population attributable to ambient PM2.5 exposures in Iran were 97 (95% CI 81–113) and 125 (95% CI 104–145), respectively using ground-monitored approach, while these figures for satellite-based PM2.5 data arose to 116 (95% CI 97–135) and 149 (95% CI 124–173). The economic loss due to the total mortality attributable to ambient PM2.5 air pollution exposures for ground and satellite-based approaches were 10,712.6 (95% CI 8889.9–12,467.4) and 12,792.1 (95% CI 10,652.0–14,837.6) million USD, respectively in Iran (Table 2), equivalent to nearly 3.7% (95% CI 3.06–4.29) and 4.3% (95% CI 3.6–4.5.0) of the total GDP in the country (https://countryeconomy.com/gdp/iran) in 2018. In addition, the economic loss in Iran due to the total mortality attributable to ambient PM2.5 air pollution exposures was nearly 133 and 160 USD per capita per year in 2018 when applying ground and satellite-based approaches.

Annual mean and population-weighted mean (PWM) concentrations for ambient PM2.5 in Iran, 2018, based on ground and satellite data.
Ambient PM2.5-related health and economic impacts at provincial- and county-level in Iran
The number of provincial all cause attributable deaths due to long-term exposure to ambient PM2.5 based on ground and satellite-based data in 2018 is provided in Table 2. Also, the number and proportion of population aged ≥ 25 years, annual PM2.5 mean concentrations and their ratio to WHO AQG as well as the economic loss due to ambient PM2.5-related health impacts at province level are shown in Table 2. Figure 3 indicates data on the annual PM2.5 mean concentrations, crude death rate and age-standardized death rate per 100 000 population attributable to PM2.5 based on ground and satellite approaches in all 429 Iranian counties, 2018. As shown in Table 2 and Fig. 3a,a′, considering both measurement approaches, the population of all 429 counties experienced annual PM2.5 mean concentrations of higher than not only the recommendation value (5 μg m−3) of the new WHO's air quality guideline but also its Interim Targets 4 (10 μg m−3) and 3 (15 μg m−3). As it is evidenced in Fig. 3, both ground and satellite-based data emphasized that the population lived in western provinces (Khuzestan and Ilam) of Iran exposed to annual mean concentration of ambient PM2.5 exceeded even the WHO's Interim Target 1 (35 μg m−3). As such, the top four polluted provinces of Iran in terms of ambient PM2.5 mean concentrations based on ground-based data were Khuzestan (52.6 μg m−3), Ilam (42.7 μg m−3), Kohgiluyeh and Boyer-Ahmad (42.3 μg m−3) and Bushehr (36.3 μg m−3). These figures for satellite-based data changed to Khuzestan (58.4 μg m−3), Ilam (44.6 μg m−3), Kohgiluyeh and Boyer-Ahmad (54.4 μg m−3) and Bushehr (56.6 μg m−3), emphasizing no significant difference between applied approaches except for Bushehr. Based on ground and satellite-based datasets, the lowest concentration of ambient PM2.5 in 2018 was found in the provinces of Ardabil (22.7 versus 28.9 μg m−3), Gilan (23.4 and 28.7 μg m−3) and East Azerbaijan (23.7 and 28. 3 μg m−3), emphasizing a mere 5–6 μg m−3 difference between the applied approaches. Data provided in Table 2 and Fig. 3 reveals that the greatest differences between ground-monitored PM2.5 data and satellite-based ones was found for the province of Sistan and Baluchestan with 27.8 μg m−3, followed by South Khorasan (25.6 μg m−3), Bushehr (20.3 μg m−3), Yazd (19.3 μg m−3) and Isfahan (13.9 μg m−3). In contrast, the smallest differences between both ground-monitored PM2.5 data and satellite-based ones were observed in the provinces of Ilam (1.9 μg m−3), Qazvin (3.5 μg m−3), North Khorasan (3.8 μg m−3) and Zanjan (4.4 μg m−3). As shown in Table 2, considering both ground and satellite-based data, the five provinces with the highest number of all-cause mortality attributable to ambient PM2.5 exposures were Tehran [9899 (95% CI 8224–11,508) versus 10,515 (95% CI 8746–12,210)], Razavi Khorasan [3795 (95% CI 3149–4416) versus 4567 (95% CI 3803–5296)], Isfahan [3509 (95% CI 2909–4088) versus 5015 (95% CI 4189–5800)], Khuzestan [3375 (95% CI 2826–3893) versus 3632 (95% CI 3048–4180)] and Fars [3294 (95% CI 2736–3830) versus 3810 (95% CI 3174–4417)] and they contributed to approximately 48.4% and 46.8% of total mortality due to ambient PM2.5 in 2018, respectively. Applying both ground and satellite-based PM2.5 data, the five lowest number of attributable deaths was found in the provinces of Semnan [419 (95% CI 347–489) versus 537 (95% CI 447–624)], Ilam [430 (95% CI 359–498) versus 436 (95% CI 364–505)], South Khorasan [447 (95% CI 370–522) versus 747 (95% CI 625–863)], Kohgiluyeh and Boyer-Ahmad [459 (95% CI 383–532) versus 555 (95% CI 464–640)] and North Khorasan [489 (95% CI 406–469) versus 528 (95% CI 439–614)] and they contributed less than 3% and 5% of ambient PM2.5-related total mortality in Iran, respectively.

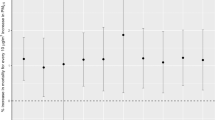
Annual PM2.5 mean concentrations (a,a′), crude death rate (b,b′) and age-standardized death rate (c,c′) per 105 population aged ≥ 25 years old attributable to PM2.5 in all Iranian counties, 2018 (these figures were generated by ArcGIS v10.7.0.10450).
The crude death rate per 100,000 population for Iran is [97 (95% CI 81–113) based on ground-monitored PM2.5 data compared to 116 (95% CI 97–135) based on satellite PM2.5 data], nearly 50% of provinces of Iran had a higher crude death rate (Table 2; Fig. 3b,b′). The five provinces with the highest number of crude death rate per 100,000 population in 2018 in Iran due to PM2.5 were Khuzestan [122 (95% CI 102–140)], Ilam [116 (95% CI 97–135)], Kohgiluyeh and Boyer-Ahmad [110 (95% CI 91–127)], Kermanshah [109 (95% CI 91–127)] and Tehran [108 (95% CI 90–126)] when applying ground-based data, whereas the figures for satellite-based data changed to South Khorasan [171 (95% CI 143–197)], Isfahan [146 (95% CI 122–169)], Yazd [139 (95% CI 116–161)], Kohgiluyeh and Boyer-Ahmad [132 (95% CI 111–153)], and Chaharmahal and Bakhtiari [132 (95% CI 111–153)]. Based on the ground-based PM2.5 data, the lowest figures for the crude death rate per 100,000 population were estimated for the provinces of Sistan and Baluchestan [71 (95% CI 59–83)], Hormozgan [73 (95% CI 61–85)], Alborz [78 (95% CI 64–91)] and West Azerbaijan [82 (95% CI 68–95)], whereas the lowest figures for this rate when applying satellite-based PM2.5 data were observed in the provinces of Hormozgan [85 (95% CI 71–99)], Qazvin [92 (95% CI 76–107)], Golestan [94 (95% CI 78–110)] and West Azerbaijan [96 (95% CI 79–111)]. With regard to age-standardized death rate per 100,000 population using ground-based PM2.5 data (Table 2 and Fig. 3c, the highest figures were estimated for the provinces of Khuzestan [189 (95% CI 158–218)], Ilam [168 (95% CI 140–194)], Kohgiluyeh and Boyer-Ahmad [159 (95% CI 133–185)], Bushehr [140 (95% CI 117–163)] and Kermanshah [137 (95% CI 114–159)], while based on the satellite PM2.5 data (Table 2; Fig. 3c′) the highest figures were estimated for the provinces of Bushehr [205 (95% CI 172–236)], Khuzestan [203 (95% CI 170–234)], Sistan and Baluchestan [194 (95% CI 163–224)], Kohgiluyeh and Boyer-Ahmad Bushehr [193 (95% CI 161–222)] and South Khorasan [186 (95% CI 155–214)]. Based on both approaches, among all 429 counties, Tehran (located in Tehran province) experienced the largest attributable deaths [7802 (95% CI 6840–9072)] to ambient PM2.5, followed by the counties of Mashhad [1870 (95% CI 1573–2203)], Isfahan [1517 (95% CI 1258–1768)], Shiraz [1297 (95% CI 1078–1508)] and Ahvaz [939 (95% CI 788–1082)] which were located in the provinces of Razavi Khorasan, Isfahan, Fars and Khuzestan, respectively. As shown in Table 2, by far the greatest economic loss (based on the VSL) was estimated for Tehran province with 2150.9 (1787.0–2500.5) million USD, followed by the provinces of Razavi Khorasan [824.5 (95% CI 684.2–959.6)], Isfahan [762.5 (95% CI 632.1–888.2)], Khuzestan [733.3 (95% CI 614.0–846.0)] and Fars [715.7 (95% CI 594.5–832.3)].
Figure S4 shows the differences of ambient PM2.5 and the number of all cause deaths due to ambient PM2.5 between both approaches (ground-based data minus satellite ones) in all 429 Iranian counties, 2018. We observe some differences in the ambient PM2.5 and attributable deaths throughout Iran when applying both datasets. In some regions the concentrations of PM2.5 were lower than those reported by satellite data resulting in negative difference values. The lowest differences were observed in the western and north-west provinces and counties of Iran, whereas the greatest differences for both datasets were found in the central and eastern regions of Iran.
Age-specific YLL and VOLY attributable to PM2.5 in Iran and its provinces
Table S1 gives the calculated age-specific YLL and VOLY (× 106 USD) attributable to ambient PM2.5 exposures in Iran (2018), based on the estimated total mortality from GEMM function and IHME life expectancy table. The YLL attributable to both ground-monitored PM2.5 data minus satellite-based ones in Iran was 833,692 (95% CI 693,020–968,773) and 994,063 (95% CI 829,366–1,150,989) in 2018. Among the age groups, as might be expected, the highest and lowest YLL was estimated for the age group 25–29 and 80–99-year-olds, respectively. The sum of VOLY in Iran in 2018 was 3000 (95% CI 2493–3486) and 3577 (95% CI 2984–4141) million USD. On the provincial level, Tehran as the most populous province of Iran had by far the greatest YLL at all age groups [167948 (95% CI 139,763–194,946) and 178,439 (95% CI 148,677–206,873) when using ground and satellite-based PM2.5 data, respectively] and VOLY [604 (95% CI 503–701) and 642 (95% CI 535–744) million USD].
Discussion
This is study is the first to estimate the health burden and economic loss due to exposure to ambient PM2.5 in Iran using both ground-monitored and satellite-based data. While there were some differences between the concentrations of PM2.5 and their related health impacts and economic loss, especially in those areas with lower number of AQMSs, the outcomes of both approaches have shown significant consistency. This should be reassuring not only to Iranian scientists and policy makers but also to those in other LMICs which lack comprehensive monitoring data and may wish to use satellite-based estimates in science and policy. Based on both PM2.5 datasets, the annual PM2.5 concentration and also its PWM were approximately 6–8 times higher than the recommendation value of the updated WHO AQGs (5 μg m−3)29,30,31. Our results showed that the ambient PM2.5 exposure concentrations had large geographical variations across Iran, suggesting a substantial spatial heterogeneity of air pollution sources in Iran, which was in agreement with previously conducted studies16,32. In other words, exposure to ambient PM2.5 concentrations varied markedly across Iranian counties with the ratio of highest to lowest annual mean nearly 3 in 2018. Among the top 100 counties with the highest annual ambient PM2.5, we can mostly see the counties in the provinces of Khuzestan, Ilam, Kermanshah, Lorestan, Chaharmahal and Bakhtiari, Fars, Bushehr, Tehran, and Isfahan. The underlying reasons of higher annual ambient PM2.5 concentrations across Iranian counties than the annual level of WHO AQGs and national standard value may be more likely due to continuing urbanization and industrialization, increasing mobile sources and associated emissions alongside ineffective ambient air quality standards and ambient air pollution abatement policies at national and subnational levels in Iran, all of which collectively amount to unsustainable development in Iran14,15,17,32,33. There were higher concentrations across the western and south western provinces of Iran in comparison to other parts due to dust storm events, particularly throughout the months of spring and summer seasons16,32,34,35,36. Dust storms originating from the arid regions of Iraq and Syria countries, including Tigris and Euphrates basin affect many regions of the western (Kermanshah, Ilam, and Lorestan) and south-western provinces (Khuzestan and Bushehr) of Iran34,37,38. Additionally, based on Hybrid Single-Particle Lagrangian Integrated Trajectory model used by previous studies in Iran, dust storm phenomenon originating each of the aforementioned sources affect central and even other provinces of Iran including Tehran, Shiraz, Isfahan, Arak, and Tabriz39,40. In addition to the aforementioned reasons, the ambient air quality of Khuzestan, Bushehr and Hormozgan provinces located along the bank of Persian Gulf and known as the most important industrialized provinces of Iran are also affected by other sources such as the major gas and petrochemical industries as well as ship traffics35,41,42,43. Hamoun lake located in the north part of the Sistan Basin in the southeast part of Iran acts as local source of dust storm affecting the southeast and eastern provinces and counties of Iran 44,45,46. This is consistent with the satellite-based PM2.5 data.
It worth to mentioned that although in the present study we focus on mortality outcomes and the vast majority deaths attributable to ambient air pollution occur in adults ≥ 25 years25,47,48, air pollution exposure also affects children e.g., via effects on LRI, asthma and pre-term birth and, therefore our work should not be mis-interpreted as proving a comprehensive estimate of all adverse effects of air pollution exposure.
Based on ground-monitored and satellite-based data, total mortality attributable to ambient PM2.5 in Iran was approximately 49,300 and 58,870 (out of 332,000 deaths recorded by the governmental organizations in our country) in 2018, respectively. YLL related to premature deaths in Iran were equivalent to the death of approximately 11 and 13 thousand children at birth. National crude death rate and age-standardized per 100 000 population attributable to ambient PM2.5 air pollution was 97 (95% CI 81–113) versus 116 (95% CI 97–135) and 125 (95% CI 104–145) versus 149 (95% CI 124–173) in 2018 using ground-monitored and satellite-based PM2.5 data, respectively. The differences between the 2 estimates could be likely due to one major factor—changes in the PM2.5 concentrations between the ground-monitored and satellite-based data because other used variables for estimations were the same49. Similar to spatial variability of ambient PM2.5 air pollution, PM2.5-related all cause and cause specific mortalities per 100,000 population had a considerable inequity throughout Iran. The observed differences are mainly due to ambient PM2.5 exposure levels, the distribution of the population and the proportion of population aged > 65 years in total population as the most important factor to affect mortality rate (Figure S3). Note that the ambient PM2.5-related all cause and cause specific mortalities per 100,000 population in the provinces with high proportion of population aged > 65 years in total population were higher than those of other counties even with the lower ambient PM2.5 exposure levels (Figure S3). Based on the estimate of the GBD study for our country, ambient PM2.5 caused approximately 39,836 (95% CI 34,477–44,833) all cause deaths for aged ≥ 25 years in 2018 (https://vizhub.healthdata.org/gbd-compare/). The difference of all cause deaths between our approach and GBD study can be attributed to the shape of concentration–response functions for all-cause of death in the GEMM and Integrated Exposure Response functions used by GBD study. Additionally, this difference is mainly due the fact that the all-cause mortality estimates in GEMM include all non-accidental deaths but the GBD estimates are based on a smaller group of causes (IHD, Stroke, COPD, LRI, LC, Diabetes and infant mortality)23,24,47,50. Regarding the GBD study, national crude death rate and age-standardized per 100,000 population aged ≥ 25 years attributable to ambient PM2.5 air pollution for Iran was 77 (95% CI 68–85) and 97 (95% CI 86–107) in 2018, respectively (http://ghdx.healthdata.org/gbd-results-tool).
In our study, the highest number of deaths was found for IHD, followed by Stroke, LRI, COPD and LC. In other words, cardiovascular and cerebrovascular disease (IHD and stroke) accounted for the majority of the deaths (nearly 61%) attributable to ambient PM2.5 air pollution. This is similar to the proportion of PM2.5-attributable mortality of IHD and stroke reported by the previous studies for China and the GBD study for the entire world51. The comparison among age groups and different causes of death indicates that the elderly age groups and those with cardiovascular and cerebrovascular disease are much more vulnerable and sensitive to ambient PM2.5 air pollution. This highlights to allocate more attention for protecting them from long- and even short-term exposure to ambient PM2.5. Based on our findings, the national and sub-national environmental and health authorities should much more focus on the provinces and counties with high proportion of population aged > 65 years (Figure S3) to enhance the efforts on risk management, resource allocation and air quality status.
Based on our findings and the previously conducted studies16,17,18, the residents of all provinces and counties of Iran have been, and continue to be, exposed to health-damaging levels of ambient PM2.5 over the three past decades. Although ambient air pollution in Iran is recognized to be a serious issue by civil society, researchers and policy-makers, there has been little progress in reducing ambient exposure, which levels remain largely unchanged (https://www.stateofglobalair.org/data/#/air/plot)15,16,17. Despite this the Iranian Department of Environment (DoE) released a revised national ambient air quality standard (NAAQS) in August 2017, in which the annual and daily PM2.5 standard increased (12 and 35 μg m−3, respectively) relative to the previous NAAQS (10 and 25 μg m−3), which was based on the WHO AQG 200518,52. Since then, the WHO has further lowered its PM2.5 AQG based on the latest scientific evidence and offered guidance to governments seeking to reduce air pollution exposure and attributable mortality, including short- and long-term measures to reduce ambient air pollution and its health burden that have been successfully applied in other countries to reduce ambient air pollution-related health impacts and corresponding economic loss (https://www.who.int/news/item/22-09-2021-new-who-global-air-quality-guidelines-aim-to-save-millions-of-lives-from-air-pollution). Such approaches include shifting to clean fuels, transportation reform, reducing traffic emission(s) from vehicles and other major sources, urban landscape reform, emission trading programs, redirection of science and funding, empowering civil society, governmental and NGO-led publicity1,13,53,54,55,56,57. When part of comprehensive air quality management programs such approaches have proven effective in decreasing ambient PM2.5 concentrations and improving public health, but their implementation poses great challenges in many LMICs where economic development and poverty reduction have often relied on heavily-polluting economic activities57,58,59,60.
Our study has some limitations. Firstly, AQMSs were not widely available in all 429 counties of Iran and we inevitably used the estimated concentrations of ambient air pollutant based on neighbor stations as the proxy for population exposures, maybe leading to exposure estimation errors. Secondly, the national-level baseline mortality data was used and more elaborate data has not yet been available in Iran. Thirdly, some of the data required for health and economic burdens were borrowed/estimated from the international studies, which were mostly carried out in other countries. Another reason to do the sensitivity analysis using the GBD 2017 and 2019 exposure estimates for 2018. In terms of the relative risks borrowed to estimate health burden, the origin of ambient PM2.5 and its chemical and toxicological effects and even the susceptibility of population in Iran might be different from those in other countries that cohort studies have been conducted. However, to date, scientific evidence has been unable to accurately estimate the relative risk of various chemical forms or sources of ambient PM2.5 around all the world.
References
Rajagopalan, S., Al-Kindi, S. G. & Brook, R. D. Air pollution and cardiovascular disease: JACC state-of-the-art review. J. Am. Coll. Cardiol. 72, 2054–2070 (2018).
Tian, Y. et al. Ambient particulate matter pollution and adult hospital admissions for pneumonia in urban China: A national time series analysis for 2014 through 2017. PLoS Med. 16, e1003010 (2019).
McDuffie, E. E. et al. Source sector and fuel contributions to ambient PM2.5 and attributable mortality across multiple spatial scales. Nat. Commun. 12, 1–12 (2021).
Southerland, V. A. et al. Global urban temporal trends in fine particulate matter (PM2· 5) and attributable health burdens: Estimates from global datasets. Lancet Planet. Health 25, 25 (2022).
Apte, J. S., Brauer, M., Cohen, A. J., Ezzati, M. & Pope, C. A. III. Ambient PM2.5 reduces global and regional life expectancy. Environ. Sci. Technol. Lett. 5, 546–551 (2018).
Lelieveld, J., Evans, J. S., Fnais, M., Giannadaki, D. & Pozzer, A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 525, 367–371 (2015).
Lanzi, E., Dellink, R. & Chateau, J. The sectoral and regional economic consequences of outdoor air pollution to 2060. Energy Econ. 71, 89–113 (2018).
Maji, K. J., Ye, W.-F., Arora, M. & Nagendra, S. S. PM2.5-related health and economic loss assessment for 338 Chinese cities. Environ. Int. 121, 392–403 (2018).
Landrigan, P. J. et al. The Lancet Commission on pollution and health. Lancet 391, 462–512 (2018).
Faridi, S. et al. Effects of respirators to reduce fine particulate matter exposures on blood pressure and heart rate variability: A systematic review and meta-analysis. Environ. Pollut. 20, 119109 (2022).
Faridi, S. et al. Can respirator face masks in a developing country reduce exposure to ambient particulate matter?. J. Expos. Sci. Environ. Epidemiol. 20, 1–12 (2020).
Barn, P. et al. The effect of portable HEPA filter air cleaner use during pregnancy on fetal growth: The UGAAR randomized controlled trial. Environ. Int. 121, 981–989 (2018).
Hadley, M. B., Baumgartner, J. & Vedanthan, R. Developing a clinical approach to air pollution and cardiovascular health. Circulation 137, 725–742 (2018).
Amini, H. et al. Short-term associations between daily mortality and ambient particulate matter, nitrogen dioxide, and the air quality index in a Middle Eastern megacity. Environ. Pollut. 254, 113121 (2019).
Danaei, G. et al. Iran in transition. Lancet 393, 1984–2005 (2019).
Hadei, M. et al. Burden of mortality attributed to PM2.5 exposure in cities of Iran; contribution of short-term pollution peaks. Atmos. Environ. 20, 117365 (2020).
Shamsipour, M. et al. National and sub-national exposure to ambient fine particulate matter (PM2.5) and its attributable burden of disease in Iran from 1990 to 2016. Environ. Pollut. 255, 113173 (2019).
Faridi, S. et al. Spatial homogeneity and heterogeneity of ambient air pollutants in Tehran. Sci. Total Environ. 697, 134123 (2019).
Yousefian, F. et al. Temporal variations of ambient air pollutants and meteorological influences on their concentrations in Tehran during 2012–2017. Sci. Rep. 10, 1–11 (2020).
Song, C. et al. Air pollution in China: Status and spatiotemporal variations. Environ. Pollut. 227, 334–347 (2017).
Murray, C. J. et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 396, 1223–1249 (2020).
De Hoogh, K. et al. Spatial PM2.5, NO2, O3 and BC models for Western Europe-evaluation of spatiotemporal stability. Environ. Int. 120, 81–92 (2018).
Burnett, R. et al. Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proc. Natl. Acad. Sci. 115, 9592–9597 (2018).
Burnett, R. & Cohen, A. Relative risk functions for estimating excess mortality attributable to outdoor PM2.5 air pollution: Evolution and state-of-the-art. Atmosphere 11, 589 (2020).
Bayat, R. et al. Health impact and related cost of ambient air pollution in Tehran. Environ. Res. 176, 108547 (2019).
Guan, Y., Kang, L., Wang, Y., Zhang, N.-N. & Ju, M.-T. Health loss attributed to PM2.5 pollution in China’s cities: Economic impact, annual change and reduction potential. J. Clean. Prod. 217, 284–294 (2019).
Yin, H. et al. Population ageing and deaths attributable to ambient PM2.5 pollution: A global analysis of economic cost. Lancet Planet. Health 5, e356–e367 (2021).
Narain, U. & Sall, C. Methodology for valuing the health impacts of air pollution (2016).
Amini, H. WHO air quality guidelines need to be adopted. Int. J. Public Health 66, 25 (2021).
Khomenko, S. et al. Health impacts of the new WHO air quality guidelines in European cities. Lancet Planet. Health 5, e764 (2021).
Organization, W. H. WHO global air quality guidelines: Particulate matter (PM2.5 and PM10), ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide (2021).
Shahsavani, A. et al. Short-term effects of particulate matter during desert and non-desert dust days on mortality in Iran. Environ. Int. 134, 105299 (2020).
Amini, H. et al. Spatiotemporal description of BTEX volatile organic compounds in a Middle Eastern megacity: Tehran study of exposure prediction for environmental health research (Tehran SEPEHR). Environ. Pollut. 226, 219–229 (2017).
Boloorani, A. D., Kazemi, Y., Sadeghi, A., Shorabeh, S. N. & Argany, M. Identification of dust sources using long term satellite and climatic data: A case study of Tigris and Euphrates basin. Atmos. Environ. 224, 117299 (2020).
Karimi, A. et al. Concentrations and health effects of short-and long-term exposure to PM2.5, NO2, and O3 in ambient air of Ahvaz city, Iran (2014–2017). Ecotoxicol. Environ. Saf. 180, 542–548 (2019).
Naimabadi, A. et al. Chemical composition of PM10 and its in vitro toxicological impacts on lung cells during the Middle Eastern Dust (MED) storms in Ahvaz, Iran. Environ. Pollut. 211, 316–324 (2016).
Boloorani, A. D. et al. Investigation of dust storms entering Western Iran using remotely sensed data and synoptic analysis. J. Environ. Health Sci. Eng. 12, 124 (2014).
Soleimani, Z. et al. An overview of bioaerosol load and health impacts associated with dust storms: A focus on the Middle East. Atmos. Environ. 223, 117187 (2020).
Hassanvand, M. S. et al. Indoor/outdoor relationships of PM10, PM2.5, and PM1 mass concentrations and their water-soluble ions in a retirement home and a school dormitory. Atmos. Environ. 82, 375–382 (2014).
Sotoudeheian, S., Salim, R. & Arhami, M. Impact of Middle Eastern dust sources on PM10 in Iran: Highlighting the impact of Tigris-Euphrates basin sources and Lake Urmia desiccation. J. Geophys. Res. Atmos. 121, 14018–14034 (2016).
Akhbarizadeh, R. et al. Suspended fine particulate matter (PM2.5), microplastics (MPs), and polycyclic aromatic hydrocarbons (PAHs) in air: Their possible relationships and health implications. Environ. Res. 192, 110339 (2021).
Arfaeinia, H. et al. The effect of land use configurations on concentration, spatial distribution, and ecological risk of heavy metals in coastal sediments of northern part along the Persian Gulf. Sci. Total Environ. 653, 783–791 (2019).
Heidari, M., Darijani, T. & Alipour, V. Heavy metal pollution of road dust in a city and its highly polluted suburb; Quantitative source apportionment and source-specific ecological and health risk assessment. Chemosphere 20, 129656 (2021).
Beyranvand, A., Azizi, G., Alizadeh-Choobari, O. & Boloorani, A. D. Spatial and temporal variations in the incidence of dust events over Iran. Nat. Hazards 97, 229–241 (2019).
Rashki, A., Rautenbach, C. D., Eriksson, P. G., Kaskaoutis, D. G. & Gupta, P. Temporal changes of particulate concentration in the ambient air over the city of Zahedan, Iran. Air Qual. Atmos. Health 6, 123–135 (2013).
Rashki, A., Kaskaoutis, D., Goudie, A. & Kahn, R. Dryness of ephemeral lakes and consequences for dust activity: The case of the Hamoun drainage basin, southeastern Iran. Sci. Total Environ. 463, 552–564 (2013).
Burnett, R. T. et al. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ. Health Perspect. 122, 397–403 (2014).
Lelieveld, J. et al. Loss of life expectancy from air pollution compared to other risk factors: A worldwide perspective. Cardiovasc. Res. 116, 1910–1917 (2020).
Ghosh, R. et al. Ambient and household PM2.5 pollution and adverse perinatal outcomes: A meta-regression and analysis of attributable global burden for 204 countries and territories. PLoS Med. 18, e1003718 (2021).
Hystad, P., Yusuf, S. & Brauer, M. (Oxford University Press, 2020).
Wang, Q., Wang, J., He, M. Z., Kinney, P. L. & Li, T. A county-level estimate of PM2.5 related chronic mortality risk in China based on multi-model exposure data. Environ. Int. 110, 105–112 (2018).
Joss, M. K., Eeftens, M., Gintowt, E., Kappeler, R. & Künzli, N. Time to harmonize national ambient air quality standards. Int. J. Public Health 62, 453–462 (2017).
Brook, R. D., Newby, D. E. & Rajagopalan, S. The global threat of outdoor ambient air pollution to cardiovascular health: Time for intervention. JAMA Cardiol. 2, 353–354 (2017).
Hadley, M. B., Vedanthan, R. & Fuster, V. Air pollution and cardiovascular disease: A window of opportunity. Nat. Rev. Cardiol. 15, 193 (2018).
Al-Kindi, S. G., Brook, R. D., Biswal, S. & Rajagopalan, S. Environmental determinants of cardiovascular disease: Lessons learned from air pollution. Nat. Rev. Cardiol. 17, 656–672 (2020).
Bard, R. L. et al. Interventions to reduce personal exposures to air pollution: A primer for health care providers. Glob. Heart 14, 47–60 (2019).
Kaufman, J. D. et al. Guidance to reduce the cardiovascular burden of ambient air pollutants: A policy statement from the American Heart Association. Circulation 142, e432–e447 (2020).
Faridi, S. et al. Cardiovascular health effects of wearing a particulate-filtering respirator to reduce particulate matter exposure: A randomized crossover trial. J. Human Hypertens. 20, 1–11 (2021).
Langrish, J. P. et al. Reducing personal exposure to particulate air pollution improves cardiovascular health in patients with coronary heart disease. Environ. Health Perspect. 120, 367–372 (2012).
Rajagopalan, S. & Landrigan, P. J. Pollution and the Heart. N. Engl. J. Med. 385, 1881–1892 (2021).
Acknowledgements
This work was funded by the National Institute for Medical Research Development; NIMAD; and Tehran University of Medical Sciences; TUMS; (Grant number for NIMAD: 983249 and Grant numbers for TUMS 1400-3-110-55912 and 99-3-110-50363). The authors are grateful to the Iranian Department of Environment (DoE) and Tehran Air Quality Control Company (TAQCC) for providing ambient air pollutant concentrations data. HA is supported by Novo Nordisk Foundation Challenge Programme (NNF17OC0027812).
Author information
Authors and Affiliations
Contributions
S.F., M.S.H., R.B., A.J.C., and J.R.B. developed the research idea and framework. M.S.H., S.F., and A.J.C. provided data. R.B. was responsible for calculations related to the health and economic impacts of air pollution in this study and S.F., M.S.H., H.A., K.N. and M.S.H.P. managed the process of calculations in detail. R.B., S.F., E.S.H.K.H., M.S.H., and M.S.H.P. contributed to generation of figures and tables. S.F. and S.N. had primary responsibility for writing the manuscript, to which all authors contributed. M.S.H., S.F., and A.J.C. verified the data underlying this study.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Faridi, S., Bayat, R., Cohen, A.J. et al. Health burden and economic loss attributable to ambient PM2.5 in Iran based on the ground and satellite data. Sci Rep 12, 14386 (2022). https://doi.org/10.1038/s41598-022-18613-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-18613-x
This article is cited by
-
Premature mortality risk and associated economic loss assessment due to PM2.5 exposure in Delhi, India during 2015–2019
Air Quality, Atmosphere & Health (2024)
-
Relationship between fine particulate matter (PM2.5) concentration and risk of hospitalization due to chronic obstructive pulmonary disease: a systematic review and meta-analysis
BMC Public Health (2023)
-
Investigating PM2.5 toxicity in highly polluted urban and industrial areas in the Middle East: human health risk assessment and spatial distribution
Scientific Reports (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
