
Abstract
Asthma affects 340 million people worldwide and varies in time. Twenty years ago, in Canada, the Saguenay–Lac-Saint-Jean asthma family cohort was created to study the genetic and environmental components of asthma. This study is a follow-up of 125 participants of this cohort to explore the appearance, persistence, and progression of asthma over 10–20 years. Participants answered a clinical standardized questionnaire. Lung function was assessed (forced expiratory volume in 1 s, forced vital capacity, bronchial reversibility, and methacholine bronchoprovocation), skin allergy testing was performed, blood samples were obtained (immunoglobulin E, white blood cell counts) and phenotypes were compared between recruitment and follow-up. From the participants without asthma at recruitment, 12% developed a phenotype of adult-onset asthma with the presence of risk factors, such as atopy, high body mass index, and exposure to smoking. A decrease of PC20 values in this group was observed and a decrease in the FEV1/FVC ratio in all groups. Also, 7% of individuals with asthma at recruitment developed chronic obstructive pulmonary disease, presenting risk factors at recruitment, such as moderate-to-severe bronchial hyperresponsiveness, exposure to smoking, and asthma. This study allowed a better interpretation of the evolution of asthma. Fine phenotypic characterization is the first step for meaningful genetic and epigenetic studies.
Similar content being viewed by others


Introduction
Nearly 340 million people around the world were affected by asthma according to the Global Burden of Disease Study in 20161, making it one of the most common chronic diseases worldwide. In Canada, 3.8 million people live with asthma2. The prevalence of asthma continues to increase in low-to-middle-income countries, whereas in high-income countries it seems to have peaked because of improved asthma control or reduced incidence3.
Asthma is a chronic inflammatory disease of the respiratory tract characterized by airway hyperresponsiveness (AHR) and airway obstruction4. It can affect people of all ages and vary over time. Some people develop asthma during childhood and see their symptoms disappear in their teenage years, while others develop the disease in adulthood5. These symptoms can be triggered by several factors, such as exposure to allergens in sensitized people and irritating agents (smoke, strong smells, or exhaust fumes), exercising, and changing seasons, as well as respiratory infections4. Environmental stimuli may trigger an inflammatory cascade driven by T-helper type 2 (TH2) cells in asthmatic patients6,7, leading to narrowing of bronchi lumen, which is reflected by a decrease in forced expiratory volume in 1 s (FEV1) in spirometry testing. AHR can be estimated by the PC20, the methacholine concentration inducing a 20% decrease in FEV1. Furthermore, persistent airflow limitation, defined as a reduced ratio of FEV1 to forced vital capacity (FVC) post-bronchodilator, can develop in a subgroup of patients with adult-onset asthma8. A reduced FEV1 to FVC ratio (below 0.70) is also observed in chronic obstructive pulmonary disease (COPD)9.
Asthma is a multifactorial disorder. Since asthma development and progression are influenced by various genetic and environmental factors, the pathogenesis and natural history of this disease are not well understood10. Longitudinal studies are required to discover the evolution of asthma over time11. Many studies have investigated the atopic march and featured childhood asthma, which helped establish a better picture of the situation12,13. An improved characterization of the various phenotypes in adults would facilitate a greater understanding of the clinical evolution of the disease and its persistence, create a better representation of asthma in an adult population over time, and may identify new therapeutic strategies.
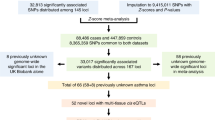
Recruitment to the Saguenay–Lac-Saint-Jean (SLSJ) asthma family cohort began 20 years ago to study the influence of the genetic determinants on asthma and its persistence over time14 (Fig. 1). Since we focused on the genetics of allergic asthma, we recruited affected probands and their parents, with the consequence that the majority of the asthmatic individuals are allergic and have mild-to-moderate asthma. The present study evaluates the respiratory condition of a subsample of the SLSJ asthma family cohort, using the same clinical procedures (health questionnaire, spirometry, and skin prick test) to study the evolution of the disease 10–20 years after their first visit. The objective of this study was to assess changes in asthma status and other respiratory or clinical parameters.

Timeline of the SLSJ asthma family cohort. Stages in the acquisition of phenotypic, genomic, and epigenomic data for the SLSJ family cohort. Description of approaches used at each stage: 1.–3. Standardized questionnaire, respiratory measurements, blood samples (IgE, differential white blood cell counts, and DNA), 2. Microsatellite markers, 4. Illumina 610 K-Quad chip, 5. Infinium Human Methylation 450 K chip (white blood cells and eosinophils), 6. Isolation of naive CD4+ T cells and eosinophils for DNA and RNA extraction for methylome and transcriptome (methylome sequencing with custom methyl capture panel [MCC-Seq] and RNA sequencing), 7. Standardized questionnaire, respiratory measurements, blood samples (IgE, differential white blood cell counts, DNA, RNA, and plasma), 8. MCC-Seq (white blood cells). Between 2001 and 2010, candidate gene studies were performed with genetic variants, expression, and methylation data.
Methods
Study population
The first phase of recruitment for the SLSJ cohort was from 1997 to 2003 and 2006–2007. It consisted of 1394 individuals from 271 independent families14. Recruitment was conducted through probands and then included all family members who wanted to participate in the study. Additional detail on recruitment is provided in the Supplementary File 1 (in the study population section). The present study was realized 20 years after the first recruitment phase (from 2016 to 2019). A total of 215 participants were selected in the context of another project and the follow-ups were done at the same time. There were initially 156 participants in the follow-up research project. Among them, 31 participants were children at recruitment, i.e., 16 years old and younger (the age corresponding to adult asthma). The remaining 125 individuals (80%), comprising 58 men and 67 women, agreed to participate in the two required visits to reassess their respiratory condition. Thus, only the adult participants at recruitment and follow-up were kept to perform analyses on an adult population only, therefore preventing mixing of children and adult clinical measures. Informed consent was obtain from all participants and/or their legal guardians at recruitment, in accordance with the rules of the ethics committee of the Centre intégré universitaire de santé et de services sociaux (CIUSSS) du Saguenay‒Lac-Saint-Jean (project #0002-001). This committee also approved experimental protocols including questionnaires, respiratory measures and skin prick tests.
Measurements and definitions of outcomes
In this longitudinal study, a clinical standardized respiratory questionnaire was completed (modified from15). The questionnaire evaluated many elements regarding asthma and related phenotypes that are self-reported such as age of onset of asthma, allergies, respiratory symptoms, medication, health habits, family history, environmental exposures, and comorbidities. Thereafter, respiratory measurements were carried out according to the guidelines of the American Thoracic Society16. FEV1, PC20 and bronchodilator (BD) reversibility test were performed to assess lung function parameters14. Allergy was assessed using skin prick test for 27 allergens including animal dander, indoor and outdoor aeroallergens, as well as food allergens (see “Supplementary File” in the data collection section). Participants were considered atopic if they exhibited at least one positive response as defined by a wheal diameter ≥ 3 mm and > 50% of positive control (histamine) reaction after 10 min. Blood samples were collected from each participant to measure serum IgE levels, white blood cell counts (basophils, eosinophils, lymphocytes, monocytes, and neutrophils), as well as to perform DNA and RNA extraction and collect plasma samples for further studies14. Data were also collected at the archives of Chicoutimi hospital (CIUSSS) for 123 of the 125 participants; two of them did not have records at this hospital. Information on asthma and COPD diagnosis were considered. Only data from the standardized respiratory questionnaire and clinical assessment at follow-up were used for the two participants with no records at the CIUSSS.
Statistical analyses
Statistical analyses were performed using the SPSS Statistics 25.0 (IBM SPSS Statistics, Version 25.0. Armonk, NY: IBM Corp). Normal distribution was verified for all groups tested, and parametric or non-parametric tests were performed accordingly. A log10- transformation was used to render total serum IgE levels and PC20 concentration distributions approximately normal. To analyze the differences between groups at recruitment and follow-up, T-test and Wilcoxon test for matched data were conducted for continuous variables and Chi-square or Fisher’s exact test for categorical data. In Table 1, the differences were measured for each group, i.e., the All participants, the No asthma, and the Asthma groups, between recruitment and follow-up and thus for each parameter. Analyses were performed in order to measure possible associations between variables. Spearman Rho correlations were used between all variables. Multiple linear regression models were also tested to identify variables explaining significant differences between recruitment and follow-up that were found in previous analyses, with models having identified variable with significant differences as dependent variable and values of likely explanatory variables at first recruitment as independent variables. P-values < 0.05 were considered significant.
Ethics declarations
All participants provided written consent for their participation, in accordance with the rules of the ethics committee of the Centre intégré universitaire de santé et de services sociaux (CIUSSS) du Saguenay‒Lac-Saint-Jean (project #0002-001).
Results
Table 1 presents the phenotypic description of the participants at recruitment and at follow-up and is divided into three groups (All participants, No asthma, and Asthma) according to the asthma status of participants at recruitment. The subsample of 125 participants included 58 men and 67 women. At recruitment, the age of these individuals ranged from 17 to 68 years (mean of 41 years). At follow-up, participants were aged 27–83 years (mean, 58 years). BMI values increased from 24.96 at recruitment to 27.06 at follow-up (p < 0.0001) and the number of smokers displayed a marked decrease at follow-up from 22 to four participants (p < 0.001).
Changes of asthma phenotype
As depicted in Table 1, 54% of the individuals, i.e., 30 men and 38 women, had asthma at recruitment. Based on asthma diagnoses validated by a physician, three women and four men developed asthma between recruitment and follow-up, all of them developing adult-onset asthma (> 16 years-old). This is a 12% status change among the 57 participants without asthma at recruitment. The mean age of onset was 43 years (see the No asthma group of the follow-up section in Table 1). They included two men and two women with obesity (BMI > 30), five smokers or ex-smokers and five participants with atopy (Table 2). In addition, three individuals observed the disappearance of asthma symptoms during the same period; however, they are still considered to have asthma as the individuals who revert to a non-asthmatic phenotype and never experience asthma symptoms again are rare (Table 3)5.
Changes have been observed in different indices of asthma severity. The severity of asthma from very mild to very severe was compared based on data collected using the questionnaire during the follow-up period. Between recruitment and follow-up, there was an increase in the number of participants who characterized their asthma as being very mild, from two to 12 individuals (χ2 p < 0.05, Fig. 2A and Supplementary Table S1). Amongst the individuals with new very mild asthma status, six categorized their asthma as mild, four as moderate, and the others had missing values at recruitment. In contrast, a decrease in the number of participants in the moderate asthma category was observed, from 16 to 10 individuals (χ2 not significant, Fig. 2A). Besides the four who now characterized their asthma as very mild, another considered its asthma as severe at recruitment. Additionally, 17 individuals perceived no change in their asthma severity. However, 28 individuals at recruitment and 30 individuals at follow-up had missing values for the asthma severity question. About asthma prescription medication, their use has increased in some categories between recruitment and follow-up. There was an increase of 31% in the number of individuals with asthma who take long-acting beta-agonists as their asthma medication combined in one inhaler with inhaled corticosteroids (ICSs) (χ2 p < 0.0001) but no significant changes were observed for those taking ICSs as a monotherapy or with an inhaler with short-acting beta-agonists or long-acting beta-agonists (Fig. 2B and Supplementary Table S2). New molecules have been developed over the past decades such as long-acting muscarinic antagonists and were added to the medication list of seven participants with asthma at follow-up. No targeted biologics were used by the Asthma group (anti-IgE, anti-interleukin (IL) 4 or anti-IL5).

Asthma severity over time. (A) Participants classified the severity of their disease using a self-reported questionnaire. (B) The use of prescription medication for asthma control evolved between recruitment and follow-up. p values < 0.05 are indicated by an asterisk and p values < 0.0001 are indicated by three asterisks.
Significant decreases in the All group were observed for FEV1/FVC pre- and post-BD (3–4% of decline, p < 0.0001, Fig. 3A,B). Therefore, analyses were done to explain this decrease with other clinical parameters. Correlations between FEV1/FVC at follow-up and different lung parameters at recruitment and at follow-up were observed (Supplementary Table S3 and Supplementary Figs. S1–S3). Positive correlations were found with FEV1/FVC data at recruitment, FEV1 (% predicted) values at both recruitment and follow-up as well as log transformed PC20. It was also inversely correlated to BD response (% BD), log transformed IgE, percentage of circulating eosinophils at recruitment and follow-up, and percentage of circulating monocytes. Multiple linear regression models were also tested to explain its decrease with different sets of relevant clinical parameters. Those include baseline, disease diagnosis, respiratory, exposure and asthma treatment parameters for the independent variables at recruitment (see “Supplementary File” in the multiple linear regression section for complete list). The best significant multiple linear regression model was observed between FEV1/FVC pre-BD at follow-up and the percentage of BD change (% BD), the percentage of predicted value for FEV1 pre-BD (FEV1 pre-BD % pred) and the percentage of eosinophil count (% eosino) at recruitment (FEV1/FVC pre-BD at follow-up = 63.344 − 0.321 [% BD at recruitment] + 0.173 [FEV1 pre-BD % pred at recruitment] − 1.027 [% eosino at recruitment], R2 = 0.539, p = 2.82 × 10−15).

Variations in lung function. Changes in the forced expiratory volume in 1 s on the forced vital capacity (FEV1/FVC) ratio were observed between recruitment and follow-up considering values (A) before or (B) after the use of bronchodilators (BDs). The All group includes all participants in the subsample, the No asthma group comprises individuals without asthma at recruitment, and the Asthma group include participants with confirmed asthma diagnosis at recruitment. p values < 0.001 are indicated by two asterisks and p values < 0.0001 are indicated by three asterisks. (C) Representation of participants with asthma at recruitment who exhibited either an increase (from PC20 ≤ 8 mg/ml to ≥ 16 mg/ml; n = 7) or a decrease (from PC20 ≥ 16 mg/ml to ≤ 8 mg/ml; n = 1) in PC20 measurements. (D) Representations of participants with asthma at recruitment who showed an increase (from FEV1 < 80% to > 80%; n = 5) or a decrease (from FEV1 > 80% to < 80%; n = 8) in measurements of FEV1 of predicted values.
Results also showed a decrease in PC20 values in the No asthma group between the two visits (p < 0.05, Table 1). Furthermore, an increase in PC20 values from < 8 to > 16 mg/ml of methacholine was noted for seven participants with asthma at recruitment and revealed the opposite for one individual (Fig. 3C). It was also observed that FEV1 values increased from < 80 to > 80% of predicted values for five participants with asthma and the opposite for eight others (Fig. 3D).
Changes of COPD phenotype and other comorbidities
Based on COPD diagnoses validated by a physician and retrieved from the data collected at the archives of Chicoutimi Hospital, five participants developed COPD between recruitment and follow-up (Table 4). These were all individuals with asthma at recruitment and who were either smokers or ex-smokers and represent 7% of the Asthma group or 4% of all participants. At follow-up, two of these participants were obese, two overweight and one underweight, three had FEV1 percentage of predicted value < 80% and four had FEV1/FVC ratio < 0.70. Overall, 23 participants with asthma at follow-up had reduced FEV1/FVC ratio (< 0.70). In approximately half of these participants (n = 12), FEV1/FVC ratio was already below 0.70 at recruitment.
BMI was significantly increased in all groups (p < 0.0001 in All and Asthma group, p < 0.001 in No asthma group) at follow-up. Overall, individuals with asthma at follow-up were more likely to suffer from allergies (46% in the No asthma group compared to 57% in the Asthma group), to develop rhinitis comorbidity (17% compared to 30%) and to develop atopic dermatitis (40% compared to 48%; Table 1). Nevertheless, the incidence of atopy, rhinitis and atopic dermatitis decreased between recruitment and follow-up but was only significant for rhinitis (p < 0.05; Table 1).
Discussion
The objective of this study was to analyze the evolution of asthma and related phenotypes in time by assessing new diagnoses as well as changes in the respiratory condition and comorbidities of a subsample of the SLSJ asthma family cohort. When considering changes in asthma status, seven new cases of asthma in this cohort’s subsample were found, representing 12% of individuals without asthma at recruitment. This is in line with the literature. Indeed, adult onset of asthma occurs in approximately 10% of the population17,18. It is interesting to note that only one individual (#6) out of the seven has a profile in agreement with the Global Initiative for Asthma (GINA) guidelines for a non-asthmatic becoming asthmatic (atopy, methacholine PC20 < 8 mg/ml and > 12% reversibility in airway obstruction following bronchodilators)4.
Atopy and BMI as risk factors of asthma
A study by Toskala et al. showed that atopy was a risk factor in the development and persistence of asthma19. This phenomenon was also observed in this study. Indeed, four of the seven individuals who developed asthma had allergies at recruitment and follow-up, and one developed atopy during this same period, representing 71% of the individuals with a new diagnosis of asthma. However, not all allergic asthma sufferers see their symptoms persist19. In fact, three individuals with asthma noticed their symptoms disappear and two of them were atopic at recruitment. The prevalence of allergic asthma phenotype considering all participants was persistent over time. The unchanged proportion of atopy phenotype in individuals with asthma at follow-up could be explained by the relatively stable concentration of IgE levels between the two periods (approximately 2.5 times higher than for individuals without asthma). This is consistent with the literature stating that deregulation of the immune system in allergic asthma results in elevated serum IgE levels19. It is remarkable that no significant change was observed for circulating IgE levels, regardless of age, asthma status, and medication, which evolved over the same period.
Another important risk factor is obesity20. Obesity is often associated with an increase in the severity of asthma, onset of asthma in adults, and difficult asthma control due to a decreased response to medication5,21. In the present study, an increase in BMI between recruitment and follow-up was observed in all groups. At follow-up, the average BMI was 27.06 kg/m2, which is considered overweight. However, the average BMI of individuals with a change in their respiratory status was greater than 30 kg/m2, which is considered obese. Four out of the seven individuals with adult-onset asthma had a BMI between 30 and 40 kg/m2. Therefore, these individuals presented a significant risk factor linked to their new respiratory status.
Indices of asthma severity
The FEV1/FVC ratio is a respiratory parameter that determines the degree of airway obstruction22, with a value usually lower than < 0.75–0.80 for asthmatic individuals, and that decreases according to the increase in asthma severity4. In this study, the mean FEV1/FVC ratio decreased in both individuals with and without asthma over the years. Therefore, 54% of the decrease in FEV1/FVC pre-BD ratio at follow-up can be explained by a regression model in the SLSJ subsample that includes values at recruitment for the percentage of BD reversibility, the percentage of predicted value of FEV1 and the percentage of eosinophils. A comparable effect of blood eosinophil on the decline of lung function was found in a population-based cohort of young adults in New Zealand among participants aged from 21 to 38 years old23. The study determined that blood eosinophil counts were associated with a decrease of FEV1/FVC ratio including participants with and without asthma23. Additionally, in a population-based birth cohort that was followed into adulthood (until 26 years of age), a similar decrease in lung function in all groups, regardless of wheezing, sex, or other parameters were reported24. It would therefore be normal to observe a decrease in lung capacity given the two decades between the two measurements.
The FEV1/FVC values reflected the results of self-reported asthma severity in the questionnaire at follow-up. Individuals with asthma had an average FEV1/FVC which corresponds to mild asthma according to the literature4, and the majority classified their asthma as very mild or mild. The severity of asthma can also be determined by the class of medication taken to relieve symptoms and exacerbations4. The medication prescribed in the subsample is primarily short-acting beta-agonists and ICSs, which also correspond to mild asthma4. However, there has been a marked increase (31%) in the prescription of long-acting beta-agonists, usually prescribed to people with moderate asthma4, and the prescription of ICSs (11%) at follow-up. The changes in respiratory medication use could be due to the modifications in the GINA guidelines since recruitment; in 2019 ICS-formoterol was recommended in intermittent asthma and mild persistent asthma4. Whereas in the 2002 GINA report ICSs were recommended to be introduced in mild persistent asthma only4. This could indicate that the symptoms are well controlled by the medication, leading to a self-reported asthma severity by the participants as very mild and mild.
Smoking has a significant impact on asthma, for example through epigenetic changes3. The number of smokers significantly decreased (from 22 to 4) between recruitment and follow-up. However, the risk of developing asthma in adulthood due to this exposure remains3. For individuals who had a new status of asthma at follow-up, five out of seven participants were either ex-smokers or smokers. Moreover, 58% of the 24 individuals with adult-onset asthma at recruitment were either ex-smokers or smokers. Among the 24 individuals at recruitment and the 7 individuals at follow-up with adult-onset asthma, 4 have developed obstructive sleep apnea and 3 have or had psychological disturbances (depression and anxiety disorder). These comorbidities can be found in people with severe asthma as can gastro-esophageal reflux disease and chronic infections and may be associated with difficult asthma outcomes25,26. Respiratory infections noted for these participants were not recurrent or chronic. Since the SLSJ asthma family cohort is mainly comprised of participants with mild-to-moderate asthma it is expected to have little comorbidities in the subsample.
Development of COPD among asthmatic participants
A study by Mirabelli et al. demonstrated the presence of COPD in 29% of a population with a history of asthma27. Individuals with asthma who smoked are more likely to develop COPD as they age and thus may develop asthma-COPD overlap (ACO) phenotypes3,28. In this study, five participants who were asthmatic at recruitment (7%) developed COPD and all of them were ex-smokers or smokers. For all of them, PC20 was also very low at recruitment, four of the five individuals who developed COPD had values less than 0.25 mg/ml which corresponds to severe AHR, and one had a value of 0.5 mg/ml, which is considered moderate AHR29. This suggests that this risk factor may have contributed to the development of COPD30,31. These results contribute to a better understanding of ACO which is critical since patients affected by both diseases have more exacerbations, poorer quality of life, and faster decline in lung function, as well as a higher death rate than patients with only asthma or COPD22,32,33,34,35.
Strength and limitations
The major strength of this study is the fine phenotyping performed both at recruitment and follow-up for respiratory diseases’ diagnoses as well as respiratory measures, comorbidities, and risk factors. A possible limitation of this study is its complexity. There are a large number of symptoms, environmental exposures, lifestyle habits, and comorbidities related to the heterogeneity of this disease36. In addition, the conception of a longitudinal study lasting 20 years after the first recruitment bears some difficulties. Thus, another limitation is due to change over time of knowledge about causes and treatments of diseases, leading to new parameters that are not comparable between the two-time points. For instance, in 1997 the standardized questionnaire used in this study at recruitment did not include questions assessing the non-pharmacological interventions to control asthma symptoms. Nor did it have questions helping determine the participants medical care satisfaction or adherence to their asthma treatments, making it impossible to incorporate those parameters in the longitudinal study. Furthermore, a memory bias from the participants may be introduced in some data from the questionnaire, as to assess when the changes in the asthma status occurred, since there is a long period between recruitment and follow-up. In order to prevent from this same kind of memory bias on other phenotypic parameters, clinical parameters that can be measured or diagnosed were prioritized in analyses. No bias about asthma sub-phenotypes was introduced in this study. In fact, a total of 215 participants were selected in the context of another project and the follow-ups were done at the same time. The only criteria for the selection of participants in the other project was to have one asthmatic and one non-asthmatic individual per family. The selection of the participants did not take into account the severity nor the type of asthma. A larger subsample of the cohort may provide a better representation of asthma over time. Moreover, difficulties linked to the recontact of participants make longitudinal studies more difficult to design as also found in other longitudinal studies11,36.
Conclusion
The 20-year follow-up of a subsample from the SLSJ asthma family cohort presented new asthma status for 12% of the participants without asthma at recruitment as well as COPD development for five individuals, with a description of risk factors for these individuals. Longitudinal studies like this one will allow a better characterization of asthma and comorbidities over time. One perspective of this type of study is to assess phenotypic changes and link them to the genetic and epigenetic signatures in order to understand the genetic mechanisms involved.
Data availability
Datasets used or analyzed during the current study are available from the corresponding author on a reasonable request.
Abbreviations
- ACO:
-
Asthma-COPD overlap
- AHR:
-
Airway hyperresponsiveness
- BD:
-
Bronchodilator
- BMI:
-
Body mass index
- CIUSSS:
-
Centre Intégré Universitaire de Santé et de Services Sociaux
- COPD:
-
Chronic obstructive pulmonary disease
- FEV1 :
-
Forced expiratory volume in 1 s
- FVC:
-
Forced vital capacity
- ICS:
-
Inhaled corticosteroids
- IgE:
-
Immunoglobulin E
- IL:
-
Interleukin
- PC20 :
-
Methacholine concentration inducing a 20% decrease in FEV1
- SLSJ:
-
Saguenay–Lac-Saint-Jean
- TH2:
-
T-helper type 2 cells
References
Vos, T. et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 390, 1211–1259 (2017).
Public Health Agency of Canada. Report from the Canadian chronic disease surveillance system: asthma and chronic obstructive pulmonary disease (COPD) in Canada. Government of Canada, Ottawa, 64 (2018).
Dharmage, S. C., Perret, J. L. & Custovic, A. Epidemiology of asthma in children and adults. Front. Pediatr. 7, 246 (2019).
Global Initiative for Asthma. Global strategy for asthma management and prevention 2002 and 2019. https://ginasthma.org/. Accessed 20 April 2020 (2019).
Fuchs, O., Bahmer, T., Rabe, K. F. & von Mutius, E. Asthma transition from childhood into adulthood. Lancet Respir. Med. 5, 224–234 (2017).
Barnes, P. J. The cytokine network in asthma and chronic obstructive pulmonary disease. J. Clin. Invest. 118, 3546–3556 (2008).
Ishmael, F. T. The inflammatory response in the pathogenesis of asthma. J. Am. Osteopath. Assoc. 111, S11-17 (2011).
Brinke, A. T., Zwinderman, A. H., Sterk, P. J., Rabe, K. F. & Bel, E. H. Factors associated with persistent airflow limitation in severe asthma. Am. J. Respir. Crit. Care Med. 164, 744–748 (2001).
Culver, B. Defining airflow limitation and chronic obstructive pulmonary disease: The role of outcome studies. Eur. Respir. J. 46, 8–10 (2015).
Russell, R. J. & Brightling, C. Pathogenesis of asthma: Implications for precision medicine. Clin. Sci. (Lond.) 131, 1723–1735 (2017).
Nwaru, B. I. et al. Cohort profile: the West Sweden Asthma Study (WSAS): A multidisciplinary population-based longitudinal study of asthma, allergy and respiratory conditions in adults. BMJ Open 9, e027808 (2019).
Pretolani, M., Soussan, D., Poirier, I., Thabut, G. & Aubier, M. Clinical and biological characteristics of the French COBRA cohort of adult subjects with asthma. Eur. Respiratory J. 50 (2017).
Bloom, C. I. et al. Exacerbation risk and characterisation of the UK’s asthma population from infants to old age. Thorax 73, 313–320 (2018).
Laprise, C. The Saguenay-Lac-Saint-Jean asthma familial collection: The genetics of asthma in a young founder population. Genes Immun. 15, 247–255 (2014).
Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease (COPD) and asthma. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, November 1986. Am. Rev. Respir. Dis. 136, 225–244 (1987).
American Thoracic Society. Pulmonary function testing (2005). https://www.thoracic.org/statements/pulmonary-function.php. Accessed 15 June 2020.
Australian institute of health and welfare, Asthma (2019). https://www.aihw.gov.au/reports/chronic-respiratory-conditions/asthma/contents/asthma. Accessed 30 April 2020.
European Resiratory Society. European lung white book, Adult asthma (2020). https://www.erswhitebook.org/chapters/adult-asthma/. Accessed 30 April 2020.
Toskala, E. & Kennedy, D. W. Asthma risk factors. Int. Forum Allergy Rhinol. 5(Suppl 1), S11-16 (2015).
Violante, R. et al. Obesity risk factors in the ISAAC (International Study of Asthma and Allergies in Childhood) in Mexico City. Rev. Alerg. Mex. 52, 141–145 (2005).
Li, Z. et al. Role of leptin in the association between body adiposity and persistent asthma: A longitudinal study. Obesity (Silver Spring) 27, 894–898 (2019).
Boulet, L. P. et al. Asthma-COPD overlap phenotypes and smoking: Comparative features of asthma in smoking or non-smoking patients with an incomplete reversibility of airway obstruction. COPD 15, 130–138 (2018).
Hancox, R.J., Pavord, I.D. & Sears, M.R. Associations between blood eosinophils and decline in lung function among adults with and without asthma. Eur. Respiratory J. 51 (2018).
Sears, M. R. et al. A longitudinal, population-based, cohort study of childhood asthma followed to adulthood. N. Engl. J. Med. 349, 1414–1422 (2003).
Matsumoto-Sasaki, M., et al. Association of longitudinal changes in quality of life with comorbidities and exacerbations in patients with severe asthma. Allergol. Int. https://doi.org/10.1016/j.alit.2022.05.009 (2022).
Fong, W.C.G., et al. The detrimental clinical associations of anxiety and depression with difficult asthma outcomes. J. Pers. Med. 12(2022).
Mirabelli, M. C., Beavers, S. F. & Chatterjee, A. B. Active asthma and the prevalence of physician-diagnosed COPD. Lung 192, 693–700 (2014).
Gibson, P. G. & Simpson, J. L. The overlap syndrome of asthma and COPD: What are its features and how important is it?. Thorax 64, 728–735 (2009).
Coates, A.L., et al. ERS technical standard on bronchial challenge testing: General considerations and performance of methacholine challenge tests. Eur. Respiratory J. 49 (2017).
Soriano, J. B. et al. The proportional Venn diagram of obstructive lung disease: Two approximations from the United States and the United Kingdom. Chest 124, 474–481 (2003).
Silva, G. E., Sherrill, D. L., Guerra, S. & Barbee, R. A. Asthma as a risk factor for COPD in a longitudinal study. Chest 126, 59–65 (2004).
de Marco, R. et al. The coexistence of asthma and chronic obstructive pulmonary disease (COPD): Prevalence and risk factors in young, middle-aged and elderly people from the general population. PLoS ONE 8, e62985 (2013).
Hardin, M. et al. The clinical features of the overlap between COPD and asthma. Respir. Res. 12, 127 (2011).
Blanchette, C. M., Gutierrez, B., Ory, C., Chang, E. & Akazawa, M. Economic burden in direct costs of concomitant chronic obstructive pulmonary disease and asthma in a Medicare Advantage population. J. Managed Care Pharm. JMCP 14, 176–185 (2008).
Tho, N. V., Park, H. Y. & Nakano, Y. Asthma-COPD overlap syndrome (ACOS): A diagnostic challenge. Respirology 21, 410–418 (2016).
Boudier, A. et al. Data-driven adult asthma phenotypes based on clinical characteristics are associated with asthma outcomes twenty years later. Allergy 74, 953–963 (2019).
Acknowledgements
We would like to thank the participants of the SLSJ asthma family cohort for their valuable participation in this study.
Funding
M.-E.L. was supported by Natural Sciences and Engineering Research Council of Canada Undergraduate Student Research Awards (NSERC-USRA). J.M. was supported by a Fonds de recherche du Québec-Santé (FRQS) Postdoctoral training award. This project was supported by operating grants from the Canadian Institute of Health Research (CIHR, PI: C.L.). C.L. is the director of the Centre intersectoriel en santé durable, codirector of the Environment, genetics and cancer axis of the Respiratory Health Network (RHN), investigator of CHILD Study, member of the InFAC consortium and the chairholder of the Canada Research Chair in the Environment and Genetics of Respiratory Disorders and Allergies (www.chairs.gc.ca).
Author information
Authors and Affiliations
Contributions
M.-E.L.: data acquisition, analyses, interpretation of data, drafting the manuscript; J.M.: interpretation of data, drafting the manuscript; A.-M.B.L.: data acquisition; A.-M.M.: revision of analyses, drafting and revision of the manuscript; P.B.: clinical evaluation at recruitment; C.M.: clinical evaluation at recruitment; L.-P.B.: clinical evaluation and interpretation of clinical status changes based on data; C.L.: designed, built and manages the SLSJ cohort; conceived and designed the study, directed the manuscript writing and revision. All authors have approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lavoie, ME., Meloche, J., Boucher-Lafleur, AM. et al. Longitudinal follow-up of the asthma status in a French–Canadian cohort. Sci Rep 12, 13789 (2022). https://doi.org/10.1038/s41598-022-17959-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-17959-6
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
