
Abstract
To evaluate whether high-resolution, non-contrast-enhanced dental MRI (dMRI) can reliably and accurately measure the canal length of incisors and canines compared with cone-beam computed tomography (CBCT). Three-Tesla dMRI was performed in 31 participants (mean age: 50.1 ± 14.2 years) with CBCT data. In total, 67 teeth were included (28 from the upper jaw and 39 from the lower jaw; 25 central incisors, 22 lateral incisors, and 20 canines). CBCT and dMRI datasets were reconstructed to visualize the root canal pathway in a single slice in the vestibulo-oral (V-O) and mesio-distal (M-D) direction. Root canal length was measured twice by two radiologists using dMRI and CBCT. Data were statistically analyzed by calculating intraclass correlation coefficients (ICCs) and performing Bland–Altman analysis. The reliability of dMRI measurements was excellent and comparable to that of CBCT measurements (intra-rater I/intra-rater II/inter-rater was 0.990/0.965/0.951 for dMRI vs. 0.990/0.994/0.992 for CBCT in the M-D direction and 0.991/0.956/0.967 for dMRI vs. 0.998/0.994/0.996 for CBCT in the V-O direction). According to Bland–Altman analysis, the mean (95% confidence interval) underestimation of root canal lengths was 0.67 mm (− 1.22 to 2.57) for dMRI and 0.87 mm (− 0.29 to 2.04) for CBCT in the M-D direction/V-O direction. In 92.5% of cases, dMRI measurements of canal length had an accuracy within 0–2 mm. Visualization and measurement of canal length in vivo using dMRI is feasible. The reliability of dMRI measurements was high and comparable to that of CBCT measurements. However, the spatial and temporal resolution of dMRI is lower than that of CBCT, which means dMRI measurements are less accurate than CBCT measurements. This means dMRI is currently unsuitable for measuring canal length in clinical practice.
Similar content being viewed by others


Introduction
Since the introduction of cone-beam computed tomography (CBCT) in the late 1990s1 three-dimensional (3D) imaging has shown great potential for dentalmaxillo-facial imaging2. CBCT can accurately depict endodontic tooth anatomy, the number of root canals, and details of the surrounding alveolar bone, allowing it to detect pathologies that would otherwise be missed in periapical intraoral radiographs3,4. Therefore, CBCT has become an essential tool in endodontics for diagnosis, treatment planning, and evaluating treatment outcomes5,6.
Accurate filling of root canals determines the success of root canal treatment7,8 several studies have evaluated whether CBCT can be used to determine the canal length and whether CBCT measurements are more precise than electronic apex locator (EAL) measurements9,10,11,12. These studies concluded that CBCT imaging is accurate enough to determine the canal length.
However, EAL remains the gold standard to determine accurate length measurements in most cases. But there are also a few exceptions in this regard. Limitations for EAL measurements are given in cases like metallic restorations13, partially or totally obliterated root canals14, root perforations15 or measurements during root canal retreatments16. The aim should always be to combine EAL measurements with imaging techniques of proven accuracy17.
Despite the benefits of CBCT over intraoral periapical radiographs, its application is limited by the high radiation dose18,19. A radiation-free imaging modality is needed, especially for young patients who are most radiosensitive20. Dental magnetic resonance imaging (dMRI) has excellent soft-tissue contrast and is a promising imaging modality for diagnosing various pathologies in endodontics21,22,23,24, including promising results in differentiating periapical lesions25,26,27, orthodontics28, craniomaxillofacial surgery29, and implantology30,31,32,33,34.
Despite promising ex vivo results35,36,37, the ability of dMRI to measure root canal length has not been evaluated in vivo. The development of dedicated coil and sequence techniques38,39,40,41 has increased the resolution of dMRI and has reduced the number of artifacts observed during clinical imaging. Thus, we hypothesized that dMRI may be a reliable and accurate alternative to CBCT for measuring root canal length. To test this hypothesis, we performed a prospective clinical study to compare dMRI measurements with corresponding CBCT measurements.
Materials and methods
This prospective study was approved by the ethics committee of the University of Heidelberg (approval number S-404/2014) and written informed consent was obtained from all participants. Inclusion criteria were the presence of incisors and canines and a CBCT scan, which had been performed for clinical reasons such as implant planning. Patient-related exclusion criteria were < 18 years of age, implants not safe for 3 T MRI, pregnancy, and claustrophobia. Tooth-related exclusion criteria were dMRI/CBCT artifacts that compromised pulp, poor visibility of the root canal or incisal edge, previous root canal treatment, and crowns. The sample size was calculated according to recommendations for clinical pilot studies42 and patients were consecutively recruited in a single center. Throughout the study dMRI measurements were directly compared to corresponding CBCT measurements.
Ethical approval and consent
The use of human participants in this study was approved by the ethics committee of the University of Heidelberg and the study was performed in accordance with the 1964 Declaration of Helsinki and its later amendments. All patients gave written informed consent prior to inclusion in this study.
Imaging
All CBCT images were acquired using a 3D Accuitomo 170 scanner (J Morita; Kyoto, Japan) with the following acquisition parameters: field of view: 8 × 8 cm2, tube voltage: 90 kV, tube current: 7 mA, 14-bit, 360° rotation in 17 s, 560 frames, and an isotropic voxel size of 160 μm. All MRI scans were performed on a 3 T MRI system (Magnetom Trio; Siemens Healthineers GmbH, Erlangen, Germany) using a dedicated 15-channel dental surface coil (Mandibula, Noras MRI products GmbH). A single PD-weighted 3D MSVAT-SPACE (multiple slab acquisition with view angle tilting gradient based on a sampling perfection with application-optimized contrasts using different flip angle evolution) sequence was applied. This sequence was optimized for dental MRI as previously described by Hilgenfeld et al.39. Sequence parameters were 6.4 ms echo time; 1170 ms repetition time; 168 mm × 131 mm field of view; 384 × 300 acquisition matrix; 0.44 mm × 0.44 mm × 0.44 mm voxel size; 220% slice oversampling; 80 slices; and 7:45 min acquisition.
Image analysis
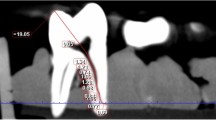
CBCT and MRI datasets were reconstructed using Osirix (v. 8.5.1., Geneva, Switzerland) to visualize the root canal pathway in a single slice in the vestibulo-oral (V-O) and mesio-distal (M-D) direction as previously described11. Next, images were randomized and evaluated twice by two experienced radiologists with an interval of 2 weeks between evaluations to exclude learning bias. CBCT and MRI datasets were also analyzed separately in each round, with an interval of 2 weeks between the imaging modalities. CBCT and MRI datasets were analyzed in different random orders. The contrast/saturation of the images could be adjusted. The root canal length was defined as the distance between the most incisal edge in the projected midline of the pulp cavity and the major foramen (Fig. 1). Curved measurement lines were placed in the pulpal center, including curvatures of the canal as previously described11.

Canal length measurements by dMRI (upper row) and CBCT (lower row) in the mesio-distal (M-D) and vestibulo-oral (V-O) directions in the second left upper incisor (A–D) and the first right lower incisor (E–H). dMRI slices of a second incisor in the left upper jaw in the M-D direction (A) and the V-O direction (B). (C,D) Are the corresponding CBCT slices. dMRI slices of a first incisor in the right lower jaw in the M-D direction (E) and the V-O direction (F). (G,H) Are the corresponding CBCT slices.
Statistical analysis
Statistical analysis was performed using SPSS 23 (SPSS Inc., Chicago, USA). To assess the reliability of CBCT and MRI measurements, intra- and inter-rater agreement were calculated using intraclass correlation coefficients (ICCs) with 95% confidence intervals (CIs). The accuracy of MRI measurements was determined using Bland–Altman plots, illustrating differences between corresponding dMRI and CBCT values. We also calculated the average difference in measurements between dMRI and CBCT and the upper and lower limit of the 95% CI for the two modalities. To allow comparison of our data with those of previous studies, we also calculated the Pearson correlation coefficient between dMRI and CBCT measurements.
Results
In total, 31 participants (13 males, 18 females) of white European ethnicity were enrolled in the study. The mean ± standard deviation (SD) age was 50.1 ± 14.2 years (median 51.0; range 28–74). Teeth with movement artifacts or metal artifacts were excluded, leaving 67 teeth (28 in the upper jaw, 39 in the lower jaw; 25 first incisors, 22 s incisors, 20 canines) in the final assessment. High-resolution 3D dMRI produced detailed images of pulp and root canals (Fig. 1).
Reliability
Intra- and inter-rater reliability of root canal length measurements were excellent for both modalities (range 0.951–0.998) (Tables 1, 2). CBCT measurements had a slightly higher intra-rater agreement than dMRI measurements did (range CBCT: 0.990–0.998; range dMRI: 0.956–0.991). A similar trend was observed for the inter-rater agreement, with higher values for CBCT (M-D: 0.992, 95% CI: 0.986–0.996; V-O: 0.996, 95% CI: 0.994–0.998) than for dMRI (M-D: 0.951, 95% CI: 0.921–0.970; V-O: 0.967, 95% CI: 0.943–0.981).
Accuracy
dMRI measurements underestimated the canal length compared to the CBCT measurements (underestimation in 95.5% of dMRI measurements in the V-O direction and in 79.1% of dMRI measurements in the M-D direction). The median ± SD underestimation was 0.84 ± 0.59 mm in the V-O direction and 0.69 ± 0.96 mm in the M-D direction (Fig. 2). The proportion of dMRI measurements that were 0–2 mm different from CBCT measurements was 92.5% in the V-O direction and 71.6% in the M-D direction. The canal length was overestimated beyond 0.5 mm of the apex in 10.4% of dMRI measurements in the M-D direction compared to the CBCT measurements. The maximum difference between dMRI measurements and the corresponding CBCT measurements was 2.51 mm underestimation and 0.41 mm overestimation in the V-O plane and 3.81 mm underestimation and 2.14 mm overestimation in the M-D plane.

Box plots with 95% CIs of differences between dMRI and CBCT canal length measurements. The bold black line represents the median differences.
Bland–Altman analysis revealed consistent underestimation of canal lengths by dMRI compared to the CBCT measurements. The mean underestimation (lower/upper limits of agreement) of root canal length was 0.67 (− 1.22 to 2.57)/0.87 (− 0.29 to 2.04) mm for M-D and V-O measurements (Fig. 3).

Bland–Altman plots, illustrating differences between corresponding CBCT and dMRI canal length measurements in the mesio-distal (A) and vestibulo-oral (B) plane. The dotted line represents the mean differences (bias) and the solid lines represent the upper and lower 95% limits of agreement.
The accuracy of dMRI measurements was similar between the upper and lower jaw. Bland–Altman analysis revealed an underestimation (95% limits of agreement) of 0.67 (− 0.88 to 2.24)/0.74 (− 0.47 to 1.97) mm for the upper jaw and 0.67 (− 1.45 to 2.80)/0.96 (− 0.13 to 2.06) mm for the lower jaw in the M-D and V-O directions.
Discussion
In this study, we compared the reliability and accuracy of root canal working lengths measured by dMRI and CBCT in vivo. The reliability of dMRI canal length measurements was similar to that of CBCT measurements in both studied directions. However, dMRI canal length measurements were less accurate than CBCT measurements in both directions 0.67 mm (− 1.22 to 2.57) for mesio-distal measurements and 0.87 mm (− 0.29 to 2.04) for vestibulo-oral measurements. These results are clinically important because they reflect how CBCT-based 3D imaging has dramatically improved diagnostic accuracy and treatment planning in endodontics5,43. However, CBCT uses higher radiation doses than conventional radiography, so is limited. A comparable radiation-free 3D imaging modality like dMRI would be of great value.
A methodological strength of this study is the evaluation of dMRI reliability and accuracy in vivo. This approach incorporated clinically relevant factors like movement and metal artifacts and tooth variations, which play a crucial role in the outcome of endodontic therapy8,44. Most previous evaluations of CBCT measurements have been performed ex vivo9,12. Liang et al. and Connert et al. included 162 and 42 extracted teeth, respectively. Other studies that were performed in vivo have been limited by their sample size10,11: Janner et al. and Jeger et al. included 9 and 40 teeth, respectively. Our in vivo study included a larger sample size than that of previous studies (67 teeth, 134 tooth datasets, and 1072 root canal measurements) and we analyzed teeth in the upper and lower jaw separately, which was not possible in previous in vivo studies because of the low sample size. This is relevant because pulp sizes differ between the upper and lower jaw, and this difference may affect the accuracy of dMRI measurements.
The intra- and inter-reliability of dMRI measurements were excellent and comparable to those of CBCT measurements. Reliability of CBCT measurements in previous studies was measured as an ICC of 0.982 under ex vivo conditions10 and a Pearson correlation coefficient of 0.99 under in vivo conditions10. In agreement, we also observed high ICCs for CBCT measurements (range 0.990–0.998) as well as for dMRI measurements (range 0.956–0.991). These results show that the reliability of dMRI measurements is comparable to that of CBCT measurements.
We investigated the root canal length in M-D and V-O directions and found a lower mean error in the M-D direction (mean difference 0.67 mm) than in the V-O direction (mean difference 0.87 mm). This result is in accordance with the results of a previous in vivo CBCT study by Jeger et al., who found a slightly lower mean error in the M-D direction than in the V-O direction (0.48 mm vs. 0.49 mm)10.
Previous studies have shown a high accuracy of CBCT root canal length measurements compared with electronic apex locator measurements. Pearson correlation coefficients for CBCT measurements compared with electronic apex measurements were 0.977 in ex vivo studies9 and 0.968–0.97 for in vivo studies10,11. We found a similarly high correlation between dMRI and CBCT measurements (0.927–0.969) in the present study.
We also investigated measurement error in canal length measurements. In previous studies of CBCT canal length measurements, Janner et al. reported errors of 0.4 mm (range 0.03–1.6 mm) and Jeger et al. reported errors of 0.51 mm (0.02–1.83 mm) under clinical conditions10,11. In agreement, Connert et al. observed an error of 0.41 mm (0.31–0.52 mm) and Liang et al. an error of 0.46 mm (0.41–0.50) under ex vivo conditions9,12. Our dMRI measurements showed a lower accuracy and a larger range of error of 0.67 mm (− 1.22 to 2.57) than these earlier CBCT measurements did. Although up to 92.5% of our measurements were within an error range of − 2 mm to 0 mm, there were some outliers. This shows that dMRI is currently not accurate enough to measure the canal length because instrumentation and root filling should be within 0–2 mm of the radiographic apex7. However, dMRI measurements were still within the magnitude of CBCT measurements, despite the higher spatial resolution (factor of voxel volume of 21) and longer acquisition time (factor 26) of CBCT.
Several limitations must be acknowledged in this study. First, we chose CBCT measurements and not electronic apex locator measurements as the reference modality. However, previous studies observed a high accuracy of CBCT-based measurements compared with clinical gold standard EAL. Second, although we chose a high-resolution dMRI setup, the spatial resolution as well as acquisition time of dMRI were substantially lower than that of CBCT, resulting in lower accuracy. Third, metallic artifacts due to dental restorations as well as claustrophobia due to narrow coils are relevant limitations in dMRI. These limitations, however, might be reduced with optimized MRI sequence techniques for metal artifact reduction39 and intraoral placement of MRI coils in the future45. Finally, the costs and availability of MRI machines also limit the clinical application of dMRI and these obstacles should be addressed in future research.
Conclusion
This prospective in vivo study has demonstrated that measuring root canal length in incisors and canines in vivo using dMRI is feasible. The reliability of dMRI canal length measurements was comparable to that of CBCT measurements. However, dMRI measurements were less accurate because of lower resolution and longer acquisition times, which currently hampers its clinical application. Further research is needed to increase the spatial resolution and reduce the acquisition time of dMRI before this promising non-ionizing imaging modality can be used to measure canal length under clinical conditions.
Data availability
The datasets generated during and/or analyzed during the current study are not publicly available because of data privacy protection of patients and participants but are available from the corresponding author on reasonable request.
References
Mozzo, P., Procacci, C., Tacconi, A., Martini, P. T. & Andreis, I. A. A new volumetric CT machine for dental imaging based on the cone-beam technique: Preliminary results. Eur. Radiol. 8, 1558–1564. https://doi.org/10.1007/s003300050586 (1998).
Pinsky, H. M., Dyda, S., Pinsky, R. W., Misch, K. A. & Sarment, D. P. Accuracy of three-dimensional measurements using cone-beam CT. Dentomaxillofac. Radiol. 35, 410–416. https://doi.org/10.1259/dmfr/20987648 (2006).
Lofthag-Hansen, S., Huumonen, S., Grondahl, K. & Grondahl, H. G. Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 103, 114–119. https://doi.org/10.1016/j.tripleo.2006.01.001 (2007).
Bornstein, M. M., Lauber, R., Sendi, P. & von Arx, T. Comparison of periapical radiography and limited cone-beam computed tomography in mandibular molars for analysis of anatomical landmarks before apical surgery. J. Endod. 37, 151–157. https://doi.org/10.1016/j.joen.2010.11.014 (2011).
Patel, S. New dimensions in endodontic imaging: Part 2. Cone beam computed tomography. Int. Endod. J. 42, 463–475. https://doi.org/10.1111/j.1365-2591.2008.01531.x (2009).
Fayad, M. I. et al. AAE and AAOMR joint position statement: Use of cone beam computed tomography in endodontics 2015 update. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 120, 508–512. https://doi.org/10.1016/j.oooo.2015.07.033 (2015).
Ng, Y. L., Mann, V., Rahbaran, S., Lewsey, J. & Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 2. Influence of clinical factors. Int. Endod. J. 41, 6–31. https://doi.org/10.1111/j.1365-2591.2007.01323.x (2008).
Ricucci, D., Russo, J., Rutberg, M., Burleson, J. A. & Spangberg, L. S. A prospective cohort study of endodontic treatments of 1,369 root canals: Results after 5 years. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 112, 825–842. https://doi.org/10.1016/j.tripleo.2011.08.003 (2011).
Liang, Y. H. et al. The validity of cone-beam computed tomography in measuring root canal length using a gold standard. J. Endod. 39, 1607–1610. https://doi.org/10.1016/j.joen.2013.08.001 (2013).
Jeger, F. B., Janner, S. F., Bornstein, M. M. & Lussi, A. Endodontic working length measurement with preexisting cone-beam computed tomography scanning: A prospective, controlled clinical study. J. Endod. 38, 884–888. https://doi.org/10.1016/j.joen.2012.03.024 (2012).
Janner, S. F., Jeger, F. B., Lussi, A. & Bornstein, M. M. Precision of endodontic working length measurements: A pilot investigation comparing cone-beam computed tomography scanning with standard measurement techniques. J. Endod. 37, 1046–1051. https://doi.org/10.1016/j.joen.2011.05.005 (2011).
Connert, T., Hulber, J. M., Godt, A., Lost, C. & ElAyouti, A. Accuracy of endodontic working length determination using cone beam computed tomography. Int. Endod. J. 47, 698–703. https://doi.org/10.1111/iej.12206 (2014).
Shabahang, S., Goon, W. W. & Gluskin, A. H. An in vivo evaluation of Root ZX electronic apex locator. J. Endod. 22, 616–618. https://doi.org/10.1016/S0099-2399(96)80033-1 (1996).
ElAyouti, A. et al. Consistency of apex locator function: A clinical study. J. Endod. 35, 179–181. https://doi.org/10.1016/j.joen.2008.10.017 (2009).
Ugur Aydin, Z. & Goller Bulut, D. Determination of root canal length up to perforation area using different electronic apex locators and CBCT images obtained at different voxel sizes: A comparative ex vivo study. Chin. J. Dent. Res. 24, 49–54. https://doi.org/10.3290/j.cjdr.b1105877 (2021).
Tufenkci, P. & Kalayci, A. Evaluation of the accuracy of different apex locators in determining the working length during root canal retreatment. J. Dent. Res. Dent. Clin. Dent. Prospects 14, 125–129. https://doi.org/10.34172/joddd.2020.026 (2020).
Kim, E., Marmo, M., Lee, C. Y., Oh, N. S. & Kim, I. K. An in vivo comparison of working length determination by only root-ZX apex locator versus combining root-ZX apex locator with radiographs using a new impression technique. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 105, e79–e83. https://doi.org/10.1016/j.tripleo.2007.12.009 (2008).
Jacobs, R., Salmon, B., Codari, M., Hassan, B. & Bornstein, M. M. Cone beam computed tomography in implant dentistry: Recommendations for clinical use. BMC Oral Health 18, 88. https://doi.org/10.1186/s12903-018-0523-5 (2018).
Pauwels, R. et al. Effective radiation dose and eye lens dose in dental cone beam CT: Effect of field of view and angle of rotation. Br. J. Radiol. 87, 20130654. https://doi.org/10.1259/bjr.20130654 (2014).
Meulepas, J. M. et al. Radiation exposure from pediatric CT scans and subsequent cancer risk in the Netherlands. J. Natl. Cancer Inst. 111, 256–263. https://doi.org/10.1093/jnci/djy104 (2019).
Leontiev, W. et al. Suitability of magnetic resonance imaging for guided endodontics: Proof of principle. J. Endod. https://doi.org/10.1016/j.joen.2021.03.011 (2021).
Ariji, Y., Ariji, E., Nakashima, M. & Iohara, K. Magnetic resonance imaging in endodontics: A literature review. Oral Radiol. 34, 10–16. https://doi.org/10.1007/s11282-017-0301-0 (2018).
Ploder, O. et al. Reperfusion of autotransplanted teeth—Comparison of clinical measurements by means of dental magnetic resonance imaging. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 92, 335–340. https://doi.org/10.1067/moe.2001.116505 (2001).
Iohara, K. et al. Assessment of pulp regeneration induced by stem cell therapy by magnetic resonance imaging. J. Endod. 42, 397–401. https://doi.org/10.1016/j.joen.2015.11.021 (2016).
Juerchott, A. et al. Differentiation of periapical granulomas and cysts by using dental MRI: A pilot study. Int. J. Oral Sci. 10, 17. https://doi.org/10.1038/s41368-018-0017-y (2018).
Lizio, G. et al. Differential diagnosis between a granuloma and radicular cyst: Effectiveness of magnetic resonance imaging. Int. Endod. J. 51, 1077–1087. https://doi.org/10.1111/iej.12933 (2018).
Geibel, M. A. et al. Characterisation of apical bone lesions: Comparison of MRI and CBCT with histological findings—A case series. Eur. J. Oral Implantol. 10, 197–211 (2017).
Juerchott, A. et al. In vivo comparison of MRI- and CBCT-based 3D cephalometric analysis: Beginning of a non-ionizing diagnostic era in craniomaxillofacial imaging? Eur. Radiol. 30, 1488–1497. https://doi.org/10.1007/s00330-019-06540-x (2020).
Juerchott, A. et al. In vivo reliability of 3D cephalometric landmark determination on magnetic resonance imaging: A feasibility study. Clin. Oral Investig. 24, 1339–1349. https://doi.org/10.1007/s00784-019-03015-7 (2020).
Hilgenfeld, T. et al. Use of dental MRI for radiation-free guided dental implant planning: A prospective, in vivo study of accuracy and reliability. Eur. Radiol. 30, 6392–6401. https://doi.org/10.1007/s00330-020-07262-1 (2020).
Duttenhoefer, F. et al. Magnetic resonance imaging in zirconia-based dental implantology. Clin. Oral Implants Res. 26, 1195–1202. https://doi.org/10.1111/clr.12430 (2015).
Probst, F. A. et al. Magnetic resonance imaging based computer-guided dental implant surgery—A clinical pilot study. Clin. Implant Dent. Relat. Res. 22, 612–621. https://doi.org/10.1111/cid.12939 (2020).
Hilgenfeld, T. et al. Accuracy of cone-beam computed tomography, dental magnetic resonance imaging, and intraoral radiography for detecting peri-implant bone defects at single zirconia implants—An in vitro study. Clin. Oral Implants Res. 29, 922–930. https://doi.org/10.1111/clr.13348 (2018).
Flugge, T. et al. Virtual implant planning and fully guided implant surgery using magnetic resonance imaging—Proof of principle. Clin. Oral Implants Res. 31, 575–583. https://doi.org/10.1111/clr.13592 (2020).
Timme, M. et al. Imaging of root canal treatment using ultra high field 9.4T UTE-MRI—A preliminary study. Dentomaxillofac. Radiol. 49, 20190183. https://doi.org/10.1259/dmfr.20190183 (2020).
Dragan, O. C., Farcasanu, A. S., Campian, R. S. & Turcu, R. V. Human tooth and root canal morphology reconstruction using magnetic resonance imaging. Clujul Med. 89, 137–142. https://doi.org/10.15386/cjmed-555 (2016).
Capuani, S. et al. Nuclear magnetic resonance microimaging for the qualitative assessment of root canal treatment: An ex vivo preliminary study. Diagnostics (Basel). https://doi.org/10.3390/diagnostics11061012 (2021).
Prager, M. et al. Dental MRI using a dedicated RF-coil at 3 Tesla. J. Craniomaxillofac Surg. 43, 2175–2182. https://doi.org/10.1016/j.jcms.2015.10.011 (2015).
Hilgenfeld, T. et al. PETRA, MSVAT-SPACE and SEMAC sequences for metal artefact reduction in dental MR imaging. Eur. Radiol. 27, 5104–5112. https://doi.org/10.1007/s00330-017-4901-1 (2017).
Flügge, T. et al. Magnetic resonance imaging of intraoral hard and soft tissues using an intraoral coil and FLASH sequences. Eur. Radiol. 26, 4616–4623. https://doi.org/10.1007/s00330-016-4254-1 (2016).
Sedlacik, J. et al. Optimized 14 + 1 receive coil array and position system for 3D high-resolution MRI of dental and maxillomandibular structures. Dentomaxillofac. Radiol. 45, 20150177. https://doi.org/10.1259/dmfr.20150177 (2016).
Johanson, G. A. & Brooks, G. P. Initial scale development: Sample size for pilot studies. Educ. Psychol. Meas. 70, 394–400. https://doi.org/10.1177/0013164409355692 (2010).
Lo Giudice, R. et al. Accuracy of periapical radiography and CBCT in endodontic evaluation. Int. J. Dent. 2018, 2514243. https://doi.org/10.1155/2018/2514243 (2018).
Sjogren, U., Hagglund, B., Sundqvist, G. & Wing, K. Factors affecting the long-term results of endodontic treatment. J. Endod. 16, 498–504. https://doi.org/10.1016/S0099-2399(07)80180-4 (1990).
Hilgenfeld, T. et al. High-resolution single tooth MRI with an inductively coupled intraoral coil-can MRI compete with CBCT? Investig. Radiol. https://doi.org/10.1097/RLI.0000000000000890 (2022).
Acknowledgements
For the publication fee we acknowledge financial support by deutsche Forschungsgemeinschaft within the funding programme “Open Access Publikationskosten” as well as by Heidelberg University.
Funding
Open Access funding enabled and organized by Projekt DEAL. This work was supported by a Grant from the Dietmar Hopp Foundation (Grant Number: 1DH2011152).
Author information
Authors and Affiliations
Contributions
M.Z. and T.H. designed the study, collected the data, analyzed and led the writing; F.S.S. designed the study, collected the data; A.J. collected and analyzed the data; M.N and Z.H. contributed to methodology and sequence development; J.M. contributed to conception and interpretation; S.H. and M.B. contributed to conception, study design and interpretation.
Corresponding author
Ethics declarations
Competing interests
Tim Hilgenfeld, Alexander Juerchott and Johannes Mente received a Grant from the Dietmar Hopp Foundation. Mathias Nittka and Zahra Hosseini are both employees at Siemens Healthcare GmbH. The rest of the authors stated explicitly that there are no competing interests in connection with this article.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zidan, M., Schwindling, F.S., Juerchott, A. et al. Reliability and accuracy of dental MRI for measuring root canal length of incisors and canines: a clinical pilot study. Sci Rep 12, 14068 (2022). https://doi.org/10.1038/s41598-022-17889-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-17889-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
