
Abstract
This study investigates the application of the 150° tangential fluoroscopic projection as a novel fluoroscopic view to detect the posterosuperior screw in–out–in (IOI) in the cannulated screws fixation of femoral neck fractures. A retrospective analysis was conducted including 33 patients with femoral neck fractures enrolled from April to November 2021. All patients underwent closed reduction and internal fixation with cannulated screws under intra-operative C-arm fluoroscopy. The posterosuperior femoral neck screw position (whether in–out–in and the distance to the femoral neck cortex) was evaluated from the standard anteroposterior (AP), lateral view, and tangential view images. Postoperative computed tomography (CT) scan results are considered the gold standard for detecting the femoral neck screw locations. Of 33 patients, no femoral neck screws were found to be placed IOI under the standard AP and lateral views. The tangential view revealed the posterosuperior screw was IOI in 8 patients, whereas the average distance between the posterosuperior screw and the posterior femoral neck cortex was 2.73 ± 1.06 mm under the standard lateral view. Postoperative CT verified that posterosuperior screw was placed IOI in these 8 patients. In the other 25 patients with the tangential view showed the posterosuperior screw completely contained in the femoral neck, the average distance between the posterosuperior screw and the posterior femoral neck cortex was 5.48 ± 1.26 mm under the standard lateral view and 2.76 ± 1.08 mm under the tangential view, with a statistically significant difference between the two groups (p < 0.05). Post-operative CT demonstrated that the femoral neck screws were completely contained in the femoral neck in these 25 patients. Intra-operative tangential view of 150° can effectively identify the posterosuperior screw IOI in the cannulated screws fixation of femoral neck fractures. Based on our study, we highly recommend the tangential view as a routine intraoperative fluoroscopic angle to detect the posterosuperior screw IOI.
Similar content being viewed by others


Introduction
Hip fractures cripple 4.5 million individuals worldwide each year, of which femoral neck fractures account for about 53%1. Inverted triangular cannulated screws were commonly used in the treatment of femoral neck fractures according to the three point principle2. Lindequist et al. demonstrated that optimal support of the femoral neck cortex can be achieved when the distance between the screw and the femoral neck cortex is less than 3 mm3.
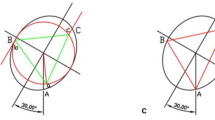
Currently, in clinical practice, the standard femoral neck AP and lateral views are used as intraoperative fluoroscopic evaluation means to assess the quality of fracture reduction and screw placement4. However, previous literatures revealed that the standard femoral neck AP and lateral views couldn’t accurately reveal the IOI posterosuperior femoral neck screw5,6. For further validation, we simulated the posterosuperior screw IOI in the inverted triangle cannulated screws fixation of femoral neck fractures via Unigraphics NX 12.0 (Siemens PLM Software), while all screws are contained within the femoral neck under the standard AP and lateral views. Subsequently, we utilized an artificial femur model simulating inverted triangular cannulated screws internal fixation of femoral neck fractures to determine the limitations of the standard AP and lateral views in detecting IOI (Fig. 1).

The limitations of the standard AP and lateral views in detecting IOI. (A) Software simulation IOI. (B) Specimen simulation IOI. (C) The standard femoral neck AP and lateral views showed all screws were contained within the femoral neck.
Anatomical studies have shown that the cross-sectional morphology of the femoral neck is approximately obliquely elliptical, with more defects in the posterosuperior and anteroinferior areas7,8. With increasing osteoporosis, the trabecular comes to lie progressively more antero-superiorly within the femoral neck9. Precisely for this reason, the posterosuperior screw has a high cortical breakage rate, creating an In–Out–In (IOI) screw. Based on the anatomy of the proximal femur, we proposed a hypothesis to identify the presence of posterosuperior screw IOI by fluoroscopy of the tangential position of the posterosuperior femoral neck cortex, usually at 150 °C-arm rotations (Fig. 2). Our study aimed to introduce a new fluoroscopic view called the tangential view, which can be used to detect the posterosuperior screw in–out–in and to signify its value in clinical applications.

(A) Positioning of C-arm during the standard femoral neck AP view, (B) positioning of C-arm during the standard femoral neck lateral view, (C) positioning of C-arm during the 150° tangential views, (D) the red circles represent femoral neck screws, the green oblique oval represents the femoral neck cross-sectional.
Materials and methods
Patients
The study retrospectively enrolled patients with femoral neck fractures who underwent closed reduction and internal fixation with cannulated screws under two-dimensional (2D) C-arm fluoroscopy in our level-1 trauma center from April to November 2021. Inclusion criteria were: the time interval from injury to operation < 3 weeks, Age > 18 years, intraoperative C-arm fluoroscopic (including the standard femoral neck AP, lateral and tangential views) and post-operative CT (both 2D and 3D imaging) of the femoral neck were available. Exclusion criteria included: pathological femoral neck fractures, patients with anatomical deformities of the proximal femur, patients with multiple fractures of the ipsilateral femur, patients with previous hip fractures. The study population consisted of 33 patients with femoral neck fractures (10 men and 23 women; 15 left and 18 right) and a mean age of 64.38 ± 12.62 years (range 43–86 years). Hip X-ray and CT were completed before surgery. AO Foundation and Orthopaedic Trauma Association (AO/OTA) classification revealed 7 cases of type 31B1.1, 9 cases of type 31B1.2, 6 cases of type 31B1.3, 7 cases of type 31B2.2, and 4 cases of type 31B2.3. The institutional review board approved the study and written informed consent was obtained from all patients. This retrospective study was approved by the Ethics Committee of the First Affiliated Hospital of Dalian Medical University (number PJ-KS-KY-2021-248) and performed in accordance with the Helsinki Declaration.
Treatment protocol
All patients with femoral neck fractures scheduled for surgery in our level-1 trauma center were evaluated preoperatively by an anesthesiologist and medical consultation if necessary. After medical contraindications were eliminated, the surgery was performed immediately by a senior trauma orthopedic surgeon under the direct supervision of the chief of trauma orthopedics. After general anesthesia, closed reduction was performed on the fracture traction table. The C-arm was routinely placed in the crotch between the two legs to observe the fracture reduction quality and the position of the implant. If the quality of the closed reduction is unsatisfactory, use the joystick reduction technique to achieve anatomical position10. Fractures were fixed using 7.5 mm diameter semi-threaded, cannulated screws. Inverted triangular cannulated screws were placed according to the three-point principle. Both ends of the screw are fixed in solid bone, respectively the proximal lateral femoral cortex and the subchondral bone of the femoral head. The shafts of screws were positioned against the inner surface of the femoral neck cortex. The surgeon decided whether to place an off-axis screw perpendicular to the fracture line through the greater trochanter to counteract shear forces, depending on the degree of fracture stability. The whole process of internal fixation implantation was under the standard femoral neck AP and lateral views.
After the implantation procedure of the femoral neck with cannulated screws, a comprehensive assessment of the position of the posterosuperior screw involved the observation of radiographs in the standard femoral neck AP, lateral and tangential views. The AP view is the position where the best outline of the greater trochanter can be seen5. In the standard lateral view (true sagittal) of the femoral neck, the angle of X-ray provided by the C-arm bulb tube and the ground is approximately 20°, thus eliminating the influence of the anteversion angle of the femoral neck and aligning the femoral head, femoral neck axis, and femoral shaft axis in a straight line11. In the tangential view of the femoral neck, the angle of X-ray provided by the C-arm bulb tube and the ground is approximately 150° so the projection plane was tangential to the posterosuperior femoral neck cortex. Under the standard femoral neck AP, lateral and tangential views, observe whether the posterosuperior cannulated screw is in–out–in. If not, measure the distance between the posterosuperior screw and the posterior femoral neck cortex under the standard lateral and tangential views.
Postoperative imaging evaluation
Plain radiographs and computed tomography scans of the injured hip were performed immediately after surgery. The director of trauma orthopedics reviewed all images to observe whether the posterosuperior screw was IOI. The postoperative computed tomography (both 2D and 3D imaging) results are considered the gold standard because it provided a full range of views of fracture reduction and cannulated screw position12. The postoperative CT images were performed with 16-detector spiral CT scanner (GE Health care, LightSpeed CT, Waukesha, WI), and the scanning parameters were as follows: layer thickness, 0.625 mm; tube voltage, 120 kVp; pitch, 1.375; matrix, 512 × 512.
Statistical analysis
Descriptive variables are presented in the text as means and standard deviations. The evaluation of the CT scan is the reference to assess the position of the posterosuperior cannulated screw. Student's T-Test was used to compare the distance between the posterosuperior screw and the posterior femoral neck cortex under the standard lateral and tangential views. Statistical significance was defined as p < 0.05.
Ethics approval and consent to participate
The collected data was anonymized and de-identified before data analysis. The Institutional Review Board of First Affiliated Hospital of Dalian Medical University granted a waiver of written informed consent and provided authorization for this study (number PJ-KS-KY-2021-248).
Results
There were 10 males and 23 females with a mean age of 64.38 ± 12.62 years (range 43–86 years). All femoral neck fractures were satisfactorily reduced, almost to the anatomical position. Of 33 patients, no femoral neck screws were found to be placed IOI under the standard AP and lateral views. The tangential view revealed the posterosuperior screw was IOI in eight patients, whereas the average distance between the posterosuperior screw and the posterior femoral neck cortex was 2.73 ± 1.06 mm under the standard lateral view. Postoperative CT (both 2D and 3D imaging) through a fine (2 mm) cut of the femoral neck revealed that the posterosuperior screw was in–out–in in 8 patients, the same as under the tangential view (Fig. 3). In the other 25 patients with the tangential view showed the posterosuperior screw completely contained in the femoral neck, the average distance between the posterosuperior screw and the posterior femoral neck cortex was 5.48 ± 1.26 mm under the standard lateral view and 2.76 ± 1.08 mm under the tangential view, with a statistically significant difference between the two groups (p < 0.05). Post-operative CT demonstrated that the femoral neck screws were completely contained in the femoral neck in these 25 patients (Table 1).

The posterosuperior femoral neck screw placed caudal to the inferior margin of the piriformis fossa in–out–in. The green arrow represents the piriformis fossa radiographic landmark. The red arrow represents the posterosuperior femoral neck screw IOI. (A,B) Intra-operative the AP and lateral views showed all screws were contained within the femoral neck. (C) Intra-operative the tangential view showed the posterosuperior screw IOI. (D,E) Postoperative plain radiographs showed all screws were contained within the femoral neck. (F,G) Postoperative CT showed the posterosuperior femoral neck screw IOI.
Discussion
The purpose of our study was to investigate the value of the intra-operative tangential view to determine the posterosuperior femoral neck screw IOI in clinical applications. This study observed that the tangential view was more sensitive than the standard lateral view in distinguishing the posterosuperior screw IOI. Therefore, we recommend that the tangential view should be used as a routine C-arm machine fluoroscopic plane during the implantation of the cannulated screw guide wire for internal fixation of femoral neck fractures. When the tangential view reveals that the femoral neck screw guide wire is IOI or very close to the femoral neck cortex, the position of the guidewire should be promptly adjusted (Fig. 4).

Tangential view instructs femoral neck screw guide wire implantation. (A) Intra-operative the lateral views showed the posterosuperior screw guide wire were contained within the femoral neck. (B) Intra-operative the tangential view showed the posterosuperior screw guide wire IOI. (C) Adjust the guidewire under the tangential view.
Bony violation during screws fixation has been widely reported in the orthopaedic literature. Routt et al. suggested iliosacral screw insertion into the sacral isthmus region required avoidance of IOI to reduce the risk of damage to the adjacent neurovascular structures13. Du et al. recommended the C2 pedicle screw IOI to provide multicortical 3-column rigid fixation in the patients with basilar invagination and atlantoaxial dislocation14. Ramesh et al. proposed anterior column lag screw IOI in the fixation of acetabular fractures to provide rigid stability and minimize the surgical duration, radiation exposure, and intra-operative complications15. A previous clinical study demonstrated the posterosuperior screws IOI incidence up to 54% in the inverted triangle cannulated screws fixation of femoral neck fractures. However, the sensitivity of the standard lateral view to identifying the posterosuperior screw IOI was only 39%6. In a cadaveric study, 2 orthopaedic traumatologists and 1 musculoskeletal radiologist determined that no screws radiographically breached the posterior and cranial cortex in 10 cadaver specimens under the standard femoral neck AP and lateral views. After dissection, 70% of the specimens emerged with the posterosuperior screw IOI16. Aibinder et al. proposed the use of the sequential fluoroscopic rollover images to detect an IOI position after placement of the posterosuperior guide wire into the femoral neck17. However, this technique significantly increases the frequency of intraoperative fluoroscopy, leading to surgeons-possible damage by occupational ionizing radiation exposure18,19. Therefore, this technique is not recommended for clinical applications. Adams et al. proposed placing the posterosuperior screw to the piriformis fossa inferior margin on AP view to avoid cortical breach during percutaneous screw fixation of femoral neck fractures5. However, we considered the screw location was a three-dimensional position so relying on the anatomical signatures on AP view alone was not credible, and our clinical cases validated the inaccuracy of this methodology (Fig. 3). In summary, no research was available to instruct guide wire implantation intraoperatively and thus avoid the femoral neck screw IOI.
However, the influence of IOI screws in the fixation of femoral neck fractures has not been clearly demonstrated. Femoral neck fractures frequently involve complications such as non-union and avascular necrosis, which are associated with disruption of the blood supply to the femoral head20. Conventionally, the superior retinacular artery (SRA) derived from the medial femoral circumflex artery is considered to be the main blood supply to the femoral head21,22. The SRA ran through the lateral retinaculum which had the form of a quadrilateral plate adjacent to the posterosuperior surface of the femoral neck23. The posterosuperior screw was “in–out–in” near the area where the superior retinacular artery enters the femoral neck, which means that there is a high risk of screw perforation invading the artery16. Due to the effects of the iatrogenic injury on the intraosseous vascular system, the blood supply of the femoral head is severely deteriorated, leading to non-union and secondary femoral head avascular necrosis24,25. Yuan demonstrated that the incidence of avascular necrosis and revision surgery in hips with and without IOI screws was 6% and 6%, respectively; however, due to the width of the confidence intervals, a true clinical difference could not be excluded6. We believe this consequence was also related to the small sample volume, and a long-term, large sample follow-up study on the relation between necrosis and iatrogenic injury will be necessary for the future.
The cross-sectional morphology of the femoral neck is displayed as a rotating forward ellipse26. With increasing osteoporosis, the trabeculae come to lie progressively more anterosuperior within the femoral neck, with a larger posterosuperior defect9. Therefore, the posterosuperior region is a risk area for bony violation during screw fixation of femoral neck fractures. This also explains that the screws appearing well contained in the standard view might have actually perforated the posterosuperior neck. It was worth mentioning that we found one patient with the inferior screw that was IOI in the postoperative CT (Fig. 5). Intraoperative standard AP and lateral fluoroscopy showed that the inferior screw was completely contained in the femoral neck, while the tangential view showed the inferior screw was IOI. This might be attributed to the inferior screw being implanted anteriorly and penetrated anteroinferior through the femoral neck, while the tangential fluoroscopy tangential to both the posterosuperior and anteroinferior cortices could reveal the accurate screw position.

(A,B) Intra-operative the AP and lateral views showed all screws were contained. (C) Intra-operative the tangential view showed the inferior screw IOI. (D,E) Postoperative plain radiographs showed all screws were contained. (F,G) Postoperative CT showed the inferior screw IOI. The red arrow represents the inferior screw IOI.
In our clinical practice, we also concluded certain experiences to avoid IOI. Apply tangential view as a conventional fluoroscopic angle to adjust the guidewire. We usually implant the posterosuperior screw lower than the anterosuperior screw to avoid bony violation, thus creating an oblique triangle configuration27. Emphasize the importance of intraoperative manipulation of the senses. A sudden loss of resistance during the cannulated screw guidewire insertion, followed by a sudden reappearance of resistance, may suggest the guidewire IOI. When the femoral neck is narrow, such as in elderly women, we will replace the posterosuperior crew with a 6.5 mm diameter screw to guarantee mechanical strength while reducing the risk of the posterosuperior femoral neck screw IOI.
However, there were some limitations to this study. This was a retrospective study and the number of cases was minor, which may be responsible for the high sensitivity of the tangential view to detect the posterosuperior femoral neck screw IOI. Therefore, a larger multicenter prospective study is necessary in the future to evaluate the sensitivity and sensitivity of the tangential view to detect the posterosuperior femoral neck screw IOI. Due to the different anatomy of the population, 150° tangential fluoroscopy may not apply to all patients. A large sample of femoral neck cross-sectional anatomical studies is necessary to obtain a more accurate tangential position projection angle. Intraoperative anatomical reduction is paramount, and non-anatomical reduction can also lead to the inaccuracy of the tangential view. This was only a radiographic comparison study, and we hope to conduct a larger multicenter study subsequently to investigate the effect of IOI screws on the clinical prognosis and complications of femoral neck fractures.
Conclusion
Intra-operative tangential view of 150° can effectively identify the posterosuperior screw IOI in the cannulated screws fixation of femoral neck fractures. Based on our study, we highly recommend the tangential view as a routine intraoperative fluoroscopic angle to detect the posterosuperior screw IOI.
Data availability
All data generated or analyzed during this study are included in this published article.
Abbreviations
- AP:
-
Anteroposterior
- IOI:
-
In–out–in
- CT:
-
Computed tomography
- 2D:
-
Two dimensions
- 3D:
-
Three dimensions
- AO/OTA:
-
AO foundation and orthopaedic trauma association
- SRA:
-
Superior retinacular artery
References
Bhandari, M. & Swiontkowski, M. Management of acute hip fracture. N. Engl. J. Med. 377, 2053–2062. https://doi.org/10.1056/NEJMcp1611090 (2017).
Bout, C. A., Cannegieter, D. M. & Juttmann, J. W. Percutaneous cannulated screw fixation of femoral neck fractures: The three point principle. Injury 28, 135–139. https://doi.org/10.1016/s0020-1383(96)00161-1 (1997).
Lindequist, S. & Tornkvist, H. Quality of reduction and cortical screw support in femoral neck fractures. An analysis of 72 fractures with a new computerized measuring method. J. Orthop. Trauma 9, 215–221. https://doi.org/10.1097/00005131-199506000-00006 (1995).
Chen, S. Y. et al. A new fluoroscopic view for evaluation of anteromedial cortex reduction quality during cephalomedullary nailing for intertrochanteric femur fractures: The 30 degrees oblique tangential projection. BMC Musculoskelet. Disord. 21, 719. https://doi.org/10.1186/s12891-020-03668-6 (2020).
Adams, J. D. J. Jr., Walker, J. B. & Loeffler, M. Avoid the in-out-in posterosuperior femoral neck screw: The use of the piriformis fossa radiographic landmark. J. Orthop. Trauma https://doi.org/10.1097/BOT.0000000000002288 (2021).
Yuan, B. J. et al. High incidence of “in-out-in” posterosuperior screws after cannulated screw fixation of femoral neck fractures. Eur. J. Orthop. Surg. Traumatol. 30, 1417–1420. https://doi.org/10.1007/s00590-020-02717-z (2020).
Zhang, R. Y. et al. The oval-like cross-section of femoral neck isthmus in three-dimensional morphological analysis. Orthop. Surg. 13, 321–327. https://doi.org/10.1111/os.12914 (2021).
Zhang, Y. Q., Chang, S. M., Huang, Y. G. & Wang, X. The femoral neck safe zone: A radiographic simulation study to prevent cortical perforation with multiple screw insertion. J. Orthop Trauma 29, e178-182. https://doi.org/10.1097/BOT.0000000000000239 (2015).
Hammer, A. The structure of the femoral neck: A physical dissection with emphasis on the internal trabecular system. Ann. Anat. 192, 168–177. https://doi.org/10.1016/j.aanat.2010.02.007 (2010).
Su, Y. et al. An irreducible variant of femoral neck fracture: A minimally traumatic reduction technique. Injury 42, 140–145. https://doi.org/10.1016/j.injury.2010.05.008 (2011).
Wang, Z. et al. How to get better TAD? Relationship between anteversion angle of nail and position of femoral neck guide pin during nailing of intertrochanteric fractures. BMC Musculoskelet. Disord. 21, 512. https://doi.org/10.1186/s12891-020-03518-5 (2020).
Jia, X., Zhang, K., Qiang, M. & Chen, Y. The accuracy of intra-operative fluoroscopy in evaluating the reduction quality of intertrochanteric hip fractures. Int. Orthop. 44, 1201–1208. https://doi.org/10.1007/s00264-020-04533-w (2020).
Routt, M. L. Jr., Simonian, P. T., Agnew, S. G. & Mann, F. A. Radiographic recognition of the sacral alar slope for optimal placement of iliosacral screws: A cadaveric and clinical study. J. Orthop. Trauma 10, 171–177. https://doi.org/10.1097/00005131-199604000-00005 (1996).
Du, Y. Q., Yin, Y. H., Qiao, G. Y. & Yu, X. G. C2 medial pedicle screw: a novel "in-out-in" technique as an alternative option for posterior C2 fixation in cases with a narrow C2 isthmus. J. Neurosurg Spine. 1–7. https://doi.org/10.3171/2020.2.SPINE191517 (2020).
Sen, R. K. et al. A safe technique of anterior column lag screw fixation in acetabular fractures. Int. Orthop. 36, 2333–2340. https://doi.org/10.1007/s00264-012-1661-z (2012).
Hoffmann, J. C. et al. Is the cranial and posterior screw of the “inverted triangle” configuration for femoral neck fractures safe?. J. Orthop. Trauma 33, 331–334. https://doi.org/10.1097/BOT.0000000000001461 (2019).
Aibinder, W. R., Yuan, B. J., Cross, W. W. 3rd. & Parry, J. A. Sequential fluoroscopic rollover images reliably identify “in-out-in” posterosuperior screws during percutaneous fixation of femoral neck fractures. Eur. J. Orthop. Surg. Traumatol. 30, 1061–1065. https://doi.org/10.1007/s00590-020-02668-5 (2020).
Mastrangelo, G. et al. Increased cancer risk among surgeons in an orthopaedic hospital. Occup. Med. (Lond) 55, 498–500. https://doi.org/10.1093/occmed/kqi048 (2005).
Fujibayashi, S. et al. An observational survey of nail and skin of spine surgeons-possible damage by occupational ionizing radiation exposure. Spine Surg. Relat. Res. 5, 359–364. https://doi.org/10.22603/ssrr.2020-0204 (2021).
Large, T. M., Adams, M. R., Loeffler, B. J. & Gardner, M. J. Posttraumatic avascular necrosis after proximal femur, proximal humerus, talar neck, and scaphoid fractures. J. Am. Acad. Orthop. Surg. 27, 794–805. https://doi.org/10.5435/JAAOS-D-18-00225 (2019).
Lazaro, L. E., Klinger, C. E., Sculco, P. K., Helfet, D. L. & Lorich, D. G. The terminal branches of the medial femoral circumflex artery: The arterial supply of the femoral head. Bone Joint J. 97-B, 1204–1213. https://doi.org/10.1302/0301-620X.97B9.34704 (2015).
Dewar, D. C. et al. The relative contribution of the medial and lateral femoral circumflex arteries to the vascularity of the head and neck of the femur: A quantitative MRI-based assessment. Bone Joint J. 98-B, 1582–1588. https://doi.org/10.1302/0301-620X.98B12.BJJ-2016-0251.R1 (2016).
Gojda, J. & Bartonicek, J. The retinacula of Weitbrecht in the adult hip. Surg. Radiol. Anat. 34, 31–38. https://doi.org/10.1007/s00276-011-0829-3 (2012).
Wang, Z., Gu, L. & Cheng, L. Open reduction and internal fixation and intraoperative exploration of the superior retinacular arterial system in young adults garden III femoral neck fracture: A 10 case report. Ann. Plast. Surg. 84, S222–S224. https://doi.org/10.1097/SAP.0000000000002364 (2020).
Zhao, D. et al. Epiphyseal arterial network and inferior retinacular artery seem critical to femoral head perfusion in adults with femoral neck fractures. Clin. Orthop. Relat. Res. 475, 2011–2023. https://doi.org/10.1007/s11999-017-5318-5 (2017).
Zhu, Q., Shi, B., Xu, B. & Yuan, J. Obtuse triangle screw configuration for optimal internal fixation of femoral neck fracture: An anatomical analysis. Hip. Int. 29, 72–76. https://doi.org/10.1177/1120700018761300 (2019).
Zhang, R. Y. et al. The oblique triangle configuration of three parallel screws for femoral neck fracture fixation using computer-aided design modules. Sci. Rep. 12, 325. https://doi.org/10.1038/s41598-021-03666-1 (2022).
Acknowledgements
We would like to thank Jiahui Liang for his assistance in the data collection and statistics process.
Author information
Authors and Affiliations
Contributions
J.Z. and X.T. conceived this idea, develop the proposal, perform the analysis, and prepared the manuscript. J.Z. collected the data and polished the language of the article. All authors have read and approved this final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhang, J., Tang, X. The application of the 150° oblique tangential fluoroscopic view to detect the posterosuperior femoral neck screw in–out–in intraoperatively. Sci Rep 12, 12790 (2022). https://doi.org/10.1038/s41598-022-17221-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-17221-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
