
Abstract
An updated exploration of the burden of thyroid cancer across a country is always required for making correct decisions. The objective of this study is to present the thyroid cancer burden and attributed burden to the high Body Mass Index (BMI) in Iran at national and sub-national levels from 1990 to 2019. The data was obtained from the GBD 2019 study estimates. To explain the pattern of changes in incidence from 1990 to 2019, decomposition analysis was conducted. Besides, the attribution of high BMI in the thyroid cancer DALYs and deaths were obtained. The age-standardized incidence rate of thyroid cancer was 1.57 (95% UI: 1.33–1.86) in 1990 and increased 131% (53–191) until 2019. The age-standardized prevalence rate of thyroid cancer was 30.19 (18.75–34.55) in 2019 which increased 164% (77–246) from 11.44 (9.38–13.85) in 1990. In 2019, the death rate, and Disability-adjusted life years of thyroid cancer was 0.49 (0.36–0.53), and 13.16 (8.93–14.62), respectively. These numbers also increased since 1990. The DALYs and deaths attributable to high BMI was 1.91 (0.95–3.11) and 0.07 (0.04–0.11), respectively. The thyroid cancer burden and high BMI attributed burden has increased from 1990 to 2019 in Iran. This study and similar studies’ results can be used for accurate resource allocation for efficient management and all potential risks’ modification for thyroid cancer with a cost-conscious view.
Similar content being viewed by others

Introduction
Thyroid cancer is the most prevalent endocrine cancer world-wide1. Globally, there were approximately 233,846 (95% Uncertainty Interval [UI]: 211,636–252,806) incident cases of thyroid cancer and 45,575 (41,289–48,775) deaths among all-ages in 2019. Thyroid cancer was accounted for approximately 1,231,841 (1,113,585–1,327,064) Disability-Adjusted Life Years (DALYs) in the same year2. Since 1990, thyroid cancer incidence is the most rapidly rising incidence among all cancers. The overall change in incidence of this cancer due to the age structure, population growth, and the incidence rate is 99% from 2005 to 20153. Moreover, thyroid cancer deaths and DALYs were also increased by 63.75% and 88.79%, respectively, among all-ages and both sexes2. Therefore, assessing the burden of thyroid cancer at national and subnational levels as well as global level could assist in appropriate policy makings and identifying new priorities in resource allocation.
Plus, there are controversies in diagnosis and treatment of thyroid cancer in the world4 and These controversies might lead to over-managing5,6. Plus, thyroid cancer treatments include invasive approaches that are not devoid of side effects6. Hence, assessing the burden of thyroid cancer is not only a matter of resource allocation but also it might help in reducing side effects of over-managements by providing the big picture to the clinicians.
According to the previous studies, Iran follows a similar trends in thyroid cancer incidence, deaths, and DALYs7,8. However, the increase in the incidence could be a result of population growth and aging as well as increased age-specific incidence rate9. Hence, there is always a requirement for an updated, precise, and detailed data at national and sub-national levels to explore the pattern of thyroid cancer burden across a country for making timely and correct decisions.
It is also essential to identify associated risk factors to the thyroid cancer and their relative importance in the disease burden. Quantifying and tracking the prevalence of a risk factor could help in the risk modification in various locations. This objective could be accomplished by measuring the risk attributable DALYs10. The suggested risk factors by the literature are iodine intake, nitrate contamination, radiation exposure, vitamin D deficiency, and high BMI11,12,13,14,15,16,17. However, according to the Global Burden of Disease (GBD) study, high Body Mass Index (BMI) is the only established risk factor for thyroid cancer18,19. It has also been established that this risk factor has an increasing pattern in Iran20.
To the best of our knowledge, this is the first report of descriptive epidemiology of thyroid cancer in Iran at national and subnational levels. This study presents the thyroid cancer incidence, prevalence, deaths, DALYs, Years of Life Lost (YLLs), Years Lived with Disability (YLDs), and deaths, DALYs, YLLs, and YLDs attributed to the high Body Mass Index (BMI) in Iran and among its provinces from 1990 to 2019. The aforementioned indices are presented for both sexes, different age groups, and Socio-demographic Index (SDI) levels across the country.
Materials and methods
Overview
In this paper, thyroid cancer incidence, prevalence, deaths, DALYs, YLLs, and YLDs are reported using the Global Burden of Disease (GBD) 2019 study estimates in Iran at national and sub-national levels in 31 provinces from 1990 to 2019. These indices are also calculated in age-standardized rates except in decomposition analysis (that are crude rates) and reported as rates per 100,000 in the population. Moreover, the risks attributable DALYs, Deaths, YLLs, and YLDs to high BMI are presented across the country. Mortality to Incidence Ratio (MIR) was also calculated for each province among males, females and both sexes through dividing Age-Standardized Death Rate (ASDR) by Age-Standardized Incidence Rate (ASIR). Data analysis, tables, and demonstrations were conducted using R statistical packages v3.4.3 (http://www.r-project.org, RRID: SCR_001905) and presented with 95% Uncertainty Intervals (UI).
Data source
GBD 2019 study2 estimated incidence, prevalence, mortality, DALYs, YLLs, and YLDs of 396 disease and injuries for 23 age groups; males, females, and both sexes combined; and 204 countries and territories that were grouped into 21 regions and seven super-regions, and sub-national data of some countries including Iran. GBD 2019 study is in agreement with the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) statement and relies on various data sources for each disease. After that, data is processed and revised to correct biases and modeled to generate the estimates2. More data regarding to the results of this study is available from the GBD Results Tool21.
Decomposition analysis
Three factors contribute to the change in thyroid cancer incidence from 1990 to 2019. The change results from population growth, population aging, and age-specific increase in incident cases. However, these factors contribute to the change of incidence to different extents. To study the extent of contribution of each factor following steps were taken. First, the age structure of the population and age-specific incidence of thyroid cancer rates in 1990 were applied to the population size of 2019. Second, the age-specific incidence rates of thyroid cancer in 1990 were applied to the age structure and population size in 2019. The difference between the numbers of incident cases in these two steps is attributable to the changes in age structure from 1990 to 2019. On the other hand, the difference between the first step and the actual incident cases in 1990 is attributable to the population growth. Finally, the difference between incident cases of the second step and the actual incidence in 2019 is attributable to the changes in age-specific incidence rates9.
Attributable risk estimation
Since risk modification is a strategy toward preventing a disease, it is crucial yet challenging to track the burden attributable to the pertinent risk factors. Accordingly, the high BMI is the only risk factor reported for thyroid cancer by the GBD study after the causal evidence met the World Cancer Research Fund International (WCRF) grades of convincing evidence18,19. Hence, DALYs, deaths, YLLs, and YLDs attributable to the high BMI in Iran are reported in this study. The details of the calculation of the risk attribution are discussed elsewhere10. In brief, after determining the risk-outcome pair, the distribution of exposure for the risk by age, sex, location, and year was estimated. Then, the Population Attributable Fraction (PAF) and attributable-burden was estimated. For example, the risk attributable DALYs were estimated by multiplying DALYs by the population attributable fraction of the risk-outcome pair for a specific age, sex, location, and year.
SDI levels
The SDI reflects socio-demographic development in a location. Three indices contribute to generating this index: average income per capita, average years of schooling among 15 years and older individuals, and the total fertility rate under the age of 2522. The first two are positively and the last one is negatively associated with SDI in a location. In this study, the SDI is categorized into five quintiles among Iran’s provinces: high SDI, high-middle SDI, middle SDI, low-middle SDI, and low SDI.
Ethics
This study was approved by the institutional review board of Endocrinology and Metabolism Research Institute at Tehran University of Medical Sciences (IR.TUMS.EMRI.REC.1400.030).
This study’s results are based on estimates from the GBD 2019 study and in accordance with relevant guidelines and regulations. The authors also confirm that data used in the present study is publicly available.
Results
Thyroid cancer in Iran at national level
The burden of thyroid cancer in Iran increased from 1990 to 2019 (Table 1 and Supplementary Table 1). The ASIR of thyroid cancer among both sexes was 1.57 (95% UI: 1.33–1.86) in 1990, 1.87 (1.64–2.17) in 2000, 2.54 (1.81–2.80) in 2010, and 3.63 (2.31–4.12) in 2019 per 100,000. This number increased 131% (53–191) from 1990 to 2019 and considering 10-year intervals, the highest change in ASIR of thyroid cancer was between 2010 and 2019 that was 43% (24–59) (Supplementary Table 2, Fig. 1). Disaggregated by sex, the age-standardized incidence rate in 2019 was 5.11 (3.08–5.96) and 2.15 (1.46–2.52) for females and males, respectively (Fig. 1). Among age groups for adults, the highest incident rate per 100,000 was in the 65 to 69 age group, whereas the lowest incident rate was in the 20 to 24 age group (i.e., 10.47 versus 1.02) (Fig. 2). The decomposition analysis of thyroid cancer in the country revealed that 342% of the total 493% increase in the all age’s incident cases between 1990 and 2019 was attributed to the increase in the age-specific incidence rate (Supplementary Table 3), whereas 107% and 44% of the total increase rate were attributable to the population aging and population growth, respectively.

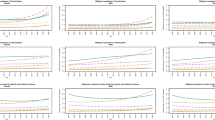
Time trend of the age-standardized and all-ages incidence, prevalence, deaths, and DALYs of thyroid cancer in Iran from 1990 to 2019 in by sex.

Thyroid cancer incidence, prevalence, deaths, and DALYs by age groups in 1990 and 2019 by sex.
The ASPR of thyroid cancer per 100,000 for both sexes was 30.19 (18.75–34.55) in 2019 which increased 164% (77–246) from 11.44 (9.38–13.85) in 1990. Females had a higher number of prevalent cases than males and the highest ASPR was in 65 to 69 age group in both sexes (Fig. 2). The ASDR of thyroid cancer was 0.49 (0.36–0.53) per 100,000 in 2019 and 0.42 (0.36–0.53) in 1990 (Table 1, Fig. 1). Females ASDR in 2019 was 0.56 (0.39–0.64) and males ASDR was 0.41 (0.32–0.45). The highest death rate was observed in the 80+ age group in both sexes (Fig. 2). In addition, thyroid cancer accounted for 13.16 (8.93–14.62) age-standardized DALYs rate per 100,000 in 2019 (Table 1, Fig. 1), of which 1.92 (0.96–3.11) is attributable to the high BMI. Furthermore, 0.07 (0.04–0.11) of the death rates were attributed to high BMI in this year. The detailed data on the burden of thyroid cancer and “its attributable risk factor” are presented in Tables 1 and 2, respectively.
Thyroid cancer in Iran at the province level
Thyroid cancer incidence
The ASIR of thyroid cancer varied across Iran from 1990 to 2019 (Fig. 3). Indeed, it ranged from 2.26 (1.77–2.79) (i.e. in Zanjan) to 4.86 (2.66–6.27) (i.e. in Alborz) among provinces in 2019 (Supplementary Table 1). Even though the ASIR increased in all provinces in this interval, the difference between the province with highest ASIR and the province with lowest ASIR was lower in 1990 (i.e. 2.40 versus 2.60). However, the extent of change varied among provinces from 8% (− 24 to 55) to 362% (85–652) (Supplementary Table 1, Fig. 4, and Supplementary Fig. 1). Although the significance of differences is discussable in some provinces, in both years, females had higher ASIR than males in all provinces. However, in 2019, all provinces had lower female to male ratio except two (i.e. Bushehr and Kerman) compared to 1990. The highest and the lowest female to male ratio in 1990 was 4.24 and 1.98, whereas in 2019, it was 4.02 and 1.33 respectively (Supplementary Table 1).

The age-standardized incidence and deaths of thyroid cancer in provinces of Iran (A: 1990, B: 2019), Republished from https://www.openstreetmap.org/ under a CC BY license, with permission from https://www.openstreetmap.org/copyright, original copyright 2022.

The changes in the thyroid cancer age-standardized incidence and deaths from 1990 to 2019 in both sexes in provinces of Iran: red arrow indicates upward ranking, blue arrow indicates downward ranking, and green arrow indicates monotone ranking.
The decomposition analysis of thyroid cancer at the province level showed that in all provinces except one (i.e. Tehran), the largest proportion of all-ages increase in both sex incidence cases was attributable to the increase in the age-specific incidence rate. In contrast, in Tehran, the largest proportion was attributed to population aging (Supplementary Table 3). Among provinces, Sistan and Baluchistan (1156.7%) had the highest increase attributable to the increase in age-specific incidence rate, Alborz (180.8%) had the highest increase attributable to the population aging, and Hormozgan (105%) had the highest increase attributable to the population growth.
Thyroid cancer prevalence
The ASPR of thyroid cancer also varied among provinces of Iran from 1990 to 2019. In 2019, it ranged from 18.42 (13.94–23.16) in Zanjan to 41.20 (21.75–53.68) in Alborz (Supplementary Table 1). The ASPR also increased in all provinces between these years, but the difference between the first and the last rank of ASPR among provinces was lower in 1990 (i.e. 19.94 versus 22.78). Although ASPR increased in all provinces, the extent of change varied from 15% (− 21 to 69) to 537% (146–1061) (Supplementary Table 1 and Supplementary Fig. 1). Females had higher ASPR than males in all provinces in both years. However, the uncertainty intervals of the ASPRs for females and males overlapped in some provinces. In 2019, all provinces had lower female to male ratio except one (i.e. Bushehr) compared to 1990, and the highest and lowest female to male ratio was 4.45 and 1.42. However, in 1990, it was 4.74 and 2.50 respectively (Supplementary Table 1).
Thyroid cancer deaths
Although there were minimal disparities, thyroid cancer causes relatively low death rates among the provinces of Iran (Fig. 3). In 2019, ASDR ranged from 0.36 (0.30–0.43) (i.e. in Zanjan) to 0.75 (0.39–0.92) (i.e. in Sistan and Baluchistan) (Supplementary Table 1). Despite the fact that ASDR increased in most provinces from 1990 to 2019, the difference between the first and the last rank of ASPR was lower in 1990 (i.e. 0.37 versus 0.39). Among the provinces in which ASDR increased between these years, the extent of change ranged from 12% (− 27 to 67) to 92% (− 11 to 191). However, the ASDR decreased in four provinces from − 0.2 (− 31.9 to 42.1) in Chahar Mahaal and Bakhtiari to − 32% (− 52 to − 6) in Tehran (Supplementary Table 1 and Supplementary Fig. 1). In 1990, females had higher ASDR than males in all provinces, whereas in 2019, males had higher ASDR in five provinces. However, the significance of these differences has to be further evaluated in most of the provinces. However, in 2019, all provinces had lower female to male ratio compared to 1990. Furthermore, the highest and lowest female to male ratio in 1990 was 2.75 and 1.34, and in 2019, it was 2.05 and 0.80 respectively (Supplementary Table 1). Moreover, the age-standardized Mortality to Incidence Ratio (MIR) was higher in males in all of the provinces from 1990 to 2019 (Supplementary Fig. 2).
Thyroid cancer DALYs
In the case of thyroid cancer DALYs among provinces of Iran, disparities were observable. Indeed, in 2019, it varied from 9.17 (7.62–10.92) in Zanjan to 21.30 (10.37–26.61) in Sistan and Baluchistan (Supplementary Table 1). Although, the age-standardized DALY rate increased in almost all provinces from 1990 to 2019, the difference between the province with the highest and the lowest rank was lower in 1990 (i.e. 9.69 versus 12.13). The age-standardized DALY rate was only decreased in Tehran [− 28% (95% UI: − 47 to − 2)]. Among the rest of provinces, the extent of change varied among provinces from 3% (− 28 to 54) to 122% (− 4 to 252) (Supplementary Table 1, and Supplementary Fig. 1). In 1990, females had higher age-standardized DALYs than males in all provinces. However, in 2019, in five provinces males had higher age-standardized DALYs. Similar to previous indices, the significance of the differences between females and males are discussable. In 2019, all provinces had lower female to male ratio compared to 1990. Moreover, the highest and the lowest female to male ratio in 1990 was 2.61 and 1.26, whereas in 2019, it was 2.10 and 0.78 respectively (Supplementary Table 1).
Thyroid cancer risk attributable DALYs
The high BMI is the only risk factor attributable to thyroid cancer introduced by the GBD studies. Here, the risk-attributable burden at national level will be reported at the Table 2, and the risk attributed burden at province level are presented in Supplementary Table 4.
The risk attributable DALY in 2019 varied from 1.21 (0.53–2.16) in Chahar Mahaal and Bakhtiari to 2.58 (1.04–4.50) in Sistan and Baluchistan (Fig. 5). The risk attributable DALY increased in all of the provinces from 1990 to 2019. However, the difference between the first and the last rank was lower in 1990 (i.e. 1.11 versus 1.37). Besides, the extent of change in this index ranged from 7% (− 24 to 57) to 262% (53–536). In 1990, females had higher risk attributable DALYs than males in all provinces, whereas in 2019, males had higher risk attributable DALYs in half of the provinces. However, the uncertainty intervals overlapped in all of the provinces in both years. In 2019, all provinces had lower female to male ratio compared to 1990. In addition, the highest and lowest female to male ratio in 1990 was 2.64 and 1.29, and in 2019, it was 1.61 and 0.62 respectively.

The thyroid cancer age-standardized DALYs attributed to high BMI in 1990 and 2019 in both sexes in provinces of Iran.
Thyroid cancer in SDI levels of Iran
The overall age-standardized rate of incidence, prevalence, deaths, and DALYs of thyroid cancer increased from 1990 to 2019 in almost all provinces in Iran from all five SDI levels (Fig. 6). However, in 2019, similar ASIRs, ASPRs, ASDRs, and DALYs were observed in provinces with different SDI levels. For example, in 2019, Isfahan [3.93 (2.32–5.03)] as a high SDI province and Sistan and Baluchistan [3.9 (1.92–4.99)] as a low SDI province were close together in case of ASIR of thyroid cancer. In contrast, East Azarbayejan [4.41 (2.52–5.66)] and Zanjan [2.25 (1.77–2.79)] with similar SDI levels were far from each other in the spectrum. However, in 1990, the SDI level was more associated with the thyroid cancer ASIR, and it was higher in higher SDI levels.

The thyroid cancer age-standardized incidence, prevalence, deaths, and DALYs in provinces of Iran in 1990 and 2019 by SDI levels.
Discussion
In this study, we have shown that although variability existed among provinces, the general burden of thyroid cancer increased from 1990 to 2019 in Iran. Moreover, the difference between provinces was higher, and female to male ratios were lower in 2019 comparing to 1990. The high BMI attributable DALYs also increased between these two years. As a matter of fact, based on the uncertainty intervals, the ASIR and the ASPR of thyroid cancer was higher in 2019 in Iran, whereas the ASDR, DALY, and the high BMI attributable DALY did not seem to be significantly different between these two years. This study’s results also suggest that SDI in a province is not significantly associated with the thyroid cancer burden in 2019. Indeed, some provinces with different SDIs had similar ASIRs. Hence, SDI had no effect on Thyroid cancer epidemiologic measures in Iran in 2019.
It is worth noting that the observed ranges of disparity in all of the indices among the provinces had overlapping uncertainty intervals. The implication of this finding is that there might not be significant differences in the burden of thyroid cancer among provinces, which needs to be evaluated in future studies.
One explanation in support of the disparities in the incidence rate among different provinces might be differences in the healthcare access and quality. The more aggressively a nodule is approached due to higher healthcare access, the more will the case finding be. In addition, it is believed that one of the factors affecting the increasing incidence and prevalence of thyroid cancer in Iran is the increasing number of skilled endocrinologists and radiologists8. Hence, the sub-clinical disease is more likely to be diagnosed23,24,25. However, since the availability of the diagnostic modalities might be affected by the SDI in a province26,27,28, an increase in the thyroid cancer ASIR in low SDI provinces, including Sistan and Baluchistan might not be solely due to the increased diagnostics. Besides, the decrease in the ASDR in four provinces, including Tehran and other two provinces nearby Tehran from 1990 to 2019, might be reflecting the inequities in the treatment of thyroid cancer across the country due to inequities in healthcare quality, possibly in favor of the capital. Nevertheless, based on the uncertainty intervals, the change from 1990 to 2019 might only be significant in Sistan and Baluchistan and only in the ASIR index. This province is a relatively deprived area in Iran and the increase in the ASIR in the recent years might be mostly due to the better diagnostics. Furthermore, the age structure of a population affects the incidence, prevalence, deaths, and DALYs of a disease. Specially, since Iran is a country in the Eastern Mediterranean Region of the WHO with a dynamic age composition29, the effect of the population age structure is strong in the findings of this study.
It is also worth noting that the observed trend of the rising thyroid cancer incidence was more significant between the years 1990 and 2010 compared to the years between 2010 and 2019. Although the duration between 1990 and 2010 was longer, this difference between these two time intervals might be due to the revision of the American Thyroid Association’s guidelines on thyroid cancer diagnosis and treatment and other countries developing similar guidelines in 201030. However, according to the GBD studies’ data source, there are limited number of data sources for thyroid cancer burden in Iran after 201031. Hence, most of the data between 2010 and 2019 is based on estimations. Therefore, more precise data needs to be acquired from future field studies.
The observed pattern and the increasing trend of thyroid cancer incidence might result from various factors. The improvement of medical techniques has occurred in diagnostics and it might have resulted in a higher rate of diagnosis of subtle malignancies32. Accordingly, the diagnosis of subtle malignancies leads to overdiagnosis which is estimated to account for over 80% of female thyroid cancer in countries including South Korea, Belarus, China, Italy, Croatia, Slovakia, and France between 2008 and 201233. Similarly, in Spain, the increased incidence of thyroid cancer is mostly attributed to the higher diagnosis rate34. However, in comparison with global rates, the increase in the incidence rate of thyroid cancer in Iran was relatively lower35. This finding might be explained by a relatively lower rate of overdiagnosis in Iran. In fact, although the increased ASIR and DALYs in other countries, including South Korea36 were mostly due to the higher diagnosis rates by cancer screening programs, this scenario does not apply to Iran because currently there are no thyroid cancer screening programs in the country. Since there are various burdens of thyroid cancer in the world, it might be a matter of the cost-effectiveness of thyroid cancer screening programs in different regions37,38. Even in South Korea, the necessity of these screenings remains controversial39. Thus, the cost-effectiveness of thyroid cancer screening programs in all countries including Iran needs future studies to be evaluated. Nevertheless, the role of increased diagnosis must not overshadow the role of other potential risk factors of thyroid cancer. Besides, advanced diagnostics are expensive and therefore, the increasing burden must not be solely attributed to overdiagnosis40. For example, in China, the exposure to endocrine-disrupting chemicals such as polychlorinated biphenyls (PCBs), asbestos, pesticides, and polybrominated diphenyl ethers (PBDEs) have been suspected to play role in the increasing incidence41,42. Another study in the Czech Republic also reported the role of other factors such as chemical exposures and iodine deficiency in the increasing burden of thyroid cancer43. Previously in Iran, radiation exposure and underlying benign thyroid disease have been found to be associated with the thyroid cancer incidence44,45. Further studies are required to assess the role of these factors more accurately in the increasing burden of thyroid cancer in Iran.
It is worth noting that despite the increasing incidence rates, the lower difference in death rates between 1990 and 2019 might be due to better clinical management of thyroid cancer in recent years42. The evidence in support of this assertion is that although the ASIR of thyroid cancer increased from 1990 to 2019, the age-standardized MIR has decreased in all provinces (Supplementary Fig. 1). However, even though Iranian health care system have been evidently successful to some extents, it is currently facing new challenges regarding the non-communicable disease and this may affect the performance of managing these disease including thyroid cancer46. Hence, more detailed analysis needs to be done in Iran at subnational level using indices measuring the quality of care47.
Finally, the increased burden attributable to the high BMI in Iran suggests that Iranian population is failing to manage this risk factor48. To explain the thyroid cancer burden disparities, disparities in other risk factors of thyroid cancer in different provinces needs to be assessed as well11,12,13,14,15,16. Accordingly, East Azarbayejan and Sistan and Baluchistan, which were among the provinces with the highest ASDRs and DALYs, had the lowest urinary iodine concentration in 201415. Moreover, Sistan and Baluchistan had the highest increase in ASIR, ASPR, DALYs, and ASDRs of thyroid cancer. On the other hand, Kurdistan was among the provinces with the highest urinary iodine concentration and the lowest ASIR, ASPR, ASDR, and DALYs. However, these are descriptive interpretations and more precise analyses are needed to evaluate the significance conclude that the aforementioned risk factors are correlated with the findings of this study.
Although the significance of the differences were debatable, the variability was also observed in different sexes. In each year from 1990 to 2019, the female gender had more ASIRs and ASDRs. Even though the reason behind the higher burden among the females in thyroid cancer remains unknown, there are some possible explanations. One explanation is that there are identical hormonal signaling pathways playing role in thyroid and breast cancer, both of which having the highest incidence in women49,50. Another explanation is that the female gender is associated with higher usage of diagnostic medical imaging modalities, especially after the age of 4551. However, in 2019, female to male ratio was lower in most of the provinces in case of thyroid cancer burden. Indeed, the high BMI attributable DALY was higher in males in half of the provinces in 2019. Thus, it might be deductible that the high BMI in males is resulting in the convergence of the thyroid cancer burden in females and males in Iran.
However, in the case of deaths, the higher rates among women was mostly due to the higher incidence. Following this theory, the age-standardized mortality to incidence ratio was calculated in all provinces of the country. Generally, the age-standardized mortality to incidence ratio was higher in males in the provinces of Iran during all years from 1990 to 2019. However, the significance of this difference needs to be evaluated as well. Indeed, a previous study (i.e., in 2009) had indicated that the survival rate was not significantly different between the two genders in Iran52. However, this study’s finding was consistent with the previous studies in the U.S, indicating that the survival was lower in the male population53. The differences in the health care seeking attitudes among men and women are probably the explanation behind these findings54.
There were also disparities among different age groups in the thyroid cancer incidence rate. The highest incidence rate of thyroid cancer in 2019 among men was in the 55 to 59 age group, whereas among women, it was in the 65 to 69 age group. In contrast, in 1990, the highest incidence rate was in the 75 to 79 age group among men and women. This finding might be due to the earlier diagnosis of thyroid cancer in recent years. However, this result was in contrast with the findings of the studies in the U.S community55. The results also indicate that thyroid cancer rarely affects children under the age of 15 in Iran8.
This study’s results are in agreement with the World Health Organization warning against thyroid cancer in the world56. The 0.049% (0.044–0.053) of total DALYs in 2019 was due to thyroid cancer57, however, only 0.003% of the cancer research budget is allocated to thyroid cancer in the world58. Therefore, resource allocation for this cancer research, subsequent management, and improving healthcare quality might need to be revised across the globe. Plus, the world is failing in lifestyle improvement10, and consequently leading to the increased distribution of risk factors (e.g., high BMI). Thus, risk modification as a strategy in managing the thyroid cancer burden remains challenging. However, it has to be elucidated that what makes provinces with low burden of thyroid cancer (e.g. Zanjan) different from the others and modify the affecting factors in other provinces.
Similar to the other GBD studies, the limitations of this study are mostly due to the data availability2. Despite the fact that GBD study relies on modeling to construct estimates, sufficient primary data is not available from every location due to weak registry systems and this lack of data might challenge the accuracy of estimations. Accordingly, representing the UI around estimates remains challenging because of the sparse data. Therefore, despite improvements in precision of the estimation models, there is always a need for better and more primary data collection. Another limitation of this study was considering high BMI as the only risk factor for thyroid cancer. Finding more causal connections between risks and outcomes would result in better explanation of the observed patterns and spotting proper intervention points. To accomplish this objective, other studies including Mendelian randomization studies could be used in the meta-regression10,59. Furthermore, thyroid cancer is not limited to a single histology and different histological types have different risk factors and outcomes. Hence, disaggregation of the thyroid cancer burden estimation by histology would provide more comprehensive insights towards this cancer60.
On the other hand, providing sub-national data, decomposition analysis, analyzing the effect of SDI on thyroid cancer burden, calculating MIR and attributed burden to a risk factor are among the strengths of this article.
In conclusion, this study illustrates that the thyroid cancer burden and high BMI attributed burden has increased from 1990 to 2019 in Iran. This study and similar studies’ results would help in the health systems appropriate resource allocation for managing the thyroid cancer burden and reduce the disparities in this regard. However, this resource allocation must have a cost-conscious view to avoid overmanaging and must be able to enhance the awareness of the medical community about overdiagnosis. In addition, the exposure to risk factors of this cancer including high BMI and the other abovementioned factors need to be reduced as much as possible, especially among the high-risk groups.
Data availability
The authors confirm that the datasets generated and/or analyzed during the current study are publicly available in the Global Health Data Exchange repository accessible from http://ghdx.healthdata.org/gbd-results-tool and https://vizhub.healthdata.org/gbd-compare/ with the GBD code of B.1.23. The GBD 2019 study was conducted by the Institute for Health Metrics and Evaluation (IHME). GBD 2019 study included 396 disease and injuries incidence, prevalence, mortality, DALYs, YLLs, and YLDs for 23 age groups; males, females, and both sexes combined; and 204 countries and territories that were grouped into 21 regions and seven super-regions. Furthermore, sub-national data of some countries including Iran is also available. Plus, the International Statistical Classification of Diseases and Related Health Problems 10th Revision, World Health Organization version (ICD-10) codes of morbidity and mortality (i.e. C73-C73.9, D09.3, D09.8, D34-D34.9, and D44.0) were used2.
Abbreviations
- ASDR:
-
Age-standardized death rate
- ASIR:
-
Age-standardized incidence rate
- ASPR:
-
Age-standardized prevalence rate
- DALYs:
-
Disability-adjusted life years
- GBD:
-
Global burden of disease
- MIR:
-
Mortality to incidence ratio
- SDI:
-
Socio-demographic index
- UI:
-
Uncertainty interval
- YLDs:
-
Years lived with disability
- YLLs:
-
Years of life lost
References
Stojsavljević, A. et al. Cadmium as main endocrine disruptor in papillary thyroid carcinoma and the significance of Cd/Se ratio for thyroid tissue pathophysiology. J. Trace Elem. Med. Biol. 55, 190–195 (2019).
Abbafati, C. et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 396(10258), 1204–1222 (2020).
Fitzmaurice, C. et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study Global Burden of Disease Cancer Collaboration. JAMA Oncol. 3, 524–548 (2017).
Vaccarella, S. et al. Worldwide thyroid-cancer epidemic? The increasing impact of overdiagnosis. N. Engl. J. Med. 375(7), 614–617 (2016).
Ito, Y. et al. Patient age is significantly related to the progression of papillary microcarcinoma of the thyroid under observation. Thyroid 24(1), 27–34 (2014).
McLeod, D. S. A., Sawka, A. M. & Cooper, D. S. Controversies in primary treatment of low-risk papillary thyroid cancer. Lancet 381, 1046–1057 (2013).
Fitzmaurice, C. et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017: A systematic analysis for the global burden of disease study. JAMA Oncol. 5(12), 1749–1768 (2019).
Safavi, A., Azizi, F., Jafari, R., Chaibakhsh, S. & Safavi, A. A. Thyroid cancer epidemiology in Iran: A time trend study. Asian Pac. J. Cancer Prev. 17(1), 407–412 (2016).
Pishgar, F., Ebrahimi, H., Saeedi Moghaddam, S., Fitzmaurice, C. & Amini, E. Global, Regional and National Burden of Prostate Cancer, 1990 to 2015: Results from the Global Burden of Disease Study 2015. J. Urol. 199(5), 1224–1232 (2018).
Abbafati, C. et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 396(10258), 1223–1249 (2020).
Aschebrook-Kilfoy, B., Grogan, R. H., Ward, M. H., Kaplan, E. & Devesa, S. S. Follicular thyroid cancer incidence patterns in the United States, 1980–2009. Thyroid 23(8), 1015–1021 (2013).
Sungwalee, W., Vatanasapt, P., Kamsa-ard, S., Suwanrungruang, K. & Promthet, S. Reproductive risk factors for thyroid cancer: A prospective cohort study in Khon Kaen, Thailand. Asian Pac. J. Cancer Prev. 14(9), 5153–5155 (2013).
Aceves, C., Anguiano, B. & Delgado, G. The extrathyronine actions of iodine as antioxidant, apoptotic, and differentiation factor in various tissues. Thyroid 23, 938–946 (2013).
Morris, L. G. T., Sikora, A. G., Tosteson, T. D. & Davies, L. The increasing incidence of thyroid cancer: The influence of access to care. Thyroid 23(7), 885–891 (2013).
Delshad, H., Mirmiran, P., Abdollahi, Z., Salehi, F. & Azizi, F. Continuously sustained elimination of iodine deficiency: A quarter of a century success in the Islamic Republic of Iran. J. Endocrinol. Investig. 41(9), 1089–1095 (2018).
Haghpanah, V. et al. Endocrine cancer in Iran: Based on cancer registry system. Indian J. Cancer. 43(2), 80–85 (2006).
Zhao, J. et al. Vitamin D deficiency as a risk factor for thyroid cancer: A meta-analysis of case-control studies. Nutrition 57, 5–11 (2019).
Gakidou, E. et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 390(10100), 1345–1422 (2017).
Stanaway, J. D. et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 392(10159), 1923–1994 (2018).
Rahmani, A. et al. Investigation of the prevalence of obesity in Iran: A systematic review and meta-analysis study. Acta Med. Iran. 53, 596–607 (2015).
GBD Results Tool|GHDx. http://ghdx.healthdata.org/gbd-results-tool (Accessed 11 Oct 2021).
Naghavi, M. et al. Global, regional, and national age-sex specifc mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 390(10100), 1151–1210 (2017).
Udelsman, R. & Zhang, Y. The epidemic of thyroid cancer in the United States: The role of endocrinologists and ultrasounds. Thyroid 24(3), 472–479 (2014).
Reitzel, L. R. et al. Trends in thyroid cancer incidence in Texas from 1995 to 2008 by socioeconomic status and race/ethnicity. Thyroid 24(3), 556–567 (2014).
Guay, B., Johnson-Obaseki, S., McDonald, J. T., Connell, C. & Corsten, M. Incidence of differentiated thyroid cancer by socioeconomic status and urban residence: Canada 1991–2006. Thyroid 24, 552–555 (2014).
Davies, L. & Welch, H. G. Current thyroid cancer trends in the United States. JAMA Otolaryngol. Head Neck Surg. 140(4), 317–322 (2014).
Pellegriti, G., Frasca, F., Regalbuto, C., Squatrito, S. & Vigneri, R. Worldwide increasing incidence of thyroid cancer: Update on epidemiology and risk factors. J. Cancer Epidemiol. 2013, 965212 (2013).
Wartofsky, L. Increasing world incidence of thyroid cancer: Increased detection or higher radiation exposure?. Hormones 9, 103–108 (2010).
GHO | Global Health Observatory Data Repository (Eastern Mediterranean Region) | Population—Data by WHO region. (WHO).
Haugen, B. R. et al. 2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association Guidelines Task Force on thyroid nodules and differentiated thyroid cancer. Thyroid 26(1), 1–133 (2016).
Advanced search | GHDx. http://ghdx.healthdata.org/advanced-search?field_geography_tid=Iran+%28Islamic+Republic+of%29&field_type_tid=All&field_keywords_tid=Thyroid+cancer&field_series_or_system_target_id=All&field_time_value%5Bmin%5D%5Byear%5D=1990&field_time_value%5Bmax%5D%5Byear%5D=2019 (Accessed 8 Feb 2021).
Brito, J. P. & Davies, L. Is there really an increased incidence of thyroid cancer?. Curr. Opin. Endocrinol. Diabetes Obes. 21(5), 405–408 (2014).
Li, M., Maso, L. D. & Vaccarella, S. Global trends in thyroid cancer incidence and the impact of overdiagnosis. Lancet Diabetes Endocrinol. 8(6), 468–470 (2020).
Rojo Álvaro, J. et al. Increased incidence of thyroid cancer in Navarra (Spain). Evolution and clinical characteristics, 1986–2010. Endocrinol diabetes y Nutr. 64(6), 303–309 (2017).
Bao, W. Q., Zi, H., Yuan, Q. Q., Li, L. Y. & Deng, T. Global burden of thyroid cancer and its attributable risk factors in 204 countries and territories from 1990 to 2019. Thorac. Cancer. 12(18), 2494–2503 (2021).
Deng, Y. J. et al. Global burden of thyroid cancer from 1990 to 2017. JAMA Netw. Open. 3(6), e208759 (2020).
Vaccarella, S. et al. The impact of diagnostic changes on the rise in thyroid cancer incidence: A population-based study in selected high-resource countries. Thyroid 25(10), 1127–1136 (2015).
Etzioni, R. & Gulati, R. Recognizing the limitations of cancer overdiagnosis studies: A first step towards overcoming them. J. Natl. Cancer Inst. 108(3), djv345 (2016).
Burki, T. K. Unnecessary thyroid cancer screening in South Korea. Lancet Oncol. 18(1), e6 (2017).
Modirian, M., Cheraghi, Z., Rahimzadeh, S., Moghaddam, S. S. & Jarrahi, A. M. Burden assessment of thyroid cancer in Iran from 1990 to 2010: Lessons obtained from global burden of disease report 2010. Asian Pac. J. Cancer Prev. 16(17), 7743–7748 (2015).
Romei, C. et al. Modifications in the papillary thyroid cancer gene profile over the last 15 years. J. Clin. Endocrinol. Metab. 97(9), E1758–E1765 (2012).
Cheng, F. et al. Burden of thyroid cancer from 1990 to 2019 and projections of incidence and mortality until 2039 in China: Findings from global burden of disease study. Front Endocrinol. 12, 738213 (2021).
Lukas, J., Drabek, J., Lukas, D., Dusek, L. & Gatek, J. The epidemiology of thyroid cancer in the Czech Republic in comparison with other countries. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 157(3), 266–275 (2013).
Parad, M. T., Fararouei, M., Mirahmadizadeh, A. R. & Afrashteh, S. Thyroid cancer and its associated factors: A population-based case-control study. Int. J. Cancer. 149(3), 514–521 (2021).
Moazezi, Z., Mahmoudi, M., Yahyahpour, Y. & Alaleh, A. R. Risk factors of thyroid cancer in Babol, northern Iran. Caspian J. Intern. Med. 2, 171–177 (2011).
Farzadfar, F. et al. Health system performance in Iran: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 399(10335), 1625–1645 (2022).
Azadnajafabad, S. et al. Global, regional, and national burden and quality of care index (QCI) of thyroid cancer: A systematic analysis of the Global Burden of Disease Study 1990–2017. Cancer Med. 10(7), 2496–2508. https://doi.org/10.1002/cam4.3823 (2021).
Vaisi-Raygani, A., Mohammadi, M., Jalali, R., Ghobadi, A. & Salari, N. The prevalence of obesity in older adults in Iran: A systematic review and meta-analysis. BMC Geriatr. 19(1), 1–9 (2019).
Bolf, E. L., Sprague, B. L. & Carr, F. E. A linkage between thyroid and breast cancer: A common etiology?. Cancer Epidemiol. Biomark. Prev. 28, 643–649 (2019).
Roche, L. M., Niu, X., Pawlish, K. S. & Henry, K. A. Thyroid cancer incidence in New Jersey: Time trend, birth cohort and socioeconomic status analysis (1979–2006). J. Environ. Public Health. 2011, 850105 (2011).
Kent, W. D. T. et al. Increased incidence of differentiated thyroid carcinoma and detection of subclinical disease. CMAJ 177(11), 1357–1361 (2007).
Mohagheghi, M. A., Mosavi-Jarrahi, A., Malekzadeh, R. & Parkin, M. Cancer incidence in Tehran metropolis: The first report from the Tehran population-based cancer registry, 1998–2001. Arch. Iran. Med. 12, 15–23 (2009).
Kilfoy, B. A. et al. Gender is an age-specific effect modifier for papillary cancers of the thyroid gland. Cancer Epidemiol. Biomark Prev. 18(4), 1092–1100 (2009).
Mazzaferri, E. L. & Jhiang, S. M. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am. J. Med. 97(5), 418–428 (1994).
Nilubol, N., Zhang, L. & Kebebew, E. Multivariate analysis of the relationship between male sex, disease-specific survival, and features of tumor aggressiveness in thyroid cancer of follicular cell origin. Thyroid 23(6), 695–702 (2013).
Alok Pathak, K., Leslie, W. D., Klonisch, T. C. & Nason, R. W. The changing face of thyroid cancer in a population-based cohort. Cancer Med. 2(4), 537–544 (2013).
GBD Compare | IHME Viz Hub. https://vizhub.healthdata.org/gbd-compare/ (Accessed 5 Jan 2021).
Jemal, A. et al. Global cancer statistics. CA Cancer J. Clin. 61(2), 69–90 (2011).
Millwood, I. Y. et al. Conventional and genetic evidence on alcohol and vascular disease aetiology: A prospective study of 500 000 men and women in China. Lancet 393(10183), 1831–1842 (2019).
Chmielik, E. et al. Heterogeneity of thyroid cancer. Pathobiology 85(1–2), 117–129 (2018).
Acknowledgements
The authors thank the Institute for Health Metrics and Evaluation (IHME) for data provision. Also, authors sincerely thank all the collaborators contributed to this study at Non-Communicable Diseases Research Center (NCDRC) of Endocrinology and Metabolism Research Institute (EMRI) at Tehran University of Medical Sciences.
Author information
Authors and Affiliations
Consortia
Contributions
Providing data or critical feedback on data sources H.A., A.A., J.A., S.S.A., S.A., A.D., M.D., Z.E., F.F., A.G., P.G., N.H., S.H., B.M., E.M.N., A.H.M., M.N., R.P., M.R., N.R., J.S., S.S., and I.Z. Developing methods or computational machinery H.A., A.A., J.A., S.S.A., S.A., A.D., M.D., Z.E., F.F., A.G., P.G., S.H., H.J., A.K., M.K., R.K., B.L., B.M., E.M.N., A.M., R.M., A.H.M., M.Naghavi, M.Naghipour, F.P.K., R.P., S.R., M.M.R., M.R., Nazila.R., Negar.R., Nima.R., S.S.M., S.S., J.S., and R.V.. Providing critical feedback on methods or results H.A., A.A., S.A., F.I.A., S.A., M.A., A.D., M.D., M.D., Z.E., F.F., N.H., S.H., H.J., A.K., R.K., S.L., N.M., B.M., A.M., A.H.M., M.Naghavi, M.Naghipour, J.N., R.P., M.R., Nazila.R., Nima.R., S.S.M., S.S., J.S., S.S., S.M.T., R.V., and I.Z.. Drafting the work or revising it critically for important intellectual content M.A., Z.A., H.A., A.A., S.Ahmadi, S.A., F.I.A., A.A.A., J.A., S.S.A., S.A., M.A., A.A.J., S.B., A.B., A.D., M.D., M.D., Z.E., F.F., A.F., S.G., A.G., P.G., M.G., N.H., A.H., H.J., A.K., M.K., R.K., M.K., A.K., F.K., H.R.K., B.L., S.L., S.M., M.M., N.M., B.M., E.M.N., S.M., E.M., A.M., R.M., A.H.M., S.M., M.Naghavi, H.N. J.N., S.A.N., M.N., A.N., F.P.K., R.P., S.Rafiei, S.R., M.M.R., M.S.R., M.R., Nazila.R., Negar.R., Nima.R., S.Rezaei, S.Rezazadeh-Khadem, F.S., S.S.M., M.S., A.S., S.S., J.S., S.S., R.S., P.S., S.M.T., R.V., and I.Z.. Managing the estimation or publications process M.A., B.L., A.H.M., M.Naghavi, Nazila.R., Negar.R., and S.S.M.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Azangou-Khyavy, M., Saeedi Moghaddam, S., Rezaei, N. et al. National, sub-national, and risk-attributed burden of thyroid cancer in Iran from 1990 to 2019. Sci Rep 12, 13231 (2022). https://doi.org/10.1038/s41598-022-17115-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-17115-0
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
