
Abstract
Air quality is heavily influenced by rising pollution distribution levels which are a consequence of many artificial activities from numerous sources. This study aims to determine the relationship between meteorological data and air pollutants. The health effects of long-term PM2.5 were estimated on expected life remaining (ELR) and years of life lost (YLL) indices in Ratchaburi province during the years 2015–2019 using AirQ+ software. Values obtained from the PM2.5 averaging, and YLL data were processed for the whole population in the age range of 0–29, 30–60 and over 60. These values were entered into AirQ+ software. The mean annual concentration of PM2.5 was highly variable, with the highest concentration being 136.42 μg/m3 and the lowest being 2.33 μg/m3. The results estimated that the highest and lowest YLL in the next 10 years for all age groups would be 24,970.60 and 11,484.50 in 2017 and 2019, respectively. The number of deaths due to COPD, IHD, and stroke related to long-term exposure to ambient PM2.5 were 125, 27 and 26, respectively. The results showed that older people (> 64) had a higher YLL index than the groups aged under 64 years. The highest and lowest values for all ages were 307.15 (2015) and 159 (2017). Thus, this study demonstrated that the PM2.5 effect to all age groups, especially the the elderly people, which the policy level should be awared and fomulated the stratergies to protecting the sensitive group.
Similar content being viewed by others


Introduction
The most detrimental factors that can influence the rise of air pollutants in urban cities are emissions from human activities1 such as power plants, industrial facilities, transportation, agriculture and waste treatment. In Thailand, there are three major sources of air pollution: vehicle emissions in the cities, biomass burning in rural and border areas,and emissions from industrial facilities2. Many research studies have found that there is a relationship between seasonal changes and their effects on air pollution. For example, the climate of summertime conditions contribute to the increase of particulate matter (PM2.5). Heat triggers more conditioning power usage in facilities and vehicles, thereby increasing particle emission, sunlight and heat transforms and worsen air pollution by triggering reactions between atmospheric particles such as nitrogen oxide and oxygen, forming ozone and transforming primary particles into even smaller particles which are hazardous to health. Heat waves and poor air movement create stagnant atmospheric conditions where air pollutants are trapped and accumulate over the ground level. Although indirectly, seasonal variations were significant contributors to human activities and air quality3,4. The studied by Ji et al. also demonstrated that heat waves enhance the impact of particulate matter on circulatory motality5. However, the temperature inversion also the remarkable factor that can trap the pollutant lead to higher pollutant concentration6. Additionally, winds influenced by seasonal variation can also affect air pollution by dispersing contaminants farther away from their source, nevertheless, higher winds in dry rural areas can generate dust7,8. The effects of these factors are shown clearly by a study in Beijing by Chen et al., and evidence has shown that seasonal changes are directly and indirectly associated with atmospheric pollution and air quality. During humid summer conditions, ozone concentration tends to increase with correlation to strong solar radiations, with intense photochemical reactions occurring atmospherically. Traffic during wintertime contributed to very high concentrations of nitrogen dioxide due to increased use of motor vehicles and coal combustion facilities, which produce atmospheric pollutants like sulfur dioxide and carbon monoxide. Wind fields have a crucial role in dispersing air contaminants particularly during heavily polluting conditions, with results suggesting that these dispersions mostly occurred during low wind speed circumstances (less than 1.5 m/s). Chen et al. have concluded that the winter and autumn were the seasons most polluted by PM2.5, PM10, SO2, NO2, and CO9. However, summer was most polluted by ozone as solar radiation-induced photochemical reactions and humid conditions contributed to the production of ozone during afternoons. Spatial patterns between air pollutants, where pollutant concentrations were much higher or lower in different regional areas of Beijing demonstrated the factor of areas with high levels of transportation. The correlation between wind profiles indicates that low wind speeds result in Beijing’s most heavily polluted incidences9. Thailand’s air pollution crisis results from 3 main sources: urban vehicle emissions, biomass burning, emissions from highly industrialized regions, and transboundary haze located in rural areas and borders10. Mueller applied risk estimates from the Global Exposure Mortality Model to calculate attributable mortality, and reported that 50,019 (95% confidence interval1: 42 189–57 849) deaths and 508 918 (95% CI 438 345–579 492) DALYs in 2016 was attributed to long-term PM2.5 exposure in Thailand11. Moreover, the studied in Thailand from Huang et al. mentioned the heatwaves related to mortality burden12.
Ratchaburi province is the one of Thailand’s central provinces, and is located west of Bangkok. This province is measured to be 5196 square kilometers wide with a population over Eight Hundred Thousand in 2018. The second contains the Tenasserim mountains and forests with an elevation of about 200–300 m. The last is the central area of this province is abundant with wetlands due to the river flowing through. Ratchaburi is one of the 14 provinces in Thailand with a large industrial estate. Industry here mainly deals with electricity, natural gas (Power plant), automotive, sugar, paper, and textiles, etc. The major commercial centers are distributed in the center of the province. Moreover, Ratchaburi is facing an air pollution crisis, due to also having a similar seasonal problem to Bangkok. The correlation between the varying air pollution data and varying seasonal changes in Ratchaburi, Thailand was drawn by analyzing statisticalresults collected from over a decade. In contrast to Beijing in China, Thailand undergoes three seasons that vary over each year; a dry season in mid-Febuary to mid- May, rainy/monsoon months from mid-May to mid-October, and a dry/cooler season during mid-October until mid-Febuary13. In the past years, several tools, including AirQ, BenMAP, Aphekom, and AirQ+ , and various organizations were developed for evaluating the health impacts along with the assessment of air pollution14. WHO developed the software AirQ+ for quantifying air pollution and its effect on health both in short-term and long-term. This research aims to survey the correlation between PM2.5 concentrations, meteorological parameters, and the estimate of all-cause annual mortality and mortality from cerebrovascular disease (stroke), ischemic heart disease (IHD), and chronic obstructive pulmonary disease (COPD) attributed to long-term exposure, and estimation of the health effects of PM2.5 on YLL indices in Ratchaburi from 2015 to 2019 using AirQ+ software.
Results
Air quality in Ratchaburi Province
The average concentration of PM2.5 was 26.86 μg/m3, which exceeding the NAAQS of Thailand (50 μg/m3) in some occasion, especially the dry season. However, severe amounts exceeding the WHO Air quality guideline values were also observed. The maximum 24-h average PM2.5 concentrations were 136.42 μg/m3, indicating that extreme particulate matter air pollution has occured in Ratchaburi province. CO, NO2 and SO2 concentrations in Ratchaburi were demonstrated to be under AQI standards. Ratchaburi had the O3 value at the minimum of 1.50 ppb, whereas the maximum concentration was 95.50 ppb. In some periods, the 8-h O3 presented over AQI. Additionally, the meteorological factor shows the lowest average wind speed (WS) being 1.2 m/s but the largest daily maximum would be 3.0 m/s. The average of Temperature (T) was 28.2 °C, and the highest of T was 33.2 °C. The annual average of wind direction (WD) blow from 245 degrees (Table 1).
Correlation of PM2.5 and other air quality parameters
The correlation between PM2.5 concentrations and the levels of PM10, CO, NO2 SO2 and O3 demonstrated the correlation coefficients of 0.91, 0.58, 0.57, 0.30, and 0.27, respectively (p-value < 0.001). Hence, the PM2.5, PM10, CO, SO2, and NO2 concentrations are negatively correlated with Temperature and WS, shown by the correlation coefficient of − 0.27 and − 0.12, respectively (p-value < 0.001) (Fig. 1).

Spearman rank correlations between PM2.5 concentrations and levels of other air quality parameters.
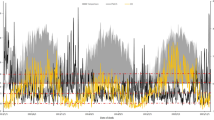
Time series of PM2.5 in Ratchaburi province
The PM2.5 concentration during 2015–2019 were presented in a similar pattern, the peak of 24 h concentration were observed twice a year, January to March and October to December as shown in Fig. 2. The annual average of PM2.5 concentration from 2015 to 2019 are shown in Table 1, along with the standard deviation (SD). In 2016, the highest PM2.5 concentration was 136.4 μg/m3, and the lowest was 2.3 μg/m3 in 2017. The annual concentration of PM2.5 and the amount of pollutants in the ambient air of Ratchaburi province was higher than the recommended value of WHO, and its variation ranged from 2.4 to 3.0 times higher than 10 μg/m3.

The pattern of PM2.5 concentration in Ratchaburi province during 2015–2019.
AirQ+ mordel estimations
Chronic obstructive pulmonary disease (COPD), ischemic heart disease (IHD) and stroke attributable cases
The AirQ+ estimation model demonstrated that people in Ratchaburi who have been exposed to long-term PM2.5 may have died due to COPD in the period of 2017–2018 for 125 cases as the annual average number. Moreover, the association beween PM2.5 and IHD was observed. The study found that 219 people may have died from IHD due to long-term exposure to PM2.5. In addition, there were 27 attributable cases per 100,000 for IHD due to PM2.5. Furthermore, the estimation model also demonstrated that 128 cases by an annual average may have died due to stroke-related complications due to long-term exposure to PM2.5. However, there were 26 attributable cases per 100,000 for stroke due to PM2.5 (Fig. 3).

Estimation model of attributable proportion and attributable cases of endpoint mortality due to PM2.5 exposure in Ratchaburi province.
Estimation of the health effects
The Year of Life Lost (YLL) was used as a health indicator in the development of public environmental policies14. Lin suggested that the essential to YLL can be used to identify appropriate interventions for risk management and improve the local efficacy for rapid response to air pollution15. Table 2 demonstrates the comparison between mortalies from PM2.5 between the years 2015 and 2019 in Ratchaburi Province. The highest YLLs were 243.6 years for the age of > 60 in 2019, and the lowest for the 0–29 age range is 5.1 years in 2017. The highest and lowest YLLs for all ages were 336.1 years in 2019 and 159.30 years in 2017, respectively. This health index was also examined for the next 10 years. The highest and lowest YLL in the next 10 years were 29,427.76 in 2019 for > 60 years age group and 476.60 in 2017 for agr range 0–29 years, respectively. Also, the highest and lowest values of this index were observed in the next 10 years for all ages: 31,819.90 in 2019 and 15,394.50 in 2017, respectively.
Discussion
In this study, the air quality and health data from Ratchaburi province were collected as secondary data. The analysis to determining the association of PM2.5 to metheorological parameters was performed using AirQ+ software designed by World Health Organization16. The annual average of PM2.5 in Ratchaburi was 26.86 μg/m3, which could be observed as exceeding the standard in some period but extreamly exceeds the WHO guildline standard. The data was consistent with the study of Fold et al. on the exceeding PM2.5 concentration in central Thailand (Bangkok)17. In addition to the relationship with human activity, especially the automobile derived the PM pollution18. In terms of gaseous pollutants, the annual average concentration were observed under the AQI. Our study showed the weak positive correlation between PM2.5 and temperature and humidity, while a studied from China and Hong Kong showed the major meteorological factors affect the accumulation, dispersion and concentration of PM2.519,20. From this point, it might be our sample size was small and the different in setting. The study of Vichit-Vadakan et al. showed that the gaseous pollutants i.e. nitrogen, nitric oxide and ozone were strong associated with several different mortality outcome21. Over the course of five years’ data collected, we detected the same pattern of PM2.5 concentration in every collected years with two peaks occurring twice a year in dry season that comply with previous studied that observed the PM2.5 obsvious exceed the standard in dry season22. The studied of Figueroa-Lara et al. showed that the PM2.5 concentration in warm-dry season were significantly higher than cold-dry season23. The AirQ+ estimation of health effect demonstrated The highest and lowest YLLs for all ages were 336.1 years in 2019 and 159.30 years in 2017 and for the next 10 years. Furthermore, the highest and lowest values of this index were observed in the next 10 years for all ages: 31,819.90 in 2019 and 15,394 in 2017. The result of this study was consistent with Zallaghi et al. on the health effects of long-term exposure to PM2.5 on ELR and YLL in Ahvaz, Iran and Zhu et al. on the effect of ambient air pollution load on YLL in Wuxi, China, using a nonlinear model (2012–2015)14,24. Moreover, the study site from China, Japan and South Korea also found the trend of total deaths were driven by population aging25. On the other hand, the study was inconsistent with Guo et al. study on the air pollution load on the YLL in Beijing, China26. However, when compared with studied from Middle Eastern populations, our study showed the YLL was lower dramatically27. Nevertheless, the different setting like in Europe, the overall air pollution that relate to morbidity and mortality have decrease considerably in the last three decades28. This study also showed the elderly population have high YLL value than others age group, due to the sensitive group. Consequently, the aging population might impact from medical resources and expenditures, and diseases by age group29.
This study was performed as a pilot study to investigating the PM2.5 effect on YLL in the western side border of Thailand. The results of this study could potentially be beneficial as platforms for further studies in other areas, provided with valid data, hence, convincing the environmental health department on the concern of the effects of particulate matter and pollutant parameters that could pose signifcant impacts on health.
Conclusions
This study aimed to evaluate the relationships of PM2.5 with meteorological in Ratchaburi province. The results of correlation analysis showed a weak positive correlation between PM2.5 concentrations and average monthly temperature (r = 0.42, P < 0.05) and average monthly humidity (r = 0.37, P < 0.05) in Ratchaburi province. For this purpose, AirQ+ as the health effects of long-term exposure to PM2.5 on YLL for 10 years. In dry period, PM2.5 concentration was over the WHO standard amount in all studies years. The results also showed that older people (> 60) had a higher YLL index than those group aged under 60 years. The highest and lowest values for all age were 336.10 (2019) and 159.30 (2017). On the other hand, the highest and lowest rates of this index were observed in the next 10 years for all ages: 31,819.90 in 2019 and 15,394 in 2017, respectively. The finding of this research can be used for further air quality and exposure measurement for reducing mortality.
However, the core limitation of this study is small sample size; the observed trend might not represent the overall population of the west part of country. The larger sample size and multi-area study should be considered to observing and verifying the trends. This study could be platform for research to increase the study scale, leading to environmental policy, health plan evaluation, as well as the welfare plan for population.
Methods and data collection
Study site
Air monitoring stations were positioned in Ratchaburi, located at the Regional Environment Office 8th. Ratchaburi province lies in Western Thailand and its border is connected to the Tanintharyi Region of Myanmar. The total population is over Eight Hundred Thousand and the area is 5196 square kilometers (Fig. 4). This city is suffering from air pollution from several sources such as powerplants, industry, agricultural activities, and transportation.

Location of sampling site in Ratchaburi province, Thailand.
Data collection
The PM2.5 and air quality parameters data were collected in the period of January 1st, 2015 to December 31st, 2019 from Pollution Control Department (PCD). The data was acquired at every hour from 1 am. to 11 pm. The data cleaning process was performed by excluding the invalid time and date. The health data in this study was collected in the period of 2015 to 2019 with the ICD10 code of J44 for Chronic Obstructive Pulmonary Diseses (COPD), I2 for Ischaemic Heart Disease (IHD) and I6 for stroke recorded by Ministry of Public Health, Thailand.
AirQ+ software
The valid PM2.5 and health data for over a 5 year period were entered into the AirQ+ software to calculate the YLL. The baseline incidence rate of all-cause mortalities and the averages data of PM2.5, Health data and YLL were converted to a .CSV file and inputs to AirQ+ software14. Table 3 shows a summary of inputted data to the AirQ+ software.
Statistical analysis
The descriptive statistic (mean, standard variation and varience) were used to analyze the annual air quality parameters to compare with the standard of Air Quality Index (AQI). The spearman rank correlation was performed to investigate the correlation of PM2.5 to other air quality parameters.
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Faculty of Tropical Medicine, Mahidol University TMEC 21-055 in compliance with Declaration of Helsinki, ICH guildline for Good Clinical Practice and other international Guildlines for Human Research Protection. Inform Consent is not applicable for this study due to the secondary data was obtained.
Data availability
Data used and analyzed in the manuscript will be made available upon request to corresponding author.
References
Martínez-Bravo, M. & Martínez-del-Río, J. Urban pollution and emission reduction. Sustain. Cities Commun. 2, 905–915 (2020).
Vichit-Vadakan, N. & Vajanapoom, N. Health impact from air pollution in Thailand: Current and future challenges. Environ. Health Perspect. 119, A197-198. https://doi.org/10.1289/ehp.1103728 (2011).
Duan, T. et al. Seasonal variation and sources of heavy metals in urban street dusts and river sediments of Dongluo River Watershed in Ji’nan City, China. KSCE J. Civ. Eng. 24, 1400–1410 (2020).
Chen, C. et al. The seasonal dynamics and the influence of human activities on campus outdoor microbial communities. Front. Microbiol. 10, 1579. https://doi.org/10.3389/fmicb.2019.01579 (2019).
Ji, S. et al. The interactive effects between particulate matter and heat waves on circulatory mortality in Fuzhou, China. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph17165979 (2020).
Beard, J. D. et al. Winter temperature inversions and emergency department visits for asthma in Salt Lake County, Utah, 2003–2008. Environ. Health Perspect. 120, 1385–1390. https://doi.org/10.1289/ehp.1104349 (2012).
Zobeck, T. M. & Van Pelt, R. S. Wind-induced dust generation and transport mechanics on a bare agricultural field. J. Hazard Mater. 132, 26–38. https://doi.org/10.1016/j.jhazmat.2005.11.090 (2006).
Xi, X. & Sokolik, I. N. Seasonal dynamics of threshold friction velocity and dust emission in Central Asia. J. Geophys. Res. Atmos. 120, 1536–1564. https://doi.org/10.1002/2014JD022471 (2015).
Chen, W., Yan, L. & Zhao, H. Seasonal variations of atmospheric pollution and air quality in Beijing. Atmosphere 6, 1753–1770 (2015).
Bucher, J. R., Thayer, K. & Birnbaum, L. S. The office of health assessment and translation: A problem-solving resource for the National Toxicology Program. Environ. Health Perspect. 119, A196-197. https://doi.org/10.1289/ehp.1103645 (2011).
Mueller, W. et al. A health impact assessment of long-term exposure to particulate air pollution in Thailand. Environ. Res. Lett. 16, 055018 (2021).
Huang, C. et al. Mortality burden attributable to heatwaves in Thailand: A systematic assessment incorporating evidence-based lag structure. Environ. Int. 121, 41–50. https://doi.org/10.1016/j.envint.2018.08.058 (2018).
Foocharoen, C., Peansukwech, U., Pongkulkiat, P., Mahakkanukrauh, A. & Suwannaroj, S. Effect of season on clinical outcomes of Thai systemic sclerosis: Analysis of the Thai national healthcare database. Mod. Rheumatol. 30, 1025–1032. https://doi.org/10.1080/14397595.2019.1702238 (2020).
Zallaghi, E., Goudarzi, G., Sabzalipour, S. & Zarasvandi, A. Effects of long-term exposure to PM2.5 on years of life lost and expected life remaining in Ahvaz city, Iran (2008–2017). Environ. Sci. Pollut. Res. Int. 28, 280–286. https://doi.org/10.1007/s11356-020-10393-z (2021).
Lin, X., Liao, Y. & Hao, Y. The burden associated with ambient PM2.5 and meteorological factors in Guangzhou, China, 2012–2016: A generalized additive modeling of temporal years of life lost. Chemosphere 212, 705–714 (2018).
Balidemaj, F., Isaxon, C., Abera, A. & Malmqvist, E. Indoor air pollution exposure of women in Adama, Ethiopia, and assessment of disease burden attributable to risk factor. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph18189859 (2021).
N, R. F. et al. An assessment of annual mortality attributable to ambient PM2.5 in Bangkok, Thailand. Int. J. Environ. Res. Public Health 17, 7298. https://doi.org/10.3390/ijerph17197298 (2020).
Jinsart, W. et al. Roadside particulate air pollution in Bangkok. J. Air Waste Manag. Assoc. 52, 1102–1110. https://doi.org/10.1080/10473289.2002.10470845 (2002).
Li, X., Feng, Y. & Liang, H. The impact of meteorological factors on PM2.5 variations in Hong Kong. IOP Conf. Ser. Earth Environ. Sci 78, 12003 (2017).
Meng, C. et al. The impact of meteorological factors on fine particulate pollution in Northeast China. Aerosol. Air Qual. Res. 20, 1618–1628 (2020).
Vichit-Vadakan, N., Vajanapoom, N., Ostro, B. & Committee, H. E. I. H. R. Part 3. Estimating the effects of air pollution on mortality in Bangkok, Thailand. Res. Rep. Health Eff. Inst. 2, 231–268 (2010).
Rana, M. M., Sulaiman, N., Sivertsen, B., Khan, M. F. & Nasreen, S. Trends in atmospheric particulate matter in Dhaka, Bangladesh, and the vicinity. Environ. Sci. Pollut. Res. Int. 23, 17393–17403. https://doi.org/10.1007/s11356-016-6950-4 (2016).
Figueroa-Lara, J. J. et al. Effect of platform subway depth on the presence of Airborne PM2.5, metals, and toxic organic species. J. Hazard Mater. 377, 427–436. https://doi.org/10.1016/j.jhazmat.2019.05.091 (2019).
Zhu, J. et al. The burden of ambient air pollution on years of life lost in Wuxi, China, 2012–2015: A time-series study using a distributed lag non-linear model. Environ. Pollut. 224, 689–697. https://doi.org/10.1016/j.envpol.2017.02.053 (2017).
Du, J. et al. A comparative study of the disease burden attributable to PM25 in China, Japan and South Korea from 1990 to 2017. Ecotoxicol. Environ. Saf. 209, 111856. https://doi.org/10.1016/j.ecoenv.2020.111856 (2021).
Guo, Y. et al. The burden of air pollution on years of life lost in Beijing, China, 2004–08: Retrospective regression analysis of daily deaths. BMJ 347, f7139. https://doi.org/10.1136/bmj.f7139 (2013).
Moradi, M. et al. Effect of long-term exposure to PM2.5 on years of life lost in a populated Middle Eastern city. Environ. Geochem. Health 43, 3229–3235. https://doi.org/10.1007/s10653-021-00827-z (2021).
Juginovic, A., Vukovic, M., Aranza, I. & Bilos, V. Health impacts of air pollution exposure from 1990 to 2019 in 43 European countries. Sci. Rep. 11, 22516. https://doi.org/10.1038/s41598-021-01802-5 (2021).
Kim, E. J., Jung, S. W., Kim, Y. E., Go, D. S. & Yoon, S. J. Assessing the impact of aging on burden of disease. Iran. J. Public Health 47, 33–38 (2018).
Acknowledgements
The authors are greatful to National Research Council of Thailand grant to KT. The Pollution Control Department (PCD), Ministry of Natural and resource of Thailand for the Air Quality data. We thanks to Ministry of Public health and National Statistical Office (NSO) of Thailand for all-cause of mortality and health data.
Author information
Authors and Affiliations
Contributions
W.K. and K.T. conceived the research; W.K. and K.T. acquired the data; W.K., K.T. designed the study; K.T., W.K., W.S., N.K. and R.S. analysed the data; K.T., W.K., S.N., and K.M. contributed to the interpretation of the data; W.K., W.S. and R.S. wrote the first draft of the manuscript; S.S. and K.T. writing-review and editing, all authors edited and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kliengchuay, W., Srimanus, W., Srimanus, R. et al. The association of meteorological parameters and AirQ+ health risk assessment of PM2.5 in Ratchaburi province, Thailand. Sci Rep 12, 12971 (2022). https://doi.org/10.1038/s41598-022-17087-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-17087-1
This article is cited by
-
Health impact pathways related to air quality changes: testing two health risk methodologies over a local traffic case study
Air Quality, Atmosphere & Health (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
