
Abstract
The aim of the present study is to explore the potential association between sleep quality and physical activity (PA) in women carriers of BRCA1/2 mutations. 63 women completed the Pittsburgh Sleep Quality Index (PSQI) and Godin Shepard Leisure-Time Physical Activity Questionnaire (GSL-TPAQ) and were included in the present cross-sectional analysis. Globally, women showed a PSQI score of 7.0 ± 3.6 and a GSL-TPAQ score of 22.8 ± 18.3. Good sleepers (PSQI score ≤ 5) showed significantly higher PA levels compared to bad sleepers (PSQI score > 5). Women in the higher tertile of GSL-TPAQ total score (≥ 27 METs/week) have a prevalence ratio (PR) of being a good sleeper of 2.85 (1.25–6.52, 95% confidence intervals) compared to women in the lower tertile (≤ 11 METs/week). These results were consistent in BRCA1 and BRCA2 women. Considering each single question of PA intensity, the PR of being a good sleeper by unit of increase of MET/week was higher and significant in women engaged in strenuous and moderate intensity PA. These results suggests a direct association between PA and sleep quality in women carriers of BRCA mutations.
Similar content being viewed by others

Introduction
Women carrying BRCA1/2 mutations have a 55% lifetime risk (penetrance) of developing breast cancer (BC)1 and the percentage is even higher at age 80 with 72% (95% CI 65–79%) for BRCA1 and 69% (95% CI 61–77%) for BRCA2 mutation carriers2. In these women the penetrance for ovarian cancer (OC) is also higher, in the order of 16–59%1,3. Epidemiological studies have suggested that the penetrance of BRCA1/2 genes may be modulated by a number of lifestyle factors. Greater body weight and life-long weight gain have been found associated with an increased BRCA penetrance4,5,6 especially for post-menopausal BC7,8 and for OC9. Consistently, higher fat mass, severe metabolic syndrome (MS) and high serum levels of insulin and insulin-like growth factor-I (IGF-I) affect BRCA penetrance10.
In recent years, sleep disorders are emerging environmental factors that influence the risk of BC11,12,13,14 and are co-morbid with the MS. The association between sleep and BC may be explained by misalignment of the molecular clock circadian rhythm that decreases melatonin secretion, an oncostatic agent and estrogen suppressor15,16,17 and by altering the regulation of glucose tolerance and insulin-sensitivity18,19. Sleep problems or bad sleep quality increase after BC diagnosis and treatment and are more common in BRCA1/2 mutation carriers compared to general population20. In fact, sleep disturbances are very frequent post-surgical symptoms (prevalence of 46.7%) in the BRCA carriers who chose risk reducing surgery for primary prevention21.
Physical activity (PA), especially during adolescence or early adulthood, affects BC risk in women with BRCA1/2 mutations22,23,24.
PA improves sleep quality and quantity and reduces obesity and MS parameters25,26,27,28. PA has a protective effect on sleep in both healthy subjects and cancer patients, including sporadic BC women26,29,30. PA is a synchronizer of the circadian rhythms by increasing the activity of sympathetic nervous system that modulates melatonin secretion31.
Furthermore, high intensity exercise upregulates the activity of peroxisome proliferator-activated receptor g (PGC-1a) that regulates the expression of the clock gene family, that are involved in sleep behaviour and insulin sensitivity32.
Despite the aforementioned evidence, there are no studies on the association of PA and sleep behaviour in women carriers of BRCA1/2 mutations. In the present paper we aim to explore the potential relationship between sleep quality and PA in a cohort of BRCA women who joined our dietary intervention trial10,33,34,35,36,37.
Materials and methods
Study design and participants
The design of the Italian multicenter dietary intervention trial on women carriers of BRCA1/2 mutations (reference number: NCT03066856) and its main results have been already described and reported10,33,34,35,36,37. In brief, the trial aimed to test if a 6-month dietary intervention based on the Mediterranean diet (MedDiet) with a moderate protein restriction significantly reduces potential modulators of BRCA1/2 penetrance such as body weight, IGF-I, insulin and main factors of MS. Eligible subjects were women aged 18–70 years, carriers of BRCA1/2 mutations, with or without a previous diagnosis of breast and/or ovarian cancer and without clinical evidence of metastases. Unaffected women who underwent bilateral prophylactic mastectomy did not enter the cohort study. All participants signed informed consent, filled questionnaires about their medical history and dietary habits, underwent anthropometric and body composition assessment and donated 20 mL of a blood sample. Anthropometric and body composition measurements, blood samples and dietary data were provided at baseline and the end of the dietary intervention. Among the 502 volunteers randomized into the trial, 63 women recruited between October 2018 and June 2019 also reported at baseline, before starting the dietary intervention, data on sleep and PA habits and were included in the present cross-sectional analysis.
The Ethics Committee of Fondazione IRCCS Istituto Nazionale dei Tumori di Milano approved the study (approval number: INT106/13).
Sleep and physical activity data collection
Two additional questionnaires for the assessment of sleep and PA habits (Pittsburgh Sleep Quality Index—PSQI and Godin Shepard Leisure-Time Physical Activity Questionnaire—GSL-TPAQ, respectively)38,39 were filled by the volunteers included in the present analysis.
The PSQI assesses sleep quality and habits in the previous 30 days. This is a retrospective self-report questionnaire, based on 19 items, in order to evaluate seven sleep components: (i) perceived sleep quality, (ii) sleep latency, (iii) sleep duration, (iv) sleep efficacy, (v) sleep disturbances, (vi) use of sleep medications, (vii) daytime dysfunctions. The score for each question ranges between 0 (no problem at all) and 3 (several problems). The sum of the seven components returns a final score from 0 to 21, with lower scores indicating a better sleep quality. The cut-off value of 5 divides participants into good sleepers (0–5) from bad sleepers (6–21). In addition, the numbers of hours spent in bed and sleeping and the sleep efficiency can be obtained from the questionnaire38,40.
The GSL-TPAQ39 assesses the amount of leasure time PA performed in the last seven days by including three questions about frequency of PA (number of activities/week). Each question refers to PA of different intensity (one question on mild, one on moderate and one on strenuous PA) which corresponds to specific Metabolic Equivalent of Task (MET) amount. Mild PA corresponds to 3 METs, moderate PA to 5 METs and Strenuous PA to 9 METs. The total GSL-TPAQ score is obtained using the following formula: (frequency of mild × 3) + (frequency of moderate × 5) + (frequency of strenuous × 9). If the final score is < 24, the subject is classified as inactive, while in the opposite case (≥ 24) is described as active39.
Statistical analysis
General characteristics of the study population were summarized by BRCA1/2 using frequencies or means and standard deviation (SD), and compared using χ2 or t tests, as appropriate.
By using the cut-off of the PSQI score, the study women were stratified into good (PSQI score ≤ 5) and bad sleepers (PSQI score > 5). Women’s metabolic and anthropometric characteristics were therefore summarized and compared with ANCOVA controlling for age and BMI. Since stratifying the population by disease status (affected and unaffected) or by age (below and above the median value of 48.8 years) we did not find any significant difference for all the variables under study, we decided to perform the analyses in the whole population and by BRCA mutation type.
As regards GSL-TPAQ, we considered both the total score and the results for each question of different PA intensity (strenuous, moderate, mild) separately in all the analyses.
We conducted a correlation analysis (Spearman coefficient) among all anthropometric, metabolic, sleep and PA data.
Since the aim of the present study was to describe potential associations between PA and sleep quality, we performed a binomial regression model to estimate the prevalence ratios (PRs) and 95% confidence intervals (CI) of being a good sleeper by increasing PA levels (increasing tertiles of GSL-TPAQ total score) in the whole population and in BRCA1 and BRCA2 women, controlling for age and BMI. We also repeated the PR analysis by MET/week increase taking into account each question of PA intensity (strenuous, moderate, mild).
A p-value of < 0.05 was taken as significant. The statistical analyses were carried out using STATA 14 (StataCorp–College Station, TX, USA) and IBM Statistical Package for the Social Sciences—SPSS Statistics version 27 (IBM Corp. Released 2019. IBM SPSS Statistics for Windows, Armonk, NY: IBM Corp).
Ethics declarations
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of Fondazione IRCCS Istituto Nazionale dei Tumori di Milano (approval number: INT106/13).
Consent to participate
Informed consent was obtained from all subjects involved in the study.
Results
The general characteristics of the study population by BRCA1 and BRCA2 are reported in Table 1. 63 women with BRCA 1/2 mutations (mean age, 47.6 ± 12.5 years), 39 with BRCA1 and 24 with BRCA2 mutation, were included in the present investigation. The distribution of general characteristics was homogeneous between BRCA1 and BRCA2 women. Taking the whole population, women presented on average a PSQI score of 7.0 ± 3.6 and a GSL-TPAQ score of 22.9 ± 18.3. As regards sleep quality and PA levels we did not found any significance difference due to the BRCA mutations.
Comparison between good and bad sleepers
Table 2 shows the baseline anthropometric, metabolic and PA data of the study population stratified by good (n = 26, 41, 3%) and bad sleepers (n = 37, 58, 7%) in the whole population and in BRCA1 and BRCA2 women. Referring to anthropometric and metabolic parameters, bad sleepers showed a slightly worse condition compared to good sleepers without any significant result. In the whole population, we observed that bad sleepers showed a significantly lower total GSL-TPAQ score. These results were consistent also in BRCA1 and BRCA2 mutation carriers. As regards the single question of different PA intensity (strenuous, moderate, mild), we found that bad sleepers showed significantly lower levels of strenuous, moderate and mild PA compared to good sleepers (p < 0.01; p < 0.01; p < 0.05, respectively). As regards the stratification by BRCA mutation type we observed consistent results. However, in BRCA1 women the results were significant only for moderate levels of PA while in BRCA2 we observed significant results for strenuous and mild PA.
Correlation analysis
Correlation analysis were performed to study the association between sleep quality, PA and anthropometric and metabolic parameters.
As regard sleep, we observed that a higher PSQI score, which corresponds to bad sleep quality, was significantly correlated with higher triglycerides levels (rs = 0.29, p < 0.05). About PA, higher GSL-TPAQ score, which indicates greater PA levels, was significantly correlated with lower values of weight (rs = − 0.27, p < 0.05), BMI (r s = − 0.32, p < 0.05), waist circumference (rs = − 0.27, p < 0.05), hip circumference (rs = − 0.31, p < 0.01), insulin (rs = − 0.35, p < 0.01), triglycerides levels (r s = − 0.28, p < 0.05), fat mass in % (rs = − 0.36, p < 0.01), fat mass in kg (rs = − 0.31, p < 0.05), and PSQI score (rs = − 0.41, p < 0.01). Taking into account the single question of PA intensity, strenuous intensity PA was significantly correlated with lower values of weight (rs = − 0.33, p < 0.01), BMI (rs = − 0.32, p < 0.01), waist circumference (rs = − 0.41, p < 0.01), hip circumference (rs = − 0.34, p < 0.01), waist/hip ratio (rs = − 0.32, p < 0.05), systolic (rs = − 0.31, p < 0.01), diastolic blood pressure (rs = − 0.43, p < 0.01), triglycerides (rs = − 0.25, p < 0.05), fat mass in % (rs = − 0.47, p < 0.01) and fat mass in kg (rs = − 0.36, p < 0.01). Even though not significant, strenuous intensity PA showed a tendency to be correlated with lower PSQI score (rs = − 0.23, p = 0.07). Moderate intensity PA was significantly correlated with lower PSQI score (rs = − 0.34, p < 0.01). Mild intensity PA was significantly correlated with lower waist circumference (rs = − 0.28, p < 0.05), but showed no significant correlation with PSQI score (rs = − 0.15, p = 0.23).
Binomial regression analysis
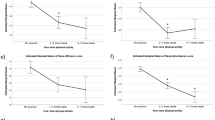
Table 3 shows the PR of being a good sleeper by considering the increasing tertiles of GSL-TPAQ total score. We observed that women in the higher tertile of GSL-TPAQ total score (≥ 27 METs/week) have a greater and significant PR of being a good sleeper compared to women in the lower tertile (≤ 11 METs/week). These results mean that women who practice strenuous PA for at least 3 times/week (or practice moderate PA 6 times/week) have about three times higher probability to have a better sleep quality. These results were consistent in both BRCA1 and BRCA2 even without any significant association.
We also estimated the PRs of being a good sleeper by unit of increase of MET/week (Table 4). In the whole population, as regards strenuous PA, every MET/week of increase was associated with a significant 10% increase of being a good sleeper. Similar results were obtained for moderate PA.
Discussion
This cross-sectional analysis suggests a direct association between PA and sleep quality in 63 women carriers of BRCA1/2 mutations. Women in the higher tertile of GSL-TPAQ total score (≥ 27 METs per week) have a greater and significant PR of being a good sleeper compared to women in the lower tertile (≤ 11 METs/week). The results were consistent also stratifying the population by BRCA mutation type. Furthermore, taking into account each single question of PA intensity, the PR of being a good sleeper by unit of increase of MET/week was higher and significant in women engaged in strenuous and moderate intensity PA. In contrast, mild intensity PA seemed not to significantly influence sleep behaviours.
To our knowledge, this is the first investigation assessing the potential influences of PA on sleep behaviour in this population. Previous studies in sporadic BC patients suggested the role of PA on the improvement of sleep behaviour (assessed both with actigraphy and questionnaires) and on the reduction of sleep deficiency at different stages of the BC pathology26,41,42,43.
Sleep quality in BC patients is essential for their quality of life. Indeed, BC diagnosis and treatments usually reflect on sleep as a long-term and side-effect symptom44. Quality of life usually decreases together with sleep after BC surgery and/or treatments, and their upgrading represents a challenging point for researchers45,46. The reasons explaining the bad sleep quality could be several: distress and anxiety of developing a very aggressive pathology or for the family's future; pain and hot flashes in consequent to surgery or treatments; fatigue that reduce the possibility to be sufficiently active46,47.
Sleep deficiency has been linked to increased inflammation and impaired immune response48. It also alters cellular signalling associated with mitochondrial respiratory function, insulin/IGF-I signalling32 and diminishes melatonin secretion, enhancing estrogen secretion49,50,51. Furthermore, sleep disorders decrease carbohydrate tolerance, alter leptin and cortisol levels52,53, thus modifying insulin sensitivity and favouring obesity and MS. For these mechanisms, sleep might represent one of the environmental factors involved in the modulation of BRCA penetrance. In this cross sectional analysis we decided not to report results by disease status because affected women showed a slightly worse sleep quality compared to unaffected, but without any significance result. Furthermore, the nature of the analysis and the small numbers of our study would not allow to draw conclusions about a potential effect of sleep on BRCA penetrance.
This cross-sectional analysis suggests that PA may be a tool for improving sleep quality in BRCA1/2 women. Increasing PA levels and modifying daily habits in favour of a more active lifestyle has been among the leading research goals in the BC field also in order to improve sleep. The mechanisms on this linkage are not yet fully understood; however, studies from healthy subjects indicated that PA could exert its beneficial action on sleep through body temperature regularization, energy conservation, decrement in anxiety, stress, endocrine function, obesity and immune-inflammation response54,55,56,57,58. A regular and constant PA practice is recognized to improve body weight, BMI and other anthropometric parameters, insulin and IGF-I levels, adipokines balance, and sexual hormones secretion59. In our study, either total PA or strenuous intensity PA levels were correlated with lower weight, BMI, waist circumference, hip circumference, fat mass and insulin levels, suggesting a positive association also in BRCA1/2 women.
The results of the present analysis should be seen in view of their limitations and strengths. Limitations may be attributable to the small sample size and to the use of questionnaires instead of objective assessment instruments for the all population (such as actigraphy). We are aware that is recommended to collect both, subjective and objective evaluations of sleep behavior and PA levels, but this was not foreseen by the MedDiet trial which had different aims10.
A further intrinsic limitation of this study is the cross-sectional design that does not allow to distinguish the cause from the effect. However, the intention of this paper was mainly to explore the sleep and PA data of the BRCA women who joined our MedDiet trial rather than to give an interpretation to the associations we found.
Despite the limitations, the preliminary results of the present analysis suggest new aspects to study in order to improve the quality of life in BRCA mutation carriers. The MedDiet results10 demonstrated that a dietary intervention in women carriers is feasible and effective in reducing metabolic and anthropometric parameters. Additional recommendations about PA for a more active lifestyle might be probably useful for the clinical management of this special group of women. These results represent therefore the seed for continuing the recruitment to broaden the sample and to evaluate the association between PA and sleep in a larger population of BRCA mutation carriers.
Conclusions
The present study suggests an association between PA and sleep in women carriers of BRCA1/2 mutations, highlighting that higher PA levels are associated with a better quality of sleep behaviour. In this perspective, future studies involving PA interventions are needed to improve sleep and quality of life in women predisposed to hereditary BC.
Change history
28 November 2022
A Correction to this paper has been published: https://doi.org/10.1038/s41598-022-25014-7
References
Antoniou, A. et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family history: A combined analysis of 22 studies. Am. J. Hum. Genet. 72, 1117–1130 (2003).
Kuchenbaecker, K. B. et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA 317, 2402 (2017).
Lalloo, F. & Evans, D. G. Familial breast cancer. Clin. Genet. 82, 105–114 (2012).
Kotsopoulos, J. et al. Changes in body weight and the risk of breast cancer in BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. 7, R833 (2005).
Bissonauth, V. et al. Weight history, smoking, physical activity and breast cancer risk among French-Canadian women non-carriers of more frequent BRCA1/2 mutations. J. Cancer Epidemiol. 2009, 1–11 (2009).
Lubinski, J. et al. The risk of breast cancer in women with a BRCA1 mutation from North America and Poland. Int. J. Cancer 131, 229–234 (2012).
Manders, P. et al. Body weight and risk of breast cancer in BRCA1/2 mutation carriers. Breast Cancer Res. Treat. 126, 193–202 (2011).
Qian, F. et al. Height and body mass index as modifiers of breast cancer risk in BRCA1/2 mutation carriers: A Mendelian Randomization Study. J. Natl. Cancer Inst. 111, 350–364 (2019).
Kim, S. J. et al. Weight gain and the risk of ovarian cancer in BRCA1 and BRCA2 mutation carriers. Cancer Epidemiol. Biomark. Prev. 30, 2038–2043 (2021).
Bruno, E. et al. A mediterranean dietary intervention in female carriers of BRCA mutations: Results from an Italian prospective randomized controlled trial. Cancers (Basel) 12, 3732 (2020).
Wang, P. et al. Night-shift work, sleep duration, daytime napping, and breast cancer risk. Sleep Med. 16, 462–468 (2015).
Samuelsson, L. B., Bovbjerg, D. H., Roecklein, K. A. & Hall, M. H. Sleep and circadian disruption and incident breast cancer risk: An evidence-based and theoretical review. Neurosci. Biobehav. Rev. 84, 35–48 (2018).
Lu, C. et al. Long-term sleep duration as a risk factor for breast cancer: Evidence from a systematic review and dose-response meta-analysis. Biomed Res. Int. 2017, 1–11 (2017).
Wang, F. et al. Meta-analysis on night shift work and risk of metabolic syndrome. Obes. Rev. 15, 709–720 (2014).
Cadenas, C. et al. Loss of circadian clock gene expression is associated with tumor progression in breast cancer. Cell Cycle 13, 3282–3291 (2014).
Blask, D. E. Melatonin, sleep disturbance and cancer risk. Sleep Med. Rev. 13, 257–264 (2009).
Pevet, P. & Challet, E. Melatonin: Both master clock output and internal time-giver in the circadian clocks network. J. Physiol. 105, 170–182 (2011).
Leproult, R., Holmbäck, U. & Van Cauter, E. Circadian misalignment augments markers of insulin resistance and inflammation, independently of sleep loss. Diabetes 63, 1860–1869 (2014).
Morris, C. J., Aeschbach, D. & Scheer, F. A. J. L. Circadian system, sleep and endocrinology. Mol. Cell. Endocrinol. 349, 91–104 (2012).
Harmsen, M. G., Hermens, R. P. M. G., Prins, J. B., Hoogerbrugge, N. & de Hullu, J. A. How medical choices influence quality of life of women carrying a BRCA mutation. Crit. Rev. Oncol. Hematol. 96, 555–568 (2015).
Campfield Bonadies, D., Moyer, A. & Matloff, E. T. What I wish I’d known before surgery: BRCA carriers’ perspectives after bilateral salipingo-oophorectomy. Fam. Cancer 10, 79–85 (2011).
Lammert, J. et al. Physical activity during adolescence and young adulthood and the risk of breast cancer in BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. Treat. 169, 561–571 (2018).
Pijpe, A. et al. Physical activity and the risk of breast cancer in BRCA1/2 mutation carriers. Breast Cancer Res. Treat. 120, 235–244 (2010).
Kiechle, M. et al. Feasibility of structured endurance training and Mediterranean diet in BRCA1 and BRCA2 mutation carriers—An interventional randomized controlled multicenter trial (LIBRE-1). BMC Cancer 17, 752 (2017).
Mustian, K. M. et al. Multicenter, randomized controlled trial of yoga for sleep quality among cancer survivors. J. Clin. Oncol. 31, 3233–3241 (2013).
Roveda, E. et al. Protective effect of aerobic physical activity on sleep behavior in breast cancer survivors. Integr. Cancer Ther. 16, 21–31 (2017).
Castelli, L. et al. Sleep problems and their interaction with physical activity and fatigue in hematological cancer patients during onset of high dose chemotherapy. Support. Care Cancer 30, 167–176 (2022).
Bruno, E. et al. Effect of aerobic exercise intervention on markers of insulin resistance in breast cancer women. Eur. J. Cancer Care 27, e12617 (2018).
Kredlow, M. A., Capozzoli, M. C., Hearon, B. A., Calkins, A. W. & Otto, M. W. The effects of physical activity on sleep: A meta-analytic review. J. Behav. Med. 38, 427–449 (2015).
Pattyn, N., Cornelissen, V. A., Eshghi, S. R. T. & Vanhees, L. The effect of exercise on the cardiovascular risk factors constituting the metabolic syndrome. Sport. Med. 43, 121–133 (2013).
Escames, G. et al. Exercise and melatonin in humans: Reciprocal benefits. J. Pineal Res. 52, 1–11 (2012).
Saner, N. J., Bishop, D. J. & Bartlett, J. D. Is exercise a viable therapeutic intervention to mitigate mitochondrial dysfunction and insulin resistance induced by sleep loss? Sleep Med. Rev. 37, 60–68 (2018).
Pasanisi, P., Bruno, E., Manoukian, S. & Berrino, F. A randomized controlled trial of diet and physical activity in BRCA mutation carriers. Fam. Cancer 13, 181–187 (2014).
Bruno, E. et al. Adherence to mediterranean diet and metabolic syndrome in BRCA mutation carriers. Integr. Cancer Ther. 17, 153–160 (2018).
Pasanisi, P. et al. A dietary intervention to lower serum levels of IGF-I in BRCA mutation carriers. Cancers (Basel) 10, 309 (2018).
Daniele, A. et al. The role of circulating adiponectin and SNP276G>T at ADIPOQ gene in BRCA-mutant women. Cancer Genomics Proteomics 17, 301–307 (2020).
Bruno, E. et al. Lifestyle characteristics in women carriers of BRCA mutations: Results from an Italian trial cohort. Clin. Breast Cancer. https://doi.org/10.1016/j.clbc.2020.11.002 (2020).
Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R. & Kupfer, D. J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 28, 193–213 (1989).
Godin, G. & Shephard, R. J. A simple method to assess exercise behavior in the community. Can. J. Appl. Sport Sci. 10, 141–146 (1985).
Curcio, G. et al. Validity of the Italian version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 34, 511–519 (2013).
Rogers, L. Q. et al. Physical activity and sleep quality in breast cancer survivors: A randomized trial. Med. Sci. Sport. Exerc. 49, 2009–2015 (2017).
Kreutz, C., Schmidt, M. E. & Steindorf, K. Effects of physical and mind–body exercise on sleep problems during and after breast cancer treatment: A systematic review and meta-analysis. Breast Cancer Res. Treat. 176, 1–15 (2019).
Yang, H., Yang, Z., Pan, H. & Zhou, Q. Effects of physical activity on sleep problems in breast cancer survivors: A meta-analysis. Support. Care Cancer 29, 4023–4032 (2021).
Fiorentino, L., Rissling, M., Liu, L. & Ancoli-Israel, S. The symptom cluster of sleep, fatigue and depressive symptoms in breast cancer patients: Severity of the problem and treatment options. Drug Discov. Today Dis. Model. 8, 167–173 (2011).
Mokhatri-Hesari, P. & Montazeri, A. Health-related quality of life in breast cancer patients: Review of reviews from 2008 to 2018. Health Qual. Life Outcomes 18, 338 (2020).
Kingsberg, S. A., Larkin, L. C. & Liu, J. H. Clinical effects of early or surgical menopause. Obstet. Gynecol. 135, 853–868 (2020).
Shochat, T. & Dagan, E. Sleep disturbances in asymptomatic BRCA1/2 mutation carriers: Women at high risk for breast-ovarian cancer. J. Sleep Res. 19, 333–340 (2010).
Irwin, M. R. Why sleep is important for health: A psychoneuroimmunology perspective. Annu. Rev. Psychol. 66, 143–172 (2015).
Schernhammer, E. S. et al. Urinary 6-sulfatoxymelatonin levels and risk of breast cancer in postmenopausal women. J. Natl. Cancer Inst. 100, 898–905 (2008).
Schernhammer, E. S. & Hankinson, S. E. Urinary melatonin levels and postmenopausal breast cancer risk in the Nurses’ Health Study Cohort. Cancer Epidemiol. Biomark. Prev. 18, 74–79 (2009).
Schernhammer, E. S. et al. Urinary 6-sulphatoxymelatonin levels and risk of breast cancer in premenopausal women: The ORDET cohort. Cancer Epidemiol. Biomark. Prev. 19, 729–737 (2010).
Spiegel, K., Leproult, R. & Van Cauter, E. Impact of sleep debt on metabolic and endocrine function. Lancet 354, 1435–1439 (1999).
Spiegel, K. et al. Leptin levels are dependent on sleep duration: Relationships with sympathovagal balance, carbohydrate regulation, cortisol, and thyrotropin. J. Clin. Endocrinol. Metab. 89, 5762–5771 (2004).
Driver, H. S. & Taylor, S. R. Exercise and sleep. Sleep Med. Rev. 4, 387–402 (2000).
Uchida, S. et al. Exercise effects on sleep physiology. Front. Neurol. 3, 1–5 (2012).
Chennaoui, M., Léger, D. & Gomez-Merino, D. Sleep and the GH/IGF-1 axis: Consequences and countermeasures of sleep loss/disorders. Sleep Med. Rev. 49, 101223 (2020).
Farnsworth, J. L., Kim, Y. & Kang, M. Sleep disorders, physical activity, and sedentary behavior among US adults: National Health and Nutrition Examination Survey. J. Phys. Act. Health 12, 1567–1575 (2015).
Zielinski, M. R. et al. Chronic sleep restriction elevates brain interleukin-1 beta and tumor necrosis factor-alpha and attenuates brain-derived neurotrophic factor expression. Neurosci. Lett. 580, 27–31 (2014).
Ortega, M. A. et al. Physical activity as an imperative support in breast cancer management. Cancers (Basel) 13, 55 (2020).
Acknowledgements
The authors thank Maria Grazia Guerrini for the editorial support. The authors would like to acknowledge with much appreciation all the volunteers who participated in the study. The authors acknowledge the support the APC central found of the University of Milan.
Funding
This research was funded by the Italian Cancer Research Association (AIRC) Grant No. IG-2015-17151 and by the Italian Ministry of Health Grant No. GR-2010-2310116.
Author information
Authors and Affiliations
Contributions
Conceptualization: P.P., E.B., and E.R.; methodology: P.P., E.B., E.R., L.G., and L.C.; formal analysis: E.B., L.G., and L.C.; investigation: P.P., E.B., A.O., and I.B.; resources: P.P.; data curation: E.B., L.G., L.C., A.O., and I.B.; writing—original draft preparation: L.G., and L.C.; writing—review and editing: P.P., E.B., F.E., A.Mo., AMu., A.O., I.B., and E.R.; supervision: P.P., E.B., and E.R.; project administration: P.P. and E.B.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained a spelling error in the name of the author Patrizia Pasanisi, which was incorrectly given as Pasanisi Patrizia.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Galasso, L., Castelli, L., Roveda, E. et al. Physical activity and sleep behaviour in women carrying BRCA1/2 mutations. Sci Rep 12, 12873 (2022). https://doi.org/10.1038/s41598-022-16687-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-16687-1
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
