
Abstract
Previous studies reported on the association between physical activity (PA) and cardiovascular diseases (CVDS) among the Western population. However, evidence on the association between different patterns of PA and the risk of CVDS among Chinese population are limited. This study aims to evaluate the association of different PA types and the risk of CVDS in a Chinese adult population. A total of 3568 community residents were recruited from Jiangsu Province of China using a stratified multistage cluster sampling method. The latent class analysis method was employed to identify the types of PA, and the Framingham risk score (FRS) was used to estimate the risk of CVDS within 10 years. Three types of PA were identified: CLASS1 represented participants with high occupational PA and low sedentary PA (32.1% of male, 26.5% of female), ClASS2 represented those engaging in low occupational PA and high leisure-time PA (27.0% of male, 14.2% of female), and CLASS3 represented low leisure-time and high sedentary PA (40.9% of male, 59.3% of female). The average of FRS in males was higher than that in females across PA types. CLASS1 (OR = 0.694, 95%CI 0.553–0.869) and CLASS2 (OR = 0.748, 95%CI 0.573–0.976) were both found to be protective against CVDS in males; however, such associations were not statistically significant among females. Therefore, higher occupational or leisure-time PA appear to be associated with decreased risk of CVDS, while more sedentary behaviors may increase the risk of CVDS, particularly for male Chinese adults.
Similar content being viewed by others


Introduction
Increasing in the number of the aging population and the acceleration of urbanization have significantly increased the prevalence of cardiovascular diseases (CVDS), including coronary heart disease, cerebrovascular disease, rheumatic heart disease, and other conditions1. According to the National Report on Cardiovascular Diseases (2018) in China2, the number of patients with CVDSin China have reached 290 million. The main causes of CVDS are unhealthy lifestyle behavior and reduced physical activity3. Previous studies revealed that regular physical activity (PA) was critical in preventing chronic diseases, including CVDS4,5. Bennett et al. proposed that PA can be categorized as occupational, commuting, household, and recreational6. The Global Burden of Diseases Report estimated that low levels of PA accounted for 1.26 million premature deaths and 2.37 million disability-adjusted life-years worldwide in 20177. Meanwhile, high levels of either occupational or leisure-time PA have been found to be associated with a lower risk of CVDS in high-income countries8. However, the association between different types of PA and the risk of CVDS among different subgroups of the population in China, so far, have been rarely reported6,9.
Latent class analysis (LCA) uses the latent class model (LCM) to explain the relationship between explicit class variables with intrinsic latent class variables10. LCA can identify subgroups of people who share common characteristics so that people within the subgroups have a similar scoring pattern on the measured variable, while the difference in scoring patterns between subgroups is as distinctly different as possible11. LCA analysis uses a mixture of distributions to identify the most likely model describing the heterogeneity of data as a finite number of classes (subgroups), also known as finite mixture models12. LCA was used for modelling the “lifestyle” variable in Miranda’s study to assess the lifestyle of female adolescents based on measurements of behavioral variables13. Moreover, in two community samples in Breslau, LCA aimed to empirically examine the structure underlying post-traumatic stress disorder (PTSD) criteria symptoms and identify discrete classes with similar symptom profiles14. Similar attempts have also been made in a cohort study, which used data during 2003–2008 from the National Violent Death Reporting System, and included 28,703 suicide decedents from 12 US states15. In the present study, we used LCA to estimate the latent PA types of adult residents in Jiangsu province of China and explored the associations of different latent PA types with CVDS risk.
Materials and methods
Participants
A multistage stratified cluster sampling method was employed to select participants. Within the seven counties (in rural areas) or districts (in urban areas) of the Chinese National Disease Surveillance System for Chronic Diseases and Risk Factors in northern and middle areas of Jiangsu Province of China16, five towns /streets were randomly selected from each county/district. Then, two villages/communities were randomly selected from each town/street, followed by sixty households being randomly selected from each village/community. Finally, using the KISH table method, one adult resident aged 18 years or above was selected from each household17.
4200 individuals were recruited for participation. We excluded 574 participants whose age did not meet the Framingham Scoring criteria (i.e., 30–74 years old)18, 52 participants who had pre-existing CVDS, cancer or other severe comorbidities, and 6 participants who did not have complete laboratory data. Finally, a number of 3568 participants were included in this study.
Questionnaire survey
A standard questionnaire which designed based on the Questionnaire for the Chinese Chronic Non-communicable Disease and Risk Factor Surveillance (2010)16 was used to collect information on demographic information (i.e., residence, gender, age, educational level, marital status), behavioral factors (i.e., tobacco smoking, alcohol drinking, physical activity and daily sedentary behaviors), and health condition (i.e., hypertension, diabetes, and dyslipidemia). All surveys were conducted face-to-face by interviewers, who had received proper training and passed relevant assessment. The Global Physical Activity Questionnaire (GPAQ)19 was used to assess the frequency and duration of several components of PA in different components, including: (1) occupational, agriculture, and housework activity; (2) commuting related physical activity; (3) leisure-time physical activity; (4) sedentary behaviors. Levels of agreement with objective measurements indicated that the GPAQ was a valid measure of moderate-to-vigorous physical activities20.
Anthropometric measurements
Height, body weight, waist circumference, and blood pressure were measured by anthropometric investigators using unified brands and models instruments. All investigators successfully completed a training program that introduced them with the specific tools and methods used in this study, as well as with the aims of this study. Briefly speaking, height was measured by a height meter with a maximum range of 2.0 m and a minimum scale of 0.1 cm. The body weight was measured by an electronic scale with a maximum range of 150 kg and an accuracy of 0.1 kg. The waist circumference was measured by a leather tape, which was measured at the midpoint between the lowest rib margin and the lower 12th costal margin. Blood pressure was measured 3 times using an automated device (OMRON HEM-7207)21 at the left-arm according to the standard measuring protocol. All sphygmomanometers were calibrated by the manufacturer and checked by the national quality assurance team department. The mean value of the three measurements was used as the final blood pressure values. Details of the anthropometric measurements had been documented elsewhere22.
Blood sample collection and laboratory tests
A volume of 4—5 ml venous blood sample was collected in a vacuum tube containing sodium fluoride in the morning, after overnight fasting of at least 10 h. Fasting plasma glucose (FPG) was measured by glucose oxidase or hexokinase methods within 12 h after collecting in an accredited laboratory. Serum total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglycerides (TG) were measured using auto-analyzers (Abbott Laboratories) in Jiangsu Province Center for Disease Control and Prevention, which was certificated by The National Laboratory Certification of China.
Measurement of the risk of CVDS
In this study, we used the Framingham Risk Score (FRS) to estimate a person’s chance of developing a CVDS event in the next ten years. The FRS, expressed as a percentage, was calculated based on the prediction equation known as the “Framingham Risk Equation” , which consisted of age, TC, HDL-C, SBP, treatment for hypertension, smoking status, and diabetic status18. The risk of CVDS was categorized as: “low” if the FRS ≤ 10%; “intermediate” if the FRS was between 11 and 20%; “high” if the FRS > 20%23.
Classification of physical activity
In this study, the PA of participants was classified using the LCA, an analysis method established on the basis of probability distribution and a log-linear model. It can make up for the traditional statistical methods that only focus on a single variable and play a role of considering the comprehensive effect of multiple factors. The model of LCA was judged using the following test standards24: (1) Akaike information criterion (AIC), Bayesian information criterion (BIC), and adjusted Bayesian information criterion (aBIC). The smaller the three indexes, the better the model fitting effect could be; (2) Entropy, the larger the value, the higher the accuracy of the classification could be; (3) In combination with the adjusted Lo-Mendell-Rubin likelihood ratio test (LMR) and the bootstrap-based likelihood ratio test (BLRT), the model of K categories was significantly better than the model of K-1 categories, while it indicates P < 0.05 of these indicators. The best classification was determined by considering all above indicators and relevant professional knowledge was used for the interpretation of results.
Definitions of other involved variables
Body mass index (kg/m2) was calculated as weight divided by height squared. Participants were categorized as: underweight (BMI < 18.5 kg/m2), normal (18.50 ≤ BMI < 24.00 kg/m2), overweight (24.00 ≤ BMI < 28.00 kg/m2), and obese (BMI ≥ 28.00 kg/m2) according to the standard made by the working group on obesity in China for Chinese population25. Central obesity was defined as: males with a waist circumference ≥ 90 cm or females with a waist circumference ≥ 85cm26.
Hypertension was defined as having a self-report history of hypertension, receiving BP-lowering treatment, or having an average measured systolic BP of at least 140 mmHg or a diastolic BP of at least 90 mmHg (or both) during the study period27.
Diabetes mellitus was defined as FPG ≥ 7.0 mmol/L, or 2-h OGTT ≥ 11.11 mmol/L, or having a self-report history of diabetes, or taking hypoglycemic drugs during the study period28. Dyslipidemia was defined as TC ≥ 6.22 mmol/L, and/or TG ≥ 2.26 mmol/L, and/or LDL-C ≥ 4.14 mmol/L, and/or HDL-C ≤ 1.04 mmol/L29.
Current smoking was defined as having smoked at least 100 cigarettes, or equivalent other tobacco products in one’s lifetime, and currently smoking cigarettes. Drinking alcohol more than once per month over the past 12 months prior to the interview was defined as current drinking16.
Statistical analysis
General descriptive analysis and χ2 test were used to compare the potential differences of categorical variable among groups. The effects of different PA types on the risk of CVDS were analyzed by ordinal logistic regression. Given that age, blood pressure, smoking status, and other factors have been included in the calculation of the FRS, these variables were not adjusted in the ordinal logistic regression analysis. A two-side P-value < 0.05 was considered statistically significant. All these analyses were performed using SPSS statistical software (v23.0), while the MPLUS statistical software (v8.0) was used to analyze the potential categories of PA (Latent Classes).
Ethics approval and consent to participate
Informed written consent was obtained from all participants. The procedures were in accordance with the standards of the ethics committee of Jiangsu Provincial Center for Disease Control and Prevention and with the Declaration of Helsinki (1975, revised 2013). This study protocol was approved by the ethical review committee at the Jiangsu Province Center for Disease Control and Prevention (the committee’s reference number: SL2017-B002-01). Individual person’s data have not been contained in any form (including any individual details, images, or videos) in this manuscript.
Results
Characteristics of participants
Of the 3568 participants (men, 43.0%), the average age was 52.04 years (SD = 11.08). Compared with females, males had a higher percentage of higher education or having a job. Males were more likely to be smokers, to consume alcohol, or to have hypertension, whilst females were more likely to have central obesity or dyslipidemia (Table 1).
Identification of PA types using LCA method
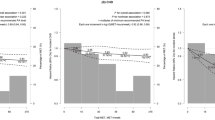
In the LCA of PA, 10 variables were included in the GPAQ, including high occupational PA, medium–low occupational PA, commuting PA, high leisure-time PA, medium–low leisure time PA, sedentary PA, TV PA, computer PA, reading PA, and sleeping PA. Five latent class models were fitted for both men and women (Table 2). As was shown in Table 2, with the increase in model categories, Log-like hood (Log (L)), AIC, BIC, and aBIC decreased. In males, BIC value of 3 category model reached the minimum and P-value for the LMR was 0.004, however fitting four category model, P-value for the LMR was 0.680. Therefore the three category model had the best fitting degree. Similarly,in females the three category model had the best fitting degree. According to the results of the conditional probability distribution of each item in three categories of each gender (Fig. 1), the performance of Latent CLASS1 was high occupational PA, low sedentary PA; the performance of Latent CLASS2 was low occupational and high leisure-time PA; the performance of Latent CLASS3 was low leisure-time PA, high sedentary PA. There were 492 (32.1%), 414 (27.0%) and 628 (40.9%) male participants in these three classifications, respectively, while there were 539 (26.5%), 288 (14.2%) and 1207 (59.3%) female participants, respectively.

(a) Conditional probability distribution for three-category of physical activity for males; (b) Conditional probability distribution for three-category of physical activity for females.
Comparison of the characteristics in different Latent Classes of PA
The baseline characteristics of participants were given by classifications in Tables 3 and 4. There were significant differences in age, education status, marital status, BMI, work status, sleep duration, smoking status, low HDL-C, high TG, hypertension, hyperglycemia and central obesity among the three Latent classes of male PA (P < 0.05).There were significant differences in age, education status, marital status, BMI, work status, sleep duration, alcohol consumption, high TG, low HDL-C, Hypertension, and Central obesity among the three Latent classes of female PA (P < 0.01).
Relationships between PA types and the risk of CVDS
Comparison analysis among the three PA types in males revealed significant differences in their 10-year FRS. As shown in Table 5, the FRSs of males were higher than that of females. Among males, the FRS for CLASS1 and CLASS2 were lower than that of CLASS3, which had the largest number of participants. CLASS1 (OR = 0.654,95%CI 0.526–0.813) and CLASS2 (OR = 0.544, 95%CI 0.432–0.685) were found to be protective against the risk of CVDS compared to CLASS3. After adjusting for potential confounding factors, the relationship between CLASS 1(OR = 0.694, 95%CI 0.553–0.869) and CLASS 2(OR = 0.748, 95%CI 0.573–0.976) and the risk CVDS was slightly attenuated but remained statistically significant. Among females, CLASS2 was inversely correlated with CVDS (OR = 0.451, 95%CI 0.316–0.643), but such association disappeared after adjusted for potential confounders.
Discussion
The China Kadoorie Biobank (CKB) study30 reported that total levels of PA was strongly, and inversely, associated with CVDS-related mortality in Chinese population31. Like in many other developed countries, the standard of living in China greatly improved, leading to drastic lifestyle changes, for example, transferring from a labor-intensive lifestyle to a sedentary lifestyle3. A prospective cohort study of 487,334 subjects conducted by Bennett et al6 in 10 regions of China showed that higher occupational or non-occupational PA was significantly associated with a lower risk of major CVDS events among Chinese adults. In this study, we classified PA in three groups (Latent Classes), i.e., CLASS1 (high occupational and low sedentary PA), CLASS2 (low occupational and high leisure-time PA), and CLASS3 (low leisure-time and high sedentary PA). Several previous LCA studies provided limited and inconsistent findings in different fields, such as sociology, biology, medicine, and psychology32. To the best of our knowledge, this is among the first studies to explore the associations between CVDS and PA types using LCA among Chinese adults with representative data.
This study found that CLASS3 accounted for a big proportion in the three categories of PA (40.9% of males and 59.3% of females). CLASS3 was manifested as high sedentary and low leisure-time activity behavior. A previous survey of nine provinces in China from 1991 to 201133 found that for both adult men and women in China, occupational and domestic PA were the largest contributors to the total PA; meanwhile, this study also revealed that the overall PA of community residents significantly declined in the two decades, and active leisure and travel PA were fairly low. Some studies have shown that the occupational PA, rather than the leisure PA, is the main source for total daily PA34,35. Inadequate total daily PA has become one of the major risk factors for China's CVDS death and disease burden36. Similarly, physical inactivity and obesity are the biggest public health threats, with 53.5% of adults being physically inactive in Canada37. Sedentary PA is also a threat to Americans' physical health, which is why the 2018 Physical Activity Guidelines for Americans, 2nd edition highlights the shift from sitting time to being more active, ideally by doing moderate- or vigorous-intensity physical activity38.
This study explored the relationship of 10-year risk of CVDS predicted by the Framingham risk scoring system with three types of PA . The current data demonstrated that the 10-year risk of CVDS incidence was higher in males compared to females in across the three categories. Previous studies indicated that males had a higher risk to have CVDS events, which may be related to differences in exposure levels, sensitivities of risk factors for CVDS between genders, and sex hormone differences39,40. In this study, CLASS3 was associated with higher CVDS risk in both genders compared to CLASS1 and CLASS2. The CLASS1(OR = 0.694, 95%CI 0.553–0.869)and CLASS2(OR = 0.748, 95%CI 0.573–0.976) were found to be related to lower risk of CVDS with 10-year. These results were consistent with previous studies8,41. As a result, the 2018 PA guidelines for Americans38 emphasize that increasing PA and reducing sedentary time are appropriate for all populations and that even a little increase in PA can bring health benefits. In addition, the American college of sports medicine (ACSM)42 suggest that regular PA (for example, exercise, cycling) may reduce insulin levels and renal sympathetic nerve tension by sodium retention and foundation, vasodilator substances by skeletal muscle release cycle, and improve blood pressure, blood lipid, blood glucose and other risk factors of CVDS43.
The LCA method takes into account the comprehensive effect of multiple factors. It can reveal the characteristics of various groups of people and provide a scientific basis for the designation of targeted intervention and prevention measures. However, several limitations of the study should be considered. First of all, the LCA takes the qualitative data into consideration instead of the comprehensive analysis of its frequency and duration. Second, in this study, a questionnaire survey was used to collect physical activity information, rather than using objective measurements (e.g., pedometers to calculate the exact daily steps), which may lead to recall bias. Nevertheless, the use of a tool with proven validity and reliability, i.e., the GPAQ, together with adequate staff training, can minimize such bias. Third, the FRS was used to estimate the 10-year CVDS risk in this study, which may has neglected important information on the possible effects of ethnicity on the findings. As this was a cross-sectional study, the causal relationship between PA and the risk of CVDS could be hardly established. Consequently, further longitudinal research with robust design is warranted to test this relationship.
To summarize, results from this study revealed potential associations between CVDS and PA types among Chinese adults. Lower occupational and leisure-time PA and higher sedentary PA were associated with increased risk of CVDS. Accordingly, we suggest relevant sectors in China to strengthen evidence-based interventions in order to increase the levels of PA of people and reduce the time of sedentary behaviors. Findings from this study can be used to advance public health, particularly in the management of public policies that promote PA and bring more health benefits.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon request.
Abbreviations
- CVDS :
-
Cardiovascular diseases
- PA:
-
Physical activity
- LCA:
-
Latent class analysis
- FRS:
-
Framingham risk score
- LCM:
-
Latent class model
- PTSD:
-
Posttraumatic stress disorder
- GPAQ:
-
Global physical activity questionnaire
- FPG:
-
Fasting plasma glucose
- TC:
-
Serum Total cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- HDL-C:
-
High-density lipoprotein cholesterol
- TG:
-
Triglycerides
- AIC:
-
Akaike information criterion
- BIC:
-
Bayesian information criterion
- aBIC:
-
Adjusted Bayesian information criterion
- LMR:
-
Lo-Mendell-Rubin likelihood ratio test
- BLRT:
-
Bootstrap-based likelihood ratio test
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- Log (L):
-
Log-like hood
- CKB:
-
China Kadoorie Biobank
References
World Health Organization (WHO). Cardiovascular diseases. https://www.cdc.gov/physicalactivity/basics/pa-health/index.htm#ReducedCancer.
Hu, S. S. et al. Summary of the 2018 Report on Cardiovascular Diseases in China. Chin. Circ. J. 34, 209–220 (2019).
Cheng, X. et al. Physical activity levels, sport activities, and risk of acute myocardial infarction: Results of the INTERHEART study in China. Angiology 65, 113–121. https://doi.org/10.1177/0003319712470559 (2014).
Shortreed, S. M., Peeters, A. & Forbes, A. B. Estimating the effect of long-term physical activity on cardiovascular disease and mortality: evidence from the Framingham Heart Study. Heart (Br. Card. Soc.). 99, 649–654. https://doi.org/10.1136/heartjnl-2012-303461 (2013).
Centers for Disease Control and Prevention. Physical activity and health. https://www.cdc.gov/physicalactivity/basics/pa-health/index.htm#ReducedCancer.
Bennett, D. A. et al. Association of physical activity with risk of major cardiovascular diseases in chinese men and women. JAMA Cardiol. 2, 1349–1358. https://doi.org/10.1001/jamacardio.2017.4069 (2017).
GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet (London, England). 392, 1923–1994. https://doi.org/10.1016/S0140-6736(18)32225-6 (2018).
Li, J. & Siegrist, J. Physical activity and risk of cardiovascular disease—A meta-analysis of prospective cohort studies. Int. J. Environ. Res. Public Health. 9, 391–407. https://doi.org/10.3390/ijerph9020391 (2012).
Du, H. et al. Physical activity and sedentary leisure time and their associations with BMI, waist circumference, and percentage body fat in 0.5 million adults: The China Kadoorie Biobank study. Am J Clin Nutr. 97, 487–496. https://doi.org/10.3945/ajcn.112.046854 (2013).
Zeng, X. H., Xiao, L. & Zhang, Y. B. Principle and case analysis of latent class analysis. Chin. J. Health Stat. 30, 815–817 (2013).
Kongsted, A. & Nielsen, A. M. Latent Class Analysis in health research. J. Physiother. 63, 55–58. https://doi.org/10.1016/j.jphys.2016.05.018 (2017).
Vermunt, J. K. & Magidson, J., eds. Applied Latent Class Analysis. Cambridge, Cambridge University Press; Latent Class Cluster Analysis. In: Hagenaars JA, McCutcheon AL.89–106 (2002).
Miranda, V. et al. Evaluation of lifestyle of female adolescents through latent class analysis approach. BMC Public Health 19, 184. https://doi.org/10.1186/s12889-019-6488-8 (2019).
Breslau, N., Reboussin, B. A., Anthony, J. C. & Storr, C. L. The structure of posttraumatic stress disorder: Latent class analysis in 2 community samples. Arch Gen Psychiatry. 62, 1343–1351. https://doi.org/10.1001/archpsyc.62.12.1343 (2005).
Logan, J., Hall, J. & Karch, D. Suicide categories by patterns of known risk factors: A latent class analysis. Arch Gen Psychiatry. 68, 935–941. https://doi.org/10.1001/archgenpsychiatry.2011.85 (2011).
Xu, Y. et al. Prevalence and control of diabetes in Chinese adults. JAMA 310, 948–959. https://doi.org/10.1001/jama.2013.168118 (2013).
Kish, L. A procedure for objective respondent selection within the household. J. Am. Stat. Assoc. 44, 380–387. https://doi.org/10.1080/01621459.1949.10483314 (1949).
D’Agostino, R. B. et al. General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation 117, 743–753. https://doi.org/10.1161/CIRCULATIONAHA.107.699579 (2008).
Armstrong, T. & Bull, F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J. Public Health. 14, 66–70. https://doi.org/10.1007/s10389-006-0024-x (2006).
Cleland, C. L. et al. Validity of the global physical activity questionnaire (GPAQ) in assessing levels and change in moderate-vigorous physical activity and sedentary behaviour. BMC Public Health 14, 1255. https://doi.org/10.1186/1471-2458-14-1255 (2014).
Bloomfield, G. S. et al. Multiple cardiovascular risk factors in Kenya: evidence from a health and demographic surveillance system using the WHO STEPwise approach to chronic disease risk factor surveillance. Heart (Br. Card. Soc.) 99, 1323–1329. https://doi.org/10.1136/heartjnl-2013-303913 (2013).
Lyu, S., Su, J., Xiang, Q. & Wu, M. Association of dietary pattern and physical activity level with triglyceride to high-density lipoprotein cholesterol ratio among adults in Jiangsu, China: A cross-sectional study with sex-specific differences. Nutr. Res. 34, 674–681. https://doi.org/10.1016/j.nutres.2014.07.007 (2014).
Ridker, P. M., Buring, J. E., Rifai, N. & Cook, N. R. Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: The Reynolds Risk Score. JAMA 297, 611–619. https://doi.org/10.1001/jama.297.6.611 (2007).
Li, D. D. et al. Application of latent class model in the classification of the patients with diabetes vulnerability. Chin. J. Health Stat. 35, 11–13 (2018).
Chen, W. & Jiang, H. Interpretation of the consensus of Chinese experts on nutritional medical treatment for overweight/obesity in 2016. Chin. J. Pract. Intern. Med. 24, 24–56 (2017).
Tian, Y. et al. A prospective study of the risk of central obesity and ischemic heart disease in Chinese adults. Chin. J. Hypertens. 27, 300 (2019).
Writing Group of 2018 Chinese Guidelinesfor the Management of Hypertension, Chinese Hypertension League, Chinese Society of Cardiology et al. 2018 Chinese guidelines for the management of hypertension. Chin J Cardiovasc Med. 24, 24–56. (2019).
Chinese Diabetes Society. Guidelines for the prevention and control of type 2 diabetes in China (2017 Edition).Chin. J. Pract. Internal Med. 38, 292–344. https://doi.org/10.19538/j.nk2018040108. (2018).
Joint committee for guideline revision. 2016 Chinese guidelines for the management of dyslipidemia in adults[J]. J Geriatr Cardiol. 15, 1–29 (2018).
Chen, Z. et al. China Kadoorie Biobank of 0.5 million people: survey methods, baseline characteristics and long-term follow-up. Int. J. Epidemiol. 40, 1652–1666. https://doi.org/10.1093/ije/dyr120 (2011).
Sadarangani, K. P., Hamer, M., Mindell, J. S., Coombs, N. A. & Stamatakis, E. Physical activity and risk of all-cause and cardiovascular disease mortality in diabetic adults from Great Britain: Pooled analysis of 10 population-based cohorts. Diabetes Care 37, 1016–1023. https://doi.org/10.2337/dc13-1816 (2014).
Tsai, J. et al. Latent class analysis of personality disorders in adults with posttraumatic stress disorder: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry. 75, 276–284. https://doi.org/10.4088/JCP.13m08466 (2014).
Ng, S. W., Howard, A. G., Wang, H. J., Su, C. & Zhang, B. The physical activity transition among adults in China: 1991–2011. Obes Rev. 1, 27–36 (2014).
Ding, X. B. Study on the correlation between physical activity and chronic diseases among residents in Chongqing. Mod. Prevent. Med. 43, 2992–2996 (2016).
Ma, F. C. et al. Relationship between the physical activity level and non-communicable chronic diseases among adult residents in Qinghai province. Chin. J. Prev. Contr. Chron. Dis. 24, 481–484 (2016).
Institute for Health Metrics and Evaluation (IHME): GBD compare data visualization [EB/OL] http: //vizhub.healthdata.org/gbd-compare.
Lanier, J. B., Bury, D. C. & Richardson, S. W. Diet and physical activity for cardiovascular disease prevention. Am. Fam. Phys. 93, 919–924 (2016).
Piercy, K. L. et al. The physical activity guidelines for Americans. JAMA 320, 2020–2028. https://doi.org/10.1001/jama.2018.14854 (2018).
Farhangi, M. A. & Jahangiry, L. Gender difference in the association between Framingham Risk Score with cardio-metabolic risk factors and psychological distress in patients with metabolic syndrome. Diabetes Metab. Syndr. 14, 71–75. https://doi.org/10.1016/j.dsx.2019.12.009 (2020).
Borhanuddin, B. et al. 10-year cardiovascular disease risk estimation based on lipid profile-based and BMI-based framingham risk scores across multiple sociodemographic characteristics: The malaysian cohort project. Sci. World J. 2018, 2979206. https://doi.org/10.1155/2018/2979206 (2018).
Pitanga, F., Matos, S., Almeida, M., Barreto, S. M. & Aquino, E. Leisure-time physical activity, but not commuting physical activity, is associated with cardiovascular risk among ELSA-Brasil participants. Arq. Bras. Cardiol. 110, 36–43. https://doi.org/10.5935/abc.20170178 (2018).
American College of Sports Medicine. Position Stand. Physical activity, physical fitness, and hypertension. Med. Sci. Sports Exerc. 25, 1–10 (1993).
The Joint Task Force for Guideline on the Assessment and Management of Cardiovascular Risk in China. Guideline on the Assessment and Management of Cardiovascular Risk in China. Chinese Circulation Journal. 34, 4–28 (2019).
Acknowledgements
We would like to thank the investigators from the ten investigation areas (Yulong District in Xuzhou, Donghai County in Lianyungang, Sucheng District in Suqian, Hongze County in Huaian, Xiangshui County in Yancheng, Hanjiang District in Yangzhou, Rugao County in Nantong, Jiangyan County in Taizhou, Pukou District in Nanjing and Runzhou District in Zhengjiang) for all their work and support. We also thank Professor Zhang Yongqing (Jiangsu Center for Disease Control and Prevention) and Professor Ling Ping (Jiangsu Center for Disease Control and Prevention) for providing constructive suggestion.
Funding
This work was supported by the Natural Science Foundations of China (81973005) and the Natural Science Foundation of Jiangsu Province (BK20151593).
Author information
Authors and Affiliations
Contributions
Q.X., Z.Z., C.C., Y.Q., Z.W. conceptualized study concept and design; C.C., J.L., S.L., G.D., J.W., Q.X. collected the data; C.C., J.L., S.L., G.D., J.W., Y.Q., Q.X., X.W. analyze and interpret data; C.C., J.L., S.L., Y.Q., X.W., Q.X. drafted the manuscript; C.C., J.L., S.L., Y.Q., Q.X. revised the manuscript that had important intellectual content; C.C., J.L., S.L., Y.Q., G.D., J. Wang conducted statistical analysis; Q.X. obtained funding; S.L., Y.Q., X.W., Z.Z., C.C. provided technical, or material support; Q.X. studied supervision. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chen, C., Liu, J., Lu, S. et al. Study on the associations of physical activity types and cardiovascular diseases among Chinese population using latent class analysis method. Sci Rep 12, 8081 (2022). https://doi.org/10.1038/s41598-022-12182-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-12182-9
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
