
Abstract
The aim of this study was to investigate whether loneliness and personality traits correlate with the treatment outcome of methamphetamine use disorder. In this 1-year longitudinal study, a total 106 participants (98 males, 8 females), with a mean age 36.3 ± 9.6 years were enrolled. We measured UCLA Loneliness Scale and Tridimensional Personality Questionnaire at baseline, while craving level at baseline, week 12, 24, 36, and 48. Urinary methamphetamine tests were given 17 times. For the evaluation of the data, multiple linear regression and generalized linear mixed models were used. The baseline results showed lower levels of the harm avoidance trait and higher levels of loneliness were significantly associated with higher craving levels (p=0.04 and 0.04). Moreover, loneliness was not only positively associated with craving levels (B=0.05, p<0.01) but with urinary methamphetamine positive results (B= 0.08, p=0.03) during one-year treatment. The findings suggested that loneliness was associated with poor methamphetamine treatment outcome (greater craving levels and higher proportion of positive methamphetamine urine tests) and lower harm avoidance traits are associated with higher craving levels.
Similar content being viewed by others
Introduction
In the past decades, the use of methamphetamine-type stimulants increased rapidly worldwide. Over the period 2009–2019, the quantities of methamphetamine seized increase almost ten times with a profound increase in East and South East Asia1. Those who abused methamphetamine-type stimulants commonly started in their late teenage years or their early twenties. Any application of methamphetamines increases the risk of cardiovascular injury2, neurological damage3, psychosis, violence, suicidality, depression, and dementia4,5. Those who had methamphetamine abuse were more likely to have domestic violence toward their intimate partners6, intentional self-inflicted injury or internal assaults7, and increased annual hospital costs8. Problematic methamphetamine use is less well defined, but methamphetamine use disorder is defined as “a pattern of amphetamine-type substance use leading to clinical significant impairment or distress when at least two of 11 criteria (Diagnostic and Statistical Manual of Mental Disorder, Fifth Edition, DSM-5) within a 12-month period” including a longer period or a larger amount consumption then intended, cravings, tolerance, and withdrawal9. Up to date, there is still no effective pharmacotherapy for methamphetamine dependence10. Therefore, it is warranted to explore and to identify the complex associations with the psychological and sociodemographic factors for individuals with methamphetamine use disorder.
Several papers across different countries and ethnicities reported personality traits play a vital role in subjective effects and addictive behaviors11,12,13. For example, individuals with lower harm avoidance traits were associated with greater positive activation effects of amphetamine but such association were not observed in those who have higher trait of impulsivity14. Individuals who were high in neuroticism and low in conscientiousness were more like to consume drugs15. Furthermore, higher levels of antisocial traits and aggressive traits in those who had substance use disorder were significant predictors of higher drop out from treatment16. That using Cloninger’s Temperament Scales is an effective tool to explore the correlations between personality traits and substance-related behaviors17. Based on Cloninger’s theory of personality, Cloninger’s Tridimensional Personality Questionnaire consist of 3 domains: Novelty Seeking (NS), Harm Avoidance (HA), and Reward Dependence (RD). In Cloninger’s personality models, NS is characterized by low tolerance to boredom and a willingness to take risks for the sake of stimulations, HA is characterized by higher tendency to responds intensely to aversive stimuli and to learn to passively avoid punishment, and RD is characterized as a tendency to respond markedly to signals of reward18. NS and HA are associated with higher risk of substance abuse17,19. For example, those who had stimulant abuse reported higher scores of NS, while those who had opioid and hypnotics abuse reported higher scores of HA20. In addition, both human and rodent studies demonstrated that high novelty seeking can predict an earlier beginning stage of drug abuse and a transition to compulsive drug use and relapse21. Moreover, high levels of HA and NS are also associated with higher risk for the development of methamphetamine dependence among methamphetamine users22. Substance abusers with higher level of NS and HA are associated with higher tendencies to suffer from somatic and emotional distress19. Nonetheless, there remains debate over RD as a reliable dimension of temperament23 and some studies tried to identify personal risk factors to reduce the severity of dependence and the odds of positive urine methamphetamine test in methamphetamine use disorder, their results remain inconclusive10,24.
Loneliness is a subjectively distressing feeling when an individual perceives a lack of quality or quantity in interpersonal relationships25. A host of reports indicate that loneliness is associated with mental health symptomatology such as depression and anxiety, and addictive behaviors26. The feeling of loneliness is stronger with drug abuse than without. The feeling of loneliness increases the odds of abusing drugs and taking part in high risk behaviors27. Lonely individuals were found significantly correlated to compulsive internet use, excessive alcohol use, and problem gambling28. Furthermore, loneliness increased odds of using illicit opioids among those who received methadone maintenance treatment29. These addictive behaviors and drug abuse may damage one's social networks, leading to loneliness in turn30,31. Although social supports may assuage loneliness and lead to healthier behaviors, loneliness oppositely diminished the positive association between social support and better health more profoundly32. However, the effects of loneliness on reducing the odds of positive urine methamphetamine tests and craving levels among those who have methamphetamine use disorder remain unclear.
In a recent study, the loneliness effects were longitudinally associated with the development of personality traits from late adolescence to early midlife. Loneliness was positively associated with neuroticism and negatively with extraversion and agreeableness33. Furthermore, higher levels of loneliness predicted less perceived self-control and a tendency to avoid risks34. Loneliness positively correlated with anxiety and negatively with social risk-taking so that loneliness may positively correlate with HA35. The rank-order pattern for loneliness was as stable as the personality characteristics and which followed an inverted U-shape trajectory across the life span36. In one Korea study, dependent personality significantly correlated with smartphone addiction and loneliness. In advance, loneliness partially mediated the relationship between dependent personality and smartphone addiction37. Both personality traits and loneliness are correlated with substance abuse, whereas there are scarce of studies examining the impacts simultaneously of loneliness and personality traits on the treatment outcome of methamphetamine use order.
In the current study, we investigate the associations between loneliness and personality traits, and treatment outcomes in patients with methamphetamine use disorder. We hypothesize that higher loneliness and greater tendency of NS and HA personality traits are associated with poorer treatment outcome of methamphetamine use disorder. We choose the independent variables as loneliness and personality traits, measuring craving levels, and the results of urinary methamphetamine tests as the treatment outcome variables of methamphetamine use disorder.
Methods
Study design
This is a 1-year longitudinal study focusing on the effects of loneliness and personality traits on treatment outcomes in those who had methamphetamine use disorder and received the 1-year treatment program.
Setting
Patients with methamphetamine use disorder were recruited between Jan. 2019 and Dec. 2020 from the addiction clinics of National Cheng Kung University Hospital (NCKUH). All of them received the 3-stage treatment program including physical and psychiatric managements, psychotherapies, and other psychosocial interventions within 1 year. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (the Institutional Review Board at NCKUH, IRB No: A-ER-106-197) and with the Helsinki Declaration of 1975, as revised in 2000. The study procedures were fully explained to each participant before they signed an informed consent.
Participants
Each participant was interviewed by a board-certified psychiatrist to confirm an initial diagnosis. The first interview was based on the criteria of the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5). The second interview was conducted by a well-trained study member to screen other comorbid psychiatric disorders. It was based on the Chinese version of the Mini International Neuropsychiatric Interview (MINI), established on the concepts of DSM-IV. MINI has been widely used in clinical trials and epidemiological studies with an interrater reliability of 0.7538.
The participants were between 18 and 65 years old. The participants who were not capable of signing the informed consent or completing the questionnaire, were excluded. Another reason for exclusion was a serious medical or physical condition requiring immediate hospitalization.
The three-stage treatment program
The treatment program was built on the “Clinical Treatment Guideline for Schedule II Substance Users” (Taiwan Ministry of Health and Welfare, 2017; http://www.dep.mohw.gov.tw/DOMHAOH/cp-4097-43400-107.html).
During the first treatment stage of 4 weeks, the patients received diagnostic interviews to evaluate their substance use history and comorbidity of physical and psychiatric condition. Their demographic data, social functions, family support, and psychological functions were also evaluated during this period. The participants also received weekly outpatient follow-up and urine methamphetamine tests to monitor treatment response.
During the second treatment stage of 8 weeks, the patients received both a supportive and a 12-session group psychotherapy based on a cognitive behavior therapeutic approach. Psychoeducation and service linkages were also provided during this period. This second stage of the treatment program was only provided if the latest previous urinary methamphetamine results were negative. The patients kept receiving biweekly urine methamphetamine tests at an outpatient clinic.
During the third treatment stage of 36 weeks, the patients received a supportive psychotherapy, a 12-session group psychotherapy, and motivation enhancements to maintain methamphetamine abstinence. The urinary methamphetamine tests were given once a month during this period. Case managers were responsible for the treatment integration and monitored during all 3 stages.
Measures
UCLA loneliness scale and tridimensional personality questionnaire at baseline
UCLA loneliness
We assessed the level of loneliness through the UCLA Loneliness Scale (version 3), which is a widely used loneliness measure of high reliability and validity39. This test contains 20 items. The Cronbach’s alpha of this sample was 0.65. Participants rated how often they felt the way described in the item using a four-point Likert scale ranging from ‘never’ to ‘often’. Higher loneliness scores indicated greater loneliness.
Tridimensional personality questionnaire
We assessed the main personality dimensions through the Tridimensional Personality Questionnaire (TPQ) is a self-report personality inventory to measure three major personality dimensions: Novelty Seeking (NS), Harm Avoidance (HA), and Reward Dependence (RD). We used the Chinese version for evaluating the participants’ personality40. The Cronbach’s alpha values were as follows: for NS, Cronbach’s α = 0.72, for HA, Cronbach’s α = 0.89, and for RD, Cronbach’s α = 0.54. In the present study, we only measured NS and HA because the RD dimension was not reliable for Han Chinese in Taiwan40.
Outcome measurement: Visual Analogue Scale and urine methamphetamine test
We assessed the outcome variable through the Visual Analogue Scale (VAS) and methamphetamine urinalysis. During 1-year treatment program, each participant received 5 sets of Visual Analogue Scale (VAS) and 17 times urine methamphetamine tests.
Visual Analogue Scale
The VAS was used to assess the craving level of amphetamine by asking the participants: “How much did you crave/desire/want methamphetamine in the preceding week?”10. The participants responded the question with a 100-point Likert scale ranging from 0 (none) to 100 (very much) which was measured at baseline, weeks 12, 24, 36, and at the end of the 1-year treatment program to evaluate the craving levels of using methamphetamine.
Urine methamphetamine test
The patient provided their urine sample at each outpatient visit and a total of 17 binary methamphetamine urinalysis results were collected from each participant during the 1-year treatment program (first stage: 4 times once/week; second stage: 4 times once/2 weeks, third stage: 9 times once/4 weeks). Their urine samples were analyzed by using the Amphetamines II (AMPS2)® which is an in vitro diagnostic test for the qualitative and semiquantitative detection of methamphetamines in human urine on the Roche/Hitachi cobas c systems. The cutoff point of amphetamine concentration were 300 ng/ml, 500 ng/ml, and 1000 ng/ml when d-methamphetamine was calibrated.
Covariates
Less perceived social support and poorer family relationships were associated with greater loneliness and more severe depression, which had been demonstrated to correlate with poorer recovery/remission of addiction41,42. We measured the social support function, family adaptation, partnership, growth, affection, the resolve index (APGAR), and the Hamilton Depression Rating Scale (HDRS) as covariates at baseline.
Measurement of support function
The self-reported Measurement of Support Function (MSF) questionnaire had been used to assess social support status. The validity of this assessment in Taiwan was approved by previous studies. In this study, the Cronbach’s alpha of the 20 items was 0.83. This questionnaire consisted of four areas: perceived crisis support, perceived routine support, received crisis support, and received routine support. A higher score indicated more social support43.
Family adaptation, partnership, growth, affection, and resolve index
The Family Adaptation, Partnership, Growth, Affection, and Resolve (APGAR) index is composed of five domains: Adaptability, Partnership, Growth, Affection, and Resolve44. The Chinese version of family APGAR index has been validated in Taiwan45. The participants responded to the follow questions: “Are you satisfied with the help that you received from your family?,” “Do you talk with your family about your household problems?,” “Do you feel that your family loves you?,” “Are you satisfied with the time that you and your family share together?,” and “Do you discuss with your family about important decisions that affect the whole family?.” Each domain was answered along a 4-point Likert scale ranging from 1 (low satisfaction) to 4 (high satisfaction), thus the total scores ranged from 4 to 20. Higher score represented better family functions.
Hamilton Depression Rating Scale
The 17-item HDRS is for the measurement of the severity of depressive symptoms. This assessment provides comprehensive coverage of depressive symptoms. It has strong psychometric properties, high concurrent and differential validity, and strong reliability. The participants had to rate 11 items for the severity of depressive symptoms along a three- to five-point Likert scale. The total score ranged from 0 to 52. The Cronbach’s alpha of this sample was 0.7746. The higher scores of the 17-item HDRS indicated greater severity of depressive symptoms.
Baseline demographic and clinical characteristics
We collected the participants’ baseline demographic characteristics including age, sex, educational attainment, and marital status. The age and educational attainment were collected as continuous variables. We also recorded the duration of methamphetamine use by asking the participant: “How many years have you used methamphetamine?”. In addition, according to the evaluation results of MINI, the psychiatric comorbidities were itemized into 5 binary categories: Mood disorder (Yes/No), Anxiety disorder (Yes/No), Psychotic disorder (Yes/No), other substance use disorder (Yes/No), and Anti-social personality disorder (Yes/No). In each category, one point was assigned if the result was yes. Based on the sum of these 5 category result, the psychiatric comorbidity index is ranging from 0 to 5 and higher scores of psychiatric comorbidity index indicated more psychiatric comorbidities.
Statistical analysis
The analysis for obtaining descriptive statistics and a multiple linear regression was carried out with SAS 9.4 statistical software. Descriptive analysis was performed for all variables at baseline. If the distribution of the variable x was different from normal, we transformed log (x + 1) into normal distribution. Independent samples t tests or Chi-squared tests were used to assess associations between the demographic data and the outcome variables.
Because the VAS and urine methamphetamine tests had to be assessed repeatedly, the generalized linear mixed models (GLMMs) method was used for obtaining multiple linear regression analysis. GLMMs in repeated-measures analyses that accommodate randomly missing data47. Furthermore, hierarchical regression models were applied to investigate the association between loneliness, personality traits (TPQ-HA and TPQ-NS), and the outcome variables (VAS and urine methamphetamine test). For each outcome variable, three models were estimated at first stage and the endpoint during the 1-year treatment program. In Model 1, we regressed loneliness and personality traits (TPQ-HA and TPQ-NS) on the outcome variable. In Model 2, we then repeated the analyses, adjusting for age and education. In Model 3, we repeated the analyses adjusting for disease duration, psychiatric comorbidities, MSF, HDRS, family APGAR, and the numbers of visits.
All tests were evaluated at a 0.05 level of statistical significance.
Results
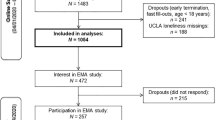
Table 1 summarized the participant characteristics at baseline and the endpoint. At baseline, there were 106 methamphetamine use patients enrolled (male: 92.4% and mean duration using methamphetamine: 6.5 ± 7.3 years). About fifty percent of the patients had psychiatric comorbidities other than methamphetamine use disorder. The independent variables of baseline loneliness score, TPQ-HA, and TPQ-NS score, and the outcome variables of baseline VAS score and the proportion of positive methamphetamine urine tests were listed in Table 1.
After 52 weeks of methamphetamine treatment, 41 out of 106 patients (male: 95.1%; and mean duration using methamphetamine: 7.7 ± 7.9 years) completed a total of 5 times of the VAS scores, but only 28 of them completed a total of 17 times of urine methamphetamine test. The latest VAS score and the proportion of positive urinary methamphetamine tests were lower than at baseline.
Table 2 displays the initial associations between independent variables and dependent variables, we collected the first stage of treatment outcome parameters for hierarchical regression analysis. Model 1 showed a positive association between loneliness and craving level (B = 0.05, p = 0.02) but a negative association between TPQ-HA and craving level (B = − 0.10, p = 0.01). In Model 2, adjusting for age and education, the positive association between loneliness and craving level (B = 0.05, p = 0.03) and the negative association between TPQ-HA and craving level (B = − 0.10, p = 0.01) remained consistent. In Model 3, the positive association between loneliness and craving level (B = 0.05, p = 0.04) and the negative association between TPQ-HA and craving level (B = − 0.09, p = 0.04) are consistent after adjusting for disease duration, psychiatric comorbidities, MSF, HDRS, family APGAR, and the numbers of visits remained robust. However, TPQ-NS was not significantly associated with craving level. We also examined the association between the independent variables and 4 times urine methamphetamine tests in total by GLMMs analysis. We found no significant association between the baseline of the independent variables and the first stage of urine methamphetamine tests.
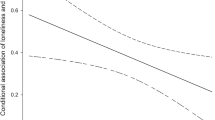
In advance, as shown in Table 3, we examined the associations between the baseline independent variables and the repetitive outcome variables, 5 sets of VAS scores and 17 urine methamphetamine tests, during the 1-year treatment program by GLMMs analysis. Model 1 on craving levels showed that loneliness was positively associated with greater levels of craving (B = 0.05, p = 0.003) but TPQ-HA was negatively associated with greater level of craving level (B = − 0.07, p = 0.02). Model 2 further added age and education, and the positive association between loneliness and craving level (B = 0.05, p = 0.003) and the negative association between TPQ-HA and craving level (B = − 0.07, p = 0.02) were consistent. Model 3 further adjusted disease duration, psychiatric comorbidities, MSF, HDRS, family APGAR, and the numbers of visits, the positive association between loneliness and craving level (B = 0.05, p = 0.03) and the negative association between TPQ-HA and craving level (B = − 0.07, p = 0.03) remained robust. However, in Model 3, the association between TPQ-NS and craving level was not significant (B = 0.05, p = 0.17).
Although, during 1-year program, Model 1 and Model 2 showed loneliness and personality traits insignificantly associated with positive urinary methamphetamine results, loneliness positively associated positive urinary methamphetamine results after adjusting disease duration, psychiatric comorbidities, MSF, HDRS, family APGAR, and the numbers of visits in Model 3 (B = 0.08, p = 0.04) (Table 3).
Discussion
In the present study, we hypothesized that higher loneliness and greater tendency of NS and HA personality traits were associated with greater craving levels of methamphetamine and higher proportion of positive urine methamphetamine results in those who attended the 1-year treatment program for methamphetamine use disorder. In accord with the hypothesis, our findings suggested that greater loneliness was associated with greater craving levels of methamphetamine and higher proportion of positive urine methamphetamine results. Not only at the first stage but at the end of treatment program remained the consistent findings between loneliness and the treatment outcomes of craving and positive urine methamphetamine results. However, inconsistent with the hypothesis, we found a negative association between HA personality trait and craving level of methamphetamine and a nonsignificant association between NS personality trait and craving level of methamphetamine. Neither HA personality trait nor NS personality were insignificantly associated with an increasing numbers of positive urine methamphetamine results.
Loneliness impacts social experiences and emotional states. It weakens the immune system and increases stress-related responses. When one feels lonely, a greater perceived loneliness is associated with increased ventral stratum and midbrain activity, contributing to “social craving” in a similar way as fasting causes hunger50,51. In parallel, it was previously shown that a negative emotional state leads to a change in the extended amygdala and increases perpetuation of drug-taking behavior to remunerate the negative feeling52. Those who experience loneliness have higher likelihood of depression and anxiety and are more likely to engage in impulsive behaviors such as unplanned spending and over-eating53,54. Both craving and stress relief trigger lonely individuals to search for the drug and impaired prefrontal top-down self-regulation diminishes their awareness of addiction52.
Our results suggest that lonely methamphetamine users have poor treatment response and higher tendency to use methamphetamine even they are under deferred prosecution status with close monitoring. We find that higher levels of loneliness are associated with higher craving levels of methamphetamine. Such association are observed both at baseline and during the 1-year methamphetamine treatment program in those participants with methamphetamine use disorder. In addition to higher craving levels, higher levels of loneliness are also associated with higher probability of using methamphetamine.
Compare with NS traits, we find lower HA traits were significantly associated with higher craving level of methamphetamine among those who received methamphetamine treatment program. In the previous study, NS and HA personality are correlated to gray’s biopsychological theory, the behavioral activation system (BAS) and behavioral inhibition system (BIS) respectively55. Once individuals know that a reward is likely to follow, those who had higher tendency of NS traits arise their behavioral action system to carry out some behaviors to attain reward when they were exposed to the environment cues of the drug. They also had higher level of craving and long-term vulnerability of relapse of psychostimulant drug abuse56. However, when individuals developed with psychostimulant drug dependence, avoiding aversive feeling passively instead of achieving rewards actively may be more significantly lead them to use psychostimulant drug57,58. Although people with higher levels of HA are associated with lower social adaption and higher risk for affective disorders59, people with lower levels of HA have difficulties in avoiding aversive outcomes when looking for immediate monetary rewards60.
There were several limitations in the present study. (1) The sample size was medium, and the attrition rate was high. Only 39% of the participants completed the 1-year longitudinal evaluation and during the 1-year treatment program we collected: 68.1% of craving level evaluations (106 participants, 5 test occasions, 361 out of 530 samples); 66.7% of urinary methamphetamine test results (106 participants, 17 test occasions, 1202 out of 1802 samples). (2) Over 95% of the participants in this study were convicted of methamphetamine abuse and underwent the deferred prosecution program, which simultaneously request them to attend the 1-year treatment-based program. Although we had explained to the participants that the assessments in the current study were not related with their legal issue, some participants may under-report their severity of craving. (3) Although the evidence of personality change following substance use remains inconsistent15, it is possible that methamphetamine use may change the personality and the personality changes may persisted over the course of the study as participants were treated61. These results need to be interpreted cautiously to determining the long-term outcomes. (4) Because of limited completion of measurement during the 1-year program, we only used the first stage of measurements in the mediation analysis about the role of loneliness between personality and craving level. The mediation effect of loneliness on the association between personality and craving level needs to be verified again in future studies.
Conclusion
We found loneliness is associated with poorer methamphetamine treatment outcomes. Higher loneliness levels were associated with higher craving levels and higher tendency of methamphetamine use. In addition, lower HA personality is associated with higher craving levels of methamphetamine. Additional studies on regulating loneliness to improve treatment outcomes in methamphetamine use patients may be warranted.
References
United Nations Office on Drug and Crime. World Drug Report 2021. https://www.unodc.org/unodc/en/data-and-analysis/wdr2021.html (2021).
Bazmi, E. et al. Cardiovascular complications of acute amphetamine abuse: Cross-sectional study. Sultan Qaboos Univ. Med. J. 17(1), e31–e37 (2017).
Silva, A. P. et al. Brain injury associated with widely abused amphetamines: Neuroinflammation, neurogenesis and blood–brain barrier. Curr. Drug Abuse Rev. 3(4), 239–254 (2010).
McKetin, R. et al. Mental health outcomes associated with the use of amphetamines: A systematic review and meta-analysis. EClinicalMedicine 16, 81–97 (2019).
Tzeng, N.-S. et al. Association between amphetamine-related disorders and dementia—A nationwide cohort study in Taiwan. Ann. Clin. Transl. Neurol. 7, 1284–1295 (2020).
Morgan, A. & Gannoni, A. Methamphetamine dependence and domestic violence among police detainees. Trends Issues Crime Crim. Justice 588, 1–17 (2020).
Tominaga, G. T. et al. Toll of methamphetamine on the trauma system. Arch. Surg. 139(8), 844–847 (2004).
Winkelman, T. N. A. et al. Evaluation of amphetamine-related hospitalizations and associated clinical outcomes and costs in the United States. JAMA Netw. Open 1(6), e183758 (2018).
Hamel, C. et al. Psychosocial and pharmacologic interventions for methamphetamine addiction: Protocol for a scoping review of the literature. Syst. Rev. 9(1), 245 (2020).
Siefried, K. J. et al. Pharmacological treatment of methamphetamine/amphetamine dependence: A systematic review. CNS Drugs 34(4), 337–365 (2020).
Shahini, N. et al. Temperament and character traits in substance use disorder in Iran: A case control study. BMC Psychol. 9(1), 138 (2021).
Seyed Hashemi, S. G. et al. Personality traits and substance use disorders: Comparative study with drug user and non-drug user population. Pers. Individ. Differ. 148, 50–56 (2019).
Hojjat, S. K. et al. Personality traits and identity styles in methamphetamine-dependent women: A comparative study. Global J. Health Sci. 8(1), 14–20 (2015).
White, T. L., Lott, D. C. & de Wit, H. Personality and the subjective effects of acute amphetamine in healthy volunteers. Neuropsychopharmacology 31(5), 1064–1074 (2006).
Kroencke, L. et al. How does substance use affect personality development? Disentangling between- and within-person effects. Soc. Psychol. Pers. Sci. 12(4), 517–527 (2020).
Papamalis, F. E. Examining the relationship of personality functioning and treatment completion in substance misuse treatment. Subst. Abuse Res. Treat. 14, 1178221820951777 (2020).
Hartman, C. et al. Using Cloninger’s temperament scales to predict substance-related behaviors in adolescents: A prospective longitudinal study. Am. J. Addict. 22(3), 246–251 (2013).
Cloninger, C. R., Svrakic, D. M. & Przybeck, T. R. A psychobiological model of temperament and character. Arch. Gen. Psychiatry 50(12), 975–990 (1993).
Ma, C. H. et al. Specific personality traits and associated psychosocial distresses among individuals with heroin or methamphetamine use disorder in Taiwan. J. Formos Med. Assoc. 119(3), 735–742 (2020).
Hurtado, G. et al. Personality dimensions and drug of choice: A descriptive study using Cloninger’s temperament and character inventory revised. Eur. Psychiatry 33(S1), S298–S299 (2016).
Wingo, T. et al. Novelty seeking and drug addiction in humans and animals: From behavior to molecules. J. Neuroimmune Pharmacol. 11(3), 456–470 (2016).
Tzeng, N.-S. et al. The dopamine transporter gene may not contribute to susceptibility and the specific personality traits of amphetamine dependence. Drug Alcohol Depend. 149, 100–107 (2015).
Gillespie, N. A. et al. The genetic and environmental relationship between Cloninger’s dimensions of temperament and character. Pers. Individ. Differ. 35(8), 1931–1946 (2003).
Khoramizadeh, M. et al. Treatment of amphetamine abuse/use disorder: A systematic review of a recent health concern. Daru 27(2), 743–753 (2019).
Weiss, R. S. Reflections on the present state of loneliness research. J. Soc. Behav. Pers. 2(Pt 2), 1–16 (1987).
Hawkley, L. C. & Cacioppo, J. T. Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Ann. Behav. Med. 40(2), 218–227 (2010).
Hosseinbor, M. et al. Emotional and social loneliness in individuals with and without substance dependence disorder. Int. J. High Risk Behav. Addict. 3(3), e22688–e22688 (2014).
Savolainen, I. et al. The role of perceived loneliness in youth addictive behaviors: Cross-national survey study. J. Med. Internet Res. 7, e14035 (2020).
Polenick, C. A. et al. Loneliness and illicit opioid use among methadone maintenance treatment patients. Subst. Use Misuse 54(13), 2089–2098 (2019).
Christie, N. C. The role of social isolation in opioid addiction. Soc. Cogn. Affect. Neurosci. 16(7), 645–656 (2021).
Wootton, R. E. et al. Bidirectional effects between loneliness, smoking and alcohol use: Evidence from a Mendelian randomization study. Addiction 116(2), 400–406 (2021).
Segrin, C. & Passalacqua, S. A. Functions of loneliness, social support, health behaviors, and stress in association with poor health. Health Commun. 25(4), 312–322 (2010).
Mund, M. & Neyer, F. J. Loneliness effects on personality. Int. J. Behav. Dev. 43(2), 136–146 (2018).
Zhu, Y. & Wang, C. The lonelier, the more conservative? A research about loneliness and risky decision-making. Psychology 08, 1570–1585 (2017).
MacDonald, K. B. & Schermer, J. A. Loneliness unlocked: Associations with smartphone use and personality. Acta Physiol. (Oxf) 221, 103454 (2021).
Mund, M. et al. The stability and change of loneliness across the life span: A meta-analysis of longitudinal studies. Pers. Soc. Psychol. Rev. 24(1), 24–52 (2020).
Ok, J. The mediating effects of loneliness on the relationship between smartphone addiction and dependent personality trait in adults. Korea J. Health Promot. 16(4), 260–267 (2016).
Sheehan, D. V. et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 59(Suppl 20), 22–33 (1998) (quiz 34–57).
Russell, D. W. UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. J. Pers. Assess. 66(1), 20–40 (1996).
Chen, W. J. et al. Cloninger’s Tridimensional Personality Questionnaire: Psychometric properties and construct validity in Taiwanese adults. Compr. Psychiatry 43(2), 158–166 (2002).
Wang, J. et al. Associations between loneliness and perceived social support and outcomes of mental health problems: A systematic review. BMC Psychiatry 18(1), 156 (2018).
Kelly, S. M. et al. The relationship of social support to treatment entry and engagement: The Community Assessment Inventory. Subst. Abuse 31(1), 43–52 (2010).
Lin, N., Ye, X. & Ensel, W. M. Social support and depressed mood: A structural analysis. J. Health Soc. Behav. 40(4), 344–359 (1999).
Smilkstein, G. The family APGAR: A proposal for a family function test and its use by physicians. J. Fam. Pract. 6(6), 1231–1239 (1978).
Chau, T.T., S.F. Hsieh, and H.W. Liu, [The use of extended family APGAR index in OPD]. Gaoxiong Yi Xue Ke Xue Za Zhi, 7(2):75–80 (1991).
Zheng, Y. P. et al. Validity and reliability of the Chinese Hamilton Depression Rating Scale. Br. J. Psychiatry 152, 660–664 (1988).
Ibrahim, J. G. & Molenberghs, G. Missing data methods in longitudinal studies: A review. Test (Madrid, Spain) 18(1), 1–43 (2009).
Baron, R. M. & Kenny, D. A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 51(6), 1173–1182 (1986).
Shrout, P. E. & Bolger, N. Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychol. Methods 7(4), 422–445 (2002).
Tomova, L. et al. Acute social isolation evokes midbrain craving responses similar to hunger. Nat. Neurosci. 23(12), 1597–1605 (2020).
Inagaki, T. K. et al. Yearning for connection? Loneliness is associated with increased ventral striatum activity to close others. Soc. Cogn. Affect. Neurosci. 11(7), 1096–1101 (2016).
Volkow, N. D., Michaelides, M. & Baler, R. The neuroscience of drug reward and addiction. Physiol. Rev. 99(4), 2115–2140 (2019).
Peng, L., Xia, X. & Su, X. The effect of consumer’s loneliness on impulse buying in the internet era: A model based on para-social interaction. In 2020 2nd International Conference on Economic Management and Model Engineering (ICEMME) (2020).
Tatsi, E. et al. Emotion dysregulation and loneliness as predictors of food addiction. J. Health Soc. Sci. 4, 43–58 (2019).
Mardaga, S. & Hansenne, M. Relationships between Cloninger’s biosocial model of personality and the behavioral inhibition/approach systems (BIS/BAS). Pers. Individ. Differ. 42, 715–722 (2007).
Arenas, M. C. et al. Influence of the novelty-seeking endophenotype on the rewarding effects of psychostimulant drugs in animal models. Curr. Neuropharmacol. 14(1), 87–100 (2016).
Franques, P., Auriacombe, M. & Tignol, J. Addiction and personality. Encephale 26(1), 68–78 (2000).
Koob, G. F. & Volkow, N. D. Neurocircuitry of addiction. Neuropsychopharmacology 35(1), 217–238 (2010).
Tse, W. S. & Bond, A. J. The Application of the Temperament and Character Inventory (TCI) in predicting general social adaptation and specific social behaviors in a dyadic interaction. J. Appl. Soc. Psychol. 35(8), 1571–1586 (2005).
Howe, L. K. & Finn, P. R. The influence of harm avoidance and impulsivity on delay discounting rates. Pers. Individ. Differ. 152, 109564 (2020).
Wada, K. & Fukui, S. Relationship between years of methamphetamine use and symptoms of methamphetamine psychosis. Arukoru Kenkyuto Yakubutsu Ison 25(3), 143–158 (1990).
Acknowledgements
This study and has not been pre-registered, and the supportive and 12-session group psychotherapy were not previously published. The authors would like to thank Miss Chien-Yu Tseng and Yu Ting Hung for their assistance in the preparation of the manuscript.
Funding
This study was supported by research grants from the Ministry of Science and Technology (MOST-109-2314-B-006 -056 and MOST-107-2314-B-006-067 to TYW), National Cheng Kung University Hospital (NCKUH-11004011), and the Integrated Drug Addiction Treatment Center of the Jianan Psychiatric Center of the Ministry of Health and Welfare, Taiwan.
Author information
Authors and Affiliations
Contributions
Author T.-Y.T. and T.-Y.W. designed the study and wrote the protocol. Author T.-Y.W. supervised the laboratory work and the data analyses. Author T.-Y.T., T.-Y.W., H.-H.T., and K.-C.C. recruited participants. T.-Y.T. wrote the first draft of the manuscript. T.-Y.W., H.-H.T., C.-J.C., P.-S.C., and Y.-K.Y. reviewed the literature and contributed to the discussion. All authors contributed to and reviewed the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tsai, TY., Wang, TY., Tseng, HH. et al. Correlation between loneliness, personality traits, and treatment outcomes in patients with methamphetamine use disorder. Sci Rep 12, 8629 (2022). https://doi.org/10.1038/s41598-022-11901-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-11901-6
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
