
Abstract
This study investigated the accuracy of self-reported weight among Kuwaiti adolescents and the associations of self-reported weight and calculated BMI with the impact of media use on adolescent’s decision to lose weight and body thinness perception. A total of 706 Kuwaiti adolescents (363 females) 15–18 year-olds were randomly selected from schools. Weight and height were self-reported by the adolescents and measured by the researchers. A specifically designed questionnaire reported the impact of media use on adolescent’s decision to lose weight and body thinness perception. There were significant (p < 0.001) relationships between measured and reported weight (r = 0.947), height (r = 0.777), and calculated BMI (r = 0.623). Intraclass correlation coefficients (95% CI) between self-reported and measured weight and height were 0.973 (0.968–0.977) and 0.867 (0.839–0.891), respectively. The mean differences between self-reported and measured weight (1.26 kg) and BMI (0.478 kg/m2) were relatively small. Females under-reported their weight and the calculated BMI from estimated weight and height was underestimated by adolescents with overweight/obesity. The impact of media use on the adolescent’s perception of being thin relative to the accuracy of the calculated BMI was significant (p = 0.043–0.001). The age-adjusted odds ratio of the calculated (underestimated) BMI in adolescents without overweight/obesity was 0.437 (95% CI = 0.257–0.741; p = 0.002). It was concluded that the validity of self-reported weight was high. Adolescents with overweight/obesity were more likely to underestimate their weight and calculated BMI. Educating adolescents about proper lifestyles and weight loss through media appears warranted.
Similar content being viewed by others

Introduction
Anthropometric measurements, including weight, height, and body mass index (BMI), are often used for assessing the physical growth, nutritional status, and overall health of children and adolescents1. Although BMI is considered a crude estimate of excess body weight, it is an internationally accepted obesity assessment method, as it generally correlates well with body fat in the population2,3. It is well-recognized, though, that excess body weight is largely associated with non-communicable diseases such as cardiovascular illness, type 2 diabetes mellitus, and hypertension3. Objective measurements of weight and height are usually desired when calculating BMI; however, due to time, financial resources, and manpower constraints4, self-reported weight and height are commonly used in large epidemiology surveys and surveillance systems to generate regional and national estimates of overweight and obesity5,6. Decision makers often use such information to allocate resources and set priorities in health care systems7.
Although self-reported body weight and height measures are subject to inaccuracy, which can result in incorrect BMI classification, self-reported measurements of body weight and height have been used to obtain estimative of important parameters in some epidemiological surveys. In a large national surveillance in Brazil, the mean agreements between self-reported and measured weight and height were 99.6% and 100.6%, respectively8. Also, results from the School Physical Activity and Nutrition surveillance system in Texas, USA, which included more than 24,000 students in the 8th and 11th grades, indicated that when direct measurement of weight and height is not practical, self-reported assessment offers a reliable proxy measure in adolescents9. Some studies, however, have identified a greater discrepancy in self-reported and measured height and weight among certain groups, including overweight or obese individuals compared to healthy or underweight individuals10,11,12,13,14. An increasing number of children and adolescents worldwide are overweight, and the first step in preventing obesity is to identify those individuals at risk of becoming overweight. Mexican children and adolescents 10–16 years old, who were diagnosed with overweight/obesity, revealed that the barriers to losing weight from the perspective of the children and their parents included lack of perception of being overweight and its identification as a disease and its consequences15. It is therefore surprising that not many studies have investigated the discrepancy between self-reported and measured body weight and height in the Arab countries10,16. Indeed, to the authors’ best knowledge, the accuracy of self-reported weight and height among Kuwaiti adolescents has not been previously reported.
Factors associated with misperception of body weight are many and include age, sex, ethnicity, socio-economic status, BMI status, body-size perception and weight status, pubertal status, place of residence, physical activity, smoking, sedentary behaviors, and vegetable and fruit consumption17,18,19. However, the pressure from mass media (television, magazines, and social media) on body weight concerns is usually enormous, especially among young people. Young women who spent time on Facebook, were reported to be in a more negative mood than those who were exposed to the control website20. In addition, a study showed that such media pressure on female university students from five Arab countries led to a greater risk of dieting to lose weight and changed their ideas of a perfect body shape21. A cross-sectional survey that was conducted on Jordanian school adolescents aged 15–18 years found that most adolescents with or without obesity had shown a high impact of reading magazines on their dieting to lose weight22. In a sample of 17- to 32-year-old university students from five Arab countries, exposure to television had a weaker association than exposure to magazines regarding females’ body weight concerns21. In addition, the majority of the American preadolescent and adolescent girls enrolled in 5th through 12th grades were unhappy with their body weight and shape, and this was strongly associated with the frequency of reading fashion magazines23. Further, an Australian study involving adolescents enrolled in Grades 7 and 9 showed that the major influences on weight loss for girls were pubertal status and exposure to the media24.
Therefore, the purpose of the present study was to investigate the accuracy of self-reported body weight and height among Kuwaiti adolescents in comparison with the measured values and to examine the associations of self-reported weight and the calculated BMI from the estimated weight and height with the impact of media use on adolescents’ decision to lose weight and their perception of body thinness.
Results
A total of 706 adolescents (363 females) between the ages of 15 and 18 years were included in the study. A very high response rate was obtained (above 95%). Based on measured weight and height, nearly 50% of the participants were overweight or obese. Approximately 33% of the participants did not report their weight and about 40% did not report their height. There were no significant differences (p values ranged from 0.071 to 0.994) in the responses to media-related variables between adolescents who reported their weight and height data and those who were missing their weight and height information. Results of ICC as a measure of absolute reliability indicated that the agreement between estimated (self-reported) and measured weight and height were high. (95% CI) were 0.973 (0.968–0.977) and 0.867 (0.839–0.891), respectively. The ICC between measured and the calculated BMI from estimated weight and height (95% CI) was 0.713 (0.647–0.766). Pearson correlation coefficients between measured and estimated weight, height, and BMI were 0.947, 0.777, and 0.623, respectively.
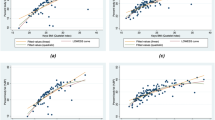
Table 1 shows the descriptive characteristics of the participants relative to gender. There was no significant difference (p = 0.466) in chronological age between male and female adolescents. However, there were significant gender differences between males and females in the reported age at pubertal maturation (p < 0.001), reported and measured body weight (p < 0.001) and height (p < 0.001), and estimated (p = 0.002) and measured (p = 0.031) BMI values. Moreover, Bland–Altman plots (Figs. 1 and 2) indicated that the mean differences between self-reported and measured weight and corresponding BMI were relatively small for the total sample (1.26 kg and 0.478 kg/m2, respectively). The majority of values fell within the upper and lower limits of agreement (± 2 SD), with random scatter plots and small systemic bias detected.

Bland and Altman levels of agreement plot for the measured and estimated body weight. The centered dotted line represents the mean differences or bias (1.26 kg) and the outer doted lines represent the upper (14.2 kg) and lower (− 11.7 kg) 95% of limits of agreement.

Bland and Altman levels of agreement plot for the actual and calculated BMI from self-reported weight and height. The centered dotted line represents the mean differences or bias (0.478 kg/m2) and the outer doted lines represent the upper (17.5 kg/m2) and lower (− 17.0 kg/m2) 95% of limits of agreement.
Table 2 presents the differences between measured and reported body weight, height, and BMI, relative to gender. No significant differences were observed between the measured and estimated weight, height, or BMI. Girls were significantly (p = 0.038) more likely to underreport their weight and hence obtain lower calculated BMI from the estimated weight and height values (not shown in table). There were no significant differences (p = 0.589) in the proportions of correctly calculated BMI from the estimated body weight and height in relation to gender (males = 4.9% and females = 5.8%). The findings also showed that self-reported age at maturation was not associated with self-reported weight, height, or with the degree of underestimation or overestimation of body weight or calculated BMI.
The accuracy of calculating BMI based on body weight and height estimation in relation to overweight or obesity status is displayed in Table 3. There was a significant difference (p = 0.028) in the accuracy of calculating BMI based on weight and height estimation by the Kuwaiti adolescents relative to overweight/obesity or non-overweight/non-obesity status. Adolescents with overweight or obese seemed to greatly underestimate their body weight and thus had lower calculated BMI from estimated weight and height values.
The influences of selected variables related to media on the accuracy of calculated BMI from body weight estimation by the Kuwaiti adolescents are shown in Table 4. The impact of reading newspapers (p < 0.001) or surfing the Internet (p = 0.002) on the adolescents’ decision to lose weight was significant. Also, the impact of the media on the adolescents’ perception to be thin relative to the accuracy of BMI calculation from the estimated weight and height was significant (p values ranged from 0.043 to 0.001). Those adolescents who were strongly influenced by the media to be thin appeared to underestimate their calculated BMI from their estimated weight and height. Finally, the results of the logistic regression analysis, adjusted for age, for selected variables relative to underestimation or overestimation of calculated BMI among Kuwaiti adolescents are shown in Table 5. The only significant difference between underestimation and overestimation of calculated BMI from estimated weight and height was overweight or obesity status. The age-adjusted odds ratio for adolescents without overweight or obesity when calculating BMI from their body weight estimation was 0.437 (95% CI = 0.257–0.741; p = 0.002).
Discussion
The present study investigated the accuracy of self-reported body weight and height among Kuwaiti adolescents and its associations with overweight or obesity. It also examined the associations of self-reported weight and BMI with the impact of media use on adolescents’ decision to lose weight and their perception of body thinness. The major findings showed that the reliability coefficient of self-reported weight was excellent (ICC = 0.973). Further, Bland–Altman plots indicated that the mean difference between self-reported and measured weight and the corresponding BMI were fairly small for the total sample (1.26 kg and 0.478 kg/m2, respectively), with random scatter plots and small systemic bias detected. Females were significantly more likely to under report their weight than males and hence obtain lower calculated BMI from estimated weight and height values. However, there were no significant differences in the proportions of correctly calculated BMI relative to gender. Moreover, adolescents with overweight or obesity, and those who were strongly influenced by the media to be thin, appeared to underestimate their calculated BMI from their estimated body weight and height. Overweight or obesity status was associated with under-estimation of adolescents’ body weight and calculated BMI.
Self-reported weight and height are commonly used in large epidemiological surveys and surveillance to create regional and national estimates of overweight and obesity, especially when direct measurements are not possible due to restrictions in budget and human resources5,6. Numerous studies have shown that self-reported weight and height may be acceptable5,9,18,25. However, the validity of self-reported weight and height among adolescents needs to be verified, as misreporting could lead to misclassification of BMI and therefore overestimation or underestimation of the burden of BMI-related diseases12,26,27,28. Self-reported weight and height data are not without some shortcomings. Missing self-reported data was raised as a problem in the Scottish Health Behaviour in School-Aged Children survey; nearly 59% of self-reported weight data was missing, with girls self-reporting less than boys29. Adolescents who reported low physical activity, low vegetable consumption, and high computer gaming on weekdays were more likely to not report their weight29. A study from Jeddah, Saudi Arabia, reported that more than half of the school children participants were unaware of their body weight and did not report such weight10. In the present study, approximately 30% of the Kuwaiti adolescents did not report their weight, and there were no significant differences in media-related variables between those adolescents reporting and not reporting their weight and height information.
In the current study, the value of absolute reliability between self-reported and measured body weight (0.973), as measured by the ICC coefficient, was considered excellent30. A similarly high ICC coefficient value between self-reported and direct measurement of body weight was reported for healthy school adolescents (0.96), and the mean difference between self-reported and direct measurement of weight, based on Bland–Altman plots, was relatively small18. Results of the Bland–Altman plot in the current study showed a small bias and a good agreement between self-reported and direct anthropometric measurements. The present study showed that the ICC between calculated BMI from measured and estimated height and weight was 0.713. In addition, based on Bland–Altman levels of agreement analysis, the mean difference between self-reported and measured weight and corresponding BMI were fairly small for the total sample (1.26 kg and 0.478 kg/m2, respectively), with random scatter plots and small systemic bias detected. Among American students from 8th to 11th grade, the differences in self-reported versus objectively measured height and weight resulted in underestimation of BMI ranging from − 0.23 kg/m2 among White boys to − 0.7 kg/m2 among African-American girls9. In a recent study conducted on young adults between 18 and 30 years, classification of BMI from self-reported and actual measurements showed that 88% of participants were placed in the same BMI category25. BMI values based on self-reported weight and height are described to be inaccurate for BMI prediction at an individual level12.
The results of the present study regarding the mean differences between self-reported and measured body weight and height were close to those reported in a study with Malaysian school adolescents18. However, the mean differences found in our study are much lower than those reported in studies with New Caledonian school-going adolescents17 and Saudi school children10. The results of this study are also similar to those found in a large surveillance with American students from 8 to 11th grade, in which adolescents overestimated their height and underestimated their weight9. Furthermore, our correlation coefficients between measured and self-reported anthropometric variables were similar, in direction and magnitude, to those reported by a recent study conducted on young Australian adults 18–30 years of age25.
Our findings showed significant gender differences between males and females in the self-reported and measured body weight, height, and calculated BMI from estimated weight and height values. Kuwaiti girls were significantly more likely to underreport their weight and hence end up with lower calculated BMI values. Elsewhere, the accuracy of anthropometric reporting by American female high school students was significantly higher than that of males31. Compared to boys in all age groups, differences between self-reported and directly measured weight, height and BMI were greater among Estonian adolescent girls32. than Among Australian youth, more females (70%) than males (35%) underreported their weight33. Also, female Saudi school children were observed to underestimate their body weight more than males10. However, the self-reported bias in body weight among Greek high school children did not differ relative to gender19.
Our study showed that nearly 70% of the Kuwaiti adolescents underreported their body weight to some degree. This finding of underreporting of body weight among adolescents is in agreement with previous studies conducted around the world9,18,19,27,33. However, the current study found a significant difference in the accuracy of calculating BMI based on weight and height estimation by the Kuwaiti adolescents relative to overweight or obesity status. Adolescents with overweight or obesity tended to underestimate their body weight and thus had lower calculated BMI values. Such findings have been substantiated in the previous literature. Underweight American high school students, underreported height and overreported weight, while overweight and obese students overreported height and underreported weight31. However, the differences between measured and estimated body weight among Greek high school students were higher among heavier students19. Also, obese Korean high school students, tended to underestimate their weight and BMI and overestimate their height more than non-obese adolescents26. In addition, the German Health Interview and Examination Survey for Children and Adolescents indicated that self-reported and measured height and weight can lead to inaccurate estimates of the prevalence of under- and overweight status27. Further, Jordanian adolescents with overweight or obesity were more likely to underestimate their weight and that having a BMI within the overweight/obesity category was a strong predictor of inconsistent weight perception16. Other studies also showing underreporting their weight include Australian youth33 and Malaysian adolescents18.
It is well recognized, however, that the prevalence of overweight or obesity based on self-reported data should be interpreted with caution because it could underestimate the true prevalence. It is not recommended to use self-reported data, especially in clinical settings, when assessing and monitoring an individual’s nutritional status for diagnosis of malnutrition and recommendation of nutritional intervention4. The magnitude of discrepancy between self-reported and measured weight and height and the corresponding BMI could be related to many potential factors, including age, sex, ethnicity, socio-economic status, sexual maturation, parental overweight, place of residence, and many lifestyle behaviors17,18,19,27. Also, parental health behaviors were reported to play a significant role in adolescents' body weight34. In the present study, self-reported age at maturation was not associated with self-reported weight, height, or degree of underestimation or overestimation of body weight or calculated BMI.
In recent years, social media marketing has become a preferred marketing strategy for a range of industries, including the food industry35, and the increase in social media marketing and communications that target children and adolescents has raised some major concerns20,36. Our findings showed that the impact of reading newspapers or surfing the Internet on adolescents’ decision to lose weight was significant, especially among those who underestimate or overestimate their calculated BMI from estimated body weight and height. Also, the media impact on the adolescents’ perception of being thin relative to the accuracy of the BMI calculation from estimated weight and height values was significant, particularly among those adolescents who underestimated or overestimated their calculated BMI. Different kinds of media may have different impacts on adolescents’ body weight-related aspects. For example, young university students from five Arab countries who were exposed to television had a weaker association than exposure to magazines regarding females’ body weight concerns21. Key indicators of eating disorders were significantly more prevalent among Fijian schoolgirls following prolonged exposure to television37. Among Jordanian school adolescents, most students with or without obesity had shown a high impact of reading magazines on their dieting to lose weight22. Furthermore, the majority of the American preadolescent and adolescent girls, who enrolled in 5th to 12th grade, were unhappy with their body weight and shape, and this was strongly associated with the frequency of reading fashion magazines23. Saudi adolescent girls exposed to television advertisements were more likely to consume dessert and have more attempts at losing weight38. Also, among American adolescents, media influence to lose weight was related to more frequent unhealthy weight control behaviors among boys with a BMI z-score of 1.23 or higher and among girls with low to average levels of global self-worth39.
The present study had several limitations. First, body weight is affected by many factors, including physical activity, sleep, and dietary habits. We did not assess any of these variables. Second, body weight, and hence BMI, is also affected by muscular status, especially among males who start engaging in body building activities at this age. This is another factor that we did not assess. Third, the survey used in the current study was subject to recall bias and social desirability effects. Fourth, the cross-sectional nature of the study does not imply causality of media impacts on overestimation or underestimation of body weight. Fifth, nearly 30% of our participants did not self-report their body weight. However, there were no significant differences in the responses to media-related variables between adolescents reporting their weight and height data and those who were missing their weight and height information. Sixth, in our questionnaires, unfortunately, we did not differentiate between mass media and social media. Despite these limitations, our results are consistent with several international studies suggesting that self-reporting of weight and height can be an acceptable method for assessing adolescent body weight and height. The results of the present study may be helpful in planning and developing novel surveys focused on health and anthropometric data.
Conclusion
The present study investigated the accuracy of self-reported body weight and height among Kuwaiti adolescents and its associations with overweight or obesity and examined the associations of self-reported weight and the calculated BMI from estimated weight and height with the impact of media use on adolescents’ decision to lose weight and their perception of body thinness. The major findings showed that the reliability coefficient of self-reported weight was excellent (ICC = 0.973). Further, Bland–Altman plots indicated that the mean difference between self-reported and measured weight and the corresponding BMI from estimated weight and height were fairly small for the total sample (1.26 kg and 0.478 kg/m2, respectively), with random scatter plots and small systemic bias detected. Females were significantly more likely to underreport their weight than males and hence end up with lower calculated BMI from estimated weight and height values. However, there were no significant differences in the proportions of correctly calculated BMI from estimated weight and height relative to gender. Moreover, adolescents with overweight or obesity appeared to underestimate their calculated BMI. Those adolescents who were strongly influenced by the media to be thin appeared to underestimate their calculated BMI from estimated weight and height. Overweight or obesity status was associated with underestimation of adolescents’ body weight and the corresponding calculated BMI. Compared to adolescents with overweight or obesity, the age-adjusted odds ratio of underestimated (calculated) BMI from weight and height in adolescents without overweight or obesity was 0.437 (95% CI = 0.257–0.741; p = 0.002). Educating adolescents about proper nutrition, physical activity, and weight loss through media appears warranted.
Methods
Sample selection
This cross-sectional study randomly selected Kuwaiti secondary students between the ages of 15 and 18 years using a multistage stratified sampling technique. Girls’ and boys’ public and private schools were used for selecting the sample based on geographical/administrative locations (governorates) in the State of Kuwait. One public boys’ school and one public girls’ school were selected from each governorate with a total of 10 schools. The data collection was conducted during the school year 2019. Additional two private boys’ schools and two private girls’ schools were also selected, totaling 14 public and private schools. In each school, one classroom from each grade (i.e., 10th, 11th, and 12th) was randomly chosen. A total sample of 343 boys and 363 girls was recruited for the study. Ethical approval was obtained from the Research Committee, College of Health Sciences, Public Authority for Applied Education and Training, Kuwait. The research procedures were conducted in accordance with the principles expressed in the Declaration of Helsinki. Informed consents were obtained from all participating students and consents were attained from their parents if they were younger than 18 year-olds. The Kuwait Ministry of Education approved the study.
Measurements
Body weight was measured to the nearest 100 g (Seca 875 Weight Scale) and height to the nearest 0.1 cm (Seca 213 Standiometer) by trained researchers. All measurements were conducted inside the schools with minimal clothing and without shoes. BMI was computed as the ratio of weight in kilograms divided by the squared height in meters. The extended International Obesity Task Force (IOTF) age- and sex-specific BMI cutoff reference standards were used to classify underweight, normal weight, and overweight or obesity relative to the adolescent’s age40. The participants were also asked to self-report their body weight and height. Further, male and female adolescents were asked to report their age at semenarche and menarche and used as indicator of age at maturation.
A previously used, specifically designed self-report questionnaire21 was utilized to obtain information on media use (television and Internet use and several questions on the impact of media on dieting to lose weight and the perception of body thinness). Examples of the questions include: How often do you read the newspapers, watch television, or use the Internet per day? Does reading the newspapers, watching television, or surfing the Internet influence you to lose weight? Does reading the newspapers, watching television or using the Internet influence your perception about body thinness?
Statistical analysis
Data were entered into an SPSS data file, checked, cleaned, and analyzed using IBM-SPSS program, version 22 (Chicago, IL, USA). Descriptive statistics were obtained for all variables and reported as means and standard deviations or percentages. Intraclass correlation coefficient (ICC) was used to test the absolute reliability of self-reported weight and height with a two-way mixed effects model. According to Shrout and Fleiss's classification, ICC values greater than 0.75 indicate excellent reliability, values between 0.04 and 0.75 indicate fair to good, and values less than 0.40 indicate poor reliability30. However, other references for the ICC coefficient consider values between 0.75 and 0.9 as indicating good reliability and values greater than 0.90 as indicating excellent reliability41.
The Bland–Altman limits of agreement were computed, and the mean differences (bias) as well as the 95% upper and lower limits of agreement plotted for differences between measured and estimated body weight or calculated BMI against means of measured and estimated weight or BMI42. Normality of the distribution of differences was tested using histograms. Differences between males and females in anthropometric measurements were tested using a t test for independent samples. Chi-square tests of proportions were used to test differences in selected variables related to the influence of media on adolescents’ decision to lose weight or their perception of body thinness according to overweight or obesity status. Two-way ANOVA (gender by age category) was used to test differences in the calculated BMI across ages and genders, with Bonferroni test used for correcting multiple testing. Logistic regression analysis, adjusted for age, was used to test differences in selected variables in relation to underestimation or overestimation of the calculated BMI from self-reported weight and height among Kuwaiti adolescents. If measured BMI was higher than the calculated BMI from estimated weight and height values, it was considered an underestimated BMI value, and if the measured BMI was lower than the estimated BMI, it was considered overestimated BMI value. The adjusted odds ratio (aOR) and confidence intervals were reported. The alpha level was set at 0.05, and a p-value less than the alpha level was considered significant.
Data availability
All data generated or analyzed during this study are included in this published article. Any additional data will be available from the corresponding author upon reasonable request.
References
Geserick, M. et al. Acceleration of BMI in early childhood and risk of sustained obesity. N. Engl. J. Med. 379(14), 1303–1312. https://doi.org/10.1056/NEJMoa1803527 (2018).
Giacchi, M., Mattei, R. & Rossi, S. Correction of the self-reported BMI in a teenage population. Int. J. Obes. Relat. Metab. Disord. 22, 673–677. https://doi.org/10.1038/sj.ijo.0800646 (1998).
NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet 387(10026), 1377–1396. https://doi.org/10.1016/S0140-6736(16)30054-X (2016).
Himes, J. H. Challenges of accurately measuring and using BMI and other indicators of obesity in children. Pediatrics 124(Suppl 1), S3–S22. https://doi.org/10.1542/peds.2008-3586D (2009).
Brener, N. D. et al. Centers for Disease Control and Prevention (CDC). Methodology of the Youth Risk Behavior Surveillance System-2013. MMWR Recomm. Rep. 62(RR-1), 1–20 (2013). https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6201a1.htm
Global School-based Student Health Survey (GSHS). http://www.cdc.gov/GSHS. Accessed 30 Apr 2021.
Gorber, S. C., Tremblay, M., Moher, D. & Gorber, B. A comparison of direct vs. self-report measures for assessing height, weight and body mass index: A systematic review. Obes Rev. 8, 307–326. https://doi.org/10.1111/j.1467-789X.2007.00347.x (2007).
Moreira, N. F. et al. Self-reported weight and height are valid measures to determine weight status: Results from the Brazilian National Health Survey (PNS 2013). Cad Saude Publica 34(5), e00063917. https://doi.org/10.1590/0102-311X00063917 (2018).
Pérez, A., Gabriel, K., Nehme, E. K., Mandell, D. J. & Hoelscher, D. M. Measuring the bias, precision, accuracy, and validity of self-reported height and weight in assessing overweight and obesity status among adolescents using a surveillance system. Int. J. Behav. Nutr. Phys. Act. 12(Suppl 1), S2. https://doi.org/10.1186/1479-5868-12-S1-S2 (2015).
Abalkhail, B. A., Shawky, S. & Soliman, N. K. Validity of self-reported weight and height among Saudi school children and adolescents. Saudi Med. J. 23, 831–837 (2002).
Elgar, F. J. & Stewart, J. M. Validity of self-report screening for overweight and obesity. Evidence from the Canadian Community Health Survey. Can. J. Public Health 99, 423–427. https://doi.org/10.1007/BF03405254 (2008).
Fonseca, H. et al. Validity of BMI based on self-reported weight and height in adolescents. Acta Paediatr. 99, 83–88. https://doi.org/10.1111/j.1651-2227.2009.01518.x (2010).
Sherry, B., Jefferds, M. E. & Grummer-Strawn, L. M. Accuracy of adolescent self-report of height and weight in assessing overweight status: A literature review. Arch. Pediatr. Adolesc. Med. 161, 1154–1161. https://doi.org/10.1001/archpedi.161.12.1154 (2007).
Wang, Z., Patterson, C. M. & Hills, A. P. A comparison of self-reported and measured height, weight and BMI in Australian adolescents. Aust. N. Z. J. Public Health 26, 473–478. https://doi.org/10.1111/j.1467-842x.2002.tb00350.x (2002).
Rodríguez-Ventura, A. L. et al. Barriers to lose weight from the perspective of children with overweight/obesity and their parents: A sociocultural approach. J Obes. 2014, 575184. https://doi.org/10.1155/2014/575184 (2014).
Al-Amer, R. et al. Accuracy of body weight estimation among Palestinian refugee adolescents living in Jordan: A cross-sectional study. J. Nurs. Scholarsh. 51, 642–650. https://doi.org/10.1111/jnu.12517 (2019).
Frayon, S. et al. Self-reported height and weight in Oceanian school-going adolescents and factors associated with errors. Asia Pac. J. Public Health 2017(29), 526–536. https://doi.org/10.1177/1010539517731362 (2017).
Kee, C. C. et al. Validity of self-reported weight and height: A cross-sectional study among Malaysian adolescents. BMC Med. Res. Methodol. 17, 85. https://doi.org/10.1186/s12874-017-0362-0 (2017).
Tokmakidis, S. P., Christodoulos, A. D. & Mantzouranis, N. I. Validity of self-reported anthropometric values used to assess body mass index and estimate obesity in Greek school children. J. Adolesc. Health 40, 305–310. https://doi.org/10.1016/j.jadohealth.2006.10.001 (2007).
Fardouly, J., Diedrichs, P. C., Vartanian, L. R. & Halliwell, E. Social comparisons on social media: The impact of Facebook on young women’s body image concerns and mood. Body Image 13, 38–45. https://doi.org/10.1016/j.bodyim.2014.12.002 (2015).
Musaiger, A. O. & Al-Mannai, M. Association between exposure to media and body weight concern among female university students in five Arab countries: A preliminary cross-cultural study. J Biosoc. Sci. 46, 240–247. https://doi.org/10.1017/S0021932013000278 (2014).
Tayyem, R. F. et al. Association between mass media and body weight concern among Jordanian adolescents’ residents of Amman: The role of gender and obesity. Environ. Health Prev. Med. 21, 430–438. https://doi.org/10.1007/s12199-016-0543-1 (2016).
Field, A. E. et al. Exposure to the mass media and weight concerns among girls. Pediatrics 103(3), E36. https://doi.org/10.1542/peds.103.3.e36 (1999).
McCabe, M. P., Ricciardelli, L. A. & Finemore, J. The role of puberty, media and popularity with peers on strategies to increase weight, decrease weight and increase muscle tone among adolescent boys and girls. J. Psychosom. Res. 52(3), 145–153. https://doi.org/10.1016/s0022-3999(01)00272-0 (2002).
Davies, A., Wellard-Cole, L., Rangan, A. & Allman-Farinelli, M. Validity of self-reported weight and height for BMI classification: A cross-sectional study among young adults. Nutrition 71, 110622. https://doi.org/10.1016/j.nut.2019.110622 (2020).
Bae, J. et al. Validity of self-reported height, weight, and body mass index of the Korea Youth Risk Behavior Web-based Survey questionnaire. J. Prev. Med. Public Health 43, 396–402. https://doi.org/10.3961/jpmph.2010.43.5.396 (2010).
Brettschneider, A. K., Rosario, A. S. & Ellert, U. Validity and predictors of BMI derived from self-reported height and weight among 11- to 17-year-old German adolescents from the KiGGS study. BMC Res. Notes 4, 414. https://doi.org/10.1186/1756-0500-4-414 (2011).
Zhou, X., Dibley, M. J., Cheng, Y., Ouyang, X. & Yan, H. Validity of self-reported weight, height and resultant body mass index in Chinese adolescents and factors associated with errors in self-reports. BMC Public Health 10, 190. https://doi.org/10.1186/1471-2458-10-190 (2010).
Aceves-Martins, M. et al. Self-reported weight and predictors of missing responses in youth. Nutrition 53, 54–58. https://doi.org/10.1016/j.nut.2018.01.003 (2018).
Shrout, P. E. & Fleiss, J. L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 86(2), 420–428. https://doi.org/10.1037//0033-2909.86.2.420 (1979).
Jayawardene, W., Lohrmann, D. & YoussefAgha, A. Discrepant body mass index: Behaviors associated with height and weight misreporting among US adolescents from the National Youth Physical Activity and Nutrition Study. Child Obes. 10(3), 225–233. https://doi.org/10.1089/chi.2014.0002 (2014).
Aasvee, K. et al. Validity of self-reported height and weight for estimating prevalence of overweight among Estonian adolescents: The Health Behaviour in School-aged Children study. BMC Res. Notes 8, 606. https://doi.org/10.1186/s13104-015-1587-9 (2015).
Bowring, A. L. et al. Measuring the accuracy of self-reported height and weight in a community-based sample of young people. BMC Med. Res. Methodol. 12, 175. https://doi.org/10.1186/1471-2288-12-175 (2012).
Baker, K. M., Healy, S., Rice, D. J. & Garcia, J. M. Adolescent weight and health behaviors and their associations with individual, social, and parental factors. J. Phys. Act. Health. https://doi.org/10.1123/jpah.2017-0279 (2018).
Kelly, B., Vandevijvere, S., Freeman, B. & Jenkin, G. New media but same old tricks: Food marketing to children in the digital age. Curr. Obes. Rep. 4(1), 37–45 (2015).
World Health Organization Regional Office for Europe. Monitoring and Restricting Digital Marketing of Unhealthy Products to Children and Adolescents: Report Based on the Expert Meeting on Monitoring of Digital Marketing of Unhealthy Products to Children and Adolescents (World Health Organization, 2018). https://www.euro.who.int/__data/assets/pdf_file/0008/396764/Online-version_Digital-Mktg_March2019.pdf. Accessed 28 Jan 2021.
Becker, A. E., Burwell, R. A., Gilman, S. E., Herzog, D. B. & Hamburg, P. Eating behaviours and attitudes following prolonged exposure to television among ethnic Fijian adolescent girls. Br. J. Psychiatry 180, 509–514. https://doi.org/10.1192/bjp.180.6.509 (2002).
Al-Jaaly, E. The impact of media and advertising of food on the eating behaviour of adolescent girls in Jeddah, Saudi Arabia. East Mediterr. Health J. 22, 662–667. https://doi.org/10.26719/2016.22.9.662 (2016).
Mayer-Brown, S., Lawless, C., Fedele, D., Dumont-Driscoll, M. & Janicke, D. M. The effects of media, self-esteem, and BMI on youth’s unhealthy weight control behaviors. Eat Behav. 21, 59–65. https://doi.org/10.1016/j.eatbeh.2015.11.010 (2016).
Cole, T. J. & Lobstein, T. Extended International (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 7, 284–294. https://doi.org/10.1111/j.2047-6310.2012.00064.x (2012).
Portney, L. G. & Watkins, M. P. Foundations of Clinical Research: Applications to Practice (Prentice Hall, 2000).
Bland, J. M. & Altman, D. G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1, 307–310 (1986).
Acknowledgements
We would like to thank all the participants for taking part in this study.
Funding
Professor Hazzaa M. Al-Hazzaa’s research has been funded by the Deanship of Scientific Research at Princess Nourah bint Abdulrahman University through the Fast-track Research Funding Program.
Author information
Authors and Affiliations
Contributions
Study concept: A.R.A. and H.M.A.; data collection: A.R.A., B.A.A., Y.A.A., F.A.A., and F.D.A.; statistical analyses: H.M.A.; interpretation of the findings: H.M.A., A.R.A., B.A.A., Y.A.A., F.A.A., and F.D.A.; drafting the paper: H.M.A. Revising the draft for important intellectual content: A.R.A., B.A.A., Y.A.A., F.A.A., and F.D.A. All authors critically read the draft, approved the final version of the manuscript to be published, and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Al-Hazzaa, H.M., Al-Awadhi, B.A., Al-Dashti, Y.A. et al. Adolescent’s self-reported weight and its association with media impact on decision to lose weight and body thinness perception. Sci Rep 12, 5908 (2022). https://doi.org/10.1038/s41598-022-09909-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-09909-z
This article is cited by
-
The influence of gender, media, and internet usage on adolescents' fast food perception and fluid intake
Journal of Health, Population and Nutrition (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
