
Abstract
The independent associations of body composition and physical fitness components with cardiovascular disease (CVD) risk factors in childhood are not fully understood. Thus, this cross-sectional study examined the independent associations of body composition and physical fitness with CVD risk factors in Swedish 9-year-old children (n = 411). Unadjusted linear regression analyses showed that body mass index (BMI), % fat mass and fat mass index were all positively associated with systolic and diastolic blood pressure, Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) and Metabolic Syndrome (MetS) score (all β ≥ 0.229, P ≤ 0.001). These associations were virtually unaffected by adjustments for basic covariates (child’s age and sex, maternal educational level and maternal BMI), fat-free mass and physical fitness. Fat-free mass index had generally weak associations with CVD risk factors and no associations were statistically significant after adjustments (all P > 0.27). Greater cardiorespiratory fitness and motor fitness were associated with lower HOMA-IR and MetS score in unadjusted models (all β ≤ − 0.158, P ≤ 0.039) but not after adjustments for basic covariates and body composition. These findings indicate that cardiovascular health promotion in childhood may focus on the maintenance of a healthy fat mass.
Similar content being viewed by others


Introduction
Childhood obesity is a global public health challenge, and more than 300 million children have obesity (≥ 100 million) or overweight (≥ 200 million)1. Obesity in childhood is linked to several negative health outcomes later in life including an increased risk of later premature mortality2,3, disability4 and cardiovascular disease (CVD)3,5,6. There is also accumulating evidence that obesity is associated with impaired cardiovascular health already in childhood. For instance, previous studies have reported linear associations of body mass index (BMI) with greater cardiometabolic risk, Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) and Metabolic Syndrome (MetS) scores in children and youth7,8. However, BMI is a relatively poor proxy of body composition especially in childhood9 and cannot differentiate between fat mass and fat-free mass10, which may have different effects on health outcomes11. Although studies have consistently shown positive associations of greater adiposity and fat mass with increased CVD risk factors in children12,13,14,15, few studies have examined the joint associations of accurately measured fat mass and fat-free mass with CVD risk factors. In particular, the associations of fat-free mass with CVD risk factors in children are poorly examined.
Physical fitness and in particular cardiorespiratory fitness has been associated with a more favorable CVD risk profile already in childhood16,17 and there is some evidence that high fitness may attenuate the negative effects of obesity on later cardiovascular health6,18. However, it is not fully examined whether the associations of physical fitness are influenced by accounting for accurately measured body composition (i.e., fat mass and fat-free mass) and vice versa. This is of importance as several studies have shown that body composition and physical fitness (especially when measured as performance in field-tests such as the 20 m shuttle run) are closely related to each other19,20,21,22. Therefore, the aim of this study was to investigate the independent associations of body composition and physical fitness with risk factors for cardiovascular disease (i.e. blood pressure, HOMA-IR and a composite MetS score) in 9-year-old children.
Methods
Study design and participants
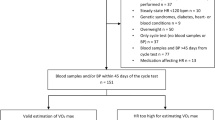
This cross-sectional study used data from the SPINACH (Studies of Prospective health determinants in INfancy And CHildhood) study which utilized follow-up measurements conducted in 9-year-olds that had previously taken part in one of three previous studies: two birth cohorts23,24 and one randomized controlled trial in 4.5-year-old-children25 that all sampled participants from the general population of Östergötland, Sweden. The inclusion criteria for the birth cohorts were a healthy, full-term (born after at least 37 weeks of gestation) singleton infant23,24. The inclusion criteria for the randomized controlled trial was a healthy 4-year-old child that could be measured at 4.5 years of age (± 2 months). Exclusion criteria included if the child was diagnosed with a disease/disorder that would affect body size or feeding and if the parents had a serious physical or psychological disease making the study too demanding for the family25. The follow-up at 9 years of age in these three studies were coordinated and conducted during 2016–2020, and thus included identical measures of body composition, physical fitness and health outcomes. Of the 632 children originally measured in infancy and preschool-age, 411 children participated in the follow-up measurements at 9 years of age and were included in the study.
Participants were also invited to provide a blood sample for the analyses of additional CVD risk factors (i.e. HOMA-IR, components of MetS) and 175 children provided a fasting blood sample. The 175 children who provided a blood sample were fairly comparable to the 236 children that did not, with regard to average BMI (17.0 vs. 16.9 kg/m2), age (9.6 vs. 9.5 years), sex distribution (55.1% vs. 46.6% boys) as well as maternal educational attainment (80.5% vs. 75.0% university degree). Ethical permission was approved by the ethics committees in Linköping (ref no 2016/300-31) and Stockholm (ref no 2018/2220-32) and was conducted in accordance with the Declaration of Helsinki. All parents provided informed written consent.
Body composition
Body composition and anthropometric measures were taken before the physical fitness tests, in accordance with standard procedures, i.e., wearing only underwear and no shoes26. Height was measured using a wall stadiometer (Tillquist, Spånga, Sweden) to the nearest 0.5 cm. Body composition was measured after a 2 h fast using air-displacement plethysmography (BodPod, COSMED USA, Concord, CA, USA), which is a reliable, valid and safe technique for the evaluation of body composition in children26. Briefly, body weight was measured to the nearest gram with an electronic scale attached to the air-displacement plethysmograph (BodPod, COSMED USA, Concord, CA, USA). Subsequently, body volume was measured using the BodPod and body density was calculated as measured weight divided by measured volume. Subsequently, body fatness was calculated utilizing the densities of fat- and fat-free mass according to Lohman’s model27. BMI was calculated as body weight (kg) divided by height (m) squared. Overweight and obesity were classified according to the BMI cut-offs by Cole and Lobstein28. Fat mass index was calculated by dividing fat mass (kg) with height (m) squared (i.e., fat mass/height2), whereas fat-free mass index was calculated as the amount of fat-free mass (kg) divided by height (m) squared (i.e., fat-free mass/height2).
Physical fitness
Physical fitness was measured using the ALPHA health related fitness test-battery29. The ALPHA-battery of tests are considered valid and reliable for evaluation of physical fitness levels in children and adolescents aged 6–18 years and detailed information about the ALPHA battery is available elsewhere29. Cardiorespiratory fitness was assessed using the 20-m shuttle run test29,30 and this was conducted last considering the maximality of the test. The participant started at a pace of 8.5 km/h, increasing with 0.5 km/h each minute of the test while running between two lines 20 m apart and keeping pace with the pre-recorded audio signals. The test continued until the child decided to stop due to fatigue or if the participant failed to run the 20-m distance before the signal was played two consecutive times.
Upper body muscular strength was evaluated using the hand grip strength test with an analogue dynamometer (TKK 5001, Grip-A, Takei, Tokyo, Japan). Hand size of the participant was measured to the nearest 0.5 cm, and the grip span of the dynamometer was adjusted in order to assure the correct setting to acquire maximal hand grip strength31. The participant squeezed the dynamometer with maximal power two times in each hand and the best of two attempts was registered. Thereafter, the average of both hands was calculated and used in the analyses.
Lower body muscular strength was assessed using the best of two attempts of the standing long jump test, where the participant jumped as far as possible with both feet together while remaining upright29. The distance from the start-line to the back of the heel nearest to the starting point was measured.
Motor fitness was evaluated using the 4 × 10 m shuttle run test29. During the test, the child ran as fast as possible between two parallel lines 10 m apart. This test was performed twice with a total distance of 40 m (4 × 10 m) covered each time. Since lower scores (seconds) indicate higher performance, the results were inverted (by multiplying by − 1) in the statistical analyses.
Cardiovascular risk factors
Systolic and diastolic blood pressure were measured in millimeter of mercury (mmHg) with an electric sphygmomanometer (WelchAllyn, ProBP 3400 series, NY, USA). The participants were sitting in an upright resting position and had to rest at least five minutes before the measurement. Two readings of blood pressure were done; if the readings differed by more than 10 mmHg, a third measurement was carried out. The mean value of two or three measures of blood pressure was calculated and used in the analyses.
Children provided fasting venous blood samples which were analyzed for glucose, insulin, total cholesterol, high density lipoprotein cholesterol (HDL cholesterol) and triglycerides as described previously32.
All analyses were conducted at the Department of Clinical Chemistry, Linköping University, Linköping, Sweden, which is accredited for the analyses (ISO/IEC 17025).
To estimate insulin resistance, HOMA-IR was calculated as fasting insulin [µU/L] × fasting glucose [mmol/L])/22.533. Due to the skewed distribution of HOMA-IR, values were transformed with the natural logarithm (ln) in the statistical analyses. A continuous cardiovascular risk score based on the most used definition of the metabolic syndrome (MetS) was used in accordance with previous studies7,32. Since body composition was an independent variable in the analysis, waist circumference was not included in the score. Thus, the MetS score was calculated as the normalized sum of sex-specific z-scores for triglycerides, inverted (by multiplying with − 1) HDL-cholesterol, fasting glucose and the average of systolic and diastolic blood pressure as described previously7,32.
Statistical analyses
Linear regression was utilized in the statistical analyses. First, we examined the associations of body composition and physical fitness using one unadjusted model and one model that was adjusted for the child’s age and sex, maternal educational level and maternal BMI. Additionally, models with fat mass index and fat-free mass index as the independent variable were mutually adjusted for each other. Second, we examined associations of body composition and physical fitness with CVD risk factors and three linear regression models were created: (1) unadjusted model; (2) basic adjusted model including child’s sex and age at measurement, maternal BMI and maternal educational attainment as covariates (models with fat mass index and fat-free mass index as the independent variable were also mutually adjusted for each other); (3) basic adjusted model plus cardiorespiratory fitness and handgrip strength (where body composition was the exposure) or adjusted model plus fat mass index and fat-free mass index (where physical fitness measures were the exposure). Thus, the latter model provides estimates that are mutually adjusted for body composition and cardiorespiratory fitness. Furthermore, we observed no violations against the assumptions of the regression models34. The statistical analyses were conducted using SPSS Statistics (IMB SPSS statistics, version 26, IBM Corp., NY, USA) and P < 0.05 was regarded as statistically significant.
Ethics approval and consent to participate
Ethical permission for all studies in this manuscript was approved by the ethics committees in Linköping (ref no. 2016/300-31) and Stockholm (ref no 2018/2220-32). All parents provided informed written consent before any measurements were conducted.
Results
Descriptive statistics
Table 1 describes the 411 children (200 girls and 211 boys) who participated in this study. They were on average 9.5 years (SD 0.1) old at the time of the measurement with an average height and weight of 139.4 cm (SD 6.1) and 33.2 kg (SD 6.8), respectively. Of the 411 children, 10.9% (22 girls and 23 boys) were classified as having overweight and another 1.9% (4 girls and 4 boys) were classified as having obesity. Maternal age was on average 40.7 years (SD 3.9) and average BMI was 24.6 kg/m2 (SD 4.1, n = 400). The majority of mothers had a university degree (78.1%, n = 321), whereas 21.7% (n = 89) had a high school education and 0.2% (n = 1) had a primary school (9 years) education.
Associations of body composition with physical fitness
Table 2 displays the associations of body composition with physical fitness. Higher BMI and % fat mass were associated with poorer physical fitness in the weight-bearing fitness test (i.e., cardiorespiratory fitness, lower body strength and motor fitness) (all β ≤ − 0.219, all P ≤ 0.001) but with better performance in upper-body muscular strength (i.e., handgrip strength, β ≥ 0.131, all P ≤ 0.008). Fat mass index and fat-free mass index had joint but opposite associations with physical fitness for the weight-bearing fitness tests in the adjusted models. Thus, higher fat mass index was associated with poorer cardiorespiratory fitness, lower body strength and motor fitness (all β ≤ − 0.439, all P ≤ 0.001), whereas a higher fat-free mass index was associated with better performance in the aforementioned physical fitness dimensions (all β ≥ 0.141, all P ≤ 0.005). Both fat mass index and fat-free mass index were positively associated with upper body muscular strength, although associations were considerably stronger for fat mass index as compared with fat-free mass index (β = 0.495 vs. 0.144 in the adjusted model).
Associations of body composition with cardiovascular risk factors
Associations of body composition with cardiovascular risk factors are presented in Table 3. BMI, % fat mass and fat mass index were positively associated with the cardiovascular risk factors (all β ≥ 0.198, all P ≤ 0.002) in all three regression models. Fat-free mass index had weak, but statistically significant associations with systolic blood pressure and MetS score in the unadjusted models (β ≥ 0.170, all P ≤ 0.026) although these associations became weaker in the basic adjusted model (adjusted child’s age and sex, maternal educational attainment and BMI) and not statistically significant (P ≥ 0.27) after further adjustments for physical fitness.
Associations of physical fitness with cardiovascular risk factors
Table 4 presents the associations of physical fitness with cardiovascular risk factors. Higher cardiorespiratory fitness and motor fitness were associated lower HOMA-IR and MetS scores in the unadjusted model (β ≤ − 0.158, P ≤ 0.039). However, estimates were attenuated in the basic adjusted model and were not statistically significant (P ≥ 0.28) in the third model (adjusting for basic covariates plus body composition). Greater upper-body strength was associated with higher systolic and diastolic blood pressure as well as MetS score in the unadjusted model (β ≥ 0.108, all P ≤ 0.030). Although estimates were weakened by adjustments, upper-body strength remained positively associated with systolic blood pressure β = 0.129, all P = 0.029) after adjustments for basic covariates and body composition. Lower body strength was inversely associated with HOMA-IR in all three regression models (β ≤ − 0.160, all P ≤ 0.047) although associations were attenuated by adjustments.
Sensitivity analyses
Although data collection at the 9-year follow-up, which is the focus of this paper, was carefully standardized, children were originally from three previous studies. Hence, we re-analyzed the associations of body composition and physical fitness with the MetS score only using data from MINISTOP25, which is the largest individual study (Tables S1 and S2). We also re-analyzed the data using only data from the two birth cohort studies (Tables S1 and S2). As shown in the tables, associations were generally very comparable in terms of direction and magnitude when analyzing all participants or participants from MINISTOP or the birth cohorts separately. Furthermore, since it has been suggested that normalizing body mass and composition (i.e., fat and fat-free mass) with height squared (i.e., the calculation of BMI, fat mass index and fat-free mass index) may not be sufficient in children15, we performed an additional analysis where height was added in the final model. As shown in Table S3, this adjustment had minor influence on the estimates, and results remained virtually the same. Finally, we also examined the influence of expressing cardiorespiratory fitness in estimated VO2-max using the equation by Léger et al.30 as shown in Table S4. However, estimates were very comparable to our main analysis, i.e., cardiorespiratory fitness was inversely associated with HOMA-IR and the MetS score but associations were attenuated by adjustments for covariates and body composition.
Discussion
Principal findings
This study comprehensively examined associations of body composition and physical fitness with CVD risk factors in 9-year-old children and reports several findings of interest. First, body composition and physical fitness were strongly associated, which highlight the need of mutual adjustments when examining the independent associations of body composition and physical fitness with CVD risk factors. Second, accurately measured fat mass and fat mass index were strongly and positively associated with CVD risk factors also after adjustments for covariates including physical fitness. Third, accurately measured fat-free mass index had generally weak associations with CVD risk factors that were attenuated after adjustments. Finally, greater cardiorespiratory fitness and motor fitness were associated with lower HOMA-IR and MetS score, although associations were strongly attenuated by the adjustments for other covariates including body composition (fat mass index and fat-free mass index).
Body composition
We found that body composition was strongly associated with physical fitness which extends our previous findings in preschool aged children19 and previous studies in children that have not examined the combined association of fat mass and fat-free mass on physical fitness. Previous studies have consistently reported that greater fat mass is strongly associated with CVD risk factors such as higher blood pressure, LDL cholesterol, triglycerides and insulin values as well as lower HDL cholesterol12,13,14,15. Our results confirm these findings and also report that the associations of BMI, % fat mass and fat mass index were quite unaffected by adjustments for covariates including physical fitness and fat-free mass index (only the model with fat mass index). There are many mechanisms by which obesity may increase the prevalence of CVD risk factors or actual CVD events35,36. For instance, impaired adipogenesis, altered fat deposition, inflammatory and adipokine dysregulation, adipose tissue hypoxia, increased circulating free fatty acids, oxidative stress and lipotoxicity have been suggested as relevant pathways35. Furthermore, excess body fatness is closely connected with insulin resistance which in turn is related with dyslipidemia (i.e., high levels of triglycerides and low levels of HDL cholesterol)36. Finally, obesity induce adaptations in the cardiac system including increased cardiac output and systemic vascular resistance which elevate the blood pressure37.
Relatively few studies have examined associations between fat-free mass with CVD risk factors in children. Grijalva-Eternod et al.38 reported that higher fat-free mass normalized for height was associated with higher systolic, but not diastolic blood pressure, which agree with our findings in the unadjusted and adjusted models. Interestingly, associations were attenuated and not statistically significant after accounting for physical fitness (i.e., cardiorespiratory fitness and handgrip strength) in our analyses. Another study reported no associations with fat-free mass and insulin resistance in 7–9-year-old children although a positive association was observed in girls only after the age of 1015 which may be reconciled with our findings. Thus, based on our and the previous studies15,38,39, fat-free mass appears not to have any beneficial association with CVD risk factors.
Physical fitness
Greater cardiorespiratory fitness and motor fitness in our unadjusted analyses were associated with lower HOMA-IR and MetS score which generally agrees well with previous studies of fitness and CVD risk factors40,41,42,43,44,45,46. However, previous studies have generally shown that the associations of cardiorespiratory fitness with CVD risk factors are strongly attenuated by adjustments for BMI or body fatness, both in studies that have used laboratory47,48 or field measures44,45,46 of cardiorespiratory fitness. Data from this and previous studies 19,20,22 have shown that performance in the 20 m shuttle run is strongly and inversely associated with body fatness in children. Given the close relationship between cardiorespiratory fitness and body fatness, it is possible that the unadjusted and statistically significant associations of cardiorespiratory and motor fitness with lower HOMA-IR and MetS are due to differences in body composition (and especially a higher fat mass). This would explain why these estimates are no longer statistically significant in the models that accounted for fat mass and fat-free mass and highlight the importance of considering body composition when examining associations of physical fitness and health outcomes. Although cardiorespiratory and motor fitness are regarded as markers of health49,50, it is important to consider that associations between fitness and health outcomes may, at least partly, be due to other factors such as body fatness.
We observed that upper body strength and lower body strength in some cases had opposite associations with the measured CVD risk factors. For instance, greater upper body strength was associated with higher systolic blood pressure and MetS score, whereas greater lower body strength was associated with lower HOMA-IR and MetS score. These results may be reconciled with previous studies of muscular strength and CVD risk factors in youth. Such studies have generally reported positive or null associations with handgrip strength46,51,52 and inverse or null associations with standing long jump46,51,52 in analyses that did not account for body composition or fatness. As shown in Table 2, associations between fat mass and upper body and lower body strength differed, which may be due to the nature of the fitness tests (weight bearing or not). Although greater fat-free mass was associated with better performance in both tests, greater fat mass was associated with better performance in the handgrip strength (non-weight bearing), but with poorer performance in the standing long jump (weight bearing). Considering the strong associations of fat mass with CVD risk factors, this difference may at least partly account for the difference in associations between strength and CVD risk factors. Indeed, when additionally adjusting for fat mass and fat-free mass, associations were generally strongly attenuated, although handgrip strength remained positively associated with systolic blood pressure and lower body strength inversely associated with HOMA-IR. Thus, future studies should consider adjustments for body composition to elucidate the independent associations of physical fitness with CVD risk factors.
Strengths and limitations
A major strength of this study was the relatively large sample of children (n = 411) that were measured using accurate body composition methodology (air-displacement plethysmography)26. Furthermore, we were able to analyze the joint associations of body composition (fat mass and fat-free mass) and physical fitness with CVD risk factors. Another strength is that children were measured at 9.5 years of age within a narrow time frame (SD 0.1 years).
The current study also has some limitations that needs to be considered. First, the cross-sectional study design limits interferences regarding the casualty of the examined associations. Moreover, the high proportion of mothers with a university degree may influence generalizability of the results. However, maternal educational attainment was accounted for in the analyses and had little influence on the estimates. Furthermore, we lacked data regarding pubertal status in the analyses which is a limitation. According to a large Danish study53, less than 2% of boys and girls had reached Tanner stage 2 at 9.5 years of age and virtually no one had reached stage 3, 4 or 5 at that time point. Thus, we consider it likely that the effects of puberty have limited influence on our estimates, although further studies should consider accounting for pubertal status in the analysis.
Implications
The findings of our study have some implications that may be of importance for the promotion of cardiovascular health in children. First, our findings showed that fat mass index and fat-free mass index have generally independent but opposite associations with physical fitness, which indicate that analyses that include both body composition and physical fitness variables should be mutually adjusted for each other. Second, BMI was generally as strongly associated to CVD risk factors as accurately measured fat mass, which indicate that more advanced body composition measurements (e.g., air-displacement plethysmography) may not convey cardiovascular health better than BMI, which is easily measured. Third, fat-free mass had no beneficial associations with CVD risk factors which provides support that cardiovascular health promotion in childhood should focus on the maintenance of a healthy fat mass. Finally, higher cardiorespiratory fitness and motor fitness were associated with lower HOMA-IR and MetS score. However, associations were strongly attenuated by accounting for body composition (fat mass and fat-free mass). Nevertheless, evidence from longitudinal studies in childhood and adolescence suggest that greater cardiorespiratory fitness, independent of BMI, is associated with better cardiovascular outcomes later in life2,6,18,54. Thus, further studies are needed to elucidate the independent influence of physical fitness on cardiovascular health in childhood and adolescence.
Conclusion
In conclusion, greater BMI and fat mass was associated with CVD risk factors even after adjustments for covariates and physical fitness. Importantly, associations with BMI were generally as strong as with accurately measured fat mass which may have implication given the easy measurement of BMI in children. However, fat-free mass did not have any beneficial associations with CVD risk factors which support the notion that the focus for cardiovascular health promotion during childhood could be on excess fat mass and not on the fat-free mass. Finally, higher cardiorespiratory and motor fitness were associated with lower HOMA-IR and MetS score although associations were strongly attenuated by adjusting the estimates for body composition (fat mass and fat-free mass).
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
References
GBD 2015 Obesity Collaborators et al. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 377, 13–27 (2017).
Crump, C., Sundquist, J., Winkleby, M. A. & Sundquist, K. Interactive effects of physical fitness and body mass index on the risk of hypertension. JAMA Intern. Med. 176, 210–216 (2016).
Twig, G. et al. Body-mass index in 2.3 million adolescents and cardiovascular death in adulthood. N. Engl J. Med. 374, 2430–2440 (2016).
Henriksson, P. et al. Fitness and body mass index during adolescence and disability later in life: A cohort study. Ann. Intern. Med. 170, 230–239 (2019).
Falkstedt, D., Hemmingsson, T., Rasmussen, F. & Lundberg, I. Body mass index in late adolescence and its association with coronary heart disease and stroke in middle age among Swedish men. Int. J. Obes. (Lond). 31, 777–783 (2007).
Henriksson, H. et al. Cardiorespiratory fitness, muscular strength, and obesity in adolescence and later chronic disability due to cardiovascular disease: A cohort study of 1 million men. Eur. Heart J. 41, 1503–1510 (2020).
Nystrom, C. D. et al. Does cardiorespiratory fitness attenuate the adverse effects of severe/morbid obesity on cardiometabolic risk and insulin resistance in children? A pooled analysis. Diabetes Care 40, 1580–1587 (2017).
Skinner, A. C., Perrin, E. M., Moss, L. A. & Skelton, J. A. Cardiometabolic risks and severity of obesity in children and young adults. N. Engl. J. Med. 373, 1307–1317 (2015).
Freedman, D. S. et al. Relation of BMI to fat and fat-free mass among children and adolescents. Int. J. Obes. (Lond). 29, 1–8 (2005).
Kyle, U. G., Schutz, Y., Dupertuis, Y. M. & Pichard, C. Body composition interpretation. Contributions of the fat-free mass index and the body fat mass index. Nutrition 19, 597–604 (2003).
Bigaard, J. et al. Body fat and fat-free mass and all-cause mortality. Obes. Res. 12, 1042–1049 (2004).
Cui, Z., Truesdale, K. P., Cai, J., Koontz, M. B. & Stevens, J. Anthropometric indices as measures of body fat assessed by DXA in relation to cardiovascular risk factors in children and adolescents: NHANES 1999–2004. Int. J. Body Compos. Res. 11, 85–96 (2013).
Lawlor, D. A. et al. Association between general and central adiposity in childhood, and change in these, with cardiovascular risk factors in adolescence: Prospective cohort study. BMJ. 341, c6224 (2010).
Steinberger, J. et al. Comparison of body fatness measurements by BMI and skinfolds vs dual energy X-ray absorptiometry and their relation to cardiovascular risk factors in adolescents. Int. J. Obes. (Lond). 29, 1346–1352 (2005).
Wells, J. C. & Cole, T. J. Height, adiposity and hormonal cardiovascular risk markers in childhood: How to partition the associations?. Int. J. Obes. (Lond). 38, 930–935 (2014).
Lang, J. J. et al. Systematic review of the relationship between 20m shuttle run performance and health indicators among children and youth. J. Sci. Med. Sport. 21, 383–397 (2018).
Ruiz, J. R. et al. Cardiorespiratory fitness cut points to avoid cardiovascular disease risk in children and adolescents; what level of fitness should raise a red flag? A systematic review and meta-analysis. Br. J. Sports Med. 50, 1451–1458 (2016).
Hogstrom, G., Nordstrom, A. & Nordstrom, P. Aerobic fitness in late adolescence and the risk of early death: A prospective cohort study of 1.3 million Swedish men. Int. J. Epidemiol. 45, 1159–1168 (2016).
Henriksson, P. et al. Associations of fat mass and fat-free mass with physical fitness in 4-year-old children: results from the MINISTOP trial. Nutrients. https://doi.org/10.3390/nu8080473 (2016).
Joensuu, L. et al. Objectively measured physical activity, body composition and physical fitness: Cross-sectional associations in 9- to 15-year-old children. Eur. J. Sport Sci. 18, 882–892 (2018).
Moliner-Urdiales, D. et al. Associations of muscular and cardiorespiratory fitness with total and central body fat in adolescents: the HELENA study. Br. J. Sports Med. 45, 101–108 (2011).
Welsman, J. & Armstrong, N. The 20 m shuttle run is not a valid test of cardiorespiratory fitness in boys aged 11–14 years. BMJ Open Sport Exerc. Med. 5, e000627. https://doi.org/10.1136/bmjsem-2019-000627 (2019).
Eriksson, B., Lof, M. & Forsum, E. Body composition in full-term healthy infants measured with air displacement plethysmography at 1 and 12 weeks of age. Acta Paediatr. 99, 563–568 (2010).
Henriksson, P., Lof, M. & Forsum, E. Parental fat-free mass is related to the fat-free mass of infants and maternal fat mass is related to the fat mass of infant girls. Acta Paediatr. 104, 491–497 (2015).
Nystrom, C. D. et al. Mobile-based intervention intended to stop obesity in preschool-aged children: The MINISTOP randomized controlled trial. Am. J. Clin. Nutr. 105, 1327–1335 (2017).
Fields, D. A., Goran, M. I. & McCrory, M. A. Body-composition assessment via air-displacement plethysmography in adults and children: A review. Am. J. Clin. Nutr. 75, 453–467 (2002).
Lohman, T. G. Assessment of body composition in children. Pediatr. Exerc. Sci. 1, 19–30 (1989).
Cole, T. J. & Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes. 7, 284–294 (2012).
Ruiz, J. R. et al. Field-based fitness assessment in young people: The ALPHA health-related fitness test battery for children and adolescents. Br. J. Sports Med. 45, 518–524 (2011).
Leger, L. A., Mercier, D., Gadoury, C. & Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 6, 93–101 (1988).
Espana-Romero, V. et al. Hand span influences optimal grip span in boys and girls aged 6 to 12 years. J. Hand Surg. Am. 33, 378–384 (2008).
Henriksson, P. et al. Associations of body composition and physical fitness with gestational diabetes and cardiovascular health in pregnancy: Results from the HealthyMoms trial. Nutr. Diabetes. 11, 16 (2021).
Matthews, D. R. et al. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28, 412–419 (1985).
Kleinbaum, D. G., Kupper, L. L., Nizam, A. & Muller, K. E. Applied regression analysis and other multivariable methods (Thomson, Belmont, 2008).
Neeland, I. J., Poirier, P. & Despres, J. P. Cardiovascular and metabolic heterogeneity of obesity: Clinical challenges and implications for management. Circulation 137, 1391–1406 (2018).
Powell-Wiley, T. M. et al. Obesity and cardiovascular disease: A scientific statement from the american heart association. Circulation 143, e984–e1010 (2021).
Koliaki, C., Liatis, S. & Kokkinos, A. Obesity and cardiovascular disease: Revisiting an old relationship. Metabolism 92, 98–107 (2019).
Grijalva-Eternod, C. S., Lawlor, D. A. & Wells, J. C. Testing a capacity-load model for hypertension: Disentangling early and late growth effects on childhood blood pressure in a prospective birth cohort. PLoS ONE 8, e56078. https://doi.org/10.1371/journal.pone.0056078 (2013).
Perreault, K., Lagace, J. C., Brochu, M. & Dionne, I. J. Association between fat free mass and glucose homeostasis: Common knowledge revisited. Ageing Res Rev. 28, 46–61 (2016).
Andersen, L. B. et al. A new approach to define and diagnose cardiometabolic disorder in children. J. Diabetes Res. 2015, 539835 (2015).
Andersen, L. B. et al. Fitness, fatness and clustering of cardiovascular risk factors in children from Denmark, Estonia and Portugal: The European Youth Heart Study. Int. J. Pediatr. Obes. 3(Suppl 1), 58–66 (2008).
Artero, E. G. et al. Muscular and cardiorespiratory fitness are independently associated with metabolic risk in adolescents: The HELENA study. Pediatr. Diabetes. 12, 704–712 (2011).
Dencker, M. et al. Aerobic fitness related to cardiovascular risk factors in young children. Eur. J. Pediatr. 171, 705–710 (2012).
Klakk, H. et al. Prospective association of adiposity and cardiorespiratory fitness with cardiovascular risk factors in healthy children. Scand. J. Med. Sci. Sports. 24, e275-282 (2014).
Perez-Bey, A. et al. The influence of cardiorespiratory fitness on clustered cardiovascular disease risk factors and the mediator role of body mass index in youth: The UP&DOWN Study. Pediatr. Diabetes. 20, 32–40 (2019).
Zaqout, M. et al. Influence of physical fitness on cardio-metabolic risk factors in European children. The IDEFICS study. Int. J. Obes. (Lond) 40, 1119–1125 (2016).
Ball, G. D. et al. Insulin sensitivity, cardiorespiratory fitness, and physical activity in overweight Hispanic youth. Obes Res. 12, 77–85 (2004).
Shaibi, G. Q. et al. Cardiovascular fitness and the metabolic syndrome in overweight latino youths. Med. Sci. Sports Exerc. 37, 922–928 (2005).
Ortega, F. B., Ruiz, J. R., Castillo, M. J. & Sjostrom, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. (Lond). 32, 1–11 (2008).
Raghuveer, G. et al. Cardiorespiratory fitness in youth: An important marker of health: a scientific statement from the American Heart Association. Circulation 142, e101–e118 (2020).
Jimenez-Pavon, D. et al. Muscular strength and markers of insulin resistance in European adolescents: The HELENA Study. Eur. J. Appl. Physiol. 112, 2455–2465 (2012).
Magnussen, C. G., Schmidt, M. D., Dwyer, T. & Venn, A. Muscular fitness and clustered cardiovascular disease risk in Australian youth. Eur. J. Appl. Physiol. 112, 3167–3171 (2012).
Brix, N. et al. Timing of puberty in boys and girls: A population-based study. Paediatr. Perinat. Epidemiol. 33, 70–78 (2019).
Hogstrom, G., Nordstrom, A. & Nordstrom, P. High aerobic fitness in late adolescence is associated with a reduced risk of myocardial infarction later in life: A nationwide cohort study in men. Eur. Heart J. 35, 3133–3140 (2014).
Acknowledgements
The authors gratefully thank the participating children and families in the study. The authors also would like to thank Eva Flinke, Emmie Söderström, Martina Johansson and Ellinor Nilsson for their assistance with the data collection.
Funding
Open access funding provided by Linköping University. Bo and Vera Ax: Son Johnson’s Foundation (ML).
Author information
Authors and Affiliations
Contributions
M.L. is the principal investigator of the SPINACH study with an overall responsibility for the study design and execution. P.H. conceptualized and designed the current analysis together with M.L. and J.S. J.S., M.H. and C.D.N. were responsible for the recruitment and data collection. P.H. analyzed the data and J.S., M.H., C.D.N., E.E., F.B.O. and M.L. contributed to interpretation of data for the work. P.H. drafted the manuscript which was critically revised by J.S., M.H., C.D.N., E.E., F.B.O. and M.L. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Henriksson, P., Sandborg, J., Henström, M. et al. Body composition, physical fitness and cardiovascular risk factors in 9-year-old children. Sci Rep 12, 2665 (2022). https://doi.org/10.1038/s41598-022-06578-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-06578-w
This article is cited by
-
Secular trends in physical fitness of rural Chinese children and adolescents aged 7–18 years from 1985 to 2019
Scientific Reports (2023)
-
Relationships of BMI, muscle-to-fat ratio, and handgrip strength-to-BMI ratio to physical fitness in Spanish children and adolescents
European Journal of Pediatrics (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
