
Abstract
The results of human studies are inconsistent regarding selenium and depressive disorders. Therefore, we aimed to conduct a systematic review and meta-analysis of observational and interventional studies and provided an overview of the role of selenium in depression. Three databases including Medline, Scopus, and Web of Science were searched on June 30, 2020 and updated on April 12, 2021. Also, we searched in electronical databases of WHO Global Index Medicus and ClinicalTrials.gov. No time or language restrictions were used for the search. A random effects model was used to pool effect sizes. In total, 20 studies were included in the systematic review, and 15 studies were included in the meta-analysis. There were no significant differences in serum selenium levels between patients with depression and healthy subjects (WMD: 2.12 mg/L; 95% CI: − 0.11, 4.36; I2 = 98.0%, P < 0.001). Also, no significant correlation was found between serum levels of selenium and depression scores (r: − 0.12; 95% CI: − 0.33, 0.08; I2 = 73.5%, P = 0.010). Nevertheless, there was a significant negative association between high selenium intake and the risk of postpartum depression (OR: 0.97; 95% CI: 0.95, 0.99; I2 = 0.0%, P = 0.507). In addition, selenium supplementation significantly reduced depressive symptoms (WMD: − 0.37; 95% CI: − 0.56, − 0.18; I2 = 0.0%, P = 0.959). Taken these results together, selenium seems to have a protective role against postpartum depression and can be considered as a beneficial adjuvant therapy in patients with depression. Further studies are necessary to draw definitive conclusions.
Similar content being viewed by others


Introduction
Depression is identified as a disabling mental illness, which can substantially impair quality of life1,2. According to the report of World Health Organization in 2018, more than 264 million people are affected by depression worldwide3. The rate of depression dramatically increased from 172 to 258 million since 1990 to 2017, showing a 50% increase4. Patients with depression may experience fatigue, sleep disturbance, loss of memory and concentration, poor appetite, loss of work motivation, and low self-confidence during their lives5,6. Also, untreated depression can lead to serious social problems and even suicide7.
It appears that nutrition plays a critical role in mental health8. For instance, several studies have supported the favorable effects of magnesium, vitamin D, B-vitamins, and omega-3 fatty acids on mood disorders9. Moreover, recent evidence has revealed the benefits of using trace elements in the prevention and treatment of depression10. Among trace elements, selenium may be of great importance in the management of depression due to its antioxidant, anti-inflammatory, immunomodulatory, and neuroprotective properties11,12. In addition to depression, selenium deficiency may be associated with many other diseases such as type 2 diabetes mellitus, cardiovascular disease, kidney diseases, infertility, and cognitive decline13,14.
The results of observational and interventional studies are inconsistent regarding the role of selenium in depression15,16,17,18,19,20,21,22. Several studies reported a significant negative relationship between dietary or serum levels of selenium and the risk of depression15,16,17. In contrast, some studies did not find such a relationship18,19. Even, a narrative review generally reported that there is an unclear relationship between selenium and depression23. Furthermore, selenium supplementation showed a positive effect on depression symptoms in some clinical trials20,21 but a neutral effect in others22. Since no comprehensive review article has yet been published on this controversial topic, we aimed to conduct a systematic review and meta-analysis of human observational and interventional studies and provide an overview of the role of selenium in depressive disorders.
Methods
Search strategy
This study was conducted according to the guidelines of Meta-Analysis of Observational Studies in Epidemiology (MOOSE) for observational studies24 and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) for interventional studies25. A systematic electronic search was performed to identify all publications on selenium and depression. Three databases including Medline (via PubMed), Scopus, and Web of Science were searched on June 30, 2020 and updated on April 12, 2021. Also, we searched in electronical databases of WHO Global Index Medicus and ClinicalTrials.gov. No time or language restrictions were used for the search. The following Medical Subject Headings (MeSH) and non-MeSH terms were used to identify potential studies: (“depression” OR “depressions” OR “depressive disorder” OR “depressive disorders” OR “depressive” OR “depressed”) AND (“selenium” OR “selenite” OR “selenite” OR “seleno” OR “Se”).
Eligibility criteria
The retrieved articles were included in the present study if they met the following criteria: (1) had an observational (cross-sectional, case–control, and cohort) or an interventional (randomized controlled trial) design, (2) conducted on humans, (3) investigated the association between dietary or supplementary intake or serum levels of selenium and depression, (4) compared dietary or supplementary intake or serum levels of selenium between patients with depression and healthy controls, and (5) assessed the effect of selenium supplementation or selenium rich diet on depression. The exclusion criteria were: (1) reviews, books, case reports, conference papers, letters to the editor, and animal or in vitro studies, (2) studies which failed to assess selenium, (3) studies which administered selenium in combination with other components, (4) studies which measured nail or hair selenium, and (5) studies reported duplicate data, (6) studies which assessed other outcomes other than depression, (7) protocol study, and (8) studies which failed to assess the association between selenium and depression.
Data extraction and quality assessment
The following characteristics were collected from the included publications: the first author’s last name, year of publication, country where the study was conducted, sample size, gender and mean or median age of participants, study design, type of depressive disorder, assessment tool of depression, adjusted covariates, main results, values of selenium intake or levels of serum or plasma selenium, serum selenium values at baseline and after-treatment, methodologies of selenium measurement. The quality assessment of observational studies was performed using the Newcastle–Ottawa Scale (NOS)26, and the quality of interventional studies was evaluated using the Cochrane Collaboration Risk of Bias Tool (CCRBT)27.
Data synthesis and analysis
To improve normal distribution, correlation coefficients between serum selenium levels and depression scores were converted to z-values using Fisher's r-to-z transformation. Subsequently, following formula was used to converted back to r-values when effect sizes were calculated: ES (z) = ½ ln [(1 + r)/(1 − r)]28. We converted standard errors (SE) to standard deviations (SD) using the formula SD = SE × √N. To calculate SD from 95% confidence interval, following formula was used: SD = √N × (upper limit − lower limit) ÷ 3.92. A random-effects model was used to calculate pooled effect size to compare serum selenium levels between depressive patients and healthy controls29. We used the random-effects model because inter-study heterogeneity was high. The random-effects model should be used for pooling heterogeneous studies30. Similar method was applied to compare change in depression scores between selenium supplementation and control groups. Since included clinical trials used different tools to assess depression score, pooled effect was calculated via Hedges' g31. Log-transformed odds ratios of depression across different categories of selenium intake were also applied to calculate overall effect sizes. Overall effect sizes were reported as odds ratio (OR), weighted mean difference (WMD) and correlation coefficient (r). I‐squared (I2) statistic was reported as an indicator of between-study heterogeneity. To detect the potential sources of heterogeneity, a subgroup analysis was applied when a significant between-study heterogeneity was observed. Sensitivity analysis was performed as a complementary analysis to assess robustness of results. Begg's rank correlation test and Egger's linear regression test were used to test publication bias. The potential effect of publication bias was assessed using trim-and-fill analysis. All statistical analyses were performed using Stata software (version 11.2, Stata Corporation, College Station, Texas, USA); additionally, analyses were two-tailed, and statistical significance was set at P < 0.05.
Results
Study selection process
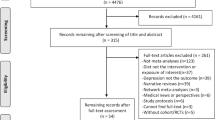
Initially, 1794 published articles were identified from the electronic databases (Fig. 1). After removing 495 duplicates, 1299 records were assessed for eligibility, and 1214 studies were excluded based on screening title and abstract (unrelated studies (n = 853), evaluation other outcomes other than depression (n = 37), selenium intake/concentration was not reported (n = 21), animal studies (n = 235), in vitro studies (n = 37), review articles (n = 27) and protocol studies (n = 4). After screening full-text of the records, 65 studies were excluded due to the following reasons: review articles (n = 20), letters to the editor (n = 8), books and case reports (n = 3), failure to assess selenium (n = 2), administration of selenium in combination with other components (n = 8), unrelated data (n = 12), measurement of nail selenium levels (n = 1), conference papers (n = 1), evaluation other outcomes other than depression (n = 2), measurement of hair selenium levels (n = 1) full text of articles were not available at databases or journal website (n = 2) and the association between selenium and depression was not assessed (n = 5). Finally, 20 studies15,16,17,18,19,20,21,22,32,33,34,35,36,37,38,39,40,41,42,43were included in the systematic review.

Flow diagram of the study selection process.
Systematic review
Characteristics of studies eligible for the systematic review are summarized in Table 1. These studies were published between 2003 and 2020. Among twenty studies, two were conducted in New Zealand15,34, four in Iran16,18,20,41, three in the US22,37,38, one in the UK21, three in Spain17,35,36, one in Bangladesh40, one in Canada33, one in Australia43, one in Pakistan39, one in Poland19, one study in Columbia42, and one study in.
Malaysia32. Four studies were randomized controlled trials20,21,22,36, nine studies used a cross-sectional design15,18,19,32,35,37,38,41,42, four were case–control studies16,39,40,43, and design of three studies were prospective cohort17,33,34. In total, 47,164 participants were enrolled in this systematic review. The age of participants ranged from 18.0 ± 1.2 to 82 years old. Twelve studies included both men and women15,17,18,22,32,35,36,37,38,39,40,41, one study did not report the gender of participants21, and seven studies enrolled women only16,19,20,33,34,42,43. Confounding variables were adjusted in half of included studies15,16,17,18,35,37,38,41,42,43. Serum selenium concentrations were measured in four cross-sectionals15,18,19,38, two case-controls39,40, and one prospective cohort34. Selenium intake levels were used in two case-controls16,43, six cross-sectionals32,35,37,38,41,42, and two prospective cohort studies17,33. Only nine studies specified the type of depression including postpartum depression (n = 4)16,20,33,34, major depressive disorder (n = 3)36,40,43, pregnant depression (n = 1)42, and postmenopausal depression (n = 1)19. The Beck Depression Inventory18,19,22,35,36,41 as well as Edinburgh Postnatal Depression Scale16,20,33,34 were the mostly used depression assessment tools in the included studies. Serum concentration, dietary or supplementary intake of selenium, and method used to measure dietary/serum selenium are reported in Supplementary Table 1. Five studies used 24-h dietary recalls to evaluate dietary or supplementary selenium intakes32,37,38,41,42. On the other hand, five studies used food-frequency questionnaires, 48-h weighted food records or a supplement intake questionnaire16,17,33,35,43. Most studies reported mean and median dietary or supplementary intake of selenium. One study reported dietary selenium as quintiles38. Serum concentration of selenium was reported as mean, median or tertile.
Two cross-sectional studies found no significant correlation between selenium intake and depressive symptoms32,42, whereas in one of the studies, there was a significant inverse correlation between selenium intake and depressive symptoms in males32. Also, two cross-sectional studies found no significant correlation between serum selenium and depression scores18,19. In addition, one cross-sectional study revealed a negative association between serum selenium levels and the risk of depression15. Furthermore, two case–control studies reported lower levels of selenium in depressive subjects compared to healthy controls39,40. Moreover, three cross-sectionals37,38,41, two case-controls16,43, and two cohorts17,33 reported a significant negative association between selenium intake and the risk of depression.
Two randomized controlled trials reported correlation coefficients. They found a significant inverse relationship between serum selenium levels and depression symptoms21,36. All interventional studies used selenium supplements except for one study that assessed the effect of selenium rich diet on depression symptoms36. The dose of selenium supplementation was varied from 100 to 200 μg20,21,22. A beneficial effect of selenium on depressive symptoms was reported in three studies20,21,36. However, one clinical trial found no significant effect of selenium on depression scores22.
Quality assessment of studies
The results of the CCRBT showed that all included randomized controlled trials had high quality (Table 2). According to the NOS, all case–control and prospective cohort studies obtained ≤ 4 stars, i.e., low quality scores (Tables 3, 4). Similarly, the quality of all cross-sectional studies was low except for Ghimire38 and Li37 that respectively received good and excellent quality (Table 5).
Meta-analysis
From 20 studies included in systematic review, five studies were not selected for meta-analysis15,32,34,35,42. Two studies not included to meta-analysis reported the correlation coefficient between dietary intake of selenium and depression32,42. We could not pool these two studies because the score of depression was derived from different depression assessment instruments. One study was not included to meta-analysis because it reported median depression score across tertiles of plasma selenium concentration34. A reported selenium intake across tertiles of mood thermometer35. Since similar report was not found in other studies, we did not include this study to meta-analysis. Another study not selected for meta-analysis reported regression coefficient15. Therefore, a quantitative analysis was performed on 15 studies including 45,795 participants16,17,18,19,20,21,22,33,36,37,38,39,40,41,43.
Correlation between serum selenium levels and depression scores was assessed in four studies. The meta-analysis showed no significant correlation between serum levels of selenium and depression scores (r: − 0.12; 95% CI: − 0.33, 0.08) (Fig. 2). Although a significant between-study heterogeneity was found (I2 = 73.5%, P = 0.010), we could not run a subgroup analysis due to the insufficient number of studies. Moreover, there was an evidence of significant publication bias using Egger's (P = 0.029) and Begg's (P = 0.042) tests. Notwithstanding, trim-and-fill analysis indicated that no trimming could be performed and the data remained unchanged.

Forest plot of the correlation between serum selenium levels and depression scores.
Comparison of serum selenium levels between depressive patients and healthy controls was reported in two studies. As shown in Fig. 3, the pooled results revealed that there were no significant differences in serum selenium concentrations between patients with depression and healthy subjects (WMD: 2.12 mg/L; 95% CI: − 0.11, 4.36). There was a significant heterogeneity between studies (I2 = 98.0%, P < 0.001). However, we could not run a subgroup analysis because of the insufficient number of studies. Moreover, the result did not show any evidence of publication bias using Begg's test (P = 0.31). Egger's test was not run for this section due to the insufficient number of studies.

Forest plot of the comparison of serum selenium levels between depressive patients and healthy controls.
Association between selenium intake and the risk of depression was reported in seven studies. The pooled risk of depression in the highest compared with the lowest categories of selenium intake was 0.98 with 95% CI of 0.93 to 1.04. A significantly high heterogeneity was observed between studies (I2 = 82.7%, P < 0.001). Therefore, we subgrouped studies based on the type of depression (postpartum or other types of depression) (Fig. 4). There was a significant association between selenium intake and the risk of postpartum depression (OR: 0.97; 95% CI: 0.95, 0.99; I2 = 0.0%, P = 0.507). Nevertheless, no significant association was found between selenium intake and the risk of other types of depression (OR: 1.06; 95% CI: 0.75, 1.50; I2 = 85.6%, P < 0.001). Between-subgroup heterogeneity was also high for the type of depression (P = 0.012). Moreover, we did not find any evidence of publication bias using Egger's (P = 0.65) and Begg's (P = 0.80) tests.

Forest plot of the association between selenium intake and the risk ratio of depression stratified by the type of depression.
The Effect of selenium supplementation on depression scores was examined in three studies. The effect of supplementation with selenium on depression scores is shown in Fig. 5. The meta-analysis indicated a significant reduction in depression symptoms following selenium supplementation compared with placebo (WMD: − 0.37; 95% CI: − 0.56, − 0.18). There was no significant heterogeneity between studies (I2 = 0.0%, P = 0.959). Moreover, no evidence of publication bias was found using Egger's (P = 0.11) and Begg's (P = 0.12) tests.

Forest plot of the effect of selenium supplementation on depression scores.
Sensitivity analysis
The sequential exclusion of each study from the pooled analysis did not significantly change the overall effect sizes except for the correlation between serum selenium concentrations and depression scores. This was significantly altered by excluding the study of Ekramzadeh et al. (r: − 0.20; 95% CI: − 0.381, − 0.031). In addition, the sequential removal of each study from the pooled analysis did not eliminate the heterogeneity except for the association between selenium intake and the relative risk of depression.
Discussion
This meta-analysis revealed that there was no significant correlation between serum selenium levels and depression scores. In addition, no significant differences were observed between depressive and healthy subjects in serum selenium concentrations. In contrast, a significant inverse association was found between selenium intake and the risk of postpartum depression. Moreover, the meta-analysis of randomized controlled trials indicated a significant reduction in depression symptoms after selenium supplementation compared with placebo. To the best of our knowledge, the present study is the first systematic review and meta-analysis of human observational and interventional studies that comprehensively investigated the role of selenium in depressive disorders. Prior to this study, three systematic reviews suggested that nutrients such as selenium may be protective against postpartum depression. Nevertheless, these studies only focused on perinatal depression, not other types of depression. Moreover, they did not run a meta-analysis44,45,46.
The findings of this meta-analysis did not show any significant correlation between serum selenium concentrations and depression scores. In contrast, one study reported that there was a significant direct association between high dietary selenium intake and mood improvement47. According to the previous studies, serum selenium levels could not estimate the absolute intake of selenium48. In fact, some factors including demographic variables and health status may influence serum selenium concentrations15. Among the studies included in the present meta-analysis, confounding variables were adjusted in only one study18. Moreover, it seems that brain function is impaired by long-term (not short-term) exposure to low serum selenium levels49. In spite of this fact, the included studies reported no data regarding the duration of selenium deficiency. These reasons may explain the non-significant association between serum selenium and depression symptoms in our meta-analysis. Nevertheless, it is noteworthy that removal of the study by Ekramzadeh et al. significantly changed this result and brought about a significant negative correlation between serum concentrations of selenium and depression scores. Ekramzadeh et al. investigated the relationship of serum selenium with depression in hemodialysis subjects. They measured serum levels of selenium before the beginning of the hemodialysis session and adjusted multiple confounding factors, unlike other three included studies18.
In this study, no significant association was observed between selenium intake and the risk of depression. The included observational studies estimated selenium intake from foods as well as nutritional supplements. Therefore, it is possible that their results were confounded by the bioavailability of dietary or supplementary selenium. Cumulative evidence has proposed that selenium bioavailability is affected by the chemical form of selenium (organic or inorganic). Organic selenium is more bioavailable than inorganic selenium and also retains in tissues more50. Similarly, the effectiveness of inorganic supplements of selenium has been reported to be less than that of organic supplements51. Moreover, components such as heavy metals, fiber, lipids, dietary sulfur, and oxalate can have antagonistic effects on the bioavailability of dietary selenium52,53. Furthermore, selenium methionine and selenium cysteine were decreased during cooking processes54. Unfortunately, the included studies did not report any data on the bioaccessibility and bioavailability of selenium in diet or supplements. Future studies need to be focused on these issues.
The subgroup analysis revealed that high selenium intake was significantly associated with low risk of postpartum depression. Due to the placental transfer of selenium to the fetus, maternal serum selenium levels are reduced during pregnancy, especially in the 3rd trimester. In addition, selenium is secreted in maternal breast milk as a component of selenoproteins. These processes increase the daily selenium requirement of pregnant and lactating women, which may result in selenium deficiency if not compensated properly55. It should be noted that supplementary selenium is more effective than dietary selenium in the improvement of low serum selenium levels56. In this meta-analysis, all studies conducted on postpartum depression considered supplementary, but not dietary, intake of selenium. This could contribute to the observed significant association between selenium intake and the risk of postpartum depression.
Interestingly, the present meta-analysis indicated that selenium supplementation significantly decreased depressive symptoms. Several mechanisms can explain this beneficial effect of selenium on depression. Selenium is known as a key regulatory factor of inflammatory and oxidative responses. Selenium deficiency can disrupt the function of multiple antioxidant enzymes such as glutathione peroxidase and thioredoxin reductases, which protect cells against oxidative damage57,58. Furthermore, inflammation is regarded as a part of depression pathogenesis59. Therefore, anti-inflammatory properties of selenium may help to improve depressive symptoms60,61. It is also possible that selenium affects depression symptoms through the modulation of neurotransmitter turnover as well as regulation of thyroid function62,63.
Several techniques have been suggested to determine serum concentration of selenium including atomic absorption spectrometry, molecular, atomic fluorescence spectrometry, inductively coupled plasma-mass spectrometry (ICP-MS) and graphite furnace atomic absorption spectrometry, flame atomic absorption, electrothermal atomic absorption spectrometry64,65,66,67. Atomic fluorescence spectrometry has higher sensitivity and is simpler than atomic absorption spectrometry. However, it has some detection limits68. Graphite furnace atomic absorption spectrometry is a selective, sensitive and easy method, however it is a single element technique69,70. Electrothermal atomic absorption spectrometry requires a small sample volume. This method is sophisticated and expensive66,71. Flame atomic absorption spectroscopy as a precise method, requires high sample preparation72. Serum or plasma selenium is assessed usually by two common methods of ICP-MS and atomic absorption spectrometry. ICP-MS is higher sensitivity than atomic spectrometry. It has multi-element capability, good stability and detects qualitative and quantitative trace element. However, this method is relatively expensive73. Atomic absorption spectrometry has a low detection limit. Although, this method is comparatively inexpensive, it is not an exclusive detection technique72. As a result, the different methodologies used to measure selenium in serum may be considered as one of the sources of heterogeneity. The method used to measure serum concentration of selenium in included studies are reported in Supplementary Table 1. Unfortunately, we could not evaluate the effect of this factor on the study findings. It has been proposed that serum concentration of selenium may be affected by sex and age74. The association between serum selenium level and gender is not clear. Some previous investigations indicated that there was no significant difference in serum selenium between males and females75,76,77. However, several studies reported serum concentration of selenium was related to gender78,79. Some studies reported that serum selenium concentration was higher in men compared with women78,79. In contrast, one study revealed that women had higher serum selenium in comparison with men80. It is possible that some factors including differences in sexual hormones, smoking and dietary habits play a role in relationship between gender to serum selenium level80,81,82. Also, the findings of studies regarding the effect of age on serum selenium concentration are inconsistent. According to the previous studies, no significant association between serum selenium and age was found79,83. However, this finding was not approved by some studies84,85. It seems that changes in body selenium distribution, dietary habits and hormonal status probably affect selenium concentration through different ages82,86,87,88. For example, plasma estrogen is positively related to serum selenium. Therefore, change of estrogen status throughout the life cycle can influence serum selenium in women89. Moreover, a significant reduction in serum selenium has been reported in elderly individuals78. Accumulation of inflammatory factors, change in physiology conditions, inadequate intake of selenium-rich sources and inefficient absorption of dietary selenium are contributed in the relationship between the declined serum selenium level and aging90,91,92.
This study has several limitations. First, there were high levels of heterogeneity in all analyses except for the effect of selenium supplementation on depression scores. Second, due to the insufficient number of studies, we could not run subgroup analyses for all outcomes except for selenium intake and the relative risk of depression. Third, potential confounding factors were not adjusted in some of the included studies, which might affect the findings.
Strengths of the present study should also be considered. First, this study is the first meta-analysis that investigated the role of selenium in depressive disorders. Second, we conducted a comprehensive search using several databases to identify eligible studies. Third, we included both interventional and observational studies in this systematic review and meta-analysis to perform a comprehensive assessment regarding selenium and depression.
Conclusion
In conclusion, the findings of this systematic review and meta-analysis suggest that high selenium intake may have a protective role against postpartum depression. In addition, our findings support that supplementation with selenium can be effective in reducing depressive symptoms. Nevertheless, further studies are needed to draw definitive conclusions.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- NOS:
-
The Newcastle–Ottawa Scale
- CCRBT:
-
The Cochrane Collaboration Risk of Bias Tool
- SE:
-
Standard errors
- SD:
-
Standard deviations
- CI:
-
Confidence interval
- WMD:
-
Weighted mean difference
- OR:
-
Odds ratio
- r:
-
Correlation
References
Depression WHO. Other Common Mental Disorders: Global Health Estimates 1–24 (World Heal Organ, 2017).
Vilagut, G., Forero, C. G., Barbaglia, G. & Alonso, J. Screening for depression in the general population with the center for epidemiologic studies depression (CES-D): A systematic review with meta-analysis. PLoS ONE 11(5), e0155431. https://doi.org/10.1371/journal.pone.0155431 (2016).
James, S. L. et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 392(10159), 1789–1858 (2018).
Liu, Q. et al. Changes in the global burden of depression from 1990 to 2017: Findings from the Global Burden of Disease study. J. Psychiatr. Res. 126, 134–140 (2020).
Maj, M. Validity and clinical utility of the current operational characterization of major depression. Int. Rev. Psychiatry. 24(6), 530–537 (2012).
Gawlik, S. et al. Subclinical depressive symptoms during pregnancy and birth outcome—A pilot study in a healthy German sample. Arch. Womens Ment. Health 16(2), 93–100 (2013).
Organisation WH. Depression. Fact Sheet N 369 (World Health Organization, 2013).
Kaplan, B. J., Field, C. J., Crawford, S. G. & Simpson, J. S. A. Vitamins, minerals, and mood. Psychol. Bull. 133(5), 747–760 (2007).
Skarupski, K. A. et al. Longitudinal association of vitamin B-6, folate, and vitamin B-12 with depressive symptoms among older adults over time. Am. J. Clin. Nutr. 92(2), 330–335 (2010).
Jiang, J. et al. Dietary intake of human essential elements from a Total Diet Study in Shenzhen, Guangdong Province, China. J. Food Compos. Anal. 39, 1–7 (2015).
Rayman, M. P. The importance of selenium to human health. Lancet 356(9225), 233–241 (2000).
Rayman, M. P. Selenium and human health. Lancet 379(9822), 1256–1268 (2012).
Wang, X., Yang, T., Wei, J., Lei, G. & Zeng, C. Association between serum selenium level and type 2 diabetes mellitus: A non-linear dose–response meta-analysis of observational studies. Nutr. J. 15(1), 48 (2015).
Shahar, A. et al. Plasma selenium is positively related to performance in neurological tasks assessing coordination and motor speed. Mov. Disord. 25(12), 1909–1915 (2010).
Conner, T. S., Richardson, A. C. & Miller, J. C. Optimal serum selenium concentrations are associated with lower depressive symptoms and negative mood among young adults. J. Nutr. 145(1), 59–65 (2015).
Amini, S. et al. The relationship between dietary intakes during pregnancy and incidence of postpartum depression: A case–control study. Nutr. Food Sci. 50, 751–764 (2019).
Sánchez-Villegas, A. et al. Micronutrient intake adequacy and depression risk in the SUN cohort study. Eur. J. Nutr. 57(7), 2409–2419 (2018).
Ekramzadeh, M., Mazloom, Z. & Sagheb, M. Association of depression with selenium deficiency and nutritional markers in the patients with end-stage renal disease on hemodialysis. J. Ren. Nutr. 25(4), 381–387 (2015).
Wieder-Huszla, S. et al. The severity of depressive and anxiety symptoms in postmenopausal women depending on their magnesium, zinc, selenium and copper levels. J. Elem. 25(4), 1305–1317 (2020).
Mokhber, N. et al. Effect of supplementation with selenium on postpartum depression: A randomized double-blind placebo-controlled trial. J. Matern. Fetal Neonatal. Med. 24(1), 104–108 (2011).
Gosney, M. A., Hammond, M. F., Shenkin, A. & Allsup, S. Effect of micronutrient supplementation on mood in nursing home residents. Gerontology 54(5), 292–299 (2008).
Shor-Posner, G. et al. Psychological burden in the era of HAART: Impact of selenium therapy. Int. J. Psychiatry Med. 33(1), 55–69 (2003).
Wang, J., Um, P., Dickerman, B. A. & Liu, J. Zinc, magnesium, selenium and depression and implications. Nutrients 10, 1–19 (2018).
Stroup, D. F. et al. Meta-analysis of observational studies in epidemiology: A proposal for reporting. JAMA 283(15), 2008–2012. https://doi.org/10.1001/jama.283.15.2008 (2000).
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G. & Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 6(7), e1000097 (2009).
Wells, G. A., et al. The Newcastle–Ottawa Scale (NOS) for assessing the quality if nonrandomized studies in meta-analyses. 2009. http://www.ohrica/programs/clinical_epidemiology/oxford.htm.
Higgins, J. P. Cochrane handbook for systematic reviews of interventions. Version 5.1.0 [updated March 2011] (2011). The Cochrane Collaboration. www cochrane-handbook org.
Juming, D. Research on Data Conversion Method in Meta Analysis (Southern Medical University, 2014).
DerSimonian, R. & Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 7(3), 177–188 (1986).
DerSimonian, R. & Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 28(2), 105–114 (2007).
Hedges, L. & Olkin, I. Statistical Methods for Meta-Analysis (Academic Press, 2014).
Choong, H., Adznam, S., Ibrahim, Z. & Norazman, C. Nutritional status in relation to depressive symptoms among Chinese elderly in Malaysia. Malays. J. Med. Health Sci. 15, 53–60 (2019).
Leung, B. M. Y. et al. Prenatal micronutrient supplementation and postpartum depressive symptoms in a pregnancy cohort. BMC Pregnancy Childbirth 13, 2 (2013).
Jin, Y., Coad, J., Pond, R., Kim, N. & Brough, L. Selenium intake and status of postpartum women and postnatal depression during the first year after childbirth in New Zealand-Mother and Infant Nutrition Investigation (MINI) Study. J. Trace Elem. Med. Biol. 61, 126503 (2020).
Perez-Cornago, A., Zulet, M. A. & Martinez, J. A. Association between mood and diet quality in subjects with metabolic syndrome participating in a behavioural weight-loss programme: A cross-sectional assessment. Nutr. Neurosci. 18(3), 137–144 (2015).
Ibarra, O. et al. The Mediterranean diet and micronutrient levels in depressive patients. Nutr. Hosp. 31(3), 1171–1175 (2015).
Li, Z., Wang, W., Xin, X., Song, X. & Zhang, D. Association of total zinc, iron, copper and selenium intakes with depression in the US adults. J. Affect. Disord. 1(228), 68–74 (2018).
Ghimire, S., Baral, B. K., Feng, D., Sy, F. S. & Rodriguez, R. Is selenium intake associated with the presence of depressive symptoms among US adults? Findings from National Health and Nutrition Examination Survey (NHANES) 2011–2014. Nutrition 1(62), 169–176 (2019).
Samad, N., Yasmin, F. & Manzoor, N. Biomarkers in drug free subjects with depression: Correlation with tryptophan. Psychiatry Investig. 16(12), 948–953 (2019).
Islam, M. R. et al. Alterations of serum macro-minerals and trace elements are associated with major depressive disorder: A case–control study. BMC Psychiatry 18(1), 1–7 (2018).
Banikazemi, Z., Mirzaei, H., Mokhber, N. & Mobarhan, M. G. Selenium intake is related to beck’s depression score. Iran Red. Crescent Med. J. 18(2), e21993 (2016).
Singh, A. et al. Micronutrient dietary intake in Latina pregnant adolescents and its association with level of depression, stress, and social support. Nutrients 9(11), 1212 (2017).
Pasco, J. A. et al. Dietary selenium and major depression: A nested case-control study. Complement. Ther. Med. 20(3), 119–123 (2012).
Sparling, T. M., Henschke, N., Nesbitt, R. C. & Gabrysch, S. The role of diet and nutritional supplementation in perinatal depression: A systematic review. Matern. Child Nutr. 13(1), e12235 (2017).
Farooq, S., Singh, S. P., Burke, D., Naeem, F. & Ayub, M. Pharmacological interventions for prevention of depression in high risk conditions: Systematic review and meta-analysis. J. Affect. Disord. 269, 58–69 (2020).
Xiao-hu, Z. & Zhi-hua, Z. Risk factors for postpartum depression: An evidence-based systematic review of systematic reviews and meta-analyses. Asian J. Psychiatr. 53, 102353. https://doi.org/10.1016/j.ajp.2020.102353 (2020).
Finley, J. W. & Penland, J. G. Adequacy or deprivation of dietary selenium in healthy men: Clinical and psychological findings. J. Trace Elem. Exp. Med. 11(1), 11–27 (1998).
Duffield, A. J. & Thomson, C. D. A comparison of methods of assessment of dietary selenium intakes in Otago, New Zealand. Br. J. Nutr. 82(2), 131–138 (1999).
Gao, S. et al. Selenium level and depressive symptoms in a rural elderly Chinese cohort. BMC Psychiatry 12, 72 (2012).
Thomson, C. D. Assessment of requirements for selenium and adequacy of selenium status: A review. Eur. J. Clin. Nutr. 58(3), 391–402 (2004).
Schrauzer, G. N. & Surai, P. F. Selenium in human and animal nutrition: Resolved and unresolved issues. A partly historical treatise in commemoration of the fiftieth anniversary of the discovery of the biological essentiality of selenium, dedicated to the memory of Klaus Schwarz (1914–1978) on the occasion of the thirtieth anniversary of his death. Crit. Rev. Biotechnol. 29(1), 2–9 (2009).
Hamilton, S. J. Review of selenium toxicity in the aquatic food chain. Sci. Total Environ. 326(1–3), 1–31 (2004).
Robinson, M. F. & Thomson, C. D. The role of selenium in the diet. Nutr. Abstr. Rev. 40, 3–26 (1983).
Khanam, A. & Platel, K. Bioaccessibility of selenium, selenomethionine and selenocysteine from foods and influence of heat processing on the same. Food Chem. 194, 1293–1299 (2016).
Bedwal, R. S. & Bahuguna, A. Zinc, copper and selenium in reproduction. Experientia 50(7), 626–640 (1994).
Combs, G. F., Clark, L. C. & Turnbull, B. W. An analysis of cancer prevention by selenium. BioFactors 14(1–4), 153–159 (2001).
Mertens, K. et al. Low zinc and selenium concentrations in sepsis are associated with oxidative damage and inflammation. Br. J. Anaesth. 114(March), 990–999 (2015).
Steinbrenner, H. & Sies, H. Selenium homeostasis and antioxidant selenoproteins in brain: Implications for disorders in the central nervous system. Arch. Biochem. Biophys. 536(2), 152–157 (2013).
Młyniec, K. et al. Essential elements in depression and anxiety. Part II. Pharmacol. Rep. 67(2), 187–194 (2015).
Mitchell, J. H., Nicol, F. & Beckett, G. J. Selenoprotein expression and brain development in preweanling selenium-and iodine-deficient rats. J. Mol. Endocrinol. 20(2), 203–210 (1998).
Bilici, M. et al. Antioxidative enzyme activities and lipid peroxidation in major depression: Alterations by antidepressant treatments. J. Affect. Disord. 64(1), 43–51 (2001).
Castaño, A. et al. Low selenium diet increases the dopamine turnover in prefrontal cortex of the rat. Neurochem. Int. 30(6), 549–555 (1997).
Roman, M., Jitaru, P. & Barbante, C. Selenium biochemistry and its role for human health. Metallomics 6(1), 25–54 (2014).
Sabé, R., Rubio, R. & García-Beltrán, L. Selenium determination in urine with atomic fluorescence detection. Anal. Chim. Acta 436(2), 215–221 (2001).
Peroxidase, G., Stress, O., Def, S., Virus, H. I. & Cancer, I. P. Selenium blood level SELENIUM | physiology what are the effects of dietary supplements (selenium and vitamin E) or aspirin/NSAIDs on prostate cancer? Oxidative stress, antioxidants and cancer trace elements: Functions and assessment of stat (2014).
Chatterjee, A., Tao, H., Shibata, Y. & Morita, M. Determination of selenium compounds in urine by high-performance liquid chromatography-inductively coupled plasma mass spectrometry. J. Chromatogr. A 997(1–2), 249–257 (2003).
Pedro, J., Andrade, F., Magni, D., Tudino, M. & Bonivardi, A. On-line submicellar enhanced fluorometric determination of Se(IV) with 2,3-diaminonaphthalene. Anal. Chim. Acta 516(1–2), 229–236 (2004).
Sánchez-Rodas, D., Corns, W. T., Chen, B. & Stockwell, P. B. Atomic Fluorescence Spectrometry: A suitable detection technique in speciation studies for arsenic, selenium, antimony and mercury. J. Anal. At. Spectrom. 25(7), 933–946 (2010).
Borges, D. L. G. & Holcombe, J. A. Graphite furnace atomic absorption spectrometry. In Encyclopedia of Analytical Chemistry (ed. Meyers, R. A.) 1–20 (London, 2017).
Butcher, D. J. Recent highlights in graphite furnace atomic absorption spectrometry. Appl. Spectrosc. Rev. 52(9), 755–773. https://doi.org/10.1080/05704928.2017.1303504 (2017).
Jackson, K. W. Electrothermal atomic absorption spectrometry and related techniques. Anal. Chem. 72(12), 159–168 (2000).
Boss, C. B. & Fredeen, K. J. Concepts, Instrumentation and Techniques in Atomic Absorption Spectrophotometry 2–12 (Perkin Elmer, 1997).
Wilschefski, S. C. & Baxter, M. R. Inductively coupled plasma mass spectrometry: Introduction to analytical aspects. Clin. Biochem. Rev. 40(3), 115–133 (2019).
Ghayour-Mobarhan, M., Taylor, A., New, S. A., Lamb, D. J. & Ferns, G. A. A. Determinants of serum copper, zinc and selenium in healthy subjects. Ann. Clin. Biochem. 42(5), 364–375 (2005).
Lopes, P. A. et al. Trace element status (Se, Cu, Zn) in healthy Portuguese subjects of Lisbon population: A reference study. Biol. Trace Elem. Res. 101(1), 1–17 (2004).
Li, N. et al. Selenium level in the environment and the population of Zhoukoudian area, Beijing, China. Sci. Total Environ. 381(1–3), 105–111 (2007).
Korunová, V. et al. Serum selenium in adult Czechoslovak (central bohemia) population. Biol. Trace Elem. Res. 37(2–3), 91–99 (1993).
Kafai, M. R. & Ganji, V. Sex, age, geographical location, smoking, and alcohol consumption influence serum selenium concentrations in the USA: Third National Health and Nutrition Examination Survey, 1988–1994. J. Trace Elem. Med. Biol. 17(1), 13–18 (2003).
Safaralizadeh, R. et al. Serum concentration of selenium in healthy individuals living in Tehran. Nutr. J. 4, 1–4 (2005).
Letsiou, S. et al. Serum total selenium status in Greek adults and its relation to age. The ATTICA study cohort. Biol. Trace Elem. Res. 128(1), 8–17 (2009).
Alfthan, G. & Neve, J. Reference values for serum selenium in various areas-evaluated according to the TRACY protocol. J. Trace Elem. Med. Biol. 10(2), 77–87. https://doi.org/10.1016/S0946-672X(96)80015-0 (1996).
Arnaud, J. et al. Serum selenium determinants in French adults: The SU.VI.M.AX study. Br. J. Nutr. 95(2), 313–320 (2006).
Pavão, M. L. et al. Comparison of whole-blood glutathione peroxidase activity, levels of serum selenium, and lipid peroxidation in subjects from the fishing and rural communities of “Rabo de Peixe” village, San Miguel Island, The Azores’ archipelago, Portugal. Biol. Trace Elem. Res. 92(1), 27–40 (2003).
Wgsowicz, W. & Zachara, B. A. Selenium concentrations in the blood and urine of a healthy polish sub-population. Clin. Chem. Lab. Med. 25(7), 409–412 (1987).
Lee, O., Moon, J. & Chung, Y. The relationship between serum selenium levels and lipid profiles in adult women. J. Nutr. Sci. Vitaminol. (Tokyo) 49(6), 397–404 (2003).
Letsiou, S. et al. Gender-specific distribution of selenium to serum selenoproteins: Associations with total selenium levels, age, smoking, body mass index, and physical activity. BioFactors 40(5), 524–535 (2014).
Adolf, L. Recommended dietary allowances. Clin. Pediatr. (Phila.) 3(122), 630–632 (1964).
Behne, D. & Hofer-Bosse, T. Effects of a low selenium status on the distribution and retention of selenium in the rat. J. Nutr. 114(7), 1289–1296 (1984).
Smith, A. M., Chang, M. P. H. & Medeiros, L. C. Generational differences in selenium status of women. Biol. Trace Elem. Res. 75(1–3), 157–165 (2000).
Lloyd, B., Lloyd, R. S. & Clayton, B. E. Effect of smoking, alcohol, and other factors on the selenium status of a healthy population. J. Epidemiol. Community Health 37(3), 213–217 (1983).
Ravaglia, G. et al. Blood micronutrient and thyroid hormone concentrations in the oldest-old. J. Clin. Endocrinol. Metab. 85(6), 2260–2265 (2000).
Ekmekcioglu, C. The role of trace elements for the health of elderly individuals. Nahrung Food. 45(5), 309–316 (2001).
Acknowledgements
Food Security Research Center, Isfahan University of Medical Sciences, Isfahan, Iran supported present study.
Funding
There is no financial arrangement between an author and a company whose product figures prominently in the submitted manuscript. This study was supported by Isfahan University of Medical Sciences [Grant Number 199229].
Author information
Authors and Affiliations
Contributions
S.H. and M.H.R. designed the study. M.H.R., S.H. and S.S.S. searched databases. S.S.S. screened the studies and checked inclusion and exclusion criteria. M.H.R. and S.F. analyzed the study. S.S.S. and S.F. wrote the manuscript. M.H.R. revised the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sajjadi, S.S., Foshati, S., Haddadian-Khouzani, S. et al. The role of selenium in depression: a systematic review and meta-analysis of human observational and interventional studies. Sci Rep 12, 1045 (2022). https://doi.org/10.1038/s41598-022-05078-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-05078-1
This article is cited by
-
Biogeochemical behavior of selenium in soil-air-water environment and its effects on human health
International Journal of Environmental Science and Technology (2024)
-
Association between serum copper, zinc, and selenium concentrations and depressive symptoms in the US adult population, NHANES (2011–2016)
BMC Psychiatry (2023)
-
Selenium alleviates modafinil-induced neurobehavioral toxicity in rat via PI3K/Akt/mTOR/GSK3B signaling pathway and suppression of oxidative stress and apoptosis: in vivo and in silico study
Environmental Science and Pollution Research (2023)
-
Knocking out Selenium Binding Protein 1 Induces Depressive-Like Behavior in Mice
Biological Trace Element Research (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
