
Abstract
To assess the distribution of axial length as surrogate for myopia and its determinants in an old population, we performed the Ural Very Old Study as a population-based cohort study. Out of 1882 eligible individuals aged 85 + years, the Ural Very Old Study performed in an urban and rural region in Bashkortostan/Russia included 1526 (81.1%) individuals undergoing ophthalmological and medical examinations with sonographic axial length measurement. Biometric data were available for 717 (47.0%) individuals with a mean age of 88.0 ± 2.6 years (range 85–98 years; 25%). Mean axial length was 23.1 ± 1.1 mm (range 19.37–28.89 mm). Prevalences of moderate myopia (axial length 24.5–< 26.5 mm) and high myopia (axial length ≥ 26.5 mm) were 47/717 (6.6%; 95% CI 4.7, 8.4) and 10/717 (1.4%; 95% CI 0.5, 2.3), respectively. In multivariable analysis, longer axial length was associated (coefficient of determination r2 0.25) with taller body height (standardized regression coefficient beta:0.16;non-standardized regression coefficient B: 0.02; 95% confidence interval (CI) 0.01, 0.03; P < 0.001), higher level of education (beta: 0.12; B: 0.07; 95% CI 0.02, 0.11; P = 0.002), and lower corneal refractive power (beta: − 0.35; B: − 0.23; 95% CI − 0.28, − 0.18; P < 0.001). Higher prevalence of moderate myopia, however not of high myopia, was associated with higher educational level (OR 1.39; 95% CI 1.09, 1.68; P = 0.007) and lower corneal refractive power (OR 0.77; 95% CI 0.63, 0.94; P = 0.01). In this old study population, prevalence of moderate axial myopia (6.6% versus 9.7%) was lower than, and prevalence of high axial myopia (1.4% versus 1.4%) was similar as, in a corresponding study on a younger population from the same Russian region. Both myopia prevalence rates were higher than in rural Central India (1.5% and 0.4%, respectively). As in other, younger, populations, axial length and moderate myopia prevalence increased with higher educational level, while high myopia prevalence was independent of the educational level.
Similar content being viewed by others


Introduction
The ocular axial length is a principal biometric measure of the eye and the most important determinant of axial ametropias, i.e. myopia and hyperopia. It is associated with ocular disorders and diseases such as primary angle-closure glaucoma, diabetic retinopathy, age-related macular degeneration, strabismus and amblyopia in the case of axial hyperopia, and with rhegmatogenous retinal detachment, myopic macular degeneration and high myopia-associated optic neuropathy in the case of axial myopia1,2,3,4. In the recent decades, the prevalence of axial myopia has markedly increased and the prevalence of axial hyperopia has subsequently decreased5. It has thus been anticipated that the prevalences of ocular disorders associated with axial length will change in the near future. In particular high myopia as the main risk factor for pathologic myopia has been estimated to be, or to become, the most common cause for irreversible vision impairment and blindness6, 7. Although axial length as the main measure of axial myopia has already been assessed in various population-based studies in several continents, data about the distribution of axial length in the very old population have been missing so far8,9,10,11,12,13,14. Knowledge about the prevalence of axial myopia, in particular of high myopia, in an elderly, yet unexplored population could give insight into the associations of axial moderate and high myopia with other ocular and systemic parameters in such a study sample, and, by comparing the prevalence of high myopia between such an elderly population and a normal-aged population could potentially give hints for the future development of the prevalence of high myopia. We therefore conducted this survey to examine the distribution of axial length and its determinants in a study population aged 85 + years15. To avoid a referral bias, we recruited the participants in a population-based manner.
Methods
The Ural Very Old Study (UVOS) is a population-based study performed in the rural region of the Karmaskalinsky District in a distance of 65 km from the capital Ufa, and in the Kirovskyi discrict—an urban region of the capital Ufa in the Republic of Bashkortostan/Russia. The study conducted between November 2017 and December 2020, was approved by the Ethics Committee of the Academic Council of the Ufa Eye Research Institute confirming that all methods were performed in accordance with the relevant guidelines and regulations, and informed written consent was obtained from all participants. Inclusion criteria were an age of 85 + years and living in the study regions. There were no exclusion criteria.
Out of 1882 eligible individuals, 1526 (81%) persons participated in the study. The eligible individuals, recruited in a census manner, included the inhabitants of three private small retirement homes in the urban study region (with about 45 study individuals from all three homes together). There were no retirement homes in the rural study region. The participation rate did not vary markedly between the urban group [1238 (81.3%) out of 1523 individuals] and the rural group [288 (80.2%) out of 359 individuals]. According to the census carried out in Russia in 2010, the composition of the UVOS population with respect to gender and age corresponded to the gender and age distribution in the Russian population beyond an age of 85 + years, with a marked preponderance of females16.
All study participants underwent a standardized interview conducted by trained social workers with about 300 questions on the socioeconomic background, diet, smoking, alcohol consumption, physical activity, quality of life and quality of vision, symptoms of chronic obstructive pulmonary disease, asthma, kidney disease and orthopedic disorders, history of any type of injuries and inter-personal violence, health assessment questions, and history of major medical disorders. The questions had been validated in previous investigations such as the Folstein test, Zung’s self-rated depression scale, and the National Eye Institute Visual Functioning Questionnaire-25 (VFQ-25) (Table 1)17,18,19.
The physical examinations consisted of measurements of anthropomorphic parameters such as body height and weight, arterial blood pressure and pulse rate, and dynamometric assessment of the handgrip strength. Blood samples taken under fasting conditions were biochemically examined. Arterial hypertension was defined according to the guidelines of the American College of Cardiology/American Heart Association20. Diabetes mellitus was characterized by a fasting glucose concentration of ≥ 7.0 mmol/L or self-reported history of physician diagnosis of diabetes mellitus or history of drug treatment of diabetes. Depression was assessed applying the Center for Epidemiologic Studies Depression Scale Scoresheet21. We calculated the estimated glomerular filtration rate using the chronic kidney disease Epidemiology Collaboration equation22. We applied the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER statement guidelines)23. The UVOS design was similar to the design of the Ural Eye and Medical Study (UEMS) which has been described in detail previously14, 24.
The ophthalmological examinations, performed for all participating individuals, consisted of automated refractometry, measurement of presenting, uncorrected and best corrected visual acuity (using the results of automatic refractometry and refining it by subjective comparison), static perimetry (PTS 1000 Perimeter, Optopol Technology Co., Zawercie, Poland; screening test program with 82 test points and an extension of 50° in all directions), anterior segment imaging using the Scheimflug camera (Pentacam HR, Typ70900, OCULUS, Optikgeräte GmbH Co., Wetzlar, Germany) for measurements of the cornea, anterior chamber and lens, biometric measurement of the axial length by sonography (Ultra-compact A/B/P ultrasound system, Compact touch; Quantel Medical, Cournon d'Auvergne, France, US-4000, Nidek, Japan), slit lamp biomicroscopy of the anterior and posterior ocular segment, photography of the cornea and lens (Topcon slit lamp and camera, Topcon Corp., Tokyo, Japan), non-contact tonometry (Tonometer Kowa KT-800, Kowa Company Ltd., Hamamatsu City, Japan, Tonoref III, Nidek, Japan, PT 100 Recharging Base,Reichert, USA), examination for the presence of lens pseudoexfoliation after medical mydriasis, photography of the optic disc and macula (VISUCAM 500, Carl Zeiss Meditec AG, Jena, Germany, Optomed smartscope EY4, Finland), and spectral-domain optical coherence tomography (RS-3000 Edvance,, NIDEK co., Ltd., Aichi Japan, DRI OCT Triton (plus), Topcon, Japan) of the optic nerve head and macula.
Using a statistical software package (SPSS for Windows, version 25.0, SPSS, Chicago, IL), we determined the mean value of axial length and of its determinants (presented as mean ± standard error or as mean and 95% confidence intervals (CI)) and performed a univariate analysis of the relationships between axial length and other systemic and ocular parameters. It was followed by a multivariable linear regression analysis with axial length as the dependent parameter and as independent variables all those parameters that were significantly correlated with axial length in the univariate analyses. In a step-by-step procedure, we first dropped those independent variables which showed a high collinearity, as measured by the variance inflation factor. We then dropped in a step-by-step procedure those parameters out of the list of independent variables which were no longer significantly associated with axial length. We calculated the odds ratios (ORs) and their 95% CIs. All P-values were two-sided and considered statistically significant when the values were less than 0.05. Since the main study parameter was axial length and not refractive error, we did not exclude pseudophakic or aphakic individuals. Only one randomly selected eye per study participant was included into the statistical analysis.
Results
Out of 1526 individuals primarily participating in the UVOS and undergoing the standardized interview at their homes, the present investigation included 717 (47.0%) individuals for whom measurements of axial length for both eyes had been performed in the hospital (Table 2; Fig. 1). The reasons for individuals not participating in the study were mainly their physical inability to be transported to the hospital and undergo the hourlong series of examinations in the hospital, or their lack of interest in participating in the study. The individuals with axial length assessment as compared with those without this examination were significantly younger (88.0 ± 2.6 years versus 88.6 ± 3.1 years; P > 0.001) and a significantly higher level of education (4.96 ± 1.95 versus 4.14 ± 2.03; P > 0.001), while they did not differ significantly in sex (P = 0.11).

Flow chart of the population of the Ural Very Old Study.
Mean axial length was 23.1 ± 1.1 mm (median 22.97 mm; range 19.37–28.89 mm) and 23.1 ± 1.2 mm (median 23.00; range 19.50–28.84 mm) in the right eyes and left eyes, respectively (Fig. 2). Both eyes did not differ significantly in axial length (P = 0.05). Prevalence of moderate myopia (arbitrarily defined by an axial length of 24.5 to < 26.5 mm) and high myopia (arbitrarily defined by an axial length of ≥ 26.5 mm) were 47/717 (6.6%; 95% CI 4.7, 8.4) and 10/717 (1.4%; 95% CI 0.5, 2.3), respectively. In univariate analysis, a longer axial length was associated (P < 0.05) with the systemic parameters of female sex, rural region of habitation, taller body height, higher body weight and lower body mass index, higher level of education (Fig. 3), more frequent history of asthma, less frequent history of dementia, lower serum concentration of high-density lipoproteins and cholesterol, higher dynamometric hand grip force, higher mini-mental test score, and with the ocular parameters of more myopic refractive error (spherical and spherical equivalent), higher cylindrical refractive error, lower corneal refractive power, and higher prevalence of dry eye syndrome (defined by a dry eye score ≥ 8 and Schirmer’s test ≤ 5 mm) (Table 1).

Histogram showing the distribution of axial length in the Ural Very Old Study.

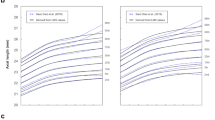
Graph showing the distribution of the prevalence of moderate myopia (axial length 24.5 mm to < 26.5 mm) in the Ural Very Old, stratified by the level of education.
In the multivariable analysis, we dropped due to collinearity the parameters of body weight (variance inflation factor (VIF): 123), and we dropped due to a lack of statistical significance the parameters of serum concentrations of cholesterol (P = 0.88) and high-density lipoproteins (P = 0.62), dynamometric hand grip force (P = 0.98), body mass index (P = 0.81), sex (P = 0.81), history of dementia (P = 0.22), mini mental test score (P = 0.24), region of habitation (P = 0.19), and diagnosis of dry eye disease (P = 0.06). In the final model, longer axial length was associated (correlation coefficient r 0.50) with taller body height (P < 0.001), higher level of education (P = 0.002), lower corneal refractive power (P < 0.001), in addition to a more myopic spherical refractive error (P < 0.001) (Table 3). The associations remained statistically significant after correcting the P-values by Bonferroni´s method to adjust for performing multiple statistical comparisons. In that model, taller body height (per centimeter) was associated with an increase in axial length by 0.02 mm, higher level of education (per each level out of 8 levels) was associated with an increase in axial length by 0.07 mm, higher corneal refractive power (per diopter) was associated with a decrease in axial length by 0.23 mm, and more myopic refractive error was associated with an increase in axial length by 0.09 mm (Table 3). Axial length was not significantly associated in that model with age (P = 0.27), sex (P = 0.55), region of habitation (P = 0.29), BCVA (P = 0.62), and intraocular pressure (P = 0.12). If the parameter of body height was dropped, longer axial length was associated with male sex (beta 0.12; B 0.28; 95% CI 0.10, 0.45; P = 0.002).
The prevalence of moderate myopia was significantly (univariate analysis) associated with body height (P = 0.02), level of education (P < 0.001), corneal refractive power (P = 0.01), and higher myopic refractive error (P = 0.004), but not with sex (P = 0.17), region of habitation (P = 0.99) or BCVA (P = 0.10). In multivariable binary analysis, a higher prevalence of moderate myopia remained to be significantly associated with a higher educational level (OR 1.39; 95% CI 1.09, 1.68; P = 0.007), lower corneal refractive power (OR 0.77; 95% CI 0.63, 0.94; P = 0.01) and more myopic refractive error (OR 0.82; 95% CI 0.74, 0.91; P < 0.001), while it was no longer associated with body height (P = 0.36).
The prevalence of high axial myopia was not significantly (univariate analysis) associated with body height (P = 0.18), level of education (P = 0.10), sex (P = 0.60), region of habitation (P = 0.99), corneal refractive power (P = 0.56). It was significantly correlated only with higher myopic refractive error (OR 0.82; 95% CI 0.72, 0.94; P = 0.002).
Discussion
In our study on an old population recruited in a population-based manner, mean axial length was 23.1 ± 1.1 mm, with a mean prevalence of moderate myopia and high myopia of 6.6% and 1.4%, respectively. Longer axial length was associated with taller body height, higher level of education, lower corneal refractive power and more myopic refractive error. Higher prevalence of moderate myopia was correlated with higher level of education, lower corneal refractive power and more myopic refractive error, while the prevalence of high axial myopia was not correlated with any of these parameters, except for higher myopic refractive error.
These results cannot directly be compared with observations made in previous investigations, since a population with an age inclusion criterion of 85 + years as in our study has not been examined previously in such a context. In younger study populations, partially similar results were obtained as in our study. To cite an example, in the UEMS, performed on a study population aged 40 + years (mean:58.8 ± 10.6 years) and conducted in the same region as the present study, the mean axial length was 23.3 ± 1.1 mm, a value similar to the result in our study population14. The mean axial length as found in our study was larger than in some other population-based studies, such as in the Central India and Medical Study (CIEMS) (22.6 ± 0.91 mm) and in a rural South Indian population study (22.8 ± 0.8 mm), they were similar to the values reported from a Mongolian population (23.1 ± 1.2 mm) and the Singaporean Tanjong Pagar Study (23.2 ± 1.2 mm), and they were lower than the mean axial length found in the Los Angeles Latino Eye Study (23.4 ± 1.1 mm), the Beijing Eye Study (23.3 ± 1.1 mm), the Beaver Dam Eye Study (23.7 ± 1.2 mm) and the EPIC-Norfolk study from England (23.8 ± 1.2 mm8, 10,11,12,13, 25, 26.
The prevalence of moderate myopia (axial length 24.5 to < 26.5 mm) was significantly lower in our study sample than in the younger population of the UEMS [6.6% (95% CI 4.7, 8.4) versus 9.7% (95% CI 9.0, 10.5)], and it was also lower than in other studies such as the Beijing Eye Study with a prevalence of moderate myopia (with the same definition) of 8.6% (95% CI 7.3, 9.2)13. It was higher than in the CIEMS (1.5%; 95% CI 1.2, 1.7).
The prevalence of high myopia (axial length > 26.5 mm) was similar in the UEMS and in the present study [1.4% (95% CI 1.1, 1.7) versus 1.4% (95% CI 0.5, 2.3), while it was in both studies lower than in the Beijing Eye Study (minimal age of 40 years) with a prevalence of 1.7% (95% CI 1.3, 2.2)13. It was markedly higher than in the population of the CIEMS (0.4%; 95% CI 0.3, 0.6). A reason for the discrepancy between the study populations in the prevalence in high myopia may be differences in the prevalence of overall myopia, since the CIEMS as compared to the present study had a lower prevalence also of moderate myopia. Another reason may be a survival factor, with a potentially lower life expectancy for highly myopic individuals in the very rural region in Central India. The cause for the differences in the prevalence of moderate myopia may be the association between longer axial length and higher level of education, with the lowest mean level of education in the very rural study region of the CIEMS. It would fit with the observation of a marked increase in the prevalence of axial myopia in the young generation in China, parallel to a profound increase in the educational activities of school children in China27.
The association between longer axial length and higher educational level is a universal phenomenon, since it was reported, besides from our investigation, also from studies performed in other countries12, 13, 28, 29. In our study, the prevalence of high myopia, in contrast to the prevalence of moderate myopia, was not significantly related to the level of education. As a corollary, the prevalence of high myopia in the Beijing Eye Study on adults aged 40 + years was associated with a lower level of education13. It fits with the results of a recent meta-analysis, in which the prevalence of high myopia in adults was not, however, the prevalence of high myopia in school children was, associated with education-related parameters30.
Longer axial length was associated with taller body height in our study as well as in the UEMS, and as also reported from the Singaporean Tanjong Pagar Study, the Icelandic Reykjavik Eye Study, the Burmese Meiktila Eye Study and the Beijing Eye Study8, 13, 31, 32. It fits with the observation that the prevalence of primary angle-closure glaucoma was associated with shorter body height in previous studies33.
In contrast to previous studies on younger populations, such as the Beijing Eye Study, the CIEMS, a study from Mongolia and the UEMS, axial length did not increase with older age in our study population10, 12,13,14. In other studies, however, axial length decreased with older age, or it was not related at all8, 10, 11. Reasons for the discrepancies may be when the marked increase in axial myopia in association with more time spent indoors versus outdoors and the more profound educational activities started in the various countries.
Axial length was not related with IOP in our study, in contrast to the UEMS and the Japanese Kumejima study, the Japanese Tajimi Study and the Chinese Handan Study14, 34,35,36. As in our study, axial length was unrelated to IOP in the Los Angeles Latino Eye Study37. While the causes for a potential association between axial length and IOP have remained elusive, it has been discussed whether higher IOP leads to longer axial length or whether axial elongation-associated factors lead to an increase in IOP. Axial length was neither associated with BCVA in our study, while in the UEMS, BCVA showed a curvilinear relationship with axial length, with an improvement of BCVA from short axial length to medium axial length values, and deterioration of BCVA towards long axial length readings14. The marked difference in age between both study population may potentially be the reason for the discrepancy between both studies since axial myopia is partially protective against age-related macular degeneration and diabetic retinopathy3, 4.
When the findings obtained in the present investigation are discussed, its limitations should be considered. First, although 1526 out of 1882 eligible individuals participated in the Ural Very Old Study, resulting in a participation rate of 81%, only 717 (47.0%) individuals underwent the clinical examination including biometric axial length measurements. The individuals with biometry, as compared to those without biometry, were significantly younger and had a significantly higher educational level. These differences might have led to a bias. If one considers, however, the relatively old age of our study population with a minimum age of 85 years and the multimorbidity often occurring in that age, the participation rate for the clinical examinations in our study population may be acceptable. Second, the study regions of the UVOS were characteristic for Southern Russia in terms of demography, geography and climate. In terms of the ethnic background, the percentage of Russians was lower in our study population than in populations from North-Western Russia and Central Russia. In the multivariable analysis, however, the ethnic background was not associated with axial length, so that the relatively high percentage of non-Russians on the total study population might not have markedly influenced the results. Strengths of our investigation are that it is the first population-based investigation on axial length in a very old population, that also the inhabitants of all retirement homes in the study regions were included into the study, and that a multitude of systemic parameters was assessed and included in the statistical multivariable analysis. Since such a study population had not been examined previously, all findings were principally novel, while of special interest was the finding that the prevalence of moderate axial myopia was lower than, and the prevalence of high axial myopia was similar as, in a younger population in the same study regions.
In conclusion, in this old, multi-ethnic study population from rural and urban Russia, the prevalence of moderate axial myopia (6.6% versus 9.7%) was lower than, and the prevalence of high axial myopia (1.4% versus 1.4%) was similar as, in a corresponding study on a younger population from the same Russian region. The prevalence rates were higher than in rural Central India (1.5% and 0.4%, respectively). As in other, younger, populations, axial length and moderate myopia prevalence increased with higher educational level, while high myopia prevalence was independent of the educational level. The association between longer axial length and taller body height agrees with the notion of larger eyes in taller individuals.
References
Xu, L., Wang, Y., Wang, S., Wang, Y. & Jonas, J. B. High myopia and glaucoma susceptibility. The Beijing Eye Study. Ophthalmology 114, 216–220 (2007).
Jonas, J. B., Weber, P., Nagaoka, N. & Ohno-Matsui, K. Glaucoma in high myopia and parapapillary delta zone. PLoS ONE 12, e0175120 (2017).
Age-Related Eye Disease Study Research Group. Risk factors associated with age-related macular degeneration. A case-control study in the age-related eye disease study: Age-Related Eye Disease Study Report Number 3. Ophthalmology 107, 2224–2232 (2000).
Ikram, M. K., van Leeuwen, R., Vingerling, J. R., Hofman, A. & de Jong, P. T. Relationship between refraction and prevalent as well as incident age-related maculopathy: The Rotterdam Study. Invest. Ophthalmol. Vis. Sci. 44, 3778–3782 (2003).
Holden, B. A. et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology 123, 1036–1042 (2016).
Xu, L. et al. Causes of blindness and visual impairment in urban and rural areas in Beijing: The Beijing Eye Study. Ophthalmology 113, 1134–1141 (2006).
GBD 2019 Blindness and Vision Impairment Collaborators, Vision Loss Expert Group of the Global Burden of Disease Study. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health. 9, e144–e160 (2019).
Wong, T. Y. et al. Variations in ocular biometry in an adult Chinese population in Singapore: The Tanjong Pagar Survey. Invest. Ophthalmol. Vis. Sci. 42, 73–80 (2001).
George, R. et al. Ocular biometry in occludable angles and angle closure glaucoma: A population based survey. Br. J. Ophthalmol. 87, 399–402 (2003).
Wickremasinghe, S. et al. Ocular biometry and refraction in Mongolian adults. Invest. Ophthalmol. Vis. Sci. 45, 776–783 (2004).
Shufelt, C. et al. Refractive error, ocular biometry, and lens opalescence in an adult population: The Los Angeles Latino Eye Study. Invest. Ophthalmol. Vis. Sci. 46, 4450–4460 (2005).
Nangia, V. et al. Ocular axial length and its associations in an adult population of Central Rural India: The Central India Eye and Medical Study. Ophthalmology 117, 1360–1366 (2010).
Yin, G. et al. Ocular axial length and its associations in Chinese: The Beijing Eye Study. PLoS ONE 7, e43172 (2012).
Bikbov, M. M. et al. Axial length and its associations in a Russian population: The Ural Eye and Medical Study. PLoS ONE 14, e0211186 (2019).
Vollset, S. E. et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: A forecasting analysis for the Global Burden of Disease Study. Lancet 396, 1285–1306 (2020).
Federal State Statistic Service. Population Census. https://eng.gks.ru/folder/76215. Accessed 16 Jan 2021.
Folstein, M. F., Folstein, S. E. & McHugh, P. R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12, 189–198 (1975).
Zung, W. W. A Self-rating depression scale. Arch. Gen. Psychiatry. 12, 63–70 (1965).
Klein, R., Moss, S. E., Klein, B. E., Gutierrez, P. & Mangione, C. M. The NEI-VFQ-25 in people with long-term type 1 diabetes mellitus: The Wisconsin Epidemiologic Study of Diabetic Retinopathy. Arch. Ophthalmol. 119, 733–740 (2001).
Whelton, P. K. et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: A report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Hypertension 71, 1269–1324 (2018).
Thomas, J. L., Jones, G. N., Scarinci, I. C., Mehan, D. J. & Brantley, P. J. The utility of the CES-D as a depression screening measure among low-income women attending primary care clinics: The Center for Epidemiologic Studies-Depression. Int. J. Psychiatry Med. 31, 25–40 (2001).
Levey, A. S. et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 150, 604–612 (2009).
Stevens, G. A. et al. Guidelines for Accurate and Transparent Health Estimates Reporting: The GATHER statement. Lancet 388, e19-23 (2016).
Bikbov, M. M. et al. Prevalence of myopic maculopathy among adults in a Russian population. JAMA Netw. Open. 3, e200567 (2020).
Lee, K. E., Klein, B. E., Klein, R., Quandt, Z. & Wong, T. Y. Association of age, stature, and education with ocular dimensions in an older white population. Arch. Ophthalmol. 127, 88–93 (2009).
Foster, P. J. et al. Refractive error, axial length and anterior chamber depth of the eye in British adults: The EPIC-Norfolk Eye Study. Br. J. Ophthalmol. 94, 827–830 (2010).
Dong, L., Kang, Y. K., Li, Y., Wei, W. B. & Jonas, J. B. Prevalence and time trends of myopia in children and adolescents in China: A systemic review and meta-analysis. Retina 40, 399–411 (2020).
Wong, T. Y., Foster, P. J., Johnson, G. J. & Seah, S. K. Education, socioeconomic status, and ocular dimensions in Chinese adults: The Tanjong Pagar Survey. Br. J. Ophthalmol. 86, 963–968 (2002).
Morgan, I. G., Ohno-Matsui, K. & Saw, S. M. Myopia. Lancet 379, 1739–1748 (2012).
Jonas, J. B. et al. Education-related parameters in high myopia: Adults versus school children. PLoS ONE 11, e0154554 (2016).
Eysteinsson, T., Jonasson, F., Arnarsson, A., Sasaki, H. & Sasaki, K. Relationships between ocular dimensions and adult stature among participants in the Reykjavik Eye Study. Acta Ophthalmol. Scand. 83, 734–738 (2005).
Wu, H. M. et al. Association between stature, ocular biometry and refraction in an adult population in rural Myanmar: The Meiktila eye study. Clin. Experiment. Ophthalmol. 35, 834–839 (2007).
Xu, L., Li, J., Wang, Y. & Jonas, J. B. Anthropomorphic differences between angle-closure and open-angle glaucoma: The Beijing Eye Study. Acta Ophthalmol. Scand. 85, 914–915 (2007).
Tomoyose, E. et al. Intraocular pressure and related systemic and ocular biometric factors in a population-based study in Japan: The Kumejima study. Am. J. Ophthalmol. 150, 279–286 (2020).
Kawase, K. et al. Ocular and systemic factors related to intraocular pressure in Japanese adults: the Tajimi study. Br. J. Ophthalmol. 92, 1175–1179 (2008).
Zhou, Q. et al. Intraocular pressure and its relationship to ocular and systemic factors in a healthy Chinese rural population: The Handan Eye Study. Ophthal. Epidemiol. 19, 278–284 (2012).
Memarzadeh, F., Ying-Lai, M., Azen, S. P. & Varma, R. Associations with intraocular pressure in Latinos: The Los Angeles Latino Eye Study. Am. J. Ophthalmol. 146, 69–76 (2008).
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Design of the study: M.M.B., G.M.K., J.B.J.; Data collection: M.M.B., G.M.K., E.M.R., I.A.R., A.A.F., A.M.T., S.P.J., T.R.G., R.M.Z., N.I.B., K.R.S., A.V.G., I.P.P., D.F.Y., N.E.B., N.A.N., J.B.J.; Organization and surveillance: M.M.B., G.M.K.; Statistical analysis: J.B.J., S.P.J.; Drafting the first version of the manuscript: J.B.J., S.P.J.; Modifying and approving the final version of the manuscript: M.M.B., G.M.K., E.M.R., I.A.R., A.A.F., A.M.T., S.P.J., T.R.G., R.M.Z., N.I.B., K.R.S., A.V.G., I.P.P., D.F.Y., N.E.B., N.A.N., J.B.J.
Corresponding authors
Ethics declarations
Competing interests
Jost B. Jonas: Advisory Board Novartis; Patent holder with Biocompatibles UK Ltd. (Farnham, Surrey, UK) (Title: Treatment of eye diseases using encapsulated cells encoding and secreting neuroprotective factor and / or anti-angiogenic factor; Patent number: 20120263794), and Europäische Patentanmeldung 16 720 043.5 “Agents for use in the therapeutic or prophylactic treatment of myopia or hyperopia”; Advisor board member Abyss Processing Co.. Songhomitra Panda-Jonas: Patent holder with Biocompatibles UK Ltd. (Farnham, Surrey, UK) (Title: Treatment of eye diseases using encapsulated cells encoding and secreting neuroprotective factor and / or anti-angiogenic factor; Patent number: 20120263794), and Europäische Patentanmeldung 16 720 043.5 “Agents for use in the therapeutic or prophylactic treatment of myopia or hyperopia”. All other authors: No financial disclosures.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bikbov, M.M., Kazakbaeva, G.M., Rakhimova, E.M. et al. Axial length and its associations in the Ural Very Old Study. Sci Rep 11, 18459 (2021). https://doi.org/10.1038/s41598-021-98039-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-98039-z
This article is cited by
-
Bi-Gaussian analysis reveals distinct education-related alterations in spherical equivalent and axial length—results from the Gutenberg Health Study
Graefe's Archive for Clinical and Experimental Ophthalmology (2024)
-
Differences in close-work activities and optical axis length between only children and non-only children: a cross-sectional study
BMC Pediatrics (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
