
Abstract
The aim of this study was to explore cardiac autonomic changes assessed by linear and nonlinear indexes of heart rate variability (HRV) and body composition modifications in breast cancer survivors and cancer-free control women. Women who were breast cancer survivors (BCS, n = 27) and without cancer with similar characteristics (Control, n = 31) were recruited for this study. We calculated some relevant linear and nonlinear parameters of 5 min of RR interval time series such as mean RR interval (RRave), the corrected Poincaré index (cSD1/SD2), the sample entropy (SampEn), the long-term fractal scaling exponent (α2) and 2UV from symbolic dynamics. Additionally, we indirectly assessed body composition measures such as body weight, fat mass, visceral fat rating (VFR), normalized VRF (nVFR), muscle mass, metabolic age, and total body water. We found that diverse HRV indexes and only one body composition measure showed statistical differences (p < 0.05) between the BCS and Control groups. RRave: 729 (648–802) vs. 795 (713–852) ms; cSD2/SD1: 3.4 (2.7–5.0) vs. 2.9 (2.3–3.5); SampEn: 1.5 (1.3–1.8) vs. 1.7 (1.5–1.8); α2: 0.6 (0.3–0.6) vs. 0.5 (0.4–0.5); 2UV: 7.1 (4.3–11.5) vs. 10.8 (6.4–15.7) and nVFR 0.12 (0.11–0.13) vs. 0.10 (0.08–0.12) points/kg, respectively. The nVFR was strongly significantly correlated with several indexes of HRV only in the BCS group.Our findings suggest that BCS exhibit lower parasympathetic cardiac activity and changes in HRV patterns compared to Controls. A concomitant increase of visceral fat, among other factors, may contribute to cardiac autonomic disturbances and changes in HRV patterns in BCS.
Similar content being viewed by others


Introduction
Breast cancer is among the five most common forms of cancer, and it is one of the most important causes of death worldwide, accounting for an estimated 627,000 deaths in 20181. In Latin America, breast cancer ranks as the first cancer type among women regarding new cases and deaths2. These statistics become more relevant in public health since breast cancer can lead to associated diseases and alterations both in early stages and even years after treatment and recuperation. Potential factors, such as metabolic dysregulation and weight gain, are associated with autonomic dysfunction and increased cardiovascular disease risk in patients with breast cancer3. Different studies indicate that breast cancer survivors (BCS) show a stronger association with metabolic syndrome4, diabetes5, and abdominal obesity6, which are major risk factors for cardiovascular disease7.
Taking into account that metabolic modifications are present in BCS, body composition seems to be a factor of interest in breast cancer management, specifically at the tissue level witch refers to amounts and distributions of adipose, skeletal, and muscle tissue in the patients8,9. Interestingly, the study of body composition has been considered as one of the most promising areas in oncology10. Concerning breast cancer, evidence suggests that body composition is a crucial contributor to clinical outcomes after surgery11. In addition, relevant findings indicate that changes in body composition may lead to modifications in the autonomic cardiac function12. It is known that autonomic dysfunction represents a loss of normal autonomic control of the cardiovascular system associated with both increases in sympathetic nervous system activation and reduced efficacy of the parasympathetic nervous system3 that may affect one or more systems of the body13,14.
Recent studies have suggested that an altered cardiac autonomic activity is associated with a high share of adipose tissue15. Other findings have also indicated that BCS may also show an autonomic impairment due to adjuvant therapies16, among other factors. Notably, BCS exhibit numerous dysfunctions: lower parasympathetic cardiac function, lower aerobic fitness, signs of altered metabolism, and higher perception of fatigue17. Data indicate that physical training can reverse impaired cardiorespiratory fitness and autonomic modulation in women with breast cancer receiving adjuvant therapy18.
The heart rate variability (HRV) analysis has been established as a complementary non-invasive and economical tool for the early diagnosis and better prognosis of autonomic cardiac dysfunction and survival in BCS women19. Studies have shown that the presence of a cardiovascular imbalance in BCS compared to healthy controls suggests that traditional linear indexes of HRV study could be clinically valuable for detecting cardiovascular disease in BCS20. Nevertheless, linear HRV analysis techniques are often insufficient to characterize the complex dynamics of the heartbeat generation since the mechanisms involved in cardiovascular regulation probably interact with each other in a nonlinear way21. With this consideration, promising nonlinear tools such as symbolic dynamics and fractal indexes have been introduced to describe the complexity of HRV. Both methodologies are especially useful given that minimize the effects of non-stationarities22,23. The nonlinear methods have shown great promise in the detection and diagnosis of heart failure24 and the evaluation of physical condition and well-being during physical activity tests25. However, in BCS, the nonlinear properties of cardiac dynamics related to changes in the autonomic nervous system (ANS) and complexity have not been fully elucidated.
As far as we know, no other studies have compared autonomic cardiac activity assessed by linear and nonlinear HRV measures in conjunction with various measures of body composition values between BCS and cancer-free women. With this background, this study aims to assess the autonomic cardiac function by nonlinear features of heart fluctuations, and body composition modifications in BCS and women with no cancer diagnosis under similar characteristics. We hypothesized that women who are BCS manifest cardiac autonomic disturbances characterized by a diminished vagal tone related to changes in body composition.
Methods
Study design
In this preliminary cross-sectional study, Mexican women between 30 and 67 years old who attended the Oncology Service at the Regional General Hospital No. 251 of the Mexican Institute of Social Security (Metepec, State of Mexico, Mexico), from March 2019 until July 2019 were invited to participate in this study. The BCS group included women who were in their post-cancer follow-up appointment. The inclusion criteria included the following: (a) previous diagnosis of breast cancer; (b) women who had undergone breast cancer surgery (lumpectomy or mastectomy) anywhere from 1 to 5 years earlier and women who did not require surgery; (c) no evidence of metastases, (d) absence of respiratory and cardiovascular diseases, diabetes mellitus, thyroid dysfunction, and hypertension; (e) normotensive; (f) capacity to stand up unaided, and (g) capacity to answer a clinical interview, including a familiar history of cancer. The exclusion criteria consisted of the following: (a) women under anticancer medication (e.g., tamoxifen26) or any other medication at the moment of the study; (b) women undergoing chemotherapy or radiotherapy (c) women being treated with any other adjuvant therapy, (d) super-obese women (BMI > 50 kg/m2) and (d) smoking women. The elimination criteria involved women whose QRS complex was not feasible to detect due to excessive movement artifacts or low signal voltage.
Moreover, the control group included women without cancer diagnosis with similar characteristics to the BCS group (ethnicity, age, weight, BMI, and height). In all controls, the presence of chronic diseases or pharmacological treatment was excluded by history and standard medical examination.
The sample size estimation was based on the study of Romanholi Palma et al.27 and was determined using the G*Power software28. We considered an 80% test power, an alpha error of 5% for a one-tailed test. The minimum sample size was determined to be 14 participants per group. Specifically, a one-tailed t-test was selected for this preliminary study based on the directional hypothesis that vagal tone is diminished in BCS.
Electrocardiogram recording and preprocessing
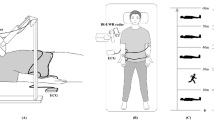
On the day of the study, all participants arrived in the Oncology service, having avoided caffeinated or alcoholic beverages. Electrophysiological recordings were performed between 08:00 a.m. and 12:00 p.m. to account for circadian rhythms of the heartbeat. All participants were asked to relax and record in a standard seated position at rest29. The first lead (DI) of the electrocardiogram (ECG) was recorded for 5 min by using an ECG sensor model EKG-BTA (Vernier®, Beaverton, Oregon, USA) for NI Elvis II (Texas Instruments®, Dallas, Texas, USA) and superficial disposable electrodes. Electrocardiographic data were acquired with a PC at a sampling rate of 1000 Hz using the Biosignal Logger and Player software (National instruments®, Austin, Texas, USA).
Raw ECG recordings for both BCS and Control groups were then processed using previously validated algorithms to generate RR time series30. All the RR time series were reconditioned by a filtering approach to exclude possible artifacts such as ectopic beats, arrhythmic events, and noise effects that may alter the estimation of the HRV31. The reconditioning step includes 60 Hz filtering for line noise elimination and an adaptative filter for artifact correction. All these calculations were obtained using Matlab® software (the MathWorks, Inc. Natick, Massachusetts, USA).
Heart rate variability (HRV) assessment
We assessed HRV according to methodological standards proposed by the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology for HRV32. We used the Kubios software version 3.1 (Kuopio, Finland)25 to analyze some linear and nonlinear measures of the RR time series. The following linear (time-domain) indexes were included: the mean RR interval (RRave), the standard deviation of the RR time series of normal sinus beats (SDNN, a biomarker of global HRV), the root mean square of successive differences (RMSSD), and the percentage of pairs of successive RR intervals that differ by more than 50 ms, these last two biomarkers are associated to the cardiac parasympathetic function32.
Linear (frequency-domain) indexes were also reported, such as the normalized high-frequency (HFnu: 0.15–0.4 Hz). HFnu is a parasympathetic dominance index33. Also, we included a marker of respiratory sinus arrhythmia, quantified as the power of HRV in the high-frequency band (HF: 0.15–0.4 Hz) expressed in absolute units (HF ms2), being an index for vagal modulation of heart rate34,35.
By default, a 4 Hz interpolation was set in the Kubios software. The spectrum for the selected RR time series was computed with Welch's periodogram method (FFT spectrum). Since our signal length is five minutes, we adjusted the window to 128 s with a 50% overlap to have enough windows to estimate the spectral components correctly36.
Furthermore, we performed a nonlinear analysis of HRV. The selection of nonlinear indexes was based on the findings carried out by Maestri et al., who has reported indexes that are not redundant among themselves and provide valuable predictive information37. This study assessed four of the six major families of some nonlinear indexes: Poincaré plots, fractality, entropy, and symbolic dynamics.
Concerning Poincaré plots, we considered the indexes SD1, SD2, and SD1/SD2. SD1 is an index of short-term variability and reflects parasympathetic activity, while the SD2 index measures long-term variability and reflects the overall variability. The (SD1/SD2) ratio represents the balance between long- and short-term HRV38. The quantitative analysis of a plot involves fitting an ellipse to the Poincaré plot, which corresponds to the length of the minor (SD1) and major (SD2) axes.
We considered the following fractal indexes from the detrended fluctuation analysis (DFA) method: the short-term fractal exponent (α1), corresponding to 4–11 beats, and the long-term fractal exponent (α2), ranging from 11 to N/4 beats39. When α = 0.5, there is no correlation, and the time series shows white noise behavior; if α = 1.5, the time series resemble Brownian motion, and if it is 0.5 < α < 1.5, there are positive correlations. If α ≈ 1.0 indicates a fractal-like behavior, if it reaches values above 1.0, the system tends to be less complex and linear40.
The fact that HRV is dependent on mean RR interval (or mean heart rate) is widely recognized. A higher mean RR interval naturally leads to higher variability. In considering this fact, some indexes were normalized (or corrected) to attenuate the mathematical HRV dependence on heart rate41 based on the method proposed by van Roon42 and recommended by de Geus43. Thus, the following indexes were corrected: RMSSD, SDNN, SD1, SD2, and SD1/SD2 ratio, generating the normalized indexes cRMSSD, cSDNN, cSD1, cSD2, and cSD1/SD2 ratio, respectively. The mentioned method for normalization is exemplified in Eq. (1) for the RMSSD. It applies similarly to the rest of the corrected indexes.
Similarly, the spectral index HF (ms2) was corrected according to Sacha et al.41 by dividing the original HF value by RRave squared, thus obtaining cHF.
Regarding the entropy family used to assess the regularity/irregularity of the RR time series, we estimated the sample entropy (SampEn) calculated with m = 2 and r = 0.2, as described by Richman and Moorman44.
Finally, the symbolic dynamics family was evaluated using the PyBioS freeware45 considering 0V, 1V, 2LV, 2UV indexes computed from the sigma method. This family of indexes evaluates the activity of both autonomous branches even when their modulation is not reciprocal46. Symbolic analysis reveals the parasympathetic and sympathetic and modulations on the heart exclusively by the indexes 2UV and 0V, respectively. A full description of this technique is described in Ref.47.
Body composition estimation
Bioelectrical impedance analysis (BIA) is a non-invasive, low-cost, helpful, and validated tool for estimating body composition48. The analysis is achieved by measuring the bioimpedance of an electrical current transmitted to the body through electrodes placed on the feet49. On the day of the study, a body composition analyzer, which employed BIA, was used to estimate body composition (BC-533 InnerScan Body Composition Monitor®, Tanita Corp., Itabashi-Ku Tokyo, Japan). Firstly, the heights of all subjects were measured and recorded. Then, participants were weighed, and body composition values were indirectly estimated using the device. The following body composition measures were collected for the BCS and Control groups: body fat percentage, body water percentage, muscle mass, bone mass, predicted daily calorie intake (DCI), metabolic age, and visceral fat rating (VFR). Particularly, VFR is given as a specific rating: (0–59 points). Ratings from 1 to 12 points indicate that the subject has a healthy level of visceral fat, while ratings from 13 to 59 points indicate that the subject has an excess level of visceral fat. The visceral fat rating has been widely applied in medical research as an indirect visceral fat amount in females50 and mixed-gender groups51. We calculated the normalized visceral fat rating (nVFR) by dividing the visceral fat rating by each participant's body weight.
Ethical considerations
This study was approved by the Research Ethics Committee No. 1503 from the Regional General Hospital No. 251 of the Mexican Institute of Social Security (IMSS). The Federal Commission for Protection Against Health Risks (COFEPRIS) authorizes this committee (authorization no. 17 CI 15 104 037) and the National Research National Commission of Bioethics in Mexico (CONABIO, authorization no. 15 CEI 002 2017033). This protocol was registered under the code R-2019-1503-012. All volunteers in this study signed an Informed Consent Form when they agreed to participate, and all methods were performed in accordance with the relevant guidelines and regulations.
Statistical analysis
The statistical analysis was done with GraphPad Prism version 8.00 for Windows (GraphPad Software, La Jolla, California USA). Descriptive results were presented as median (25th–75th percentile) for quantitative variables and frequency (percentage) for categorical variables. A Shapiro–Shapiro–Wilk test was used to assess the normality of distribution. However, the data did not appear to have a normal distribution. Thus, the continuous variables were compared using one-tailed Mann–Whitney's U tests, and categorical variables were evaluated by Fisher's exact test. Associations between body composition and HRV measures (BCS group) were evaluated by Spearman's correlation coefficient. For all tests, results of p < 0.05 were considered significant.
Results
Of 80 invited BCS women, 20 women were unwilling to participate in the study; 32 women were excluded because they were under chemotherapy, radiotherapy, or medication. Finally, the data of 27 BCS women were analyzed. Thirty-one women without cancer conformed the Control group with similar characteristics to the BCS group. Table 1 shows their general clinical parameters; as was expected, there were no significant differences between both groups (p > 0.05).
Table 2 exhibits the HRV linear and nonlinear indexes, several significant differences (p < 0.05) were found between the BCS and Control groups. RRave: 729 (648–802) vs. 795 (713–852) ms; cSD2/SD1: 3.4 (2.7–5.0) vs. 2.9 (2.3–3.5); SampEn: 1.5 (1.3–1.8) vs. 1.7 (1.5–1.8); α2 0.6 (0.3–0.6) vs 0.5 (0.4–0.5); 2UV: 7.1 (4.3–11.5) vs. 10.8 (6.4–15.7). Notably, the cSD2/SD1 ratio followed by the RRave, and 2UV had lower p-values than other HRV indexes.
Table 3 depicts all the body composition measures indirectly estimated by BIA. Interestingly, only one body composition measure showed statistical differences (p < 0.05) between the BCS and Control groups: nVFR: 0.12 (0.11–0.13) vs. 0.10 (0.08–0.12) points/kg, respectively.
We explored associations between body composition measures and HRV indexes for both groups. Although the mentioned correlations were executed for both groups, only BCS presented significant correlations, showing strong positive and negative associations for nVFR. Table 4a depicts the significant (p < 0.05) Spearman's rank correlation coefficient (ρ) between nVFR and HRV variables for BCS. Notably, BCS's abdominal fat is linked with multiple autonomic and nonlinear features variables. Table 4b exhibits the analogous correlations between nVFR and HRV for the Control group for comparison purposes.
Discussion
This study suggests that women who are BCS manifest cardiac autonomic modifications and HRV pattern changes compared to women with no-cancer diagnosis. BCS were characterized by a reduction of average RR interval and cardiac parasympathetic activity, a modified balance between long- and short-term HRV, lower irregularity of RR time series, and distinct fractal-like behavior. Moreover, a higher amount of visceral fat is likely manifested in BSC compared to control women. Our discussion is structured into three main findings, (1) the changes in the linear and nonlinear measures between BCS and Control women; (2) the differences in body composition in these groups, and (3) the significant correlations between HRV measures and body composition.
Concerning the linear HRV indexes, we found lower RRave values (associated with higher average heart rate) in BCS compared to controls. Generally, changes in RR intervals have been reported in BCS women even 18 years after different adjutant treatments of early breast cancer52. Recent results indicate that elevated heart failure risks have been observed after treatment with anthracyclines and trastuzumab treatment53.
Our results showed a higher cSD2/SD1 ratio in BCS women compared to Controls. Mainly, SD2/SD1 ratio offers information on the relationship between long- and short-term HRV; a higher ratio may reflect a decrease in SD1, an increase in SD2, or both. Following the interpretation of diverse authors for the SD2/SD1 ratio55,38,54, a higher ratio could imply a decreased vagal tone and increased sympathetic influence in BSC than Controls.
On the other hand, symbolic analysis results showed a significant decrease of the 2UV index that proves a diminished cardiac parasympathetic activity in BCS46. It is crucial to consider the importance of the symbolic analysis because these indexes do not suffer the heart rate bias than the linear indexes. Furthermore, a lower irregularity (indicated by SampEn) and different fractal-like behavior of the RR time series (indicated by α2) was found in BCS compared to Control. Lower values of SampEn have been associated with pro-inflammatory processes (e.g., experimental endotoxemia and neonatal sepsis) in preclinical and clinical studies56,57. Evidence indicates that fatigue is associated with a maladaptive autonomic profile characterized by lower parasympathetic activity in cancer survivors. Thus, we speculate that a diminished parasympathetic activity may be reflected as a disrupted cholinergic anti-inflammatory pathway58, resulting in higher inflammation in BCS. There are emerging findings on inflammatory cytokines' role in the recurrence of breast cancer59.
Concerning body composition, interestingly, only the nVFR was different between the BCS and cancer-free women. This result is in line with a previous study in a sample of Iranian women, indicating that most BCS are abdominally obese6. Another study also demonstrated a high incidence of abdominal obesity among BCS from Malaysia60. According to some studies, fat gain is most common for women who undergo menopause because of cancer therapy and is often accompanied by changes in body composition61. Relevant findings suggest that abdominal adiposity could adversely affect the sympathetic and parasympathetic function62. Other findings suggest that an excess of visceral fat is associated with sympathetic activation63.
According to the consulted literature, no studies have been conducted for evaluating the associations between central adiposity and linear and nonlinear indexes of HRV in BCS. In this study, we observed significant negative associations between visceral adiposity measured by BIA and cardiac parasympathetic function at BCS (indicated by cRMSSD, pNN50, 2UV, HFnu, cHF, and cSD1) and global heart rate variability (indicated by cSDNN). Moreover, we found significant positive associations between visceral adiposity and sympathetic function (indicated by 0V), fractal scaling properties (indicated by α1 and α2), and the balance between long- and short-term HRV (indicated by cSD2/SD1 ratio). These results are consistent with previous studies that demonstrate that central adiposity influences cardiac autonomic modulation of obese persons, increasing the risk of cardiovascular diseases64. Thus, we consider that a concomitant increase of visceral fat, among other factors, may contribute to cardiac autonomic modifications and changes in HRV patterns in women who are BCS.
This study found significant correlations between nVFR and HRV measures only in BCS (but not in Controls). It could be explained by the relevant role of intra-abdominal fat to influence cardiac autonomic disturbances in this specific condition, given that nVFR was the only significantly different body composition measure between the two groups. It is also essential to take into account the possibility that the ANS alterations on BCS also may be related to additional mechanisms not exclusively related to visceral fat (e.g., reduced number of control mechanisms regulating sinus node activity, loss in the exchange of information between cardiovascular subsystems, or to increased activity of one of these subsystems65 indicated by SampEn and α2).
The HRV and VFR are promising tools for evaluating the ANS and body composition in BCS, respectively. These low-cost, affordable, and non-invasive tools can be routinely monitored in BCS for a clinical assessment or control of exercise training. Exercise training has mainly shown increment muscle strength, endurance, flexibility, decreased body fat percentage, waist circumference, and visceral fat area in cancer survivors66. Alternative therapies such as massages67 and mindfulness68 lead to an immediate increase of HRV, reduce inflammation, and improve BCS mood with cancer-related fatigue.
Limitations
A small sample size limits this preliminary study; our findings and interpretation should be confirmed in further clinical explorations with a larger population. Nonetheless, previous studies have confirmed that even with a small number of participants (N = 15), it is possible to detect significant differences in some indexes of HRV of BCS27. We recognize that Poincaré indexes and symbolic dynamics are superior that linear indexes to identify autonomic-related changes in BCS.
Additionally, the beat-to-beat change seen in the RR time series is not only under ANS influence. Humoral factors and respiratory variation may also play a role. Given the study's cross-sectional nature, it is unknown whether some observed differences had already been present before breast cancer treatment. At this stage, it is not possible to determine the causality between autonomic cardiac alterations and visceral fat. However, according to our results, we suggest that visceral fat and autonomic disturbances are highly related to BCS.
Although the decrease in parasympathetic function is mild in BCS than in Controls (2UV, p = 0.03), the BCS participants have, on average, four years after completion of chemotherapy, surgery, or medications. Thus, BCS women may be long-term repercussions in their autonomic activity, and it is likely related to a chronic inflammation process reported in BCS69.
In this study, we selected a simple method for correcting the HRV indexes, however, it is important to mention that some other studies have already explored new robust methods to attenuate the mean heart rate bias in linear and nonlinear HRV indexes70,71. We will explore these relevant methods in future work as well as studying other indexes such as fatigue, stress, or anxiety, which are shown to induce changes in HRV72,73 and might help explain the differences observed between the groups. Additional future work will involve applying the ECG-Derived respiration technique and the quantification of cardio-respiratory coupling in BCS data.
Conclusions
Women who are BCS exhibited changes in HRV compared to controls; it included: (a) lower average RR intervals, (b) lower parasympathetic cardiac activity (as indicated by 2UV), a modified balance between long- and short-term HRV, and a lower irregularity of RR time series (indicated by cSD2/SD1 and SampEn, respectively) and different fractal-like behavior (indicated by α2). Additionally, survivors may have an increase in visceral fat compared to control women. Thus, a concomitant increase of visceral fat, among other factors, may contribute to cardiac autonomic disturbances and changes in HRV patterns in BCS. The visceral fat and HRV may be valuable biomarkers for monitoring breast cancer survivors' health and well-being.
References
World Health. WHO|Breast cancer. WHO (Accessed 01 November 2020); https://www.who.int/cancer/prevention/diagnosis-screening/breast-cancer/en/ (2018).
PAHO/WHO. Breast Cancer. (Accessed 10 December 2020); https://www.paho.org/hq/index.php?option=com_content&view=article&id=5041:2011-breast-cancer&Itemid=3639&lang=en (2020).
Lakoski, S. G., Jones, L. W., Krone, R. J., Stein, P. K. & Scott, J. M. Autonomic dysfunction in early breast cancer: Incidence, clinical importance, and underlying mechanisms. Am. Heart J. https://doi.org/10.1016/j.ahj.2015.05.014 (2015).
Buttros, D. D. A. B. et al. Risk of metabolic syndrome in postmenopausal breast cancer survivors. Menopause 20, 448–454 (2013).
Hamood, R., Hamood, H., Merhasin, I. & Keinan-Boker, L. Diabetes after hormone therapy in breast cancer survivors: A case-cohort study. J. Clin. Oncol. https://doi.org/10.1200/JCO.2017.76.3524 (2018).
Mohammadi, S., Sulaiman, S., Koon, P. B., Amani, R. & Hosseini, S. M. Association of nutritional status with quality of life in breast cancer survivors. Asian Pac. J. Cancer Prev. https://doi.org/10.7314/APJCP.2013.14.12.7749 (2013).
Mehta, L. S. et al. Cardiovascular disease and breast cancer: Where these entities intersect: A scientific statement from the American Heart Association. Circulation https://doi.org/10.1161/CIR.0000000000000556 (2018).
Deluche, E. et al. Impact of body composition on outcome in patients with early breast cancer. Support. Care Cancer https://doi.org/10.1007/s00520-017-3902-6 (2018).
Duren, D. L. et al. Body composition methods: Comparisons and interpretation. J. Diabetes Sci. Technol. 2, 1139–1146 (2008).
Brown, J. C., Cespedes Feliciano, E. M. & Caan, B. J. The evolution of body composition in oncology-epidemiology, clinical trials, and the future of patient care: Facts and numbers. J. Cachexia. Sarcopenia Muscle 9, 1200–1208 (2018).
Liu, L.-N., Lin, Y.-C., Miaskowski, C., Chen, S.-C. & Chen, M.-L. Association between changes in body fat and disease progression after breast cancer surgery is moderated by menopausal status. BMC Cancer 17, 863 (2017).
León-Ariza, H. H., Botero-Rosas, D. A. & Zea-Robles, A. C. Heart rate variability and body composition as VO2max determinants. Rev. Bras. Med. Esporte https://doi.org/10.1590/1517-869220172304152157 (2017).
Colombo, J., Arora, R., DePace, N. L. & Vinik, A. I. Clinical autonomic dysfunction: Measurement, indications, therapies, and outcomes. Clin. Auton. Dysfunct. Meas. Indic. Ther. Outcomes https://doi.org/10.1007/978-3-319-07371-2 (2015).
De Couck, M. & Gidron, Y. Norms of vagal nerve activity, indexed by Heart Rate Variability, in cancer patients. Cancer Epidemiol. https://doi.org/10.1016/j.canep.2013.04.016 (2013).
Smoljo, T. et al. The relationship between autonomic regulation of cardiovascular function and body composition. J. Obes. Metab. Syndr. 29, 188–197 (2020).
Lucini, D. et al. Endocrine adjuvant therapy might impair cardiac autonomic regulation in breast cancer survivors. Cardiol. Cardiovasc. Med. 03, 34–49 (2019).
Vigo, C. et al. Evidence of altered autonomic cardiac regulation in breast cancer survivors. J. Cancer Surviv. 9, 699–706 (2015).
Mostarda, C. et al. Short-term combined exercise training improves cardiorespiratory fitness and autonomic modulation in cancer patients receiving adjuvant therapy. J. Exerc. Rehabil. 13, 599–607 (2017).
Arab, C. et al. Heart rate variability measure in breast cancer patients and survivors: A systematic review. Psychoneuroendocrinology 68, 57–68 (2016).
Caro-Morán, E. et al. Heart rate variability in breast cancer survivors after the first year of treatments: A case-controlled study. Biol. Res. Nurs. https://doi.org/10.1177/1099800414568100 (2016).
Fernandes de Godoy, M. Nonlinear analysis of heart rate variability: A comprehensive review. J. Cardiol. Ther. https://doi.org/10.17554/j.issn.2309-6861.2016.03.101-4 (2016).
Magagnin, V. et al. Non-stationarities significantly distort short-term spectral, symbolic and entropy heart rate variability indices. Physiol. Meas. 32, 1775–1786 (2011).
Buccelletti, F. et al. Linear and nonlinear heart rate variability indexes in clinical practice. Comput. Math. Methods Med. 2012, 1–5 (2012).
Tsai, C. H. et al. Usefulness of heart rhythm complexity in heart failure detection and diagnosis. Sci. Rep. https://doi.org/10.1038/s41598-020-71909-8 (2020).
Solís-Montufar, E. E., Gálvez-Coyt, G. & Muñoz-Diosdado, A. Entropy analysis of RR-time series from stress tests. Front. Physiol. 11, 1–15 (2020).
Borgo, M. V. et al. Effect of tamoxifen on the coronary vascular reactivity of spontaneously hypertensive female rats. Braz. J. Med. Biol. Res. https://doi.org/10.1590/S0100-879X2011007500099 (2011).
Palma, M. R. et al. The relationship between post-operative time and cardiac autonomic modulation in breast cancer survivors. Int. J. Cardiol. https://doi.org/10.1016/j.ijcard.2016.09.053 (2016).
Erdfelder, E., Faul, F., Buchner, A. & Lang, A. G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav Res. Methods https://doi.org/10.3758/BRM.41.4.1149 (2009).
Young, F. L. S. & Leicht, A. S. Short-term stability of resting heart rate variability: Influence of position and gender. Appl. Physiol. Nutr. Metab. 36, 210–218 (2011).
Echeverria, J. C., Ortiz, R., Ramirez, N., Medina, V. & Gonzalez, R. A reliable method for abdominal ECG signal processing. Comput. Cardiol. 25, 1–3 (1998) (Cat. No.98CH36292).
Wessel, N. et al. Nonlinear analysis of complex phenomena in cardiological data. Herzschrittmachertherapie und Elektrophysiologie 11, 159–173 (2000).
Malik, M., Bigger, J., Camm, A. & Kleiger, R. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur. Heart J. 17, 354–381 (1996).
Burr, R. L. Interpretation of normalized spectral heart rate variability indices in sleep research: A critical review. Sleep https://doi.org/10.1093/sleep/30.7.913 (2007).
Hirsch, J. A. & Bishop, B. Respiratory sinus arrhythmia in humans: How breathing pattern modulates heart rate. Am. J. Physiol. Hear. Circ. Physiol. 10, 620–629 (1981).
Shaffer, F. & Ginsberg, J. P. An overview of heart rate variability metrics and norms. Front. Public Health. https://doi.org/10.3389/fpubh.2017.00258 (2017).
Tarvainen, M. P., Niskanen, J.-P., Lipponen, J. A., Ranta-Aho, P. O. & Karjalainen, P. A. Kubios HRV—Heart rate variability analysis software. Comput. Methods Programs Biomed. 113, 210–220 (2014).
Maestri, R. et al. Nonlinear indices of heart rate variability in chronic heart failure patients: Redundancy and comparative clinical value. J. Cardiovasc. Electrophysiol. 18, 425–433 (2007).
Guzik, P. et al. Correlations between the Poincaré plot and conventional heart rate variability parameters assessed during paced breathing. J. Physiol. Sci. https://doi.org/10.2170/physiolsci.RP005506 (2007).
Huikuri, H. V. et al. Fractal correlation properties of R-R interval dynamics and mortality in patients with depressed left ventricular function after an acute myocardial infarction. Circulation 101, 47–53 (2000).
Peng, C. K., Havlin, S., Stanley, H. E. & Goldberger, A. L. Quantification of scaling exponents and crossover phenomena in nonstationary heartbeat time series. Chaos 5, 82–87 (1995).
Sacha, J. Interaction between heart rate and heart rate variability. Ann. Noninvasive Electrocardiol. 19, 207–216 (2014).
Van Roon, A. M., Snieder, H., Lefrandt, J. D., De Geus, E. J. C. & Riese, H. Parsimonious correction of heart rate variability for its dependency on heart rate. Hypertension 68, e63–e65 (2016).
de Geus, E. J. C., Gianaros, P. J., Brindle, R. C., Jennings, J. R. & Berntson, G. G. Should heart rate variability be “corrected” for heart rate? Biological, quantitative, and interpretive considerations. Psychophysiology 56, 1–26 (2019).
Richman, J. S. & Moorman, J. R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 278, H2039–H2049 (2000).
Silva, L. E. V., Fazan, R. & Marin-Neto, J. A. PyBioS: A freeware computer software for analysis of cardiovascular signals. Comput. Methods Programs Biomed. 197, 105718 (2020).
Porta, A. et al. Assessment of cardiac autonomic modulation during graded head-up tilt by symbolic analysis of heart rate variability. Am. J. Physiol. Circ. Physiol. https://doi.org/10.1152/ajpheart.00006.2007 (2007).
Cysarz, D. et al. Quantifying heart rate dynamics using different approaches of symbolic dynamics. Eur. Phys. J. Spec. Top. 222, 487–500 (2013).
Guida, B. et al. Bioelectrical impedance analysis and age-related differences of body composition in the elderly. Nutr. Metab. Cardiovasc. Dis. 17, 175–180 (2007).
Long, V., Short, M., Smith, S., Sénéchal, M. & Bouchard, D. R. Testing bioimpedance to estimate body fat percentage across different hip and waist circumferences. J. Sports Med. 2019, 1–5 (2019).
Fernandez-Garcia, J. C. et al. An increase in visceral fat is associated with a decrease in the taste and olfactory capacity. PLoS ONE 12, e0171204 (2017).
Puri, A., Singh, V., Pandey, S., Singh, C. K. & Singh, S. R. K. Visceral fat rating is a useful indicator in risk assessment among coronary artery disease patients treated with aggressive lipid lowering therapy. Clin. Epidemiol. Glob. Health. https://doi.org/10.1016/j.cegh.2013.11.002 (2014).
De Azambuja, E. et al. Cardiac assessment of early breast cancer patients 18 years after treatment with cyclophosphamide-, methotrexate-, fluorouracil- or epirubicin-based chemotherapy. Eur. J. Cancer https://doi.org/10.1016/j.ejca.2015.08.011 (2015).
Boekel, N. B. et al. Heart failure after treatment for breast cancer. Eur. J. Heart Fail. https://doi.org/10.1002/ejhf.1620 (2020).
Goit, R. K., Pant, B. N. & Shrewastwa, M. K. Moderate intensity exercise improves heart rate variability in obese adults with type 2 diabetes. Indian Heart J. https://doi.org/10.1016/j.ihj.2017.10.003 (2018).
Goit, R. K., Jha, S. K. & Pant, B. N. Alteration of cardiac autonomic function in patients with newly diagnosed epilepsy. Physiol. Rep. 4, e12826 (2016).
Reyes-Lagos, J. J. et al. Exogenous oxytocin reduces signs of sickness behavior and modifies heart rate fluctuations of endotoxemic rats. Physiol. Behav. 165, 223–230 (2016).
Lake, D. E., Richman, J. S., Pamela Griffin, M. & Randall Moorman, J. Sample entropy analysis of neonatal heart rate variability. Am. J. Physiol. Regul. Integr. Comp. Physiol. https://doi.org/10.1152/ajpregu.00069.2002 (2002).
Huston, J. M. & Tracey, K. J. The pulse of inflammation: Heart rate variability, the cholinergic anti-inflammatory pathway and implications for therapy. J. Intern. Med. 269, 45–53 (2011).
Ma, Y. et al. IL-6, IL-8 and TNF-α levels correlate with disease stage in breast cancer patients. Adv. Clin. Exp. Med. https://doi.org/10.17219/acem/62120 (2017).
Yaw, Y. H. et al. Weight changes and lifestyle behaviors in women after breast cancer diagnosis: A cross-sectional study. BMC Public Health https://doi.org/10.1186/1471-2458-11-309 (2011).
Gadéa, E., Thivat, E., Planchat, E., Morio, B. & Durando, X. Importance of metabolic changes induced by chemotherapy on prognosis of early-stage breast cancer patients: A review of potential mechanisms. Obes. Rev. https://doi.org/10.1111/j.1467-789X.2011.00957.x (2012).
Windham, B. G. et al. The relationship between heart rate variability and adiposity differs for central and overall adiposity. J. Obes. https://doi.org/10.1155/2012/149516 (2012).
Hillebrand, S. et al. Body fat, especially visceral fat, is associated with electrocardiographic measures of sympathetic activation. Obesity 22, 1553–1559 (2014).
Oliveira, C. et al. Risk factors associated with cardiac autonomic modulation in obese individuals. J. Obes. https://doi.org/10.1155/2020/7185249 (2020).
Porta, A., Rienzo, M. D., Wessel, N. & Kurths, J. Addressing the complexity of cardiovascular regulation. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 367, 1215–1218 (2009).
Kim, T. H. et al. Effects of exercise training on circulating levels of Dickkpof-1 and secreted frizzledrelated protein-1 in breast cancer survivors: A pilot single-blind randomized controlled trial. PLoS One https://doi.org/10.1371/journal.pone.0171771 (2017).
Fernández-Lao, C. et al. Attitudes towards massage modify effects of manual therapy in breast cancer survivors: A randomised clinical trial with crossover design. Eur. J. Cancer Care (Engl.) 21, 233–241 (2012).
Rådmark, L., Sidorchuk, A., Osika, W. & Niemi, M. A systematic review and meta-analysis of the impact of mindfulness based interventions on heart rate variability and inflammatory markers. J. Clin. Med. 8, 1638 (2019).
Van Der Willik, K. D. et al. Inflammation markers and cognitive performance in breast cancer survivors 20 years after completion of chemotherapy: A cohort study. Breast Cancer Res. 20, 135 (2018).
Bailón, R. et al. The integral pulse frequency modulation model with time-varying threshold: Application to heart rate variability analysis during exercise stress testing. IEEE Trans. Biomed. Eng. 58, 642–652 (2011).
Bolea, J., Pueyo, E., Orini, M. & Bailón, R. Influence of heart rate in non-linear HRV indices as a sampling rate effect evaluated on supine and standing. Front. Physiol. 7, 501 (2016).
Chalmers, J. A., Quintana, D. S., Abbott, M. J. A. & Kemp, A. H. Anxiety disorders are associated with reduced heart rate variability: A meta-analysis. Front. Psychiatry 5, 80 (2014).
Kim, H. G., Cheon, E. J., Bai, D. S., Lee, Y. H. & Koo, B. H. Stress and heart rate variability: A meta-analysis and review of the literature. Psychiatry Investig. 15, 235–245 (2018).
Acknowledgements
The participation of volunteers and staff from the Regional General Hospital No. 251 of the Mexican Institute of Social Security (IMSS) is gratefully acknowledged, especially to Dr. Alejandro Esquivel Loza and Dr. Jesús Alcantar Ramírez. We greatly appreciate the financial support (Grant number: 4755-2019-CIB) from the Research and Advanced Studies Board of Universidad Autónoma del Estado de México.
Author information
Authors and Affiliations
Contributions
D.E-R. and J.J.R-L. designed the study. D.E-R., J.J.G-G., G.E.L-C. and A.G-V. helped with subject recruitment and data collection. D.E-R. and J.J.R-L analyzed the data. D.E-R. and J.J.R-L. wrote the first draft of the manuscript. A.E.-.P., D.E-R., A.C.P-C., J.J.G-G. and J.J.R-L. discussed the results, reviewed and edited the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Escutia-Reyes, D., de Jesús Garduño-García, J., Emilio-López-Chávez, G. et al. Differences in heart rate variability and body composition in breast cancer survivors and women without cancer. Sci Rep 11, 14460 (2021). https://doi.org/10.1038/s41598-021-93713-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-93713-8
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
