
Abstract
Using ArcGIS to analyze satellite derived PM2.5 estimates, this paper obtains the average concentration and maximum concentration of fine particulate matter (PM2.5) in China's 31 provinces from 2002 to 2015. We adopt fixed effects model and spatial Durbin model to investigate the association between PM2.5 and perinatal mortality rates. The results indicate that PM2.5 has a significantly positive association with perinatal mortality rates. A 1% increase of log-transformed average concentration and maximum concentrations of PM2.5 is associated with 1.76‰ and 2.31‰ increase of perinatal mortality rates, respectively. In spatial econometrics analysis, we find PM2.5 has significant spatial autocorrelation characteristics. The concentrations of log-transformed average and maximum PM2.5 increase 1% is associated with a 2.49% increase in a 2.49‰ and 2.19‰ increase of perinatal mortality rates, respectively. The potential mechanism is that air pollution has an impact on infant weight to impact perinatal mortality rates.
Similar content being viewed by others

Introduction
With the rapid growth of the economy, the environment pollution has become a serious issue in China. According to data of the Ministry of Environmental Protection, the average fine particulate matter (PM2.5) concentrations reached 72 µg/m3 in 2013. Therefore, 99% of the China’s population lived in areas exceeding the World Health Organization (WHO) Air Quality Guideline of 10 µg/m3 PM2.51,2. According to the Asian Development Bank (ADB) Annual Report 2012, less than 1% of China’s 500 biggest cities is up to the WHO standards, and seven cities in China list among the ten most polluted cities in the world3. China has become one of countries with the highest environmental burden of disease in the world4. The Institute for Health Metrics and Evaluation Global of Disease in 2012 estimates that outdoor air pollution contributes to 1.20 million premature deaths in China, and air pollution is the fourth leading cause of premature deaths in 67 risk factors5. In addition, outdoor air pollution in China is responsible for 12.34 million deaths and 25 million healthy life-years lost per year. The frequency of severe air pollution events has spurred widespread concern about the environment among citizens and scholars.
A great number of studies find a significant and negative relationship between air pollution and health. The levels of PM2.5 in the air are associated with the risk of deaths from all causes6. Based on the national database of air pollution and mortality for the 88 largest U.S. cities for the period of 1987–1994, which concluded that previous-day PM10 concentrations are positively associated with total mortality in most locations, Dominici et al.7 find that the mortality rate increased by 0.5% for every µg/m3 increase of PM10. Wong et al.8 and Fang et al.9 come to a similar conclusion in studying the effects of air pollution on mortality in Asia and China. Using prefectural panel data from China, Chen and Chen10 find that a 1% increase in gas emission leads to an increase in the number of deaths from respiratory diseases and lung cancer by 0.05‰ and 0.03‰, respectively. Pope et al.11 find that each 10 µg/m3 elevation in fine particulate air pollution is associated with approximately a 4%, 6%, and 8% increased risk of all-cause, cardiopulmonary and lung cancer mortality, respectively.
The carrier of air pollutants such as PM2.5 has been linked to lung and cardiovascular diseases, which increase mortality rates12,13,14,15,16. A number of studies investigate mechanisms through which air pollution causes diseases. Kampa and Castanas17 find that air pollution has both acute and chronic effects on human health by affecting a number of different systems and organs. Tallon et al.18 find that exposures to long-term PM2.5 and NO2 are associated with decreased cognitive function in a cohort of older Americans. Individuals who experience a stroke or elevated anxiety are more susceptible to the effects of PM2.5 on cognition.
There is also an important literature which mainly studies the concentration response curve between air pollution and mortality. Its main conclusion is that the concentration response curve between air pollution and mortality is not linear, but nonlinear. In view of this nonlinear relationship, some scholars estimate the logarithm of air pollution and get the relationship between the growth rate of pollution and mortality19,20,21. Liu et al.22 estimated the shape of concentration–response curves of ballistic "S" curve between PM2.5 and cardiopulmonary disease mortality, which was linear in the range of low to medium PM2.5 and flattened in the range of high PM2.5. The current literature mainly studies the concentration response curve between adult or child mortality and air pollution, but there is little research on the response curve between perinatal mortality and air pollution. Therefore, based on the existing research gaps, this paper focuses on the concentration response curve between perinatal mortality and air pollution.
There is also a literature to study that the different groups of individuals are affected by air pollution in different ways. Vulnerable population, such as children, are more susceptible to the adverse effects of exposure to air pollution than others are. A number of studies examine the adverse health effects of ambient air pollution on kids. Chay & Greenstone23 take the significant drop in the level of air pollution caused by the U.S. economic recession of 1981–1982 as an external shock. They conclude that a 1% reduction in total suspended particulates (TSPs) leads to a 0.35% decline in the infant mortality rate at the county level, implying that 2,500 fewer infants died during 1980–1982 than would have in the absence of the TSPs reductions. Chay and Greenstone24 find that after the implementation of the 1970 Clean Air Act in the U.S, the air quality has been improved and infant mortality rate has also decreased to a certain extent. Currie and Neidell25 examine the impact of three criteria pollutants on infant death in California over the 1990s. Reductions in carbon monoxide over the 1990s saved approximately 1000 infant lives in California. Currie et al.26 find negative association with exposure to CO on infant health.
If a mother during pregnancy is exposed to increased environmental stressors, it could result in an increased risk of fetal growth restriction or a preterm birth, which are strong predictors for infant mortality and morbidity27,28. DeFranco et al.29 find that exposure to high levels of PM2.5 in the third trimester of pregnancy is associated with a 42% increase in stillbirth risk. Faiz et al.30 find that the relative odds of stillbirth are associated with interquartile range increases in the mean pollutant concentrations on lag day 2 and lag days 2–6 before delivery.
The above studies demonstrate the relationship between air pollution and infant mortality. There are also some literatures on the relationship between air pollution and perinatal mortality. For example, Woodruff et al.31 use 4 million infants born between 1989 and 1991 in the 86 metropolitan statistical areas (MSAs) in the United States to find that the particulate matter is associated with risk of post neonatal mortality; De Medeiros et al.32 studied the relationship between traffic-induced air pollution and perinatal mortality rates through case studies; Hackley et al.33 study the impact that exposure to air pollution has on the health of a pregnancy and offer suggestions on how to minimize exposures.
In this study, we aim to test the hypothesis that exposure to PM2.5 in the air during pregnancy is associated with the perinatal mortality rate. Perinatal mortality is an indicator of mother and child health and may reflect the conditions of reproductive health34,35. Using data of China’s provincial level PM2.5 concentrations from 2002 to 2015, we adopt both fixed effects model and spatial Durbin model (SDM) to investigate the relationship between PM2.5 and the perinatal mortality rates. This paper contributes to the literature in several respects. First, many studies on China examine the association between some pollutants, such as CO, PM10, SO2 and health; however, few studies investigate the effect of PM2.5 on mortality. We enrich existing literature by examining the effect of pollutants on mortality rates. Second, we contribute to literature that examines the association between air pollution and perinatal death rates. The prenatal stage of life is a very sensitive period such that exposure to PM2.5 pollutions might have an adverse effect on the development of fetuses. Third, we adopt spatial panel model to analyze the spatial autocorrelation of PM2.5 pollutions among Chinese provinces and demonstrate time and space lag association between PM2.5 pollutions and health.
The paper is organized as follows. “Methodology” section explains our methodology. “Data” section describes the data. “Results” section presents regression results. “Conclusions and discussion” section is the discussion.
Methodology
We use fixed effects model and spatial econometrics model to estimate the relationship between PM2.5 and infant mortality rates.
Fixed effects model
We use the following baseline econometric model:
In the above, i and t indicate the region i and year t, respectively; \(mortality\) is the perinatal mortality rates; province is the province fixed effects; year represents year fixed effects; and \(\varepsilon\) is the random disturbance term (In empirical research, we use clustered standard errors at the province level). \(\left( {{\text{ln}}PM_{2.5} } \right)_{i,t - 1}\) is the natural logarithms of one-year-lagged PM2.5, β is the estimated coefficient of interest. \(X^{\prime}\) represents a vector of control variables, including the total number of health agencies per 10,000 people, the total number of health beds per 10,000 population and gross domestic product (GDP) per capita.
Spatial econometrics model
Shao et al.36 show that PM2.5 pollution has significant spatial autocorrelation characteristics, which indicates that the perinatal mortality rates are affected not only by the local PM2.5 pollution, but also the neighborhood PM2.5 pollution. Therefore, we use a spatial econometric approach to investigate the relationship between PM2.5 and the perinatal mortality rates.
The most commonly used spatial econometric models in applied research are the spatial lag model (SLM), the spatial error model (SEM) and the SDM model37. The SDM model includes spatial lag terms from dependent variables and independent variables to capture the spillover effects deriving from different variables, which is used widely in environment research38,39.
We estimate the following SDM specification:
where W is the spatial weighting matrix; \(Wmortality\) represents perinatal mortality rates in neighboring areas; \(W\left( {\ln PM_{2.5} } \right)_{i,t - 1}\) represents the natural logarithms of one-year-lagged PM2.5 in neighboring areas; \(WX^{\prime}\) is a vector of control variables in neighboring areas; \(\rho\) is the spatial autoregressive parameter; \(\varphi\) is the coefficient of neighboring PM2.5 effecting on local influence; \(\gamma\) and \(\phi\) are the parameters of the two matrices, respectively; and \(\varepsilon\) obeys normal distribution with standard deviation of \(\theta \,\).
To study the spatial distribution of perinatal mortality rates in 31 province-level regions, the spatial weight matrix W needs to be defined first. There are many specifications for spatial weighting matrix, such as spatial contiguity weights, inverse distance matrix and socio-economic distance matrix, but the most commonly used one is the binary contiguity matrix. In this study, we choose the specification of binary contiguity to create the spatial weight matrix W. The elements of spatial weight matrix W are defined as Wij = 1 if location i is adjacent to location j. It is convenient to normalize spatial weights to remove dependence on extraneous scale factors. Therefore, row-normalized weight matrices are used in the study.
To investigate the spatial clustering pattern of PM2.5 and perinatal mortality rates, we calculate Moran’s I index, which is the correlation coefficient of observed values and spatial lagged variables. The value of Moran’s I index is between -1 and 1, with positive values implying positive spatial autocorrelation, negative values implying negative spatial autocorrelation and a zero-value indicating a random spatial pattern. The formula for calculating Moran’s I index is as follows:
where \(S^{2} = \sum {_{i = 1}^{n} (x_{i} - \overline{x})^{2} /N} , \, \overline{x}{ = }\sum {_{i = 1}^{n} x_{i} /N}\); \(x_{i}\) represents mortality rates of region \(i\); \(N\) is the number of samples; and Wij is the spatial weighting matrix.
Data
Perinatal mortality rates
World Health Organization (WHO) defines a perinatal death as ‘a death occurring at 22 weeks completed weeks of gestation and over, during childbirth and up to seven completed days of life’.
In this paper, the definition of perinatal mortality rate is the ratio of neonatal mortality (including stillbirths) from 28 weeks of gestation to 7 days after delivery to live births (Unit is ‰). Data on perinatal mortality rates is from China Health and Family Planning Statistical Yearbook.
Main explanatory variable (PM2.5)
In China, the main sources of air pollution data are data on (TSPs (before 2013 and Air Quality Index (AQI, after 2013). The TSP is a comprehensive index, with only a few cities as monitoring cities. The AQI level is based on the level of six atmospheric pollutants, which covers most major cities in China, but no data is available before 2013. We downloaded the data from the Socioeconomic Data and Applications Center, hosted by the Center for International Earth Science Information Network (CIESIN) at Columbia University. Accordance to research of Van Donkelaar et al.40,41, the data is a hybrid product with inputs including Aerosol Optical Depth measured by satellites and a chemical transport modeling component that uses baseline emissions data to model the movement of pollution. The dataset contains information on three-year running mean of PM2.5 concentrations for 0.01° × 0.01° grids from 1998 to 2016. Adjacent grid points are approximately 10 km apart. We use ArcGIS software to extract PM2.5 estimates data of years from 2002 to 2015. For each province-year observation, we calculate the average and maximum PM2.5 concentration using the data of the grid points that fall within the province42. We take the average value of PM2.5 concentrations as province's annual air pollution level. It should be pointed out that the satellite data in the monitoring process will be affected by meteorological factors, which is slightly lower than the actual ground monitoring data. However, compared to the ground monitoring using "point to surface" measure, the satellite data is relatively reasonable. Therefore, we perform a robustness test using maximum PM2.5 concentrations as the air pollution measure. Referring to method of Van Donkelaar et al.41,42, Hammer et al.43 re-estimate the PM2.5 data concluding the provinces, cities and counties data in China from 2000 to 2018, which can be obtained from Atmospheric Composition Analysis Group in Dalhous University. This data is used to test the robustness.
Other explanatory variables
According to the literature44, we control the following variables.
Regional medical conditions. We control for the number of hospital beds per ten thousand persons (bed_pop) and the number of hospital agencies per ten thousand persons (ha_pop) at the province level, which represent the availability of health care.
Regional economic development level. Regional economy provides the necessary material and nonmaterial support for decreasing perinatal mortality. We assume the higher the level of regional economic development is, the larger the health care spend is. So, a negative relationship between regional economic development and perinatal mortality is expected. In this paper, per capita actual gross domestic product (GDP) is used as a proxy for regional economic development, which is inflation-adjusted by constant 2002 prices.
Urbanization rate. It is the proportion of population in urban areas in a province. It is related to the social economic status (SES) of citizens, such as economic status and education. The higher the urban rate is, the higher the SES of citizens is, and the more attention will be paid to health, resulting in lower perinatal mortality rates. However, higher urban rate will also lead to serious air pollution, which might have a negative effect on perinatal mortality rates.
The above data are available from China Statistical Yearbook, China Health and Family Planning Statistical Yearbook, China Urban Statistical Yearbook and China Regional Economic Statistical Yearbook.
Descriptive statistics
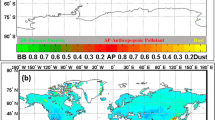
We construct data of China’s 31 provinces from 2002 to 2015. The descriptive statistics of data is provided in Table 1. Figure 1 shows the spatial distribution of PM2.5 in 2002 and 2015 (µg/m3). The maximum and average value of PM2.5 are higher than Air Quality Guideline (10 µg/m3) of the WHO.

Spatial distribution of PM2.5 in 2002 and 2015 (µg/m3), respectively. The left two maps are the spatial distribution maps of average PM2.5 pollution concentration in 31 provinces in 2002 and 2015, respectively, and the right two maps are the spatial distribution maps of maximum PM2.5 pollution depth in 31 provinces in 2002 and 2015, respectively. Maps generated in ArcGIS 10.3.
Results
Fixed effects model
Baseline model
Fixed effects model is used based on the Hausman test. Table 2 displays the results of the baseline model (1). Column (1) and Column (2) reports the results of the impacts of average concentrations of PM2.5 on perinatal mortality rates controlling for only province fixed effects or both province and year fixed effects. Column (3) and (4) include all controls on the basis of the first two columns. The estimate coefficients of the log value of PM2.5 are 2.439, 2.759, 1.644 and 1.76, respectively, which are positive and significant. Column (4) is our referred model, which shows that for every 1% increase in (log) pollution, we find an associated 1.76% increase in perinatal mortality rates.
The association with the average PM2.5 concentrations and the perinatal mortality in the Column (4) might be underestimated because of measurement error. Therefore, we define maximum concentrations of PM2.5 as a measure of PM2.5 pollutions for re-estimate the association. The results are presented in Table 3. After controlling covariates, the results in column (5) show that maximum concentrations of PM2.5 have a significant and positive association with the perinatal mortality rates. A 1% increase of the log value of maximum concentrations of PM2.5 is association with 2.312‰ increase of perinatal mortality rates. The association with the maximum PM2.5 concentrations and the perinatal mortality is stronger.
The coefficient of the GDP (log) per capita is -5.161 in Column (4), which is negative at the 1% significance level, meaning that a 1% increase of the log value of GDP per capita results in 5.16‰ increase of perinatal mortality rates. The coefficient of bed_ number of hospital beds per ten thousand persons and the number of hospital agencies per ten thousand persons are -0.076 and -0.106 respective, which mean they and are negatively related to perinatal mortality rates (shown in Column (4)), which shows that the improvement of access to healthcare is conducive to reducing mortality rates. The coefficients of urbanization rates are insignificant.
Robustness check
Considering the PM2.5 data updated by hammer et al.44, this paper uses the updated PM2.5 data for estimation, and the estimation results are presented in column (1) and column (2) of Table 3. The results show that the estimated coefficient of the new PM2.5 data has a certain decline, but it is still significantly positive, indicating that the positive association with PM2.5 pollution and the perinatal mortality is still valid.
In order to control for time-varying, unobserved characteristics at the province-level to some extent, the columns (3)–(6) of the Table 3 are the results under controlling the interaction between provinces and time trend to test the robustness. It can be seen from the results that whether using the PM2.5 data from Columbia University or the new PM2.5 data from Dalhous University, PM2.5 pollution can bring to a significant increase in perinatal mortality. The difference between the results and those in Table 2 is mainly reflected in the change of coefficient. Once again, this result is robust, that is, the PM2.5 pollution has a significant positive association with the perinatal mortality.
Spatial analysis
Moran’s I index
Table 4 lists the results of the Moran’s I test for overall spatial correlation of perinatal mortality rates and regional PM2.5. The values of Moran’s I for mortality rates are more than 0.3 and pass the 1% significance test, which indicates that there exists significant and positive autocorrelation among regional perinatal mortality rates in the geographical space. There also exists significant positive autocorrelation among regional PM2.5.
Results of spatial analysis
Table 5 reports the results of formula (2). The spatial lag coefficients of perinatal mortality rates were significant and negative in four models, indicating that it is competitive in improving health among neighboring provinces; that is, the decrease of mortality rates in the surrounding provinces would promote the decrease of mortality rate in the region. Column (1) and column (2) present the result using the average concentrations of PM2.5. Column (3) and column (4) present the corresponding results using maximum concentrations of PM2.5. Column (1) and column (3) are the result only controlling for the province fixed effects. Column (2) and column (4) further control the year fixed effects. The difference between the coefficients of PM2.5 in four model is very small, which are all significant at the 5% level.
Spatial effects can be further decomposed into direct effect, indirect effect (spillover effects) and total effect with reference to the research result of LeSage and Pace45. Table 6 illustrates the direct effect, indirect effect and total effect of the variables in SDM model. The results show that the estimated coefficient of PM2.5′s direct effect has the same direction as the estimated coefficients of SDM model in Table 6. But the estimated coefficient of PM2.5′s indirect effect is negative and insignificant. When it comes to the estimated coefficients of controlled variables, we find that not all the spatial spillover effects of variables are significant. Overall, the GDP per capita have direct and indirect influence on perinatal mortality. The number of hospital beds per thousand persons has the significant direct effect, while the indirect effect is insignificant.
Mechanisms
In this section, we explore how PM2.5 pollution affects perinatal mortality rates. The PM2.5 pollutions may affect the ratio of infants weighing less than 2.5 kg. Infants weighing less than 2.5 kg are considered as low birth weight, who have a higher risk of early childhood death. The proportion of infants with low birth weight in a province (w5) is obtained to investigate whether it is the mechanism through which PM2.5 pollution has an impact on perinatal mortality rates. The results are presented in column (1) and (2) of Table 7. An interaction of w5*average PM2.5 (log) is included column (1) and w5*Max PM2.5 (log) is included in column (2). We find that the coefficients of PM2.5 pollutions and w5 were not significant, only the coefficients of the interactions are positive and statistically significant. There are two reasons for this result: first, due to the serious PM2.5 pollutions, the weight of perinatal infants significantly is affected, bring to a larger proportion of perinatal infants less than 2.5 kg, increasing their risk of death. Secondly, because the weight of perinatal infants is lower (less than 2.5 kg), they live in the province with more serious PM2.5 pollutions, which will increase their risk of death. But no matter what the possible reason is, PM2.5 pollution and weight together affect the perinatal mortality.
Conclusions and discussion
The air quality in China, particularly the PM2.5 level, has become an increasing public concern because of its relation to health risks. Using ArcGIS to analyze satellite raster estimates data, this paper explores the relationship between PM2.5 pollution and perinatal mortality rates in China for the years of 2002–2015. The main results are as follows: (1) The PM2.5 pollution has a significant and positive association with the perinatal mortality rates. A 1% increase of average or maximum concentrations of PM2.5(log) bring to 1.76‰ increase of perinatal mortality rates. These conclusions are similar to those of the study on air pollution and infant mortality rate and child mortality rate31,32,33. (2) The PM2.5 pollution has strong spatial dependence after analyzing Moran’s I index of the PM2.5 pollutions. Therefore, we apply SDM method and find local and neighborhood PM2.5 pollution has a significant and positive impact on local perinatal mortality rates. A possible explanation is that pollutants move between areas due to natural conditions such as rainfalls, and wind. (3) The mechanisms analysis showed that PM2.5 pollutions would affect perinatal mortality rates through the weight of newborn infants.
This paper contributes to the literature linking PM2.5 pollutions to perinatal mortality rate as there has been very little empirical evidence. It also provides policy-making basis for government to put more efforts to prevent and control PM2.5 pollutions. The policy recommendations of this paper are as follows: Firstly, the state should increase investment to control the PM2.5 pollutions, and improve the efficiency of primary energy utilization for reducing the generation of PM2.5 pollutant emissions; Secondly, the state should promulgate relevant laws and regulations to strengthen joint prevention and control of air pollution among regions; Thirdly, pregnant women should try to be exposed to as little pollution as possible. For example, they could install air purifier indoors or wear a mask when going out.
There are still some deficiencies in this study. Firstly, China is a typical country with urban–rural dual structure. Because of the limitations of data, it is impossible to conduct analysis for urban and rural areas separately in the paper. Secondly, this paper uses on macro-data, but micro-data may better identify the relationship between PM2.5 pollutant emissions and perinatal mortality rates. Thirdly, this paper only studies PM2.5 pollutions, which can be expanded about the impact of other pollutants on perinatal mortality rates. Fourthly, due to the missing variables, this paper can’t identify the causality between PM2.5 pollutant emissions and perinatal mortality rates, only get the association between them.
References
Brauer, M. et al. Ambient air pollution exposure estimation for the global burden of disease 2013. Environ. Sci. Technol. 50, 79–88 (2015).
Zheng, S. & Kahn, M. E. A new era of pollution progress in urban China?. J. Econ. Perspect. 31, 71–92 (2017).
Asian Development Bank. Toward an environmentally sustainable future: Country environmental analysis of the People's Republic of China. Asian Development Bank (2012).
Lozano, R. et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380, 2095–2128 (2012).
Lim, S. S. et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380, 2224–2260 (2012).
Samet, J. M., Dominici, F., Curriero, F. C., Coursac, I. & Zeger, S. L. Fine particulate air pollution and mortality in 20 US cities, 1987–1994. N. Engl. J. Med. 343, 1742–1749 (2000).
Dominici, F., Daniels, M., Zeger, S. L. & Samet, J. M. Air pollution and mortality: estimating regional and national dose-response relationships. J. Am. Stat. Assoc. 97, 100–111 (2002).
Wong, C. M., Vichit-Vadakan, N., Kan, H. & Qian, Z. Public Health and Air Pollution in Asia (PAPA): a multicity study of short-term effects of air pollution on mortality. Environ. Health Perspect. 116, 1195–1202 (2008).
Fang, D. et al. Mortality effects assessment of ambient PM2.5 pollution in the 74 leading cities of China. Sci. Total Environ. 569, 1545–1552 (2016).
Chen, S. & Chen, T. Air pollution and public health: evidence from sulfur dioxide mission of coal-fired power stations in China. Econ. Res. J. 8, 158–183 (2014).
Pope, C. A. III. et al. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 287, 1132–1141 (2002).
Bell, M. L., Samet, J. M. & Dominici, F. Time-series studies of particulate matter. Annu. Rev. Public Health 25, 247–280 (2004).
Dominici, F. et al. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. J. Am. Medical Ass. 295, 1127–1134 (2006).
Samoli, E. et al. Acute effects of ambient particulate matter on mortality in Europe and North America: results from the APHENA study. Environ. Health Perspect. 116, 1480–1486 (2008).
Chen, R. et al. Short-term exposure to sulfur dioxide and daily mortality in 17 Chinese cities: The China air pollution and health effects study (CAPES). Environ. Res. 118, 101–106 (2012).
Liu, S. K. et al. The effect of pollution haze on pulmonary function. J. Thorac. Dis. 8, E41 (2016).
Kampa, M. & Castanas, E. Human health effects of air pollution. Environ. Pollut. 151, 362–367 (2008).
Tallon, L. A., Manjourides, J., Pun, V. C., Salhi, C. & Suh, H. Cognitive impacts of ambient air pollution in the National Social Health and Aging Project (NSHAP) cohort. Environ. Int. 104, 102–109 (2017).
Schwartz, J. et al. The concentration-response relation between air pollution and daily deaths. Environ. Health Persp. 109, 1001–1006 (2001).
Dominici, F. et al. Air pollution and mortality: estimating regional and national dose-response relationships. JAMA 97, 100–111 (2002).
Di, Q. et al. Air pollution and mortality in the Medicare population. New Engl. J. Med. 376, 2513–2522 (2017).
Liu, L. et al. Shape of concentration-response curves between long-term particulate matter exposure and morbidities of chronic bronchitis: a review of epidemiological evidence. J. Thorac. Dis. 6, S720–S727 (2014).
Chay, K. Y., & Greenstone, M. Air quality, infant mortality, and the Clean Air Act of 1970 (No. w10053). National Bureau of Economic Research (2003).
Chay, K. Y. & Greenstone, M. The impact of air pollution on infant mortality: evidence from geographic variation in pollution shocks induced by a recession. Q. J. Econ. 118, 1121–1167 (2003).
Currie, J. & Neidell, M. Air pollution and infant health: what can we learn from California’s recent experience?. Q. J. Econ. 120, 1003–1030 (2005).
Currie, J., Neidell, M. & Schmieder, J. F. Air pollution and infant health: Lessons from New Jersey. J. Health Econ. 28(3), 688–703 (2009).
Khoo, K. L. The haze and health: a blog about the fog. Ann. Acad. Med. Singap. 35, 909 (2006).
Hannam, K., McNamee, R., Baker, P., Sibley, C. & Agius, R. Air pollution exposure and adverse pregnancy outcomes in a large UK birth cohort: use of a novel spatio-temporal modelling technique. Scand. J. Work Environ. Health 40, 518–530 (2014).
DeFranco, E. et al. Air pollution and stillbirth risk: exposure to airborne particulate matter during pregnancy is associated with fetal death. PLoS ONE 10, e0120594 (2015).
Faiz, A. S. et al. Does ambient air pollution trigger stillbirth?. Epidemiology 24, 538–544 (2013).
Woodruff, T. J., Grillo, J. & Schoendorf, K. C. The relationship between selected causes of post neonatal infant mortality and particulate air pollution in the United States. Environ. Health Perspect. 105, 608–612 (1997).
De Medeiros, A. et al. Traffic-related air pollution and perinatal mortality: a case–control study. Environ. Health Perspect. 117, 127–132 (2008).
Hackley, B., Feinstein, A. & Dixon, J. Air pollution: impact on maternal and perinatal health. J. Midwifery Women Health 52, 435–443 (2007).
Jackson, D. J., Lang, J. M. & Ganiats, T. G. Epidemiological issues in perinatal outcomes research. Pediatr. Perinatal Epidemiol. 13, 392–404 (1999).
Yu, X. & Miao, Y. Analysis on death causes and changes trends in perinatal infants during 13 years. Mater. Child Health Care China 24, 815–817 (2009).
Shao, S., Li, X., Cao, J. H. & Yang, L. L. China’s economic policy choices for governing smog pollution based on spatial spillover effects. Econ. Res. J. 9, 73–88 (2016).
Tao, C. & Yang, H. Spatial econometric model selection and its simulation analysis. Stat. Res. 31, 88–96 (2014).
Peng, W., Wu, W. & Kuang, C. H. the impact of environmental regulation on the spatial evolution of pollution industry: Based on the spatial panel Durbin model. World Econ. Pap. 6, 99–110 (2014).
Chen, Z. Eco-efficiency, urbanization and spillover effects: based on spatial panel durbin model. Manage. Rev. 28, 66–74 (2016).
Van Donkelaar, A. et al. High-resolution satellite-derived PM2.5 from optimal estimation and geographically weighted regression over North America. Environ. Sci. Technol. 49, 10482–10491 (2015).
Van Donkelaar, A. et al. Global estimates of fine particulate matter using a combined geophysical-statistical method with information from satellites, models, and monitors. Environ. Sci. Technol. 50, 3762–3772 (2016).
Boys, B. L. et al. Fifteen-year global time series of satellite-derived fine particulate matter. Environ. Sci. Technol. 48, 11109–11118 (2014).
Hammer, M. S. et al. Global estimates and long-term trends of fine particulate matter concentrations (1998–2018). Environ. Sci. Technol. 54, 7879–7890 (2020).
Xiang, K. & Song, D. Y. Spatial analysis of China province-level perinatal mortality. Iran J. Public Health 45, 614 (2016).
Lesage, J. & Pace, R. K. Introduction to Spatial Econometrics (Taylor & Francis, 1999).
Acknowledgements
We thank the financial support from the National Natural Science Foundation of China (No. 71934001) and the Natural Science Foundation of Zhejiang Province in China (No. LY18G030014).
Author information
Authors and Affiliations
Contributions
G. Li is responsible data processing, paper revision; L. Li is in charge of data processing and is the first author of the paper; D. Liu put forward the idea of paper revision and later embellishment of papers. J. Qin is responsible for responding to the reviewers' comments. H. Zhu is responsible for the second amendment and the third amendment. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, G., Li, L., Liu, D. et al. Effect of PM2.5 pollution on perinatal mortality in China. Sci Rep 11, 7596 (2021). https://doi.org/10.1038/s41598-021-87218-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-87218-7
This article is cited by
-
Effects of fine particulate matter on bone marrow-conserved hematopoietic and mesenchymal stem cells: a systematic review
Experimental & Molecular Medicine (2024)
-
The effects of surface vegetation coverage on the spatial distribution of PM2.5 in the central area of Nanchang City, China
Environmental Science and Pollution Research (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
