
Abstract
The limited availability of randomized controlled trials (RCTs) in nephrology undermines causal inferences in meta-analyses. Systematic reviews of observational studies have grown more common under such circumstances. We conducted systematic reviews of all comparative observational studies in nephrology from 2006 to 2016 to assess the trends in the past decade. We then focused on the meta-analyses combining observational studies and RCTs to evaluate the systematic differences in effect estimates between study designs using two statistical methods: by estimating the ratio of odds ratios (ROR) of the pooled OR obtained from observational studies versus those from RCTs and by examining the discrepancies in their statistical significance. The number of systematic reviews of observational studies in nephrology had grown by 11.7-fold in the past decade. Among 56 records combining observational studies and RCTs, ROR suggested that the estimates between study designs agreed well (ROR 1.05, 95% confidence interval 0.90–1.23). However, almost half of the reviews led to discrepant interpretations in terms of statistical significance. In conclusion, the findings based on ROR might encourage researchers to justify the inclusion of observational studies in meta-analyses. However, caution is needed, as the interpretations based on statistical significance were less concordant than those based on ROR.
Similar content being viewed by others


Introduction
Randomized controlled trials (RCTs) provide high-level evidence because they can minimize threats to internal validity. However, it is difficult to conduct RCTs in certain situations, such as with participants with serious complications, interventions with ethical constraints (e.g. surgical procedures) and serious adverse effects1,2,3,4. In particular, RCTs in nephrology have been limited because patients with kidney diseases generally have a number of complications5,6,7,8,9. When the number of available RCTs is insufficient, meta-analyses restricted to RCTs can be misleading10,11. Authors of such meta-analyses might then be justified in including observational studies3,12. Observational studies can reflect real world practices and have superior generalizability in comparison with RCTs under ideal conditions. However, the GRADE system states that nonrandomized studies constitute only a low level of evidence due to many threats to internal validity13. Discrepancies in the findings between observational studies and RCTs can be caused by differences in sample size, confounding factors, and biases such as selection bias, publication bias, and follow-up period14,15. In particular, unmeasured confounding factors can hamper causal inferences between the exposure and outcome16,17. Despite such controversy, several studies reported that risk estimates obtained from meta-analyses of observational studies did not differ from those from RCTs14,18,19. However, the evidence has not been sufficiently established in nephrology. Further, recent meta-analyses which compared observational studies with RCTs based their conclusions on the ratio of odds ratios (ROR) between the pooled OR derived from observational studies and those derived from RCTs, whereas most clinical studies generally interpret efficacy based on statistical significance18,19,20,21,22.
Therefore, in the present study, we aimed to (1) assess the trends and characteristics of systematic reviews of observational studies in nephrology in the past decade; and (2) quantify systematic differences in effect estimates between observational studies and RCTs in meta-analyses using two statistical methods: ROR, and discrepancies in statistical significance between the two study designs among meta-analyses combining observational studies and RCTs.
Methods
Literature search and selection of studies
The literature searches were conducted in January 2017 using EMBASE and MEDLINE. We searched studies published from January 2006 to December 2016 with no language limitation. The search strategy was developed with the assistance of a medical information specialist and included key words related to 'observational study', 'systematic review', and 'kidney disease' (see Supplement Table 1). Search terms relevant to this review were collected through expert opinion, literature review, controlled vocabulary—including Medical Subject Headings (MeSH) and Excerpta Medica Tree—and a review of the primary search results. The titles and abstracts were screened independently by two authors (M.K, K.K) and were excluded during screening if they were irrelevant to our research question or duplicated. Studies suspected of including relevant information were retained for full text assessment using inclusion and exclusion criteria. If more than one publication of one study existed, we grouped them together and adopted the publication with the most complete data. The present study was conducted according to a protocol prospectively registered at PROSPERO (CRD42016052244).
Evaluation of the characteristics of the systematic reviews of observational studies
We included systematic reviews of all comparative observational studies in nephrology to assess the trends and characteristics of systematic reviews of observational studies in nephrology in the past decade. We included systematic reviews published from 2006 to 2016 to assess the influence of reporting assessment tools including PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses)23 published in 2009 and the risk of bias (RoB) tools including the Newcastle–Ottawa Scale (NOS)24 in 2007 and the Cochrane Risk of Bias Assessment Tool for Non-Randomized Studies of Interventions (ACROBAT-NRSI)25 in 2014.
We selected studies of kidney disease based on the following two criteria:
-
1.
We included studies on participants with kidney diseases. Kidney diseases were defined as diseases that occurred in the renal parenchyma, such as acute or chronic kidney injury, kidney neoplasms, and nephrolithiasis, based on the MeSH search builder of the term 'Kidney Diseases'. Studies were excluded if they had participants with extra-renal diseases including ureteral, urethral, and urinary bladder diseases.
-
2.
We included studies with primary outcomes related to kidney diseases. We used the same definition of kidney diseases as above. We excluded studies in which kidney diseases were treated as a composite outcome (e.g. composite outcome of kidney, pancreas, and liver cancers).
We described the characteristics of systematic reviews of observational studies as follows:
-
1.
The number of published systematic reviews of observational studies per year
-
2.
Country of first author’s institution
-
3.
Designs of observational studies
-
Cohort studies included prospective and retrospective cohort studies
-
Case–control studies included ordinary and nested case–control studies.
-
-
4.
Number of primary studies included in each review
-
5.
Cause of kidney injury
-
6.
Funding source
-
Included support from both public institutions and industrial firms
-
-
7.
Whether each review assessed the RoB
-
8.
Whether each review performed a reporting assessment
-
Reporting assessment tools were PRISMA23, MOOSE (Meta-analyses of Observational Studies in Epidemiology)26, and QUAROM (The Quality of Reporting of Meta-analyses)27. STROBE (Strengthening the Reporting of Observational Studies in Epidemiology)28, CONSORT (Consolidated Standards of Reporting)29, and others were excluded.
-
Comparison of effect estimates between observational studies and RCTs in meta-analyses combining both types of study
To compare the effect estimates between study designs, we focused on meta-analyses which combined observational studies and RCTs and compared two specific interventions. We included non-randomized studies, such as cohort, case–control, cross-sectional, and controlled trials that use inappropriate strategies of allocating interventions (sometimes called quasi-randomized studies), as observational studies30. We included all studies related to the above-mentioned kidney diseases and did not focus on specific comparative studies. We compared the effect estimates obtained from observational studies as a measurement of exposure with those from randomized studies as a measurement of control in meta-analyses combining both types of studies. We expressed the quantitative differences in effect estimates for primary efficacy outcomes between study designs, taking the ROR31. Further, we assessed discrepancies in statistical significance between study designs. The absence of discrepancies, which represents agreement between efficacy and effectiveness, was defined as follows: (1) both study types were significant with the same direction of point estimates, and (2) both study types were not significant. In contrast, the presence of discrepancies was defined as follows: (1) one study type was significant while the other type was not significant, and (2) both study types were significant, although the point estimates had the opposite direction24. The assessment of the methodological quality of these meta-analyses combining both types of studies was performed using the AMSTAR (assessment of multiple systematic reviews) 2 appraisal tool32.
Data extraction
Two authors (M.K., K.K.) independently performed full screening to capture the trends and characteristics of systematic reviews of observational studies in the past decade. Three authors (M.K., A.O., A.T.) independently extracted the relevant data, such as the number of events or non-events, to compare the effect estimates between observational studies and RCTs in meta-analyses combining both types of studies. In addition, two authors (M.K., A.O.) independently graded each review for overall confidence as high, moderate, low, and critically low using the AMSTAR 2 tool.
Statistical analyses
We described the baseline characteristics of systematic reviews of observational studies using means (standard deviation [SD]) for continuous data with a normal distribution, medians (interquartile range [IQR]) for continuous variables with skewed data, and proportions for categorical data.
For the comparison of effect estimates between observational studies and RCTs in meta-analyses combining both types of studies, we estimated the ROR of the pooled OR obtained from observational studies versus those from RCTs. If an OR was not reported in a review, we recalculated the OR by extracting the number of events and non-events in both the intervention and control groups from a review or the primary study itself. If the number of events or non-events was 0, we added 0.5 to all cells of each result30. If we could not find the number of events or non-events from a review or primary articles to calculate the OR, we substituted original outcome measures, such as relative risks or risk ratios (RR), and hazard ratios (HR), instead of OR21,31. In addition, standardized meanfrom a review or the primary study itself. If the number differences (SMD) and mean differences (MD) were converted to ORs based on a previous study33. The standard errors (SEs) and 95% CI were calculated in accordance with previous studies22,31. Further, if the reviews did not report effect sizes separately for two designs, we synthesized the results obtained from primary articles. If positive outcomes such as survival were adopted, the OR comparing the intervention with control were coined. In addition, if ordinary or older interventions were included in the numerator of the OR, those OR were also coined. If several outcomes were reported, we used the first outcome that was described in the paper.
We estimated the differences in the primary efficacy outcomes between study designs by calculating the pooled ROR with the 95% CI using a two-step approach34. First, the ROR was estimated with the OR obtained from observational studies and RCTs in each review using random effects meta-regression. Second, we estimated the pooled ROR with the 95% CI across reviews with a random-effects model. Further, we performed sensitivity analysis using fixed effect model. If the ROR was more than 1.0, this would indicate that the OR from observational studies were larger than those from RCTs22,31. Heterogeneity was estimated using I2 test30. I2 values of 25%, 50% and 75% represent low, medium and high levels of heterogeneity.
Further, we examined the association between discrepancies in statistical significance of each design in accordance with above-mentioned definitions and risk factors using a multiple logistic regression model, adjusted for differences in the number of primary articles between study designs, publication year, countries of first authors, pharmacological intervention, adjustment for confounding factors, and methodological quality of systematic reviews based on rating overall confidence of AMSTAR 2 tool.
All statistical analyses were performed using STATA 16.0 (StataCorp LLC, College Station, TX, USA).
Results
Study flow diagram
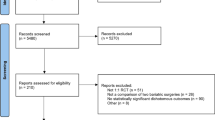
The PRISMA flow diagram (see Fig. 1) shows the study selection process. Of 5,547 records identified through database searching, we screened the titles and abstracts of the 3994 records remaining after removing duplicates and ultimately obtained 613 records. After a full-text review, we included a total of 477 records for the description of characteristics of systematic reviews of observational studies. Further, of the 114 records that combined both observational studies and RCTs, 56 were eligible for the evaluation of quantitative systematic differences in effect estimates of meta-analyses between observational studies and RCTs (see Supplement Table 2).

Study flow diagram and study selection process.
Trends over the past decade and description of study characteristics
We summarized the baseline characteristics of 477 nephrology systematic reviews of all comparative observational studies (see Table 1). The number of systematic reviews of observational studies in nephrology increased 11.7-fold between 2006 and 2016. In particular, the number of publications from China, as well as the United States of America (USA) and European countries increased (see Supplement Table 3). As shown in Table 1, most of the reviews dealt with topics related to therapies for patients with acute kidney injury, malignancy, end-stage renal diseases, and renal transplantation, aside from basic research. As for the eligible designs of observational studies, 67.1% of records included cohort studies and 33.8% included case–control studies. Of the 82 reviews related to basic research, 75 (91.5%) included case–control studies. Case series and before-after studies without comparisons were excluded in many studies. NOS was the most frequently used tool for assessing the risk of bias. ACROBAT-NRSI was used in only 0.8% of records.
Comparison of qualitative systematic differences in effect estimates between observational studies and RCTs in meta-analyses combining both types of studies
Fifty-six meta-analyses combining both observational studies and RCTs were eligible for the analyses. A total of 418 observational studies and 204 RCTs were included, and the median number (interquartile range) per meta-analysis was 7 (2.5 to 10) observational studies and 3 (2 to 5) RCTs. Almost all reviews indicated a critically low quality (see Supplement Table 4).
We compared the effect estimates of primary outcomes between study designs using ROR with 95% CI. No significant differences were noted in the effect estimates by study designs (ROR 1.05, 95% CI 0.90 to 1.23) (see Fig. 2). There was moderate heterogeneity (I2 = 47.5%). Additionally, the result obtained using the fixed effect model was closely similar to that obtained using the random effect model (ROR 0.98, 95% CI 0.89 to 1.07). Of the 56 studies, 2 reviews showed that observational studies had significantly larger effects than RCTs (ROR > 1.0), while 6 showed that observational studies had significantly smaller effects than RCTs (ROR < 1.0). The remaining 48 reviews indicated no significant differences between the study designs.

Forest plot of the pooled ROR with the 95% CI to assess systematic differences in the effect estimates between observational studies and RCTs in meta-analyses combining both types of study in nephrology. ROR ratio of odds ratio, CI confidence interval, RCT randomized controlled trial.
Of the 56 studies, 29 reviews showed no discrepancy in terms of statistical significance (14 reviews, significant in the same direction as the point estimates; 15 reviews, neither significant), while 27 reviews showed some discrepancy (all 27 studies, one significant and the other not significant). No review showed statistical significance in the opposite direction of the point estimates. Table 2 compares baseline characteristics between the presence and absence of discrepancies. In addition, we explored the factors associated with discrepancies (see Table 3) but found no significant association for any covariate; in particular, we found no differences in the number of papers between observational studies and RCTs (OR 1.10, 95% CI 0.99 to 1.23).
Further, on comparison of the results of ROR and the distribution of discrepancies of statistical significance, of 48 records (85.7%) that indicated non-significance of the ROR, 20 (35.7%) showed discrepancies in statistical significance (see Table 4).
Discussion
Our findings indicate that the number of systematic reviews of observational studies in nephrology have dramatically increased in the past decade, especially from China and the USA. Around 60% of reviews assessed the risk of bias, mostly using the NOS. A comparison of effect estimates between observational studies and RCTs in meta-analyses combining both types of studies revealed that the effect estimates from observational studies were largely consistent with those from RCTs. However, when interpreted in terms of statistical significance, almost half of the reviews led to discrepant interpretations.
Observational studies generally have larger sample sizes and better represent real-world populations than RCTs. Nevertheless, confounding factors, especially confounding by indication, often disturb the precise assessment of causal inference and establishment of high levels of evidence35,36,37,38. The quality of evidence based on observational studies might depend on how confounding factors are controlled. Adjustment using appropriate techniques, including propensity score matching and instrumental variables, are likely to be useful, although these methods cannot completely deal with unmeasured variables39,40. However, most of the reviews included in the present study did not mention the implementation of adjustment in detail.
Recently, several risk of bias appraisal tools for evaluating the quality of systematic reviews of observational studies in multiple domains have been developed, including ACROBAT-NRSI25,41,42. However, the present study showed that these tools are not yet widely implemented. Most of the studies reported the risk of bias using the NOS, although this has been reported to show uncertain reliability and validity in previous studies24,43.
In the present study, we compared the effect estimates between observational studies and RCTs in meta-analyses combining both types of studies using two analytical methods: ROR and discrepancies in statistical significance between the study designs. ROR with a 95% CI revealed that effect estimates were, on average, consistent between the two study designs. These findings would encourage researchers to justify the inclusion of observational studies in meta-analyses. Combining different types of designs in meta-analyses based on the ROR may be reasonable, as improvement in statistical power leads to a more definite assessment if a sufficient number of RCTs cannot be obtained. Further, the degree of guideline recommendations in nephrology is almost always low because evidence from high-quality RCTs is lacking. The increase in evidence derived from the finding that the effect estimates of observational studies are similar to those of RCTs might lead to an improvement in the quality of guidelines in nephrology.
However, with regard to the interpretation of the findings, almost half of records showed discrepancies in statistical significance between the study designs. Further, 35.7% of records indicated disagreement in judgement between the two analytical methods. Therefore, the findings should be interpreted with care, as inconsistent findings due to the modification of analytical methods might reflect poor internal validity between the study designs. In addition, the present study failed to identify systematic review-level factors associated with discrepancies in statistical significance, including differences in the number of primary articles between study designs and the implementation of adjustment with confounding factors. Future studies should explore risk factors at the primary study level.
Several limitations of our study should be mentioned. First, it is possible that we failed to include several gray-area studies or smaller studies, Albiet that we performed a comprehensive search. Second, we included similar research questions that were published by different authors, which might have led to overestimation. Third, to compare effect estimates between study designs, we substituted original outcome measures, such as RR or HR instead of OR, if the number of events could not be determined from primary articles to calculate the OR, similarly to previous studies21,44. However, results using the RR and HR are not necessarily consistent with those using the OR, particularly when the number of events is large. Fourth, we were unable to estimate the ROR adjusted for the methodological quality of systematic reviews based on the AMSTAR 2 tool, as almost all reviews were judged to be of low quality. Fifth, in the present study, we performed a literature search using two databases recommended by AMSTAR 2: the EMBASE and MEDLINE databases, which are the most universally used in the medical field. Sixth, we were unable to adjust for several potential risk factors that may have influenced the results in each primary study, such as the sample size, details concerning the techniques used to adjust for confounding factors, presence of selection bias, degree of risk of bias, and funding sources. In particular, differences in the sample size in each primary study might have influenced the results, but we only adjusted for differences in the number of primary articles between study designs at the systematic review level. Future studies should explore those risk factors at the primary study level. In addition, meta-analyses of observational studies are likely to have dramatically increased in number over the past few years, so we must continue to update our research. Finally, because we sampled meta-analyses which included both observational studies and RCTs, it is conceivable that extreme results, either from observational studies or from RCTs, could have been excluded when the original meta-analysis was conducted, leading to spurious greater concordance between the two study designs. Without a pre-specified protocol, we cannot assess the extent of such practices.
Conclusion
This study indicates that evidence synthesis based on observational studies has been increasing in nephrology. When we examined ROR, we found no systematic differences in effect estimates between observational studies and RCTs when meta-analyses included both study design types. These findings might encourage researchers to justify the inclusion of observational studies in meta-analyses. This approach can increase statistical power and allow stronger causal inference. However, caution is needed when interpreting the findings from both observational studies and RCTs because the interpretations based on statistical significance were shown to be less concordant than those based on ROR. Further studies are necessary to explore the causes of these contradictions.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Nardini, C. The ethics of clinical trials. Ecancermedicalscience 8, 387 (2014).
Black, N. Why we need observational studies to evaluate the effectiveness of health care. BMJ 312, 1215–1218 (1996).
Egger, M., Schneider, M. & Davey, S. G. Spurious precision? Meta-analysis of observational studies. BMJ 316, 140–144 (1998).
Barton, S. Which clinical studies provide the best evidence? The best RCT still trumps the best observational study. BMJ 321, 255–256 (2000).
Strippoli, G. F., Craig, J. C. & Schena, F. P. The number, quality, and coverage of randomized controlled trials in nephrology. J. Am. Soc. Nephrol. 15, 411–419 (2004).
Samuels, J. A. & Molony, D. A. Randomized controlled trials in nephrology: State of the evidence and critiquing the evidence. Adv. Chronic Kidney Dis. 19, 40–46 (2012).
Campbell, M. K. et al. Evidence-based medicine in nephrology: Identifying and critically appraising the literature. Nephrol. Dial. Transplant. 15, 1950–1955 (2000).
Palmer, S. C., Sciancalepore, M. & Strippoli, G. F. Trial quality in nephrology: How are we measuring up?. Am. J. Kidney Dis. 58, 335–337 (2011).
Charytan, D. & Kuntz, R. E. The exclusion of patients with chronic kidney disease from clinical trials in coronary artery disease. Kidney Int. 70, 2021–2030 (2006).
Deo, A., Schmid, C. H., Earley, A., Lau, J. & Uhlig, K. Loss to analysis in randomized controlled trials in CKD. Am. J. Kidney Dis. 58, 349–355 (2011).
Garg, A. X., Hackam, D. & Tonelli, M. Systematic review and meta-analysis: When one study is just not enough. Clin. J. Am. Soc. Nephrol. 3, 253–260 (2008).
Norris, S. L. et al. Observational studies in systematic [corrected] reviews of comparative effectiveness: AHRQ and the Effective Health Care Program. J. Clin. Epidemiol. 6, 1178–1186 (2011).
Guyatt, G. H. et al. GRADE guidelines: 9 rating up the quality of evidence. J. Clin. Epidemiol. 64, 1311–1316 (2011).
Reeves, B. C. et al. An introduction to methodological issues when including non-randomised studies in systematic reviews on the effects of interventions. Res. Synth. Methods. 4, 1–11 (2013).
Greene, T. Randomized and observational studies in nephrology: How strong is the evidence?. Am. J. Kidney Dis. 53, 377–388 (2009).
Ray, J. G. Evidence in upheaval: Incorporating observational data into clinical practice. Arch. Intern. Med. 162, 249–254 (2002).
Klein-Geltink, J. E., Rochon, P. A., Dyer, S., Laxer, M. & Anderson, G. M. Readers should systematically assess methods used to identify, measure and analyze confounding in observational cohort studies. J. Clin. Epidemiol. 60, 766–772 (2007).
Kuss, O., Legler, T. & Borgermann, J. Treatments effects from randomized trials and propensity score analyses were similar in similar populations in an example from cardiac surgery. J. Clin. Epidemiol. 64, 1076–1084 (2011).
Lonjon, G. et al. Comparison of treatment effect estimates from prospective nonrandomized studies with propensity score analysis and randomized controlled trials of surgical procedures. Ann. Surg. 259, 18–25 (2014).
Tzoulaki, I., Siontis, K. C. & Ioannidis, J. P. Prognostic effect size of cardiovascular biomarkers in datasets from observational studies versus randomised trials: Meta-epidemiology study. BMJ 343, d6829 (2011).
Anglemyer, A., Horvath, H. T. & Bero, L. Healthcare outcomes assessed with observational study designs compared with those assessed in randomized trials. Cochrane Database Syst. Rev. 1, 000034 (2014).
Sterne, J. A. et al. Statistical methods for assessing the in uence of study characteristics on treatment e ects in ‘meta-epidemiological’ research. Statist. Med. 21, 1513–1524 (2002).
Liberati, A. et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 339, b2700 (2009).
Wells, G. A. et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-analysis (University of Ottawa, 2020).
Sterne JAC, Higgins JPT, Reeves BC. A Cochrane Risk of Bias Assessment Tool: For Non-Randomized Studies of Interventions (ACROBAT-NRSI), Version 1.0.0, http://www.riskofbias.info. (2014).
Stroup, D. F. et al. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA 283, 2008–2012 (2000).
Moher, D. et al. Improving the quality of reports of meta-analyses of randomised controlled trials: The QUOROM statement. Lancet 354, 1896–1900 (1999).
Vandenbroucke, J. P. et al. Strengthening the reporting of observational studies in epidemiology (STROBE): Explanation and elaboration. Epidemiology 18, 805–835 (2007).
Schulz, K. F., Altman, D. G. & Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 340, 332 (2010).
Higgins, J. P. T., Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, www.cochrane-handbook.org (2011).
Golder, S., Loke, Y. K. & Bland, M. Meta-analyses of adverse effects data derived from randomised controlled trials as compared to observational studies: Methodological overview. PLoS Med. 8, e1001026 (2011).
Shea, B. J. et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 358, j4008 (2017).
Tajika, A., Ogawa, Y., Takeshima, N., Hayasaka, Y. & Furukawa, T. A. Replication and contradiction of highly cited research papers in psychiatry: 10-year follow-up. Br. J. Psychiatry. 207, 357–362 (2015).
Sterne, J. A. et al. Statistical methods for assessing the influence of study characteristics on treatment effects in “meta-epidemiological” research. Stat.Med. 21, 1513–1524 (2002).
Deeks, J. J. et al. European Carotid Surgery Trial Collaborative Group. Evaluating non-randomised intervention studies. Health Technol. Assess. 7, 1–173 (2003).
Kyriacou, D. N. & Lewis, R. J. Confounding by indication in clinical research. JAMA 316, 1818–1819 (2016).
Rothman, K. J., Greenland, S. & Lash, T. L. Modern Epidemiology 3rd edn, 183–209 (Wolters Kluwer Lippincott Williams Wilkins, 2008).
Patel, C. J., Burford, B. & Ioannidis, J. P. Assessment of vibration of effects due to model specification can demonstrate the instability of observational associations. J. Clin. Epidemiol. 68, 1046–1058 (2015).
Ripollone, J. E., Huybrechts, K. F., Rothman, K. J., Ferguson, R. E. & Franklin, J. M. Implications of the propensity score matching paradox in pharmacoepidemiology. Am. J. Epidemiol. 187, 1951–1961 (2018).
Staffa, S. J. & Zurakowski, D. Five steps to successfully implement and evaluate propensity score matching in clinical research studies. Anesth. Analg. 127, 1066–1073 (2018).
Sterne, J. A. et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355, i4919 (2016).
Viswanathan, M. & Berkman, N. D. Development of the RTI item bank on risk of bias and precision of observational studies. J. Clin. Epidemiol. 65, 163–178 (2012).
Lo, C. K., Mertz, D. & Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 14, 45 (2014).
Hayden, J. A., Cote, P. & Bombardier, C. Evaluation of the quality of prognosis studies in systematic reviews. Ann. Intern. Med. 144, 427–437 (2006).
Downs, S. H. & Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Commnity Health. 52, 377–384 (1998).
Harris, R. P. et al. Current methods of the U.S. preventive services task force a review of the process. Am. J. Prev. Med. 20, 21–35 (2001).
Acknowledgements
We sincerely appreciate the members of the Research Group on Meta-epidemiology at The Kyoto University School of Public Health (Tomoko Fujii, Yuki Kataoka, Yan Luo, Kenji Omae, Yasushi Tsujimoto, and Yusuke Tsutsumi) for their valuable advice.
Funding
A.O. reports personal fees from Chugai, personal fees from Ono Pharmaceutical, personal fees from Eli Lilly, personal fees from Mitsubishi-Tanabe, personal fees from Asahi-Kasei, personal fees from Takeda, personal fees from Pfizer, grants from Advantest, outside the submitted work; A.T. reports personal fees from Mitsubishi-Tanabe, personal fees from Dainippon-Sumitomo, and personal fees from Otsuka, outside the submitted work; T.A.F. reports grants and personal fees from Mitsubishi-Tanabe, personal fees from MSD, personal fees from Shionogi, and outside the submitted work; M.K. and K.K. declare that they have no relevant financial interests.
Author information
Authors and Affiliations
Contributions
M.K., A.O., A.T., K.K., and T.A.F. contributed to the research conception and design; M.K., A.O., A.T., and K.K. contributed to data extraction; M.K., A.O., A.T., K.K., and T.A.F. contributed to data analysis and interpretation. Each author contributed important intellectual content during manuscript drafting or revision and accepts personal accountability for the overall work, and agrees to ensure that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kimachi, M., Onishi, A., Tajika, A. et al. Systematic differences in effect estimates between observational studies and randomized control trials in meta-analyses in nephrology. Sci Rep 11, 6088 (2021). https://doi.org/10.1038/s41598-021-85519-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-85519-5
This article is cited by
-
Synthesis methods used to combine observational studies and randomised trials in published meta-analyses
Systematic Reviews (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
