
Abstract
In a previous study, we found that higher waist circumference (WC) and higher body mass index (BMI) both increase the risk of chronic spontaneous urticaria (CSU). The aim of this study was to determine whether WC and BMI also increase the duration of CSU. We used multivariable Cox proportional hazards models to determine the hazard ratio (HR) for longer disease duration (longer than 3 years) according to WC and BMI. A total of 52,667 subjects were enrolled and their mean age was 54.5. After adjustments for other confounding variables the high WC/high BMI group had 1.062 times higher HR (95% CI, 1.028–1.098) than the normal WC/normal BMI group. Interestingly, the high WC/normal BMI group showed a significantly higher HR (1.053; 95% CI, 1.008–1.101) than the normal WC/normal BMI group, but not the normal WC/high BMI group (0.998; 95% CI, 0.951–1.046). Taken together, our results suggest that high WC rather than high BMI is a predictive risk factor for the longer disease duration of CSU.
Similar content being viewed by others

In a previous study, we found that higher waist circumference (WC) and higher body mass index (BMI) both increase the risk of chronic spontaneous urticaria (CSU)1. Another population-based study from Italy found a positive correlation between CSU risk and obesity defined by BMI2. A population-based study of the natural course of CSU in Korea found that the 1-, 2-, 3-, 4-, and 5-year remission rates of CSU were 21.5%, 33.0%, 38.9%, 42.6%, and 44.6%, respectively3. A retrospective observational study of 549 CSU patients in Spain revealed that the percentage of patients who experienced disease durations of 1 year, 3 years, 5 years, and more than 5 years were 64.1%, 32.4%, 17.3% and 8.4%, respectively4. Several risk factors such as the presence of autoantibodies, age older than 45 years, and vitamin D deficiency have been reported to be associated with longer duration of CSU4,5,6,7. A study of 85 CSU patients in Poland revealed that higher BMI values had a trend towards longer disease duration8.
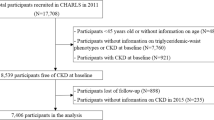
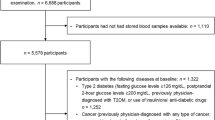
The aim of the current study was to determine whether WC and/or BMI also increase the duration of CSU. We conducted a nationwide, cross-sectional, population-based study using data from the Korean National Health Insurance Service (NHIS). The NHIS is a national health care program covering the entire Korean population. This study was approved by the Ethics Committee of Seoul St. Mary’s Hospital, the Catholic University of Korea (KC17ZESI0487), and was conducted according to the principles of the Declaration of Helsinki. The need of the written informed consent has waived by the ethics committee of Seoul St. Mary's Hospital, the Catholic University of Korea. The follow-up period was from January 2009 to December 2015. We used the following diagnosis-based algorithm to identify CSU patients: patients who had visited outpatient clinics twice at least 6 weeks apart and received 2 diagnoses designated by the International Classification of Disease (ICD)-10 code for idiopathic urticaria (L50.1), other specified urticaria (L50.8), or unspecified urticaria (L50.9), or patients who had visited outpatient clinics twice at least 6 weeks apart with one diagnosis of L50.1, L50.8, or L50.9 plus another diagnosis of angioneurotic edema (T78.3)1,9. Considering the total follow-up period of 7 years, we defined the incidence rate of longer disease duration as the percentage of patients with disease durations of longer than 3 years among the total CSU patients. We followed-up CSU patients identified by the diagnosis-based algorithm for at least 3 years after the first detection to determine whether they could be identified with the CSU diagnosis-based algorithm again, until December 2015. The clinical characteristics (sex, age, WC, BMI, smoking, alcohol, exercise, residential area, household income, diabetes mellitus, hypertension, and hyperlipidemia) of CSU patients were analysed using Student’s t-test and the chi-square test. Normal BMI was defined as < 25 kg/m2 and normal WC was defined as < 90 cm in male or < 85 cm in female, according to the Korean definition for obesity10. As WC and BMI are not always directly proportional to each other, we divided CSU patients into 4 groups as follows: normal WC/normal BMI, normal WC/high BMI (≥ 25 kg/m2), high WC (≥ 90 cm in male or ≥ 85 cm in female)/normal BMI, and high WC/high BMI. We used these categories to determine the impacts of WC and/or BMI on the duration of CSU. We used multivariable Cox proportional hazards models to determine the hazard ratio (HR) for longer duration CSU according to WC and BMI after adjustments for confounding variables. P < 0.05 was considered to be statistically significant. We performed statistical analyses using SAS version 9.4 (SAS Institute, Cary, NC, USA).
A total of 52,667 CSU patients were enrolled in this study. Their mean age was 54.5. Number of patients in 20–30, 40–64, 65–79, and ≥ 80 years age groups were 7883 (15.0%), 30,122 (57.2%), 11,686 (22.2%), and 2976 (5.7%), respectively. Number of female patients was 28,632 (54.4%). 22,215 patients (42.18%) were found to have longer disease duration (> 3 years). Female patients had a significantly higher incidence rate of longer duration (42.62%) than male patients (41.66%) (P < 0.05). Patients equal or above 80 years old had the highest incidence rate of longer disease duration (47.08%), followed by patients aged 65–79 (44.70%), 40–64 (42.45%) and 20–39 (35.57%). Patients with high WC (44.59%) and high BMI (43.43%) also had significantly higher incidence rates of longer disease duration, compared with normal WC patients and normal BMI patients, respectively (P < 0.05). Other factors that were associated with significantly higher incidence rates of longer disease duration were residential area (rural) (43.39%), diabetes mellitus (DM) (44.2%), hypertension (44.2%), and hyperlipidemia (44.2%) (P < 0.05), but not smoking, alcohol, exercise, or household income.
After adjustments for age, gender, comorbidities of diabetes mellitus, hypertension, and hyperlipidemia, there was no significantly higher HR in each BMI group, but two WC groups (90/85 ≤ WC < 95/90, 95/90 ≤ WC < 100/95) showed significantly higher HRs (1.056; 95%CI, 1.006–1.109, 1.082; 95% CI, 1.016–1.152, respectively) (Table 1). After adjustments for the same variables above, the high WC/high BMI group had 1.062 times higher HR (95% CI, 1.028–1.098) than the normal WC/normal BMI group. Interestingly, the high WC/normal BMI group showed a significantly higher HR (1.053; 95% CI, 1.008–1.101) than the normal WC/normal BMI group, but the normal WC/high BMI group did not (0.998; 95% CI, 0.951–1.046) (Table 2).
Zbiciak-Nylec et al8 firstly reported that higher BMI values had a trend towards longer disease duration. In this study, we further revealed that higher WC rather than higher BMI is more related with the longer disease duration of CSU, although both WC and BMI can affect the disease duration. Nevertheless, the pathophysiology of causal relationship between obesity and CSU has not been fully elucidated so far. According to previous studies, adipokines may act on human mast cells to induce endothelial inflammation11. As endothelial inflammation progresses, atherosclerotic changes proceed12. In the atherosclerotic plaque mast cells can be activated by variable proinflammatory factors such as C3a, C5a, cytokines, monocyte chemoattractant protein-1 and oxidized low-density lipoprotein13. Activation of mast cells through this process may affect the development of CSU8. Our results that especially, high WC/normal BMI group showed a higher risk for a longer disease duration of CSU but the normal WC/high BMI group did not, may reflect that those with high WC/normal BMI may have relatively high fat mass while those with normal WC/high BMI may have relatively high muscle mass.Taken together, these results suggest that high WC rather than high BMI is a predictive risk factor for the longer disease duration of CSU.
References
Kim, Y. S., Han, K. D., Lee, J. H., Lee, J. Y. & Park, Y. M. Can body mass index and/or waist circumference be the risk factors of chronic spontaneous urticaria? A nationwide population-based study. Ann. Dermatol. 31, 482 (2019).
Lapi, F. et al. Epidemiology of chronic spontaneous urticaria: Results from a nationwide, population-based study in Italy. Br. J. Dermatol. 174, 996–1004 (2016).
Kim, Y. S. et al. Clinical course of chronic spontaneous urticaria in the Korean adult population. Allergy Asthma Immunol. Res. 10, 83–87 (2018).
Curto-Barredo, L., Archilla, L. R., Vives, G. R., Pujol, R. M. & Gimenez-Arnau, A. M. Clinical features of chronic spontaneous urticaria that predict disease prognosis and refractoriness to standard treatment. Acta Dermato-Venereol. 98, 641–647 (2018).
Sabroe, R. A. & Greaves, M. W. Chronic idiopathic urticaria with functional autoantibodies: 12 years on. Br. J. Dermatol. 154, 813–819 (2006).
Woo, Y. R., Jung, K. E., Koo, D. W. & Lee, J. S. Vitamin D as a marker for disease severity in chronic urticaria and its possible role in pathogenesis. Ann. Dermatol. 27, 423–430 (2015).
Caproni, M. et al. Chronic idiopathic and chronic autoimmune urticaria: Clinical and immunopathological features of 68 subjects. Acta Dermato-Venereol. 84, 288–290 (2004).
Zbiciak-Nylec, M. et al. Overweight and obesity may play a role in the pathogenesis of chronic spontaneous urticaria. Clin. Exp. Dermatol. 43, 525–528 (2018).
Cherepanov, D. et al. Validation of an ICD-9-based claims algorithm for identifying patients with chronic idiopathic/spontaneous urticaria. Ann. Allergy Asthma Immunol. Off. Publ. Am. Coll. Allergy Asthma Immunol. 114, 393–398 (2015).
Kim, M. K. et al. 2014 clinical practice guidelines for overweight and obesity in Korea. Endocrinol. Metab. (Seoul, Korea) 29, 405–409 (2014).
Prevete, N. et al. Expression and function of angiopoietins and their the receptors in human basophils and mast cells. J. Biol. Regul. Homeost. Agents 27, 827–839 (2013).
Woollard, K. J. Immunological aspects of atherosclerosis. Clin. Sci. (Lond.) 125, 221–235 (2013).
Spinas, E. et al. Role of mast cells in atherosclerosis: A classical inflammatory disease. Int. J. Immunopathol. Pharmacol. 27, 517–521 (2014).
Author information
Authors and Affiliations
Contributions
Y.M.P., Y.H.K. and K.D.H. were responsible for the conception and design of the study. K.D.H. was responsible for acquisition of data. Y.H.K., K.D.H. and Y.G.P. performed the data analysis. Y.H.K. drafted the manuscript. Y.M.P., C.H.B., J.H.L., J.Y.L. contributed on revising the manuscript content. All authors participated in interpretation of the findings and all authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kim, Y.H., Do Han, K., Bang, C.H. et al. High waist circumference rather than high body mass index may be a predictive risk factor for the longer disease duration of chronic spontaneous urticaria. Sci Rep 11, 1875 (2021). https://doi.org/10.1038/s41598-021-81484-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-81484-1
This article is cited by
-
Welche Augmentations- und Triggerfaktoren sind bei der Urtikaria relevant?
Die Dermatologie (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
