
Abstract
Long working hours have been presumed to negatively influence health. However, evidence is lacking regarding any associations of working hours with depressive mood or suicidal ideation. We investigated the relationships of working hours with depressive mood and suicidal ideation in a representative sample of the Korean general population. We analyzed data collected by the Korea National Health and Nutrition Examination Surveys VI and VII (2013–2018). Depressive mood and suicidal ideation were identified through self-reporting. We divided participants into four groups according to weekly working hours: 30–40, 41–50, 51–60, and > 60 h/week. Sampling weights were applied to obtain estimates for the general Korean population. We analyzed 14,625 participants, of whom 5383 (36.8%), 4656 (31.8%), 2553 (17.5%), and 2033 (13.9%) worked 30–40, 41–50, 51–60, and > 60 h/week, respectively. In these groups, 3.6%, 4.4%, 5.2%, and 6.3% of the participants reported depressive mood, while 1.8%, 1.9%, 2.2%, and 3.6% reported suicidal ideation. In multiple regression analyses, compared with the 30–40 h/week group, the adjusted odds ratios of the 41–50, 51–60, and > 60 h/week groups for depressive mood were 1.35 (1.08–1.69), 1.5 (1.14–1.97), and 1.6 (1.19–2.14). A similar trend was evident for suicidal ideation (odds ratios 1.16 [0.82–1.63], 1.48 [0.99–2.21], and 2.29 [1.53–3.42]). Long working hours are significantly associated with depressive mood and suicidal ideation.
Similar content being viewed by others


Introduction
Long working hours are associated with negative health effects; many countries worldwide seek to limit working hours. In most European countries, the legal limit is fewer than 48 h per week; approximately half of all European countries impose a 40-h limit1. However, approximately one-third of the world's workforce still works more than 48 h per week2. Among Organization for Economic Co-operation and Development (OECD) member countries, Korea has the third longest working week worldwide (after Mexico and Costa Rica)3. In 2019, Korean working hours were 1967 annually, thus 241 h more than the mean of 1726 h among the 35 OECD countries.
Long working hours are closely associated with hypertension, diabetes, cardiovascular disease, and stroke4,5,6. Long working hours also affect mental health, such that they cause increasing fatigue and distress7. Such negative effects are manifested in several manners, including depressive mood and suicidal behavior that can cause injury and hospitalization, thereby imposing societal burdens of billions of dollars8,9.
Suicidal ideation is one of the strongest predictors of suicidal death and suicide attempts can have negative consequences such as injury and hospitalization, even if it does not end in death9. Various efforts have been made to explore the psychological processes in the development of suicide ideation and suicidal behavior10,11,12. The integrated motivational-volitional (IMV) model of suicidal behavior provides an explanation of the development of suicidal ideation. Suicidal ideation and intent are described as occurring when a person feels that he or she is subjectively trapped in a hopeless situation (entrapment)11. Entrapment consists of a two-dimensional construct: an external entrapment describes external conditions (e.g., obligations, work problems) from which one feels trapped and wants to escape, and an internal trap describes one's own internal limitations and painful thoughts that one feels unable to escape13.
Because workplace problems can act as an external entrapment that can generate suicidal ideation, there have been many studies on the association between work environment and suicidal behavior14,15,16. Several studies found that long working hours have negative effects on mental health (e.g., depressive mood and suicidal ideation), but only a few were large-scale studies using nationwide databases8,17,18. Mental health problems are also affected by socioeconomic and environmental factors, which must thus be considered19,20. Therefore, using a nationwide survey database that includes socioeconomic and environmental factors could be of great advantage. A previous study using nationwide survey data in Korea reported that long working hours were linked to suicidal thoughts18. However, the socioeconomic and environmental factors such as education level, perceived health status, and comorbidities related to suicide were not considered in the study21,22. We considered potential confounders including social demographic factors and health status when examining the relationships of working hours with depressive mood or suicidal ideation in a large sample of Korean adults.
Our primary purpose was to examine the associations of working hours with mental health problems, such as depressive mood (sadness or hopelessness) and suicidal ideation (seriously considered), in adults ≥ 19 years of age. Our secondary purpose was to determine the associations of mental health with working hours in subgroups stratified according to sex, shift work status, and occupation type (white-, pink-, or blue-collar).
Materials and methods
Study design and participants
This cross-sectional study used the databases of the 6th and 7th National Health and Nutrition Surveys (KNHANESs) conducted by the Korea Centers for Disease Control and Prevention (KCDC) from 2013 to 2018. The KNHANES has been performed annually since 1998 to evaluate the health and nutritional status of the Korean population. A national representative sample is obtained using a stratified, multistage cluster-sampling design. Participants vary among years and are not continuously monitored. The survey includes approximately 10,000 independent samples from 192 primary sampling units (PSUs) every year; each PSU is selected based on administrative districts and housing types, using a sampling frame of all census blocks containing the Korean resident registration addresses. The survey features a health interview, health examination, and nutritional survey. In this study, workers ≥ 19 years of age were analyzed. The exclusion criteria were (1) age under 19; (2) unemployed (not working for money, including students or housewives)23; (3) working for fewer than 30 h per week (such people are not regarded as full-time employees in Korea)5,24; or (4) non-completion of the working hours and/or job questionnaire(s).
Working hours
Working hours were determined by asking: “What is your average number of hours worked per week?” Overtime work was included and mealtimes were excluded. The answers were divided into 10-h increments: 31–40, 41–50, 51–60, and > 60 h per week5,24.
Depressive mood and suicidal ideation
Depressive mood was assessed by asking “Have you felt sadness or despair which hindered everyday life consistently for 2 weeks or more during the last year?” (yes or no). Suicidal ideation was assessed by asking “Have you ever seriously considered suicide in the last year?” (yes or no).
Potential mediators and confounders
Demographic characteristics, socioeconomic status, medical histories, and lifestyle habits revealed in the health interview and examination were used in the analysis. The body mass index was the weight divided by the height squared. All participants were divided into non-smokers, ex-smokers, and current smokers. Alcohol consumption was divided into none, ≤ 1 drink/month, 2 drinks/month to 3 drinks/week, and ≥ 4 drinks/week. Educational level was divided into elementary school, middle school, high school, and college or university. Household income level was divided into quartiles. Marital status was divided into single, married, separated, separated by death, and divorced. Perceived health status was recorded as very good, good, average, bad, and very bad, depending on answers to the question “How do you perceive your health?”. Sleep duration was explored by asking “How many hours do you sleep each day?”. Weekly, aerobic physical activity was categorized by intensity: mid-intensity for ≥ 2 h 30 min, high-intensity for > 1 h 15 min, or a combination of mid- and high-intensity activity for a longer time than stated above (1 min of high-intensity activity was considered equivalent to 2 min of mid-intensity activity)25. Occupational types were classified as white-collar (office workers, professionals, or managers); pink-collar (service or sales workers); and blue-collar (manufacturing, construction, craft, and related workers)26. Shift work status was identified. Any major comorbidity such as hypertension, diabetes, dyslipidemia, stroke, myocardial infarction, angina, or a malignancy (e.g., lung, stomach, liver, colon, breast, or cervical cancer) was recorded.
Statistical analysis
Analysis of variance was used to compare continuous variables; the data are presented as means with standard deviations. The chi-squared test was employed to analyze categorical variables; the data are presented as numbers with percentages. We used logistic regression to calculate odds ratios (ORs) with 95% confidence intervals (CIs). We constructed three models to explore potential mediators and confounders. Model 1 was unadjusted. Model 2 was adjusted for age and sex. Model 3 was fully adjusted for age, sex, smoking status, alcohol consumption, educational level, household income, marital status, perceived health status, occupation, sleep duration, physical activity, and comorbidities. We performed subgroup analysis according to sex (male or female); shift work status (no or yes); and occupation (white-, pink-, or blue-collar). As KNHANES data were derived from multistage complex probability sampling, population weights were applied to all data to ensure that they were representative of the entire Korean population. All statistical analyses were performed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA). A two-sided p-value < 0.05 was considered to indicate statistical significance.
Ethics statement
KNHANES VI and VII were approved by the KCDC Institutional Review Board (approval nos. 2013–12EXP-03–5C, 2018–01–03-P-A). Informed consent was obtained from all participants. The study adhered to the principles of the Declaration of Helsinki. All study procedures followed relevant guidelines and regulations.
Results
In total, 47,217 people were surveyed. The following individuals were excluded: 9794 aged < 19 years, 13,362 who were unemployed, 4995 who were working fewer than 30 h per week, 4434 who did not report working hours, and 47 who did not report occupations. We finally analyzed 14,625 people (Fig. 1).

Flow chart of study participants among individuals included in the 2013 to 2018 Korea National Health and Nutrition Examination Surveys (KNHANES VI and VII).
General characteristics stratified according to working hours
The 14,625 participants were divided into individuals who worked 31–40 (5383; 36.8%), 41–50 (4656; 31.8%), 51–60 (2553; 17.5%), and > 60 h/week (2033; 13.9%). Participant demographic and general characteristics are shown in Table 1. Age, sex, height, weight, body mass index, smoking status, alcohol consumption, educational level, household income, marital status, perceived health status, sleep duration, aerobic physical activity, occupation, shift work, and comorbidities (except malignancy) differed significantly among the groups because the study population was very large. The depressive mood rates differed significantly among the four groups; depressive moods were reported by 196 (3.6%), 206 (4.4%), 133 (5.2%), and 128 (6.3%) participants who worked 31–40, 41–50, 51–60, and > 60 h/week, respectively (p < 0.001). The rates of suicidal ideation also differed significantly among the four groups: 96 (1.8%), 86 (1.9%), 55 (2.2%), and 74 (3.6%) (p < 0.001).
Relationships of working hours with depressive mood and suicidal ideation
In Model 1 (unadjusted), the ORs for depressive mood of the 41–50-, 51–60-, and > 60-h groups were higher than the OR of the 31–40-h group: 1.29 (95% CI 1.04–1.60, p = 0.022), 1.5 (95% CI 1.17–1.93, p = 0.001), and 1.8 (95% CI 1.39–2.33, p < 0.001), respectively. Compared with participants who worked 31–40 h, participants who worked > 60 h had a higher OR (2.39, 95% CI 1.66–3.44, p < 0.001) for suicidal ideation. In Model 2 (adjusted for sex and age), the ORs for depressive mood of the 41–50-, 51–60-, and > 60-h groups were higher than the OR of the 31–40-h group: 1.42 (95% CI 1.14–1.77, p = 0.002), 1.75 (95% CI 1.35–1.25, p < 0.001), and 2.03 (95% CI 1.55–2.66, p < 0.001). Compared with participants who worked 31–40 h, participants who worked 51–60 and > 60 h had higher ORs for suicidal ideation: 1.59 (95% CI 1.09–2.33, p = 0.017) and 2.7 (95% CI 1.86–3.91, p < 0.001), respectively. In Model 3 (adjusted for potentially confounding variables), the ORs for depressive mood of the 41–50-, 51–60-, and > 60-h groups remained higher than the OR of the 31–40-h group: 1.35 (95% CI 1.08–1.69, p = 0.01), 1.5 (95% CI 1.14–1.97, p < 0.001), and 1.6 (95% CI 1.19–2.14, p < 0.001). A dose–response relationship was evident between increased working hours and the risk of depressive mood. Compared with participants who worked 31–40 h, participants who worked > 60 h (OR 2.3, 95% CI 1.54–3.45, p < 0.001) exhibited the strongest association with suicidal ideation (Table 2).
Subgroup analysis by sex, shift work status, and occupation
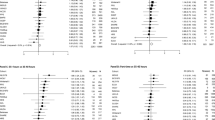
We explored the effects of sex, shift work, and occupation. In men, participants who worked > 60 h exhibited a higher risk of depressive mood, compared with participants who worked 31–40 h (OR 1.77, 95% CI 1.14–2.76). For non-shift work, longer working hours were strongly associated with depressive mood (ORs for 41–50, 51–60, and > 60 h: 1.13 [95% CI 1.02–1.69], 1.56 [95% CI 1.16–2.11], and 1.64 [95% CI 1.19–2.26], respectively). In terms of occupation, longer white-collar working hours were associated with higher risks of depressive mood (ORs for 41–50, 51–60, and > 60 h: 1.45 [95% CI 1.01–2.09], 2.11 [95% CI 1.31–3.41], and 2.19 [95% CI 1.13–4.23]). Blue-collar work > 60 h was strongly associated with depressive mood (OR 1.58, 95% CI 1.04–2.39) (Fig. 2).

Associations of depressive mood with working hours according to subgroup. Model 3 was fully adjusted for age, sex, smoking status, alcohol consumption, educational level, household income, marital status, perceived health status, occupation, sleep duration, physical activity, and comorbidities. CI, confidence interval.
Suicidal ideation risk increased significantly with working hours in men (ORs for 41–50, 51–60, and > 60 h: 1.89 [95% CI 1.05–3.39], 2.30 [95% CI 1.16–4.59], and 3.93 [95% CI 2.05–7.52]). In the group working > 60 h, shift work featured a larger OR than did non-shift work (3.02 [95% CI 1.24–7.34] vs. 2.22 [95% CI 1.41–3.49]). Among occupations, blue-collar work > 60 h was associated with the highest risk of suicidal ideation (OR 3.54 [95% CI 2.07–6.06]) (Fig. 3).

Associations of suicidal ideation with working hours according to subgroup. Model 3 was fully adjusted for age, sex, smoking status, alcohol consumption, educational level, household income, marital status, perceived health status, occupation, sleep duration, physical activity, and comorbidities. CI, confidence interval.
Discussion
We found that longer working hours were significantly associated with depressive mood and suicidal ideation in adults. The relationship with suicidal ideation was stronger in men who were blue-collar or shift workers.
Suicidal ideation is defined as any thoughts, images, beliefs, voices, or other cognitions reported by the individual about intentionally ending his or her own life27. Suicidal ideation can be presumed to exist when an individual has thought about suicide even if he or she has not seriously considered it, and various screening tools have been developed to measure the severity of suicidal ideation28,29,30. One of them, the Beck Depression Inventory-II (BDI-II), evaluates a patient's suicidal ideation on one of four scales; 0 ("I have no intention of committing suicide), 1 (I have thoughts of suicide, but I will not do it."), 2 ("I would like to commit suicide), and 3 (I would commit suicide if I had the chance"). In the KNHANES data we used, the question was asked about seriously considered suicidal ideation, so it could be considered to be equivalent to a level of 2 or higher on the BDI-II scale. A study of 6891 psychiatric outpatients by GK Brown et al. found that those with a BDI-II score of 2 or greater were 6.9 times more likely to commit suicide than those with less than score of 231.
A recent study suggested new risk factors related to suicidal ideation through the IMV model of suicidal behavior32. The IMV model consists of three phases: a pre-motivational phase (background factors), a motivational phase (suicidal ideation/intention formation), and a volitional phase (behavioral enaction). The pre-motivational phase explains that background factors such as socioeconomic and environmental factors influence suicidal behavior33. In the motivational phase, it was argued that defeat and/or humiliation from which there is no perceived escape—a sense of entrapment is involved in the psychological processes for suicidal ideation to occur. In this process, it was explained that the presence or absence of threat to self-moderators (e.g. social problem-solving and coping) and motivational moderators (e.g. more positive future thoughts and goals) influence the development of suicidal ideations. In our study, we considered background factors (socioeconomic and environmental factors) as much as possible and tried to investigate the effect of long working hours, which could act as entrapment, on suicidal ideation.
Long working hours create distress and affect physical health because of their relationships with lack of exercise, more smoking, and more alcohol consumption8,34,35,36. Long hours also increase anxiety and depression37. Among United Kingdom public officials, individuals who worked more than 55 h were 1.66-fold more likely to have depression and 1.74-fold more likely to experience anxiety, compared with individuals who worked 35–40 h38. Similarly, in our study, the OR for depressive mood was 1.6-fold higher (95% CI 1.19–2.14) for participants who worked > 60 h, compared with participants who worked 31–40 h. Long working hours are also associated with suicidal risk; Kim et al. reported that suicidal ideation was 1.38-fold higher among individuals working > 60 h than among individuals working 40–51 h39. Yoon et al. reported an increased risk of suicidal ideation among individuals working ≥ 60 h compared with individuals working < 52 h18. In our study, compared with participants who worked 31–40 h, the OR for suicide was 2.3-fold greater for participants who worked > 60 h (95% CI 1.54–3.45).
Previous studies have shown that long working hours affected mental health more among women than among men40,41. We found that women who worked > 60 h exhibited a higher OR for depressive mood, compared with men. However, we found a relationship between suicidal ideation and working hours only in men. Shift work causes sleep problems because it does not synchronize with the 24-h circadian rhythm, thereby worsening mental health42. We found similar results. Among shift workers, participants who worked > 60 h exhibited a higher OR for suicidal ideation, compared with non-shift workers. In terms of occupation, Kim et al. reported that blue-collar workers exhibited higher depression scores than did white-collar workers43. In our study, the OR (3.54) for suicidal ideation was highest for blue-collar participants who worked > 60 h.
There are several possible explanations for blue-collar workers being more suicidal. Blue-collar workers are usually employed as one of the non-managerial occupations, and thus often have low autonomy and decision-making rights44. Blue-collar workers tend to be more stressed due to conflicts caused by problems such as vertical communication with managers45. Also, blue-collar workers show a more vulnerable health condition than white-collar workers, because they are much exposed to dangerous physical conditions such as hard physical work, noise, and chemicals, and tend to have relatively little interest in health46,47,48,49. Stress and physical illness are well known as major risk factors for suicidal behavior33,50.
In our study, the relationship between pink-collar occupation and suicidal ideation showed opposite results depending on whether environmental factors were adjusted or not. In model 1 (unadjusted) and model 2 (adjusted by age and sex), pink-collar occupation was positively related with suicidal ideation, whereas in model 3 (fully adjusted including environmental factors) it showed a negative relationship. This is because environmental factors such as smoking status, alcohol consumption, educational level, household income, marital status, perceived health status, sleep duration, physical activity, and comorbidities acted as mediators or confounders.
How do long working hours affect mental health? First, home rest time is shortened; workers do not fully recover from work-induced stress and fatigue51. Second, long working hours reduce sleep quality and volume; sleep problems are associated with depression and anxiety52,53. Furthermore, if a worker cannot control the workload (and thus may work overtime), an imbalance between effort and reward may develop. Stress increases if the work reward is perceived to be inadequate54. In this way, workers who work long hours may feel defeated and humiliated, with their self-moderators keep threatened, and eventually fall into entrapment55.
The principal strength of this study is the very large and nationally representative sample used for analysis. The results can be generalized to the entire adult population of Korea. To the best of our knowledge, this is the largest study thus far regarding the relationships of working hours with depressive mood and suicidal ideation in an Asian population. However, this work had several limitations. First, the KNHANES data were not collected for this study's purposes, so we were not able to go through the rigorous data collection strategies commonly implemented in established research studies. Second, because the study was cross-sectional in nature, we could not infer any causal relationship. Third, because all data were self-reported, recall bias may have influenced the analysis. For example, the number of working hours was measured via a single self-reported question. Though self-reported questionnaires had been proven useful in examining working hours at the population level in several studies, more objective measurements will be needed in further studies8,18,54,56. Fourth, as the questionnaire investigated the mental health of the past year, the specific point in time of the depressive symptoms or suicidal ideation was not clarified. Fifth, depressive mood and suicidal ideation were defined through yes/no dichotomous questions. Though various symptoms such as sadness, hopelessness, fear of the future, and the persistent thought that life is not worth living can indicate depressive mood, the questionnaire used in KNHANES data asked only the sadness or hopelessness57. Suicidal ideation may also vary in severity or definition depending on the measurement method28,29,30. Sixth, because ethnic and geographical characteristics may have affected the results, caution is needed when generalizing the results to non-Korean populations. A well-designed large-scale study is required.
Conclusion
We studied a nationally representative Korean population. After adjustments for sociodemographic and mental health-related variables, we found that long working hours were strongly associated with depressive mood and suicidal ideation. Men, as well as shift and blue-collar workers, were more vulnerable to suicidal ideation. Working hours should be limited by law.
Data availability
The KCDC data are available at https://knhanes.cdc.go.kr/knhanes/sub03/sub03_02_05.do (accessed 8 April 2021). The raw data can be downloaded by anyone who meets the criteria specified by the KCDC.
References
Rodriguez-Jareño, M. C. et al. European Working Time Directive and doctors’ health: A systematic review of the available epidemiological evidence. BMJ Open 4(7), e004916 (2014).
Wadsworth, E. & Walters, D. Safety and health at the heart of the future of work: Building on 100 years of experience. (accessed 23 August 2021); https://www.ilo.org/safework/events/safeday/WCMS_687610/lang--en/index.htm (2019).
OECD. Average annual hours actually worked per worker. (accessed 8 April 2021); https://stats.oecd.org/indexaspx?DataSetCode=ANHRS
Bannai, A. & Tamakoshi, A. The association between long working hours and health: A systematic review of epidemiological evidence. Scand. J. Work Environ. Health. 5–18 (2014).
Yoo, D. H. et al. Effect of long working hours on self-reported hypertension among middle-aged and older wage workers. Ann. Occup. Environ. Med. 26(1), 25 (2014).
Kivimäki, M. et al. Long working hours and risk of coronary heart disease and stroke: A systematic review and meta-analysis of published and unpublished data for 603,838 individuals. Lancet 386(10005), 1739–1746 (2015).
Park, J. et al. Long working hours and subjective fatigue symptoms. Ind. Health. 39(3), 250–254 (2001).
Park, S. et al. The negative impact of long working hours on mental health in young Korean workers. PLoS ONE 15(8), e0236931 (2020).
Klonsky, E. D., May, A. M. & Saffer, B. Y. Suicide, suicide attempts, and suicidal ideation. Annu. Rev. Clin. Psychol. 12, 307–330 (2016).
Joiner, T. Why People Die by Suicide (Harvard University Press, 2007).
O’Connor, R. C. Towards an Integrated Motivational–Volitional Model of Suicidal Behaviour. International handbook of suicide prevention: Research, policy and practice (Wiley Blackwell, 2011).
Klonsky, E. D. & May, A. M. The three-step theory (3ST): A new theory of suicide rooted in the “ideation-to-action” framework. Int. J. Cogn. Ther. 8(2), 114–129 (2015).
Gilbert, P. & Allan, S. The role of defeat and entrapment (arrested flight) in depression: An exploration of an evolutionary view. Psychol. Med. 28(3), 585–598 (1998).
Stack, S. Occupation and suicide. Soc. Sci. Q. 82(2), 384–396 (2001).
van Wijngaarden, E. An exploratory investigation of suicide and occupational exposure. J. Occup. Environ. Med. 45(1), 96–101 (2003).
Woo, J.-M. & Postolache, T. Τ. The impact of work environment on mood disorders and suicide: Evidence and implications. Int. J. Disab. Hum. Dev. 7(2), 185–200 (2008).
Yoon, Y. et al. Working hours and depressive symptoms: The role of job stress factors. Ann. Occup. Environ. Med. 30(1), 1–9 (2018).
Yoon, J.-H. et al. Relationship between long working hours and suicidal thoughts: Nationwide data from the 4th and 5th Korean National Health and Nutrition Examination Survey. PLoS ONE 10(6), e0129142 (2015).
Rowe, J. L., Bruce, M. L. & Conwell, Y. Correlates of suicide among home health care utilizers who died by suicide and community controls. Suicide Life Threat Behav. 36(1), 65–75 (2006).
Atay, I. M., Eren, I. & GündoğAr, D. The prevalence of death ideation and attempted suicide and the associated risk factors in Isparta, Turkey. Turk Psikiyatri Derg. 23(2) (2012).
Pompili, M. et al. Does the level of education influence completed suicide? A nationwide register study. J. Affect. Disord. 147(1–3), 437–440 (2013).
Turvey, C. L. et al. Risk factors for late-life suicide: A prospective, community-based study. Am. J. Geriatr. Psychiatry. 10(4), 398–406 (2002).
Ma, X. et al. Smoking and psychiatric disorders in the rural and urban regions of Beijing, China: A community-based survey. Drug Alcohol. Depend 100(1–2), 146–152 (2009).
Seok, H., Won, J-U., Lee, T. I., et al. A dose-response relationship between long working hours and unmet need for access to hospital facilities. Scand. J. Work Environ. Health. 135–143 (2016).
Park, S.-M. et al. Depression is closely associated with chronic low back pain in patients over 50 years of age: A cross-sectional study using the sixth Korea National Health and Nutrition Examination Survey (KNHANES VI-2). Spine 43(18), 1281–1288 (2018).
Min, K.-B. et al. Precarious employment and the risk of suicidal ideation and suicide attempts. Prev. Med. 71, 72–76 (2015).
Wenzel, A., Brown, G. K. & Beck, A. T. Cognitive Therapy for Suicidal Patients: Scientific and Clinical Applications (American Psychological Association, 2009).
Beck, A. T., Steer, R. A. & Brown, G. K. Manual for the Beck Depression Inventory-II (Psychological Corporation, 1996).
Beck, A. T., Kovacs, M. & Weissman, A. Assessment of suicidal intention: The Scale for Suicide Ideation. J. Consult. Clin. Psychol. 47(2), 343 (1979).
Silverman, M. M. et al. Rebuilding the tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors: Part 2: Suicide-related ideations, communications, and behaviors. Suicide Life Threat Behav. 37(3), 264–277 (2007).
Brown, G. K. et al. Risk factors for suicide in psychiatric outpatients: A 20-year prospective study. J. Consult. Clin. Psychol. 68(3), 371 (2000).
O’Connor, R. C. & Kirtley, O. J. The integrated motivational–volitional model of suicidal behaviour. Philos. Trans. R. Soc. Lond. B Biol. Sci. 373(1754), 20170268 (2018).
O’Connor, R. C. & Nock, M. K. The psychology of suicidal behaviour. Lancet Psychiatry 1(1), 73–85 (2014).
Kouvonen, A. et al. Work stress, smoking status, and smoking intensity: An observational study of 46 190 employees. J. Epidemiol. Commun. Health. 59(1), 63–69 (2005).
Lipton, R. The relationship between alcohol, stress, and depression in Mexican Americans and non-Hispanic whites. Behav. Med. 23(3), 101–111 (1997).
Norris, R., Carroll, D. & Cochrane, R. The effects of physical activity and exercise training on psychological stress and well-being in an adolescent population. J. Psychosom. Res. 36(1), 55–65 (1992).
Afonso, P., Fonseca, M. & Pires, J. F. Impact of working hours on sleep and mental health. Occup. Med. 67(5), 377–382 (2017).
Virtanen, M., Ferrie, J. E., Singh-Manoux, A., et al. Long working hours and symptoms of anxiety and depression: A 5-year follow-up of the Whitehall II study. Psychol. Med. 1 (2011).
Kim, K. U. et al. Association between long working hours and suicidal ideation. Korean J. Occup. Environ. Med. 24(4), 339–346 (2012).
Oler, M. J. et al. Depression, suicidal ideation, and substance use among adolescents: Are athletes at less risk?. Arch. Fam. Med. 3(9), 781–785 (1994).
Amagasa, T. & Nakayama, T. Relationship between long working hours and depression: A 3-year longitudinal study of clerical workers. J. Occup. Environ. Med. 55(8), 863–872 (2013).
Park, H., Suh, B. S. & Lee, K. The difference of suicidal ideation between shift workers and day workers by gender. Arch. Suicide Res. 1–9 (2020).
Kim, W. et al. The impact of occupation according to income on depressive symptoms in south Korean individuals: Findings from the Korean welfare panel study. Int. J. Soc. Psychiatry. 62(3), 227–234 (2016).
Siblot, Y. et al. Sociologie des Classes Populaires Contemporaines (Armand Colin, 2015).
Nydegger. R. Occupational stress and job satisfaction in white-and blue-collar workers. Int. J. Bus. Econ. Res. 1(12) (2002).
Kolmet, M., Marino, R. & Plummer, D. Anglo-Australian male blue-collar workers discuss gender and health issues. Int. J. Mens. Health. 5(1), 81 (2006).
Snashall, D. Occupational health in the construction industry. Scand. J. Work Environ. Health 5–10 (2005).
Stocks, S. et al. Occupation and work-related ill-health in UK construction workers. Occup. Med. 61(6), 407–415 (2011).
Jacobsen, H. B. et al. Construction workers struggle with a high prevalence of mental distress and this is associated with their pain and injuries. J. Occup. Environ. Med. 55(10), 1197 (2013).
Conwell, Y. et al. Health status and suicide in the second half of life. Int. J. Geriatr. Psychiatry. 25(4), 371–379 (2010).
Jansen, N. et al. Need for recovery from work: Evaluating short-term effects of working hours, patterns and schedules. Ergonomics 46(7), 664–680 (2003).
Nakashima, M. et al. Association between long working hours and sleep problems in white-collar workers. J. Sleep Res. 20, 110–116 (2011).
Taylor, D. J. et al. Epidemiology of insomnia, depression, and anxiety. Sleep 28(11), 1457–1464 (2005).
Bannai, A., Ukawa, S. & Tamakoshi, A. Long working hours and psychological distress among school teachers in Japan. J. Occup. Health. 57(1), 20–27 (2015).
Rasmussen, S. A. et al. Elaborating the cry of pain model of suicidality: Testing a psychological model in a sample of first-time and repeat self-harm patients. Br. J. Clin. Psychol. 49(1), 15–30 (2010).
Yamauchi, T. et al. Long working hours, sleep-related problems, and near-misses/injuries in industrial settings using a nationally representative sample of workers in Japan. PLoS ONE 14(7), e0219657 (2019).
Fink, M. Depressive Mood Disorders (Oxford University Press, 1999).
Acknowledgements
This work was supported by the Soonchunhyang University Research Fund.
Author information
Authors and Affiliations
Contributions
Conceptualization, S.H. and Y.K.; methodology, S.H. and Y.K.; software, J.E.M.; validation, Y.S.C.; formal analysis, Y.K.; investigation, S.H. and Y.K.; resources, S.H.; data curation, J.E.M.; writing-original draft preparation, S.H.; writing-review and editing, S.H. and Y.S.C.; visualization, S.H.; supervision, Y.S.C.; project administration, S.H.; funding acquisition, S.H. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Han, S., Ko, Y., Moon, J.E. et al. Working hours are closely associated with depressive mood and suicidal ideation in Korean adults: a nationwide cross-sectional study. Sci Rep 11, 23102 (2021). https://doi.org/10.1038/s41598-021-02574-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-02574-8
This article is cited by
-
Female workers with long working hours are more likely to have depressive symptoms when having family-to-work conflict
International Archives of Occupational and Environmental Health (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
