
Abstract
The number of patients with traumatic intracranial hemorrhage (tICH) that are taking antithrombotics (ATs), antiplatelets (APs) and/or anticoagulants (ACs), has increased, but the influence of it for outcome remains unclear. This study aimed to evaluate an influence of AT for tICH. We retrospectively reviewed all patients with tICH treated between 2012 and 2019, and analyzed demographics, neurological status, clinical course, radiological findings, and outcome data. A total of 393 patients with tICH were included; 117 were on AT therapy (group A) and 276 were not (group B). Fifty-one (43.6%) and 159 (57.6%) patients in groups A and B, respectively, exhibited mRS of 0–2 at discharge (p = 0.0113). Mortality at 30 days was significantly higher in group A than in group B (25.6% vs 16.3%, p = 0.0356). Multivariate analysis revealed that higher age (OR 32.7, p < 0.0001), female gender (OR 0.56, p = 0.0285), pre-injury vitamin K antagonist (VKA; OR 0.42, p = 0.0297), and hematoma enlargement (OR 0.27, p < 0.0001) were associated with unfavorable outcome. AP and direct oral anticoagulant were not. Hematoma enlargement was significantly higher in AC-users than in non-users. Pre-injury VKA was at high risk of poor prognosis for patients with tICH. To improve outcomes, the management of VKA seems to be important.
Similar content being viewed by others
Introduction
Intracranial hematoma and its expansion are associated with unfavorable outcome of patients with head trauma1,2,3. As the Japanese population ages, the number of patient with traumatic intracranial hemorrhage (tICH) that are taking antithrombotic agents (AT), antiplatelet (AP) and/or anticoagulant (AC) therapy, is increasing. However, there is a discrepancy in the influence of pre-injury AT on outcomes in patients with head trauma. Furthermore, there remains no strong consensus on which patients should receive antithrombotic reversal agents, due to increased risk of thromboembolic events4. In addition, to our knowledge, there are no reports about the effect of resumption of AT after head trauma and the timing of resumption. Hence, use of reversal agent, resumption of AT, timing of resumption, and rebleeding risk of resumption after tICH are clinical conundrums. We hypothesize that the patients with tICH on AT therapy would be more likely to have unfavorable outcome than those without AT and reversal agent would be reduced hematoma expansion but increased thromboembolic events. The aim of this study was to evaluate the clinical factors, especially pre-injury AT, affected outcomes in patients with tICH. In addition, to assess the effects of use of reversal agent, resumption of AT, optimal time to restart AT, and rebleeding risk of resumption, the patients with AT in which thromboembolic events occurred after using reversal agents or rebleeding occurred after AT were restarted were extracted.
Methods
Ethical approval
All procedures performed in this study was approved by the local ethics committee of the Hitachi General Hospital (Research Ethics Committee of Corporate Hospital Group, Hitachi, Ltd: #2019-71), and complied with the conditions laid out by the Declaration of Helsinki. The opt-out consent was used for patients and the requirement to obtain informed consent was waived by Research Ethics Committee of Corporate Hospital Group, Hitachi.
Patient population
This study was conducted at the Hitachi General Hospital, a critical care medical center. We retrospectively reviewed the medical records of all patients with head trauma who were hospitalized for treatment during the 7-year period between April 2012 and March 2019. Head trauma was defined as all damages of soft tissue of the head, skull, and/or intracranial regions. Patients who were aged under 16 years old, with chronic subdural hematoma, without intracranial hematomas, with spontaneous intraparenchymal hemorrhage (IPH), and whose modified Rankin Scale (mRS) was ≥ 3 before the trauma were excluded.
The following data were collected from medical records: age, sex, main type of tICH, Marshall classification, emergency surgery, IPH, international normalized ratio (INR), activated partial thromboplastin (APTT), extracranial injury, hematoma enlargement within 72 h, mRS at discharge, mortality within 30 days, and neurological death. Main type of tICH was defined if it seemed to be the major factor affecting symptoms.
Imaging protocol
All computed tomography (CT) scans were performed using a SCENARIA CT scanner (Hitachi Medical Corporation, Hitachi, Japan) with a 2.5-mm slice thickness. All radiologists blinded and did not know the object of this study. All head trauma patients that were admitted to Hitachi General Hospital underwent an initial head CT scan within 60 min of arrival and a 2nd CT scan was performed within 24 h of admission if intracranial hemorrhage was identified on the initial CT scan. The existence and enlargement of intracranial hematomas were evaluated by the first author. IPH volume was calculated using the “ABC/2” formula5. “Enlargement” of IPH was defined as when the hematoma volume increased by more than 25%. In the case of epidural hematomas, subdural hematomas, or subarachnoid hemorrhage, “enlargement” was judged by authors based on the thickness of the thickest part. Rebleeding was defined when hematoma enlargement was identified in the patients, in which hemostasis was confirmed at least once in repeated CT.
Reversal agents
All patients with tICH were checked international normalized ratio (INR) on arrival and within 24 h after administration if reversal agent was used. In Japan, KCENTRA (CSL Behring, King of Prussia, PA, USA) is the only approved 4-factor prothrombin complex concentrate (4F-PCC) by Japan’s pharmaceutical affairs since March 2017 as the urgent reversal of acquired coagulation factor deficiency induced by Vitamin K antagonist (VKA) therapy. Before approval of this drug, patients on VKA were injected 5 or 10 mg vitamin K2 (Vit. K2) intravenously. After approval, the indicated dose of 4F-PCC was administered in addition to Vit. K2; patients with an INR of 2–4 was 25 IU/kg, INR of 4–6 was 35 IU/kg, and INR more than 6 was 50 IU/kg. All patients on AP agents did not receive platelet transfusions or l-deamino-8-d-arginine vasopressin.
Clinical outcomes
The primary endpoint was a favorable outcome, defined as mRS 0–2 at discharge. The secondary endpoints were enlargement of the intracranial hematoma within 72 h, all-cause mortality within 30 days, and in-hospital neurological death. Neurological death was defined as death caused by any intracranial disease that was identified by neurosurgeons.
To investigate the optimal time to restart AT treatment, we evaluated the cases in which rebleeding occurred after antithrombotic drug treatment was restarted or in-hospital thromboembolic events, which include ischemic stroke, myocardial infarction (MI), pulmonary embolism (PE), and venous thromboembolism (VTE), occurred, and reviewed past literatures.
Statistical analysis
To determine the features of clinical characteristics of AT users, we compared clinical factors between the patients that were and were not treated with such drugs. To determine the clinical factors that influenced clinical outcome of patients with tICH, univariate and multivariate logistic regression analysis was performed. The variables that were statistically significant by univariate analysis were included in multivariate analysis.
Summary statistics for the examined variables are presented (frequencies and percentages for categorical data and medians and interquartile ranges for continuous data). Fisher’s exact test was used for analyzing categorical data, and the Wilcoxon rank sum test was used for analyzing continuous data.
All comparisons were planned, and all tests were 2-sided. P-values of < 0.05 were considered to be statistically significant. All statistical analyses were performed using JMP (Japanese version 12 for Windows; SAS Institute Inc., Cary, NC, USA).
Results
Study selection and characteristics
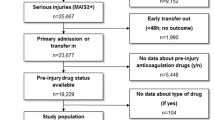
A total of 727 consecutive patients with head trauma were identified during 7-year period. After excluding 50 patients who were aged under 16 years old, 206 patients with chronic subdural hematomas, 62 patients without intracranial hematomas, 4 patients with spontaneous intraparenchymal hemorrhage (IPH), 9 patients whose modified Rankin Scale (mRS) was ≥ 3 before the trauma, and 3 patients for whom detailed information was not available, 393 patients with tICH were included in this study (Fig. 1). Of the 393 patients, 46 did not undergo a 2nd CT scan before emergency surgery. Another 20 further patients did not undergo a 2nd CT scan because they died or had very small hematomas. Thus, 327 patients, 44 of whom with AC, were performed repeated CT scan at least once within 24 h. They were included in the calculation of the ratio of hematoma enlargement within 72 h. In addition, totally 359 patients were performed CT or MRI at least once during hospitalization. The incidence of ischemic stroke or rebleeding were evaluated in them.

Schematic drawing of patient selection method.
Table 1 summarizes the clinical characteristics of the whole study population and the two groups; i.e., the patients that were (group A, 117 patients) and were not (group B, 276 patients) treated with AT. In group A, 62 patients (53.0%) were using AP alone, 38 patients (32.5%) were using AC alone, and 17 patients (14.5%) were using both types of drugs. Aspirin was the most frequently used antiplatelet medication (49 patients, 62.0%), followed by clopidogrel (26, 32.9%), cilostazol (12, 15.2%), and others (7, 8.9%). In these 79 patients, dual antiplatelet therapy (DAPT) was performed in 24 patients (30.4%) and triple antiplatelet therapy (TAPT) in 1 patient (1.3%). On the other hand, VKA was more frequently used anticoagulant medication (42 patients, 76.4%), followed by direct oral anticoagulant (DOAC) (13, 23.6%). The most common reason for AP use was a cardiovascular event [35/66 (43.2%); i.e., myocardial infarction] followed by a cerebrovascular event [25/66 (30.9%)]. The most common reasons for using AC were atrial fibrillation or cardiac valve surgery [47/53 (85.5%)]. The reasons for AT use were unknown in 13 patients who were using AP and 2 patients who were using AC. The median age of group A was significantly higher than that of group B (79.0 vs. 71.0, p < 0.0001). IPH was found in 42 (35.9%) patients in group A and 133 (48.2%) patients in group B (p = 0.0268). Eighteen (15.4%) patients in group A and 79 (28.6%) patients in group B had extracranial injuries (p = 0.0049).
Clinical outcomes
As shown in Table 1, 51 (43.6%) patients in group A and 159 (57.6%) patients in group B had mRS 0–2 at discharge (p = 0.0113). Thirty (25.6%) patients in group A and 45 (16.3%) patients in group B died within 30 days of their injuries occurring (p = 0.0356). On the other hand, the incidence of hematoma enlargement did not differ significantly between groups A and B (31.6% vs 33.6%, p = 0.7960). The incidence of neurological death also did not differ significantly between the groups (71.4% vs 78.3%, p = 0.5809). In the multivariate analyses (Table 2), the independent risk factors for poor outcome were found to be higher age (OR 32.7, p < 0.0001), female (OR 1.77, p = 0.0285), VKA use (OR 2.36, p = 0.0297), and hematoma enlargement within 72 h (OR 3.73, p < 0.0001).
Sub-analyses revealed that hematoma enlargement occurred in 21 of 44 (47.7%) patients that were being treated with AC and in 87 of 283 (30.7%) patients that were not being treated with such drugs. Hematoma enlargement also occurred in 80 of 146 (54.8%) patients in whom IPH was detected on the 1st CT scan and in 28 of 181 (15.5%) patients in which IPH was not detected on the 1st CT scan. AC use and the presence of IPH on the 1st CT exhibited significant associations with hematoma enlargement (p = 0.0376 and p < 0.0001, respectively). The use of AP, however, was not associated with hematoma enlargement (22.7% vs 35.6%, p = 0.0565).
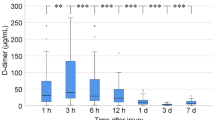
The duration of the period from arrival to hematoma enlargement did not differ significantly between groups A and B (4 vs. 3 h, p = 0.4613). In almost all cases, hematoma enlargement occurred within 24 h, regardless of whether the patient was taking AT. Only 1 patient without AT was detected hematoma enlargement after 50 h from onset because 2nd CT was not performed until then.
Reversal agent for AC
In 55 patients of AC user, 9 patients received 4F-PCC in addition to Vit. K2, 20 patients received Vit. K2 only, and 1 patient received Idarucizumab as a reversal agent for AC. The median INR on arrival was 1.7 (IQR 1.3–2.3) in patients without reversal agent, 2.3 (IQR 2.1–2.5) in patients with 4F-PCC, and 2.4 (IQR 1.7–3.4) in patients with Vit.K2 only. There was significant difference in reversal agent users and in non-users (2.3 vs 1.7, p = 0.0095), and there was no significant difference in patients with 4F-PCC and in patients with Vit. K2 only (p = 0.9436). Hematoma expansion occurred in 7 of 20 patients (35.0%) who were not used reversal agents, in 3 of 9 patients (33.3%) reversed by 4F-PCC, and in 13 of 20 patients (65%) reversed by Vit. K2 only. Hematoma expansion tend to be occurred less frequently in patients with 4F-PCC than in patients with Vit. K2 only, although there was no significant difference (p = 0.2256).
Thromboembolic events
Repeated CT or MRI were performed in all patients of group A and 242 patients (87.7%) of group B. There were totally 7 patients of ischemic stroke after admission (Fig. 2) and no patients of MI, PE or VTE in this study. Ischemic stroke occurred in 5 patients (4.3%) of group A and in 2 patients (0.8%) of group B, and incidence of ischemic stroke was significantly higher in group A (p = 0.0396). In group A, 3 of 30 patients (10%) with reversal agent and 2 of 87 patients (2.3%) without it had ischemic stroke. Ischemic stroke tended to be occurred more frequently in patients with reversal agent than in patients without it, although there was no significant difference (p = 0.1057). Furthermore, ischemic stroke was occurred in 2 of 9 patients (22.2%) reversed by 4F-PCC and in 1 of 20 patients reversed by only Vit. K2. Ischemic stroke tend to be more frequent in patients used 4F-PCC. In group A, all ischemic strokes occurred by day 31 after the injury. Three of 5 patients in group A suffered ischemic stroke before AT was restarted. In a patient used 4F-PCC, an ischemic stroke occurred on day 1.

The incidence of ischemic stroke in patients with traumatic intracranial hemorrhage. There was significant difference in the incidence of ischemic stroke between AT users and AT non-users. And ischemic stroke tend to be occurred in reversal agent users, especially in 4F-PCC users.
Rebleeding after resumption of AT
AP was restarted in 21 of 79 patients (26.6%), and AC was restarted in 35 of 55 patients (63.6%). The median days from admission to resumption was 6 (IQR 3–11) days. Rebleeding occurred in 2 cases in which AC was restarted within 2 days of the injury, and these events made the patients’ outcomes worse. There were no cases of rebleeding in AP users and in AT non-users.
Discussion
This study investigated the clinical characteristics and outcomes of head trauma patients with intracranial hemorrhage that were taking AT. The features of clinical characteristics of AT users were lower frequencies of IPH and extracranial injuries compared with the patients that were not taking AT. In case of high-energy trauma, IPH and extracranial injury may increase. These clinical features suggest that tICH was occurred more frequently in AT users than in non-users even in cases of low-energy trauma, which is consistent with past literature6. The comparison between two groups showed that pre-injury AT was associated with unfavorable outcome. Furthermore, multivariate analysis revealed that VKA use, as well as higher age, female gender, and hematoma expansion within 72 h, but not AP or DOAC use, were associated with unfavorable outcome.
Pre-injury use of AC, especially VKA, was reported to be associated with increase mortality following head trauma6,7,8,9. A retrospective cohort study revealed that the adjusted OR for 30-day mortality of VKA users was 8.3 (95% CI 2.0–34.8)9. Another retrospective study also revealed that VKA was a significant predictor of the progression of IPH after head trauma compared with non-use of VKA (OR 5.30, 95% CI 2.48–11.31)6. In contrast, the influence of pre-injury use of AP for outcome is conflicting. A meta-analysis indicated that patients with AP had a higher risk of IPH and hematoma expansion compared with patients without AP after mild head trauma10. A multicenter retrospective observational study also revealed that AP was a risk factor for unfavorable outcome in patients with head trauma7. They reported that the risk of hematoma enlargement in the patients using AP was two-fold higher and the risk of a poor outcome was 50% higher (relative risk 1.58, 95% CI 1.28–1.95)7. On the other hand, a large cohort study showed that no increased hematoma enlargement in patients with AP and no increased mortality risk in patients with SAPT6. These differences of influence of AP for outcome and hematoma enlargement after head trauma might be caused by biases of clinical characteristics. The results of this study suggest that the influence of AP on outcome and hematoma enlargement is smaller than that of VKA.
In this study, almost all cases of hematoma enlargement detected within 24 h after the initial injury, regardless of whether the patients were using AT. On the other hand, the time from the injury to hemostasis being achieved could not be examined. Two retrospective study of spontaneous IPH reported that most hematoma enlargement occurred within 24 h from onset11,12. In contrast, a prospective cohort study of spontaneous IPH with VKA revealed that VKA users were at risk for bleeding well beyond 24 h13. To our knowledge, there are no reports that investigated the timing of hemostasis after head injury with AT. In this study, pre-injury AC was associated with hematoma enlargement within 72 h. In addition, pre-injury VKA and hematoma enlargement were associated with unfavorable outcome. Scotti et al. revealed that the patients with DOAC had substantially lower rates of IPH progression compared with the patients with VKA6. From these results, it is speculated that aggressive treatment by reversal agents for pre-injury VKA is important.
Two randomized controlled trials of 4F-PCC vs. Vit. K2 or plasma for cases of spontaneous IPH involving patients that were taking VKA showed that 4F-PCC had a superior ability to rapidly reduce the INR4,14. In addition, 4F-PCC reduced the frequencies of hematoma enlargement and hematoma-related early death in spontaneous IPH patients15. In this study, although there were no significant differences, the hematoma expansion rate was halved in the patients administered 4F-PCC compared with the patients reversed by Vit.K2 only. The use of 4F-PCC might thus be effective to reduce hematoma expansion after head trauma.
As the number of patients treated with reversal agents has increased, on the other hand, the frequency of thromboembolic events may increase. In this study, ischemic strokes occurred in 2 of the 9 patients (22.2%) in which 4F-PCC was used and this rate was relatively higher than in patients using Vit. K2 only (5%). To prevent thromboembolic events, the early resumption of AC might be necessary. In a retrospective study of chronic subdural hematomas, early resumption of AT was recommended because many thromboembolic events occurred within one month of drug withdrawal16. In a meta-analysis of spontaneous IPH, the resumption of AC between days 10 and 39 after onset produced good results2. In this study, there were 2 cases of rebleeding after AC was restarted within 2 days of admission. And these event influenced their outcomes. To determine the timing of resumption of AT for tICH cases, we need to collect more cases.
Limitations of this study
This study was retrospective, and hence, background factor variability was its greatest limitation. As these differences of background likely influenced the treatment outcome, multivariate analysis was performed to reduce the bias. Nevertheless, because this was a retrospective study, biases could not be eliminated. In addition, an important limitation to the present study is the potential for underestimation of hematoma enlargement. Hematoma formation mainly occurred during initial a few hours from injury, so the detection rate of hematoma enlargement depend on the duration from injury to first CT scan. In this study, however, the time from injury to the first CT scan was not evaluated because of data missing. As a result, the amount of hematoma enlargement might be underestimated. Furthermore, treatment for head trauma, the timing of repeat CT or MRI, and whether additional CT scans were performed or not were decided at the discretion of the doctor in charge. These differences might be affected the outcomes, the rate of ischemic stroke and the rate of rebleeding. Furthermore, it was difficult to classify ischemic stroke, which occurred by thromboembolism or direct injury. Because there were small number of cases, the efficacy of reversal agents, resumption of AT, and the timing of resumption are still controversial. A prospective cohort study is needed to provide more accurate data about the outcomes of head trauma among patients taking AT.
In conclusion, patients that are taking AT are at high risk of a poor prognosis after head trauma, even after low-energy head trauma. The prognosis of those that exhibit pre-injury VKA and acute hematoma enlargement are poor, and active hemostasis, such as using reversal agents, could improve the outcomes.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Fabbri, A., Servadei, F., Marchesini, G., Stein, S. C. & Vandelli, A. Early predictors of unfavorable outcome in subjects with moderate head injury in the emergency department. J. Neurol. Neurosurg. Psychiatry 79, 567–573 (2008).
Chang, E. F., Meeker, M. & Holland, M. C. Acute intraparenchymal hemorrhage: Risk factors for progression in the early post-injury period. Neuryosurgery 58, 647–656 (2006).
Chieregato, A. et al. Factors associated with neurological outcome and lesion progressioin in traumatic subarachnoid hemorrhage patients. Neurosurgery 56, 671–680 (2005).
Sarode, R. et al. Efficacy and safety of a 4-factor prothrombin complex concentrate in patients on vitamin K antagonists presenting with major bleeding: A randomized, plasma-controlled, phase IIIb study. Circulation 128, 1234–1243 (2013).
Kothari, R. U. et al. The ABCs of measuring intracerebral hemorrhage volumes. Stroke 27, 1304–1305 (1996).
Scotti, P. et al. Antithrombotic agents and traumatic brain injury in the elderly population: Hemorrhage patterns and outcomes. JNS 133, 486–495 (2020).
Fabbri, A. et al. Antiplatelet therapy and the outcome of subjects with intracranial injury: The Italian SIMEU study. Crit. Care 17, R53 (2013).
Macki, M. et al. The effect of antithrombotics on hematoma expansion in small- to moderate-sized traumatic intraparenchymal hemorrhages. World Neurosurg. 149, e101–e107. https://doi.org/10.1016/j.wneu.2021.02.072 (2021).
Narum, S., Brørs, O., Stokland, O. & Kringen, M. K. Mortality among head trauma patients taking preinjury antithrombotic agents: A retrospective cohort analysis from a Level 1 trauma centre. BMC Emerg. Med. 16, 29 (2016).
Fiorelli, E. M. et al. Incremental risk of intracranial hemorrhage after mild traumatic brain injury in patients on antiplatelet therapy: Systematic review and meta-analysis. J. Emerg. Med. 59, 843–855 (2020).
Fujii, Y. et al. Hematoma enlargement in spontaneous intracerebral hemorrhage. JNS 80, 51–57 (1994).
Lim-Hing, K. & Rincon, F. Secondary hematoma expansion and perihemorrhagic edema after intracerebral hemorrhage: From bench work to practical aspects. Front. Neurol. 8, 74 (2017).
Flibotte, J. J., Hagan, N., O’Donnell, J., Greenberg, S. M. & Rosand, J. Warfarin, hematoma expansion, and outcome of intracerebral hemorrhage. Neurology 63, 1059–1064 (2004).
Goldstein, J. N. et al. Four-factor prothrombin complex concentrate versus plasma for rapid vitamin K antagonist reversal in patients needing urgent surgical or invasive interventions: A phase 3b, open-label, non-inferiority, randomised trial. Lancet 385, 2077–2087 (2015).
Steiner, T. et al. Fresh frozen plasma versus prothrombin complex concentrate in patients with intracranial haemorrhage related to vitamin K antagonists (INCH): A randomised trial. Lancet Neurol. 15, 566–573 (2016).
Fornebo, I. et al. Role of antithrombotic therapy in the risk of hematoma recurrence and thromboembolism after chronic subdural hematoma evacuation: A population-based consecutive cohort study. Acta Neurochir. 159, 2045–2052 (2017).
Author information
Authors and Affiliations
Contributions
T.K. and Y.K. were involved in the study conception and design, the data acquisition and analysis, and the writing and drafting of the manuscript. M.G. and T.T. were involved in the study conception and data acquisition. Y.M. and E.I. were involved in the study conception and the drafting of the manuscript. The authorship requirements have been met by all of the authors. All of the authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Koiso, T., Goto, M., Terakado, T. et al. The effects of antithrombotic therapy on head trauma and its management. Sci Rep 11, 20459 (2021). https://doi.org/10.1038/s41598-021-00091-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-00091-2
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
