
Abstract
Patients undergoing knee joint replacement (KJR) are at high risk of postoperative venous thromboembolism (VTE), but data on the time trends of VTE rate in this population are sparse. In this analysis of the German nationwide inpatient sample, we included all hospitalizations for elective primary KJR in Germany 2005–2016. Overall, 1,804,496 hospitalized patients with elective primary KJR (65.1% women, 70.0 years [IQR 63.0–76.0]) were included in the analysis. During hospitalization, VTE was documented in 23,297 (1.3%) patients. Total numbers of primary KJR increased from 129,832 in 2005 to 167,881 in 2016 (β-(slope)-estimate 1,978 [95% CI 1,951 to 2,004], P < 0.001). In-hospital VTE decreased from 2,429 (1.9% of all hospitalizations for KJR) to 1,548 (0.9%) cases (β-estimate − 0.77 [95% CI − 0.81 to − 0.72], P < 0.001), and in-hospital death rate from 0.14% (184 deaths) to 0.09% (146 deaths) (β-estimate − 0.44 deaths per year [95% CI − 0.59 to − 0.30], P < 0.001). Infections during hospitalization were associated with a higher VTE risk. VTE events were independently associated with in-hospital death (OR 20.86 [95% CI 18.78–23.15], P < 0.001). Annual number of KJR performed in Germany increased by almost 30% between 2005 and 2016. In parallel, in-hospital VTE rates decreased from 1.9 to 0.9%. Perioperative infections were associated with higher risk for VTE. Patients who developed VTE had a 21-fold increased risk of in-hospital death.
Similar content being viewed by others


Introduction
Knee joint replacement (KJR) surgery is one of the most common orthopedic procedures currently performed in the ageing populations of Western countries1. In the year 2010, the number of KJR procedures performed in the United States increased to more than 700,000 per year2. It has been foreseen that this number will further grow to approximately 3.5 million KJR procedures by the year 20302. Although this operation is one of the most successful and life-changing interventions available today1 and can substantially improve mobility and quality of life, these patients are characterized by high risk for perioperative venous thromboembolism (VTE), presenting as deep vein thrombosis and/or pulmonary embolism (PE), even in the era of established pharmacological thromboprophylaxis1,2,3,4,5,6. The release of thromboplastins from the dissected soft tissue and reamed bone, as well as venous stasis both initiated during surgery and the postoperative immobility, provoke a high rate of VTE events1.
Without thromboprophylaxis, the rate of proximal deep vein thrombosis after KJR surgery was reported to be between 5 and 22%, that of PE of 1.5–10%2,6,7. This risk can be reduced substantially by the use of pharmacological thromboprophylaxis and with a three-month cumulative incidence of symptomatic VTE falling to 2.3%2,8.
With increasing numbers of KJR procedures in western countries2,6,9,10,11, the number of VTE events is expected to rise2,6. Actual data about temporal trends regarding total numbers of performed KJR and particularly the impact of VTE on in-hospital mortality of KJR patients is sparse. This knowledge for optimizing secondary prevention strategies in this patient population. Thus, the aims of our study were to investigate, (a) temporal trends in the total numbers of KJR performed in Germany between 2005 and 2016, including trends in the patients’ age as well as comorbidities; (b) the total burden and temporal trends of VTE complications following KJR; (c) the impact of VTE on mortality rates in KJR patients; and (d) predictors of VTE during hospitalization.
Results
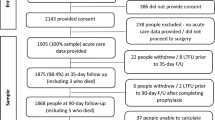
A total of 1,804,496 hospitalizations were recorded for elective (primary) KJR in Germany from 2005 to 2016 and were included in the present analysis (see Fig. S1 in the supplementary material for study flow chart). Among these, the majority of patients hospitalized (65.1%) were women, and 53.4% were 70 years or older (median 70.0 years [IQR 63.0–76.0]). The estimated average crude annual incidence of elective primary KJR was 221.0 KJR per 100,000 population-years during this time period.
Temporal trends of primary surgical knee joint replacements, patients’ baseline characteristics and in-hospital events
The total number of KJR performed as well as in-hospital death rates increased substantially with age (Fig. 1A). While men were more frequently represented than women in the first three decades of life, the proportion of women was higher among patients aged 30 years and older (Fig. S2C in the supplementary material).

Time trends in absolute number of hospitalizations, in-hospital mortality and VTE rate in patients undergoing elective primary KJR in Germany from 2005 to 2016. (A) Total numbers of patients undergoing elective primary KJR (grey bars) and in-hospital death rate (orange line), stratified per decade of age, over the entire period 2005–2016 (cumulative data). (B) Annual total numbers of patients undergoing elective primary KJR (grey bars) and corresponding annual in-hospital death rates (orange line) in Germany in the period 2005–2016. (C) Percentage of patients undergoing elective primary HJR who developed in-hospital VTE (light blue bars); the panel further shows percentage of deep vein thrombosis and thrombophlebitis (DVT, light blue line), pulmonary embolism (PE, admiral blue line), and high-risk PE with hemodynamic instability (dark blue line).
The total number of patients who underwent KJR in Germany increased from 129,832 in the year 2005 to 167,881 in 2016 (β-(slope)-estimate 1,978 [95% CI 1,951 to 2,004] increase per year, P < 0.001). A total of 2,112 patients undergoing elective primary KJR died during the in-hospital stay for an overall perioperative death rate of 0.1%. The crude annual in-hospital death rate decreased from 0.14% (184 deaths) to 0.09% (146 deaths) of KJR-related hospitalizations (β-estimate − 0.4 deaths per year [95% CI − 0.6 to − 0.3], P < 0.001) over the time period studied (Fig. 1B, Table S2 in the supplementary material). The median duration of hospitalization for KJR decreased from 15 (13–16) days in 2005 to 10 (8–12) in 2016 (β-estimate − 0.12 [95% CI − 0.12 to − 0.12], P < 0.001) (Fig. 2A) and was primarily depending on patients’ age (Fig. S3 in the supplementary material).

Time trends in length of hospitalization and rates of serious complications in patients undergoing elective primary KJR in Germany from 2005 to 2016. (A) Median duration of hospitalization (solid black line) with 25% and 75% IQR (dashed black lines). (B) Percentage of patients developing shock (dark blue bars) and undergoing cardio-pulmonary resuscitation (CPR, light blue bars) out of all patients undergoing elective KJR. (C) Percentage of patients with bleeding events such as intracerebral bleeding (ICB, light red bars), subarachnoid bleeding (SAB, dark red bars) and gastrointestinal bleeding (GIB, orange bars) as well as necessitation for transfusions of blood constituents (red line) out of all patients undergoing elective KJR.
The proportion of patients aged 70 years or older among those who underwent KJR, decreased from 54.0% in 2005 to 50.3% in 2016 (β-estimate − 0.14 [95% CI − 0.15 to − 0.13], P < 0.001). In parallel, the prevalence of some important comorbidities such as cancer and coronary artery disease decreased during the same timeframe (Fig. S2B + C, Fig. S4 and Table S1 in the supplementary material). Although females outweighed male patients with regard to KJR performed throughout the entire study period, the proportion of male patients increased slightly over time (Fig. S2A and Table S1 in the supplementary material). The rate of myocardial infarction, stroke, intracerebral bleeding complications as well as necessity of transfusions of blood constituents decreased (Fig. 2B + C, Fig. S5 and Table S2 in the supplementary material).
Thromboembolic complications in patients undergoing elective knee joint replacement
A VTE event was recorded in 23,297 (1.3%) patients during hospitalization, presenting as deep venous thrombosis or thrombophlebitis (DVT) in 19,535 (83.9%) and of PE in 5,040 (21.6%) cases. Importantly, haemodynamic instability was recorded in 10.9% of the patients who suffered acute PE in-hospital. VTE events and consistently its subentities decreased over time. While 2,429 (1.9%) patients operated for KJR suffered VTE in hospital in the year 2005, only 1,548 (0.9%) VTE were recorded in 2016 (β-estimate − 0.77 [95% CI − 0.81 to − 0.72], P < 0.001). The rate of DVT (1.6% in 2005 to 0.8% in 2016; β-estimate − 0.82 [95% CI − 0.87 to − 0.77], P < 0.001) and PE (0.4% in 2005 to 0.2% in 2016; β-estimate − 0.52 [95% CI − 0.61 to − 0.42], P < 0.001) were reduced by almost 50% (Fig. 1 and Table S2 in the supplementary material). The number of VTE events increased with the patients’ age (β 0.14 [0.12 to 0.15], P < 0.001) (Fig. 1A).
Patients undergoing primary KJR who suffered VTE during hospitalization were more often women (72.5% vs. 65.0%, P < 0.001), older (72.0 [65.0–77.0] vs. 70.0 [63.0–76.0] year, P < 0.001), and more often obese (27.9% vs. 22.9%, P < 0.001) compared to those without VTE (Table 1). Typical risk factors for thrombosis such as cancer (1.4% vs. 0.8%, P < 0.001) and thrombophilia (whenever sought and detected; 0.3% vs. 0.1%, P < 0.001), were more prevalent in patients with VTE. Patients with VTE more frequently revealed cardiovascular, renal and respiratory comorbidities (Table 1). In-hospital infections such as pneumonia (2.8% vs. 0.3%, P < 0.001), urinary tract infections (5.2% vs. 2.8%, P < 0.001), and sepsis (0.26% vs. 0.04%, P < 0.001) all were more often recorded in association with VTE. Finally, myocardial infarction (0.6% vs. 0.2%, P < 0.001) and stroke (0.6% vs. 0.2%, P < 0.001) also were more frequently reported in patients with VTE (Table 1). The rate of infectious complications remained largely unchanged over time (Figures S5 as well as Table S2 in the supplementary material). At multivariable analysis, cancer, heart failure as well as infections such as sepsis, pneumonia, and urinary tract infection were independently associated with VTE events during the hospital stay (Table 2).
In patients undergoing primary KJR, the risk of death was 22-fold higher if they suffered VTE compared to patients without VTE (2.2% vs. 0.1%, P < 0.001) (Table 1). In the logistic regression models, VTE increased the risk of dying during hospitalization univariably (OR 25.65 [95% CI 23.22–28.34], P < 0.001), but also independently from age, sex and comorbidities (OR 20.86 [95% CI 18.78–23.15], P < 0.001). The impact of VTE on in-hospital varied annually (Table S3 in the supplementary material). In addition, we analysed the total numbers of in-hospital deaths in patients undergoing primary KJR at each day of hospitalization (day 1–15) and the proportion of deaths, which were related to prior VTE events during hospitalization at each day. The proportion of VTE related death was highest at the first 7 days after admission and decreased over the hospitalization period (Fig. 3). As expected, bleeding complications such as intracerebral and gastrointestinal bleeding as well as transfusions of blood components were more often detected in KJR patients with VTE (Table 1). The rate of VTE and bleeding complications remained low and decreased over time, as did the need for transfusions of blood constituents (Figs. 2C and 3C as well as Table S2 in the supplementary material). The length of in-hospital stay was in median 12.0 days (IQR 10.0–14.0) and was longer in patients with (14 [12–18]) vs. without (12 [10–14] days) VTE (P < 0.001; Table 1). VTE occurrence was associated with hospitalization longer than 14 days (crude: OR 3.09 [95% CI 3.01–3.18], P < 0.001]; adjusted model: OR 3.09 [95% CI 3.00–3.18], P < 0.001). This result remained stable after additional adjustment for the year of hospitalization (OR 3.11 [95% CI 3.02–3.20], P < 0.001). Nevertheless, the impact of VTE regarding prolonged hospitalization increased slightly over time (Table S4 in the supplementary material).

Time trend regarding cumulative number of deaths during the hospitalization period in patients undergoing elective primary KJR in Germany from 2005 to 2016. Total numbers of in-hospital deaths at the different hospitalization days (black bars), in-hospital deaths of patients undergoing elective primary KJR with VTE (green bars) and proportion of deaths in conjunction with VTE. Only the in-hospital deaths of the first 15 days after admission were taken into account.
Discussion
VTE, with its clinical manifestations of DVT and PE, is responsible for significant morbidity and mortality in Europe and worldwide5,12. Important major provoking risk factors of VTE are represented by orthopaedic-related issues, notably major trauma and surgery, lower-limb fracture, joint replacement, and spinal cord injury5.
Our study results demonstrate an increasing demand and rising annual numbers of performed KJR in the aging western populations, in line with what described in other high-income states2,6,8,9,10,11. These temporal trends regarding total numbers of KJR and perioperative complications are important for adequate management of public health as well as health care service planning. Although KJR can substantially improve patients` mobility and quality of life in patients with advanced gonarthritis, it is accompanied by a high risk of VTE2,13,14,15,16. While without thromboprophylaxis, the rate of DVT in screening examinations in patients undergoing KJR was reported as approximately 60% (including symptomatic as well as asymptomatic DVT events)13,14, the risk of VTE after KJR can be significantly decreased by the use of pharmacological thromboprophylaxis2. In accordance with results from studies of KJR conducted in other states reporting a 1.1% in-hospital VTE rate after KJR17, we identified an in-hospital VTE rate of 1.3% in patients undergoing elective KJR in Germany. Importantly for adequate health care planning, the VTE rate decreased significantly from 1.9% in 2005 to 0.9% in 2016. This favorable trend may be due to several factors, including the introduction of the direct oral anticoagulants, the decrease in the use of tourniquets and/or surgical time of tourniquet use, a small increase in the number of uncemented KJR procedures18, the incline in unicondylar KJR18, decreasing age and the introduction of fast-track procedures improving early mobilization and discharge19,20.
Current practice guidelines provide partly conflicting recommendations for the medical VTE prophylaxis after KJR21,22. Additionally, the appropriate duration of anticoagulation following elective KJR is highly controversial and a dynamically evolving topic. Country-specific guideline recommendations as well as physicians’ and patients’ preferences, have a major impact on the management strategies. While the German AWMF guidelines recommend low-molecular weight heparins (LMWH), fondaparinux or novel oral anticoagulants (NOAC) at a prophylactic dose for 11–14 days after KJR22, the National Institute of Health and Care Excellence guidelines (NICE) in the United Kingdom recommend LMWH, or NOACs, with aspirin recommended for extended prophylaxis21,23. The guidelines of the American College of Chest Physicians and the American Association of Orthopaedic Surgeons recommend LMWH, (N)OACs or aspirin3,6,7,21,24.
There is still a great controversy about the effect of tourniquets on development of VTE after KJR25,26,27,28. The use of a tourniquet improves visualization during KJR surgery and may shorten the operating time28. However, there is also some evidence that the use of tourniquet during KJR surgery may lead to increased numbers of DVT25,26,27,28. Furthermore, previous studies have reported that cemented fixation as compared to cement-less fixation was found as a risk factor for VTE in hip and KJR29,30; nevertheless, the role of cement as a thrombogenic agent and cause of emboli during or after joint replacements is not entirely clear to date30,31,32. In Germany more than 90% of the KJR were operated with cement fixation18. Finally, the decreasing proportion of VTE in KJR patients may partly be explained by trends regarding patients’ age during the observational period. It is known that the incidence of VTE grows exponentially with age33,34,35. The proportion of patients aged ≥ 70 years decreased from 2005 to 2016, and this may have contributed to the decrease of the proportion of VTE events in KJR.
We confirmed the role of relevant predictors of VTE, such as age19,36,37, cancer37, female gender38, obesity37,39 as well as heart failure37,40, AF41, peripheral artery disease42, COPD43,44, and renal insufficiency45. In addition, acute cardiovascular events during hospitalization for elective KJR such as myocardial infarction40,46 and stroke37,47, but also infections48 occurring during hospitalization were significantly associated with VTE development, although our study design does not permit speculation about cause and effect. In fact, our results demonstrated that systemic infectious diseases (pneumonia and sepsis) were accompanied with a higher VTE risk than traditional VTE risk factors like cancer and thrombophilia. VTE events in patients undergoing primary KJR were associated with a significant 3.1-fold risk of prolonged hospitalization (beyond 14 days).
Our study highlights that perioperative VTE events aggravate the early prognosis of patients operated at the knee joint: perioperative VTE events were associated with a 21-fold increased risk of in-hospital deaths independently from age, sex and comorbidities. In parallel with reduction of VTE events, the KJR patients’ in-hospital mortality decreased from 2005 to 2016. In addition, we detected a decreasing rate of periprocedural myocardial infarction, stroke and major bleeding, which might have contributed to this mortality reduction.
Although the median duration of hospitalization for elective KJR decreased from 15 days in the year 2005 to 10 days in the year 2016, the median length of stay in the year 2016 was still substantially longer in Germany than in the United Kingdom (6 days in regular medical care and 3 days for enhanced recovery programs)49 or in the United States (4 days)50. In other European countries, enhanced recovery protocols have been adopted, resulting in short length of hospitalization of only 2 days (in median)20. Interestingly, enhanced recovery with halved length of in-hospital stay was accompanied by lower rate of cardiac ischemic events and lower mortality rate at 30 and 90 days follow-up after KJR and hip joint replacement49.
Recent studies of nationwide cohorts reported that patients treated according these protocols had a low 90-day VTE rate of 0.39%20. The results of these mentioned studies contributed to fuel the discussion on whether prolonged pharmacological thromboprophylaxis (after discharge from hospital) is beneficial and needed for all patients treated with an enhanced recovery protocol and hospitalized for a period of 5 days or shorter19,20. In these patients, a preventive strategy based on in-hospital thrombo-prophylactic treatment with the Factor Xa inhibitor rivaroxaban followed by low-dose aspirin appeared to be effective and safe for thromboprophylaxis50. These results remain to be confirmed in other countries, in which fast-track surgery and enhanced recovery protocols will be introduced or were introduced more recently21.
The key strength of our present analysis of the German nationwide inpatient sample is the very large number of unselected patients undergoing KJR, presenting real-world and practice-based data without selection bias. On the other hand, since our study results are based on ICD discharge codes and OPS diagnostic, procedural and/or surgical coding, it has to be mentioned that misclassification of clinical events, underestimation of event rates driven by underreporting or undercoding by the hospital personnel cannot be excluded. Additionally, we could not analyze any possible repeated hospitalizations of the same patient. A further limitation of our study is the focus on the in-hospital period without assessment of events after discharge, which may also potentially lead to an underestimate of the total number of postoperative VTE events. Due to coding reasons, we were not able to distinguish between unilateral and bilateral KJR. Nevertheless, it has been published that the proportion of bilateral KJR during one hospitalization is < 4% in Germany51. Neither prior VTE, nor anticoagulant, antiplatelet treatment or tranexamic acid use were assessed in the German nationwide inpatient sample. Thus, the potential impact of these factors on occurrence of VTE after KJR could not be analyzed, which has to be mentioned as a further limitation of our study52. As per routine clinical practice, venous ultrasound to diagnose DVT was primarily performed in symptomatic patients. It must be considered that the results from the German nationwide sample may not be generalizable for other geographic regions, countries, and health systems.
In conclusion, perioperative VTE was recorded in 1.3% of the KJR patients during hospitalization. While the number of KJR increased in Germany from 2005 to 2016, the rate of VTE events decreased from 1.9% in the year 2005 to 0.9% in 2016. VTE events in patients undergoing primary elective KJR were associated with a 21-fold risk of in-hospital death rates and a 3.1-fold risk for prolonged hospitalization.
Patients and methods
Data source
The analyses of our study were run on our behalf by the Research Data Center (RDC) of the Federal Statistical Office and the Statistical Offices of the federal states in Wiesbaden, Germany (source: RDC of the Federal Statistical Office and the Statistical Offices of the federal states, DRG Statistics 2005–2016, own calculations). Priorly, we had provided the created SPSS scripts to the RDC. After computing the analyses by the RDC, we received the aggregated results of the statistics (SPSS software, version 20.0, SPSS Inc., Chicago, Illinois). For this study, we selected and included all surgical patients with elective primary KJR hospitalized in the timeframe between January 2005 and December 2016 in German hospitals. Since we intended to focus only on hospitalized patients with elective primary procedures, we excluded patients with acute fractures. The study flow was described in part previously53,54,55,56. The study results are not part of the routine work of the RDC, but is an analysis especially done for our needs and proposed contents (see Fig. S1 in the supplementary material for study flow chart).
Ethical aspects and study oversight
As described above, the investigators had no access to data of individual patients, but only to aggregated results provided by the RDC. Thus, approval by an ethics committee and patients’ informed consent were not required, in accordance with German law. The study was prepared according to STROBE recommendations.
Diagnosis and procedural codes
In the year 2004, diagnosis- and procedure-related remuneration system was introduced in Germany with the German Diagnosis Related Groups (G-DRG) system. Data about patients’ diagnoses were gathered by the RDC of the Federal Statistical Office and the Statistical Offices of the federal states in Wiesbaden (Germany). The diagnoses are coded according to the International Classification of Diseases and Related Health Problems with German Modification (10th Revision with German Modification-ICD-10-GM), and the performed patients’ diagnostic, surgical and interventional procedures are coded according to the German Procedure Classification (OPS, surgery and procedures codes [Operationen- und Prozedurenschlüssel])35,52.
In our study, we included all hospitalizations, which refer to surgical patients undergoing elective primary KJR in Germany from the year 2005 to the year 2016. All hospitalized patients with primary KJR were identified based on the OPS code 5–822, after exclusion of patients with revision-surgery or replacement of existing prostheses (OPS-code 5–823) as well as acute fractures (excluding patients with distal femur fracture (ICD-code S72.4) and proximal tibia fracture (ICD-code S82.1)52.
Study outcomes
The outcomes of this study were defined as VTE (including deep venous thrombosis or thrombophlebitis (DVT, ICD codes I80, I81, I82) and/or PE (ICD code I26)), prolonged hospitalization (of more than 14 days) and death from any causes, respectively recorded during hospital stay.
Statistical methods
Descriptive statistics for patient characteristics of KJR patients with and without perioperative VTE were provided as median and interquartile range (IQR) or absolute numbers and corresponding percentages. The Mann–Whitney-U test was used to test the continuous variables of the groups regarding differences and categorical variables were compared with chi2 test or Fisher’s exact test, as appropriate52.
We analysed total numbers and incidence of VTE events in elective KJR in Germany between the years 2005 and 2016 and tested for temporal trends of VTE incidence and in-hospital death rate using linear regression models. Results are presented as estimated slope beta (β)-estimates and corresponding 95% confidence intervals (CI)35.
In addition, we analysed univariate and multivariable logistic regression models in order to detect influences regarding possible predictors of VTE events. Furthermore, we analysed the association between VTE and in-hospital death as well as VTE and prolonged hospitalization (of more than 14 days). These results of our study are presented as odds ratio (OR) and 95% CI. Multivariable regression models were adjusted for age, sex, obesity, cancer, coronary artery disease, heart failure, atrial fibrillation/flutter (AF), essential arterial hypertension, chronic obstructive pulmonary disease (COPD), acute and chronic renal failure, and diabetes mellitus. These covariates were selected a priori since they represent known risk factors for VTE and in-hospital death. The software SPSS (version 20.0; SPSS Inc., Chicago, Illinois) was used for computerised analysis. P values of < 0.05 (two-sided) were considered to be statistically significant53,54,55,56.
Abbreviations
- AF:
-
Atrial fibrillation/flutter
- CI:
-
Confidence interval
- COPD:
-
Chronic obstructive pulmonary disease
- DRG:
-
Diagnosis related groups
- DVT:
-
Deep venous thrombosis or thrombophlebitis
- ICD:
-
International Classification of Diseases and Related Health Problems
- IQR:
-
Interquartile range
- KJR:
-
Knee joint replacement
- LMWH:
-
Low-molecular weight heparins
- NOAC:
-
Novel oral anticoagulant
- OAC:
-
Oral anticoagulant
- OPS:
-
Diagnostic, surgery and interventional procedures codes (Operationen- und Prozedurenschlüssel)
- OR:
-
Odds ratio
- PE:
-
Pulmonary embolism
- RDC:
-
Research data center
- VTE:
-
Venous thromboembolism
References
Warwick, D. Prevention of venous thromboembolism in total knee and hip replacement. Circulation 125, 2151–2155 (2012).
Messerschmidt, C. & Friedman, R. J. Clinical experience with novel oral anticoagulants for thromboprophylaxis after elective hip and knee arthroplasty. Arterioscler. Thromb. Vasc. Biol. 35, 771–778 (2015).
Johanson, N. A. et al. American academy of orthopaedic surgeons clinical practice guideline on. Prevention of symptomatic pulmonary embolism in patients undergoing total hip or knee arthroplasty. J. Bone Joint Surg. Am. 91, 1756–1757 (2009).
Afshari, A. et al. European guidelines on perioperative venous thromboembolism prophylaxis: executive summary. Eur. J. Anaesthesiol. 35, 77–83 (2018).
Konstantinides, S.V., et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. (2019).
Falck-Ytter, Y. et al. Prevention of VTE in orthopedic surgery patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 141, e278S-e325S (2012).
Anderson, D. R. et al. American Society of Hematology 2019 guidelines for management of venous thromboembolism: prevention of venous thromboembolism in surgical hospitalized patients. Blood Adv. 3, 3898–3944 (2019).
Warwick, D. et al. Insufficient duration of venous thromboembolism prophylaxis after total hip or knee replacement when compared with the time course of thromboembolic events: findings from the Global Orthopaedic Registry. J. Bone Joint Surg. Br. 89, 799–807 (2007).
Wengler, A., Nimptsch, U. & Mansky, T. Hip and knee replacement in Germany and the USA: analysis of individual inpatient data from German and US hospitals for the years 2005 to 2011. DeutschesArzteblatt Int. 111, 407–416 (2014).
MaraditKremers, H. et al. Prevalence of total hip and knee replacement in the United States. J. Bone Joint Surg. Am. 97, 1386–1397 (2015).
Leitner, L. et al. Trends and economic impact of hip and knee arthroplasty in Central Europe: findings from the Austrian National Database. Sci. Rep. 8, 4707 (2018).
Barco, S., et al. Trends in mortality related to pulmonary embolism in the European Region, 2000–15: analysis of vital registration data from the WHO Mortality Database. Lancet Respir Med (2019).
Agnelli, G. Prevention of venous thromboembolism in surgical patients. Circulation 110, IV4-12 (2004).
Geerts, W. H. et al. Prevention of venous thromboembolism. Chest 119, 132S-175S (2001).
Kearon, C. Natural history of venous thromboembolism. Circulation 107, I22–I30 (2003).
Bjornara, B. T., Gudmundsen, T. E. & Dahl, O. E. Frequency and timing of clinical venous thromboembolism after major joint surgery. J. Bone Joint Surg. Br. 88, 386–391 (2006).
Januel, J. M. et al. Symptomatic in-hospital deep vein thrombosis and pulmonary embolism following hip and knee arthroplasty among patients receiving recommended prophylaxis: a systematic review. JAMA 307, 294–303 (2012).
rimberg, A., Jansson, V., Liebs, T., Melsheimer, O. & Steinbrück, A. Endoprothesenregister Deutschland (EPRD)—Jahresbericht 2016. https://www.eprd.de/fileadmin/user_upload/Dateien/Publikationen/Berichte/EPRD-Jahresbericht_2016_Einzelseiten_Online-Version.pdf. (2016).
Petersen, P. B., Jorgensen, C. C., Kehlet, H. & Lundbeck Foundation Centre for Fast-track Hip Knee Replacement Collaborative, G. Venous Thromboembolism despite ongoing prophylaxis after fast-track hip and knee arthroplasty: a prospective multicenter study of 34,397 procedures. Thromb.Haemost. 119, 1877–1885 (2019).
Petersen, P. B., Kehlet, H., Jorgensen, C. C. & Lundbeck Foundation Centre for Fast-track H, Knee Replacement Collaborative G. Safety of in-hospital only thromboprophylaxis after fast-track total hip and knee arthroplasty: a prospective follow-up study in 17,582 procedures. Thromb.Haemost. 118, 2152–2161 (2018).
Sidhu, V. S. et al. CRISTAL: protocol for a cluster randomised, crossover, non-inferiority trial of aspirin compared to low molecular weight heparin for venous thromboembolism prophylaxis in hip or knee arthroplasty, a registry nested study. BMJ Open 9, e031657 (2019).
Encke, A., et al. S3-Leitlinie Prophylaxe der venösen Thromboembolie (VTE). AWMF-Institut für Medizinisches Wissensmanagement (2015).
Venous thromboembolism in over 16s: reducing the risk of hospital-acquired deep vein thrombosis or pulmonary embolism. (National Institute for Health and Care Excellence, www.nice.org.uk/guidance/ng89, 2018).
Eikelboom, J. W., Karthikeyan, G., Fagel, N. & Hirsh, J. American Association of Orthopedic Surgeons and American College of Chest Physicians guidelines for venous thromboembolism prevention in hip and knee arthroplasty differ: what are the implications for clinicians and patients?. Chest 135, 513–520 (2009).
Mori, N. et al. Use of a pneumatic tourniquet in total knee arthroplasty increases the risk of distal deep vein thrombosis: a prospective, randomized study. Knee 23, 887–889 (2016).
Zan, P. et al. Release of the tourniquet immediately after the implantation of the components reduces the incidence of deep vein thrombosis after primary total knee arthroplasty. Bone Joint Res. 6, 535–541 (2017).
Harvey, E. J., Leclerc, J., Brooks, C. E. & Burke, D. L. Effect of tourniquet use on blood loss and incidence of deep vein thrombosis in total knee arthroplasty. J.Arthroplast. 12, 291–296 (1997).
Wang, K. et al. The effects of tourniquet use in total knee arthroplasty: a randomized, controlled trial. Knee Surg. Sports Traumatol.Arthrosc. 25, 2849–2857 (2017).
Zhang, Z. H. et al. Risk factors for venous thromboembolism of total hip arthroplasty and total knee arthroplasty: a systematic review of evidences in ten years. BMC MusculoskeletDisord. 16, 24 (2015).
Lindberg-Larsen, M. et al. Postoperative 30-day complications after cemented/hybrid versus cementless total hip arthroplasty in osteoarthritis patients > 70 years. Acta Orthop. 91, 286–292 (2020).
Clarke, M. T., Green, J. S., Harper, W. M. & Gregg, P. J. Cement as a risk factor for deep-vein thrombosis. Comparison of cemented TKR, uncementedTKR and cemented THR. J. Bone Joint Surg. Br. 80, 611–613 (1998).
Wong, K. L., Daguman, R., Lim, K., Shen, L. & Lingaraj, K. Incidence of deep vein thrombosis following total hip arthroplasty: a Doppler ultrasonographic study. J. Orthop. Surg. (Hong Kong) 19, 50–53 (2011).
Torbicki, A. et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur. Heart J. 29, 2276–2315 (2008).
Oger, E. Incidence of venous thromboembolism: a community-based study in Western France. EPI-GETBP Study Group. Grouped’Etude de la Thrombose de Bretagne Occidentale. Thromb. Haemost. 83, 657–660 (2000).
Keller, K. et al. Trends in thrombolytic treatment and outcomes of acute pulmonary embolism in Germany. Eur. Heart J. 41, 522–529 (2020).
Righini, M., Goehring, C., Bounameaux, H. & Perrier, A. Effects of age on the performance of common diagnostic tests for pulmonary embolism. Am. J. Med. 109, 357–361 (2000).
Anderson, F. A. Jr. & Wheeler, H. B. Venous thromboembolism. Risk factors and prophylaxis. Clin. Chest Med. 16, 235–251 (1995).
Migita, K. et al. Venous thromboembolism after total joint arthroplasty: results from a Japanese multicenter cohort study. Arthritis Res. Ther. 16, R154 (2014).
Kabrhel, C., Varraso, R., Goldhaber, S. Z., Rimm, E. B. & Camargo, C. A. Prospective study of BMI and the risk of pulmonary embolism in women. Obesity (Silver Spring) 17, 2040–2046 (2009).
Sorensen, H. T. et al. Heart disease may be a risk factor for pulmonary embolism without peripheral deep venous thrombosis. Circulation 124, 1435–1441 (2011).
Enga, K. F. et al. Atrial fibrillation and future risk of venous thromboembolism:theTromso study. J. Thromb. Haemost. 13, 10–16 (2015).
Agnelli, G. & Becattini, C. Venous thromboembolism and atherosclerosis: common denominators or different diseases?. J. Thromb. Haemost. 4, 1886–1890 (2006).
Tillie-Leblond, I. et al. Pulmonary embolism in patients with unexplained exacerbation of chronic obstructive pulmonary disease: prevalence and risk factors. Ann. Intern. Med. 144, 390–396 (2006).
Borvik, T. et al. COPD and risk of venous thromboembolism and mortality in a general population. Eur. Respir. J. 47, 473–481 (2016).
Wattanakit, K. & Cushman, M. Chronic kidney disease and venous thromboembolism: epidemiology and mechanisms. Curr. Opin. Pulm. Med. 15, 408–412 (2009).
Rinde, L. B. et al. Impact of incident myocardial infarction on the risk of venous thromboembolism: the Tromso Study. J. Thromb. Haemost. 14, 1183–1191 (2016).
Kelly, J., Rudd, A., Lewis, R. & Hunt, B. J. Venous thromboembolism after acute stroke. Stroke 32, 262–267 (2001).
Schmidt, M., Horvath-Puho, E., Thomsen, R. W., Smeeth, L. & Sorensen, H. T. Acute infections and venous thromboembolism. J. Intern. Med. 271, 608–618 (2012).
Khan, S. K. et al. Reduced short-term complications and mortality following enhanced recovery primary hip and knee arthroplasty: results from 6,000 consecutive procedures. Acta Orthop. 85, 26–31 (2014).
Anderson, D. R. et al. Aspirin or rivaroxaban for VTE prophylaxis after hip or knee arthroplasty. N. Engl. J. Med. 378, 699–707 (2018).
Pfeil, J., Hohle, P. & Rehbein, P. Bilateral endoprosthetic total hip or knee arthroplasty. Dtsch. Arztebl. Int. 108, 463–468 (2011).
Keller, K. et al. Venous thromboembolism in patients hospitalized for hip joint replacement surgery. Thromb. Res. 190, 1–7 (2020).
Keller, K., et al. Trends in thrombolytic treatment and outcomes of acute pulmonary embolism in Germany. Eur. Heart J. (2019).
Keller, K., Hobohm, L., Munzel, T. & Ostad, M. A. Impact of symptomatic atherosclerosis in patients with pulmonary embolism. Int. J. Cardiol. 278, 225–231 (2019).
Keller, K., Hobohm, L. & Engelhardt, M. Risk of venous thromboembolism after endoprosthetic surgeries: lower versus upper extremity endoprosthetic surgeries. Heart Vessels 34, 815–823 (2019).
Keller, K., Hobohm, L. & Engelhardt, M. Impact of atrial fibrillation on postoperative adverse outcomes of surgical patients with knee endoprosthetic surgery. J. Arthroplast. 33, 3567–3573 (2018).
Acknowledgements
We thank the Federal Statistical Office of Germany (source: RDC of the Federal Statistical Office and the Statistical Offices of the federal states, DRG Statistics 2005–2016, own calculations) for providing the data/results and the kind permission to publish these data/results.
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was supported by the German Federal Ministry of Education and Research (BMBF 01EO1503), institutional grant for the Center for Thrombosis and Hemostasis. The authors are responsible for the contents of this publication. The funder had no impact on conceptualization, design, data collection, analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
K.K., L.H., S.V.K. and P.D. developed the conception and design of the study. K.K., L.H., S.B., I.S., T.M., M.E., L.E., S.V.K. and P.D. contributed to analysis and interpretation of the data. Particularly, K.K., L.H., S.V.K. and I.S. insert their statistical expertise. K.K., L.H. and S.V.K. drafted the article. K.K., L.H., S.B., I.S., T.M., M.E., L.E., S.V.K. and P.D. revised the manuscript critically for important intellectual content and all authors gave their final approval of the article. K.K. (E-Mail: Karsten.Keller@unimedizin-mainz.de) takes the responsibility for the integrity of the work as a whole, from inception to finished article.
Corresponding author
Ethics declarations
Competing interests
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article. KK, IS, TM, ME, LE and PD report no conflict of interest. LH reports having received lecture honoraria from MSD. TM is PI of the DZHK (German Center for Cardiovascular Research), Partner Site Rhine-Main, Mainz, Germany. SB received lecture or consultant fees from Bayer HealthCare, BTG Pharmaceuticals, and LeoPharma and economical support for travel or congress costs from Daiichi Sankyo and Bayer HealthCare, outside of the submitted work. SK reports having received consultancy and lecture honoraria from Bayer, Boehringer Ingelheim, Daiichi-Sankyo, MSD and Pfizer-Bristol-Myers Squibb; and institutional grants from Actelion, Bayer, Boehringer Ingelheim, Daiichi-Sankyo and Pfizer-Bristol-Myers Squibb. The employment as well as the commercial support—mentioned above—had no impact on conceptualization, design, data collection, analysis, decision to publish, or preparation of the manuscript.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Keller, K., Hobohm, L., Barco, S. et al. Venous thromboembolism in patients hospitalized for knee joint replacement surgery. Sci Rep 10, 22440 (2020). https://doi.org/10.1038/s41598-020-79490-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-79490-w
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
