
Abstract
SARS-CoV-2 symptoms are non-specific and can range from asymptomatic presentation to severe pneumonia. Asymptomatic subjects carrying SARS-CoV-2 often remain undiagnosed and it is still debated whether they develop immunoglobulins (Ig) and how long they persist. The aim of this study was to investigate the development and persistence of antibodies against SARS-CoV-2 in asymptomatic subjects infected by the virus. This follow-up study was performed on the 31 asymptomatic subjects who presented a positive nasal swab or serology against SARS-CoV-2 (Ig against Spike-RBD) in the first part of the UNICORN study (March 2020) aimed at attesting previous or current contacts with the virus in the personnel of the University of Milan. Eight weeks after the first Ig measure, these subjects were invited to donate a second blood sample for testing serum antibodies (IgM, IgG and total antibodies) and to fill-in a structured questionnaire. About 80% of asymptomatic subjects did not present circulating immunoglobulins against SARS-CoV-2 after 8 weeks from a positive nasal swab against the virus. Moreover, in more than 40% of these subjects, no Ig against SARS-CoV-2 were detected at any time. Finally, about two third of subjects with immunoglobulins at baseline did not present IgG against SARS-CoV-2 after 8 weeks. The majority of subjects who developed an asymptomatic SARS-CoV-2 infection do not present antibodies against the RBD-spike protein after 8 weeks of follow-up. These data should be taken into account for the interpretation of the serological evidences on SARS-CoV-2 that are emerging nowadays.
Similar content being viewed by others

Introduction
Coronaviruses are known to cause diseases ranging from the common cold to fatal infections1. Among these viruses, the SARS-CoV-2 is responsible for the current infectious outbreak that has been declared a pandemic public health emergency by the World Health Organization.
SARS-CoV-2 symptoms are non-specific and can range from no symptoms to severe pneumonia2. This makes of primary importance to profile individual characteristics, such as the variability in immune response, linked to the relevance of clinical signs. Asymptomatic subjects carrying SARS-CoV-2 often remain undiagnosed and it is still debated whether they are able to transmit the disease3,4 and develop immunoglobulins (Ig)5.
Ig reveal evidence of a previous infection from about a week after the infection occurred6, but to date it is not clear if they are produced by all subjects encountering the virus and how long they persist in blood. Moreover, the actual capacity of anti-SARS-CoV-2 Ig to be neutralizing antibodies is still under debate7,8,9, especially for asymptomatic subjects. Many different methods have been proposed to detect Ig against SARS-CoV-2. To date, the most promising antigen for serodiagnosis of COVID-19 is probably the spike (S) protein, in particular the receptor-binding domain (RBD) mediating the interaction with angiotensin-converting enzyme 2 (ACE2)10,11.
At the end of March 2020, we examined plasma samples from 197 asymptomatic (at recruitment and in the 14 days before) subjects, enrolled during the lockdown period in Milan (Italy)12. This study was the first part of the UNICORN (“UNIversity against CORoNavirus”) project that was conducted among the personnel of the University of Milan, the largest university in Lombardy (Italy). A total of 31 subjects (16%) presented at least one positive test attesting a previous or current contact with SARS-CoV-2. In particular, 10% presented antibodies (IgM or IgG) against SARS-CoV-2 and the SARS-CoV-2 RNA was detected in the nasal swab of 21 subjects (11%)12.
The aim of the study was to investigate the development or persistence of antibodies against the spike-RBD among the 31 asymptomatic subjects, 8 weeks after the first sampling.
Methods
In this follow-up study, the 31 subjects who presented a positive nasal swab or serology against SARS-CoV-2 in the first part of the UNICORN project (T1)12 were eligible.
Eight weeks after the first sampling (T2), these individuals were invited to donate a second blood sample and to fill-in a structured questionnaire.
The study was approved by the ethics committee of the University of Milan (approval number 17/20, approval date March 6, 2020) and conducted in accordance with the Declaration of Helsinki. All participants signed an informed consent form.
Blood collection and Ig analyses
Blood was collected in ethylenediaminetetraacetic acid (EDTA) tubes (9.5 ml), and transported to the EPIGET Lab (University of Milan) within 2 h after phlebotomy. Blood-EDTA was processed to separate buffy coat and plasma, by centrifuging at 1200×g for 15 min at room temperature. Cell-free plasma was used to assess immunoglobulin-M (IgM) and immunoglobulin-G (IgG) against SARS-CoV-2 using validated enzyme linked immunosorbent assay (ELISA) methods.
The Wantai anti-SARS-CoV-2 IgM ELISA (Beijing Wantai Biological Pharmacy Enterprise, Beijing, China)13 were performed according to the manufacturer’s instructions. Reported sensitivity is 0.86 and specificity is 1. The assays detect antibodies binding SARS-CoV-2 spike protein receptor binding domain (RBD) in human serum or plasma. Briefly, 10 μl plasma samples and 100 μl of Specimen Diluent were added to wells coated with antibodies directed against the human immunoglobulin M proteins, and incubated for 30 min at 37 °C. Each well was aspirated and washed five times using an automatic microplate washer (MicroFill Dispenser, BioTek Instrument Winooski, VT, USA). Then, a recombinant HRP-conjugated SARS-CoV-2 antigen was added and incubated for 30 min at 37 °C. After a further washing, a chromogen solution was added. The reaction was stopped after 15 min at 37 °C, and the resultant absorbance was read on a microplate reader (Synergy HT, BioTek Instrument) at 450 nm with reference at 620 nm. The cut-off value for a positive result was calculated according to the manufacturer’s instruction, and equal to 0.105 for Anti-SARS-CoV-2 IgM ELISA.
To perform RBD Enzyme-Linked Immunosorbent Assay (ELISA) IgG, ELISA plates were coated with 1 µg/mL of purified recombinant Spike-RBD HEK-derived protein (Sino Biological, China). After overnight incubation at + 4 °C, coated plates were washed three times with 300 µl/well of ELISA washing solution containing Tris Buffer Saline (TBS)-0.05% Tween 20, then blocked for 1 h at 37 °C with a solution of TBS containing 5% of Non-Fat Dry Milk (NFDM) ( Euroclone, Pero, Italy)14.
Human serum samples were heat inactivated at 56 °C for 1 h in order to reduce the risk of the presence of live virus in the sample, then diluted 1:100 in TBS-0,05% Tween 20 5%. Plates were washed three times as previously than 100 µl of each serum dilution was added to the coated plates and incubated for 1 h at 37 °C. Next, after the washing step, 100 µl/well of Goat anti-Human IgG-Fc HRP-conjugated antibody diluted 1:100,000, (Bethyl Laboratories, Montgomery USA) were added. Plates were incubated at 37 °C for 30 min. Following incubation, the plates were washed and 100 µl/well of 3,3′,5,5′-Tetramethylbenzidine (TMB) substrate (Bethyl Laboratories, Montgomery, USA) was added and incubated in the dark at room temperature for 20 min. The reaction was stopped by adding 100 µl of ELISA stop solution (Bethyl Laboratories, Montgomery, USA) and read at 450 nm. Cut-off value was established as 3 times the average of optical density (OD) values from blank wells (background-no addition of analyte). Samples with the ODs under the cut off value at the first (1:100) dilution were assigned as negative, samples where the ODs at 1:100 dilution were above the cut-off value were assigned as positive. Borderline samples were defined where one replicate was under the cut-off and the other was above14.
Statistical analyses
We used standard descriptive statistics to summarize data. Categorical data were presented as frequencies and percentages. Continuous variables were expressed as the mean ± standard deviation (SD) or as the median and interquartile range [Q1–Q3], as appropriate. To investigate the characteristics of study participants who had Ig G against Sars-CoV-2 at T2, the Fisher exact test for categorical variables and t-test or Wilcoxon sum-rank test for continuous variables, were used. We reported the odds ratio and 95% confidence intervals (CI) to evaluate the association between SARS-Cov-2 RNA, IgM and IgG measured at T1 with IgG measured at T2. Statistical analyses and graph were performed with SAS software (version 9.4; SAS Institute Inc., Cary, North Carolina, USA, https://www.sas.com) and R software (version 3.6.1; Foundation for Statistical Computing, Vienna, Austria, https://www.r-project.org/).
Ethics committee approval
The study was approved by the ethics committee of the University of Milan (approval number 17/20, approval date March 6, 2020) and conducted in accordance with the Declaration of Helsinki.
Results
Among the 31 eligible subjects, 29 (94%) completed the follow-up study, while 2 subjects revoked their participation before T2. Characteristics of the 29 volunteers (17 females and 12 males, median age 44 years) are described in Table 1. Most subjects had high-level education: all participants had at least a higher school degree (high school: 20.7%; university: 20.7%, postgraduate: 58.6%). 79% had at least one cohabiting family member, and in 34.5% of cases the family member was < 10-year-old.
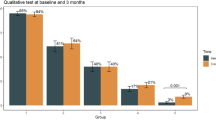
In the 6 months preceding T1, 67.7% of the enrolled volunteers reported at least one episode of upper airway infections, 3.5% of lower airway infections, and 37.9% of fever (Table 1 and Fig. 1). However, none required hospitalization. One subject developed fever and symptoms consistent with an upper respiratory infection two day after the first nasal swab sampling.

Left panel, a timeline showing symptoms occurrence from October 2019 to the second UNICORN examination (May-June 2020). Right panel, for each subject the presence/absence of Ig or viral RNA is reported.
Eleven (52.3%) out of 21 subjects with a positive nasal swab at T1 never developed antibodies against SARS-CoV-2. Antibody production was not associated to viral load (Supplementary Table 1).
Only 4 (21%) out of 19 participants (as 2 subjects were lost at T2) presented with immunoglobulins against SARS-CoV-2 at T2. Six (35%) out of 17 subjects with immunoglobulins at T1 presented IgG against SARS-CoV-2 at T2 (Fig. 1).
Subjects showing positive IgG at T2 did not differ from negative subjects for demographics and the number of upper and lower respiratory infections in the previous months (Table 1).
The presence of IgM at T1 or having 2 or more positive markers (among viral RNA, IgM or IgG) at T1 increase more than eightfold the probability of having positive IgG at T2 (respectively, OR 8.44, 95% CI (1.23 ; 58.16), p-value = 0.03; OR 8.50, 95% CI (1.25 ; 57.92), p-value = 0.03). On the contrary, the presence of positive IgG at T2 is not associated to the presence of viral RNA at T1 (OR 0.62, 95% CI (0.11 ; 3.56), p-value = 0.59). No other variables (listed in Table 1) are associated to the probability of having positive IgG at T2 (data not shown).
Discussion
This study points out that about 80% of subjects with a mild SARS-CoV-2 infection do not present circulating immunoglobulins against SARS-CoV-2 after 8 weeks from a positive nasal swab against the virus. Moreover, in more than 40% of these subjects, no Ig against SARS-CoV-2 were detected. Finally, about two third of subjects with immunoglobulins at baseline did not present IgG against SARS-CoV-2 after 8 weeks.
Patients with severe forms of COVID-19 were demonstrated to develop immunoglobulins against the S protein within 2–3 weeks after the symptoms onset15,16. Very recent data also suggest that circulating immunoglobulins against the S protein in symptomatic patients tend to persist at least for three months10. Our data appear to show a discrepancy from what was previously observed in patients with symptomatic forms of SARS-CoV-2. Only a minority of subjects who were positive for viral RNA at T1 then developed IgG (38%), and only a part of them then maintained a measurable level of IgG after 8 weeks (14,3%). This apparent difference could be explained by the fact that the populations under study are different as regards the severity of the symptoms. We speculate that asymptomatic/paucisymptomatic positive subjects might benefit of some protective factors capable of limiting the spread of the virus within the body, or alternatively a more effective innate immune T cell-based response, as recently raised by Grifoni et al., 202017. These factors could reduce the need for an adaptive response by the body, and consequently limit the production and persistence of antibodies.
Our data are in line with two very recent reports. In non-severe symptomatic COVID-19 patients, a decrease in IgG against RBD-spike protein was observed approximately 3 months after symptoms onset18. Moreover, a weaker immune response to SARS-CoV-2 infection was demonstrated in asymptomatic/paucisymptomatic individuals compared to symptomatic patients19.
To estimate the percentage of subjects who have been infected by SARS-CoV-2, an increasing number of studies have been conducted to assess the seroprevalence of antibodies against SARS-CoV-2 among the general population20,21,22,23. It has been proposed that these data may represent a starting point to predict how viral diffusion will evolve in the coming months24. At the light of our results, this assumption should be made with great caution. Considering the transient persistence of IgG in the asymptomatic/paucisymptomatic subjects, and that SARS-CoV-2 infection very often presents without symptoms, seroprevalence might not correspond to the real spread of the virus over time. Furthermore, to date there is no information available on the real protection from future infections in anti-SARS-CoV-2 IgG positive subjects.
Surprisingly, the only presence of SARS-CoV-2 RNA in the nasal swab at baseline was not associated with the probability of having anti- SARS-CoV-2 IgG after 8 weeks, with an odds ratio that was even protective, although not significant. On the contrary, the presence of IgM at T1 is associated with a strong increase in the probability of having IgG at T2. Although this association is significant, it is important to point out that the confidence intervals for the odds ratios are extremely wide and therefore this finding need to be interpreted cautiously. Moreover, since the analysis of the swab only detects the presence of viral RNA in the upper airways, this might not reflect a real active replication of the virus25,26, whereas Ig development implies an interaction between the virus and the immune system.
This study has some limitations. First of all, the population under study is small, although well characterized. The first part of the UNICORN project (the end of March, 2020) was conducted in Milan during a strict lockdown, and therefore subjects’ enrolment was limited. Second, the follow-up of positive subjects was relatively short. Finally, we did not perform any neutralizing test, although Ig against SARS-CoV-2 spike are the main, and likely the only neutralizing antibodies27.
In conclusion, this study points out that the majority of subjects who developed a mild SARS-CoV-2 infection do not present antibodies against the RBD-spike protein after 8 weeks of follow-up. These findings should be taken into account for the interpretation of seroprevalence data that are emerging nowadays.
References
Paules, C. I., Marston, H. D. & Fauci, A. S. Coronavirus infections—more than just the common cold. JAMA 323, 707–708 (2020).
Guan, W. J. et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 382, 1708–1720 (2020).
Rothe, C. et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N. Engl. J. Med. 382, 970–971 (2020).
Bai, Y. et al. Presumed asymptomatic carrier transmission of COVID-19. JAMA 323, 1406–1407 (2020).
Abbasi, J. The promise and peril of antibody testing for COVID-19. JAMA 323, 1881–1883 (2020).
Okba, N. M. A. et al. Severe acute respiratory syndrome coronavirus 2-specific antibody responses in coronavirus disease patients. Emerg. Infect. Dis. 26, 1478–1488 (2020).
Zhou, G. & Zhao, Q. Perspectives on therapeutic neutralizing antibodies against the Novel Coronavirus SARS-CoV-2. Int. J. Biol. Sci. 16, 1718–1723 (2020).
Jiang, S., Hillyer, C. & Du, L. Neutralizing antibodies against SARS-CoV-2 and other human coronaviruses. Trends Immunol. 41, 355–359 (2020).
Jawhara, S. Could intravenous immunoglobulin collected from recovered coronavirus patients protect against COVID-19 and strengthen the immune system of new patients?. Int. J. Mol. Sci. 21, 2272 (2020).
Wajnberg, A. et al. SARS-CoV-2 infection induces robust, neutralizing antibody responses that are stable for at least three months. medrxiv, 2020.2007.2014.20151126 (2020).
Gheblawi, M. et al. Angiotensin-converting enzyme 2: SARS-CoV-2 receptor and regulator of the renin-angiotensin system: celebrating the 20th anniversary of the discovery of ACE2. Circ. Res. 126, 1456–1474 (2020).
Milani, G. P. et al. SARS-CoV-2 infection among asymptomatic homebound subjects in Milan, Italy. Eur. J. Intern. Med. 78, 161–163 (2020).
Zhao, J. et al. Antibody responses to SARS-CoV-2 in patients of novel coronavirus disease 2019. Clin. Infect. Dis. https://doi.org/10.1093/cid/ciaa344 (2020).
Mazzini, L. et al. Comparative analyses of SARS-CoV-2 binding (IgG, IgM, IgA) and neutralizing antibodies from human serum samples. bioRxiv, 2020.2008.2010.243717 (2020).
Long, Q. X. et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat Med 26, 845-+ (2020).
To, K. K. W. et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. Lancet Infect. Dis. 20, 565–574 (2020).
Grifoni, A. et al. Targets of T cell responses to SARS-CoV-2 coronavirus in humans with COVID-19 disease and unexposed individuals. Cell 181, 1489–1501 (2020).
Ibarrondo, F. J. et al. Rapid decay of anti-SARS-CoV-2 antibodies in persons with mild Covid-19. N. Engl. J. Med. 383, 1085–1087 (2020).
Long, Q. X. et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 26, 1200–1204 (2020).
Stringhini, S. et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Geneva, Switzerland (SEROCoV-POP): a population-based study. Lancet 396, 313–319 (2020).
Sood, N. et al. Seroprevalence of SARS-CoV-2-Specific Antibodies Among Adults in Los Angeles County, California, on April 10–11, 2020. JAMA 323, 2425–2427 (2020).
Pollan, M. et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. Lancet 396, 535–544 (2020).
Havers, F. P. et al. Seroprevalence of Antibodies to SARS-CoV-2 in 10 Sites in the United States, March 23-May 12, 2020. JAMA Intern. Med. (2020).
Holmdahl, I. & Buckee, C. Wrong but useful: what Covid-19 epidemiologic models can and cannot tell us. N. Engl. J. Med. 383, 303–305 (2020).
Perlman, S. & Netland, J. Coronaviruses post-SARS: update on replication and pathogenesis. Nat. Rev. Microbiol. 7, 439–450 (2009).
Yang, S. & Rothman, R. E. PCR-based diagnostics for infectious diseases: uses, limitations, and future applications in acute-care settings. Lancet Infect. Dis. 4, 337–348 (2004).
Amanat, F. & Krammer, F. SARS-CoV-2 vaccines: status report. Immunity 52, 583–589 (2020).
Acknowledgments
We thank all the AVIS-Milano volunteers for their support with blood collection, Patrizia Angiolillo for electronic questionnaire preparation, Nicla Diomede for informatics security, Elena del Giorgio for support during subject’s enrolment, Angelo Casertano and all the University of Milan staff for their precious help.
Funding
GPM and VB received a grant from “Ricerche Emergenza coronavirus”, University of Milan, 2020 to support the study (https://lastatalenews.unimi.it/statale-individuati-sette-progetti-ricerca-ad-alta-priorita-contro-covid-19). Funds have been used for purchasing reagents.
Author information
Authors and Affiliations
Author notes
A list of authors and their affiliations appears at the end of the paper.
Consortia
Contributions
G.M.: Study design, literature search, data collection, data analysis, data interpretation, writing. L.D., L.C., C.M., S.D.: Laboratory analysis. C.F.: Statistical analysis and database management. MB: Study design, data interpretation, writing. E.M.: Data collection, data analysis, data interpretation. V.B.: Study design, figures, data collection, data analysis, data interpretation, writing. UNICORN CONSORTIUM: Subject’s enrolment, Laboratory analysis, data interpretation. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Milani, G.P., Dioni, L., Favero, C. et al. Serological follow-up of SARS-CoV-2 asymptomatic subjects. Sci Rep 10, 20048 (2020). https://doi.org/10.1038/s41598-020-77125-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-77125-8
This article is cited by
-
SARS-CoV-2 epidemiological trend before vaccination era: a seroprevalence study in Apulia, Southern Italy, in 2020
Journal of Public Health (2024)
-
Anti-SARS-CoV-2 antibody levels predict outcome in COVID-19 patients with type 2 diabetes: a prospective cohort study
Scientific Reports (2023)
-
Test concordance and diagnostic accuracy of three serological assays for detection of anti-SARS-CoV-2 antibody: result from a population-based sero-epidemiological study in Delhi
BMC Infectious Diseases (2022)
-
Relationship between gene expression patterns from nasopharyngeal swabs and serum biomarkers in patients hospitalized with COVID-19, following treatment with the neutralizing monoclonal antibody bamlanivimab
Journal of Translational Medicine (2022)
-
Quantitative serology for SARS-CoV-2 using self-collected saliva and finger-stick blood
Scientific Reports (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
