
Abstract
Unicompartmental knee arthroplasty (UKA) can be either a fixed bearing (FB) or a mobile bearing (MB) construct with controversy as to which design is superior. This question is addressed with a systematic review and meta-analysis. A literature search was performed using PubMed, Embase and the Cochrane Library. Studies were reviewed according to the inclusion and exclusion criteria developed in advance. We compared the differences in clinical and radiological outcomes between the FB and MB UKAs. Analyses were performed with the Review Manager and STATA software. A total of 17 studies involving 2612 knees were included. No significant differences were presented between the FB and MB prostheses in clinical and radiological outcomes. However, it was evident that there were differences in the modes and timing of the failures, bearing dislocation led to earlier failures in the MB prosthesis, while the FB prosthesis failed later due to polyethylene wear. There was no evidence of publication bias using the incidence of revisions. There is no significant difference between the FB and MB UKAs; however, there are differences in the modes and timing of failures.
Similar content being viewed by others

Introduction
UKA was originally introduced as a FB construct to address unicompartmental osteoarthritis of the knee1. More recently MB constructs were introduced to minimize contact stress and polyethylene wear2,3. Each prosthesis design has its own strengths and weaknesses and there remains discussion on which prosthetic design has superior long-term results. The MB prosthesis, by offering more congruent bearing surfaces with a large contact area generates less contact stresses, theoretically decreasing the risk of aseptic loosening, polyethylene wear, and implant revision in the long term4. However, the MB prosthesis is technically more difficult to implant. Without precise alignment and ligament balancing, it can lead to bearing dislocation or impingement causing increased wear5. Conversely, the FB prosthesis often has a flat tibial articular surface, which is technically easier to implant and there is no risk of bearing dislocation1,6. However, the advantages are also the disadvantages, the FB prosthesis is less conforming as flexion occurs and can lead to point loading due to the flat tibial articular surface7. Direct comparison between FB and MB prostheses have been made in several studies, however, findings were inconsistent and unable to demonstrate an advantage of one prosthesis design over the other5,8,9. A previous meta-analysis attempted to resolve this debate but was limited by a lack of clinical studies to support a robust statistical analysis2. However, since then further studies have been published, which allows a more in-depth analysis. Some recent studies have demonstrated higher knee scores and lower revision rates of the MB prosthesis compared to the FB prosthesis10,11,12, while other studies have demonstrated the opposite relationship13,14,15. In addition, previous retrospective cohort studies comparing mid-term and long-term survivorship between the two UKA prostheses did not demonstrate obvious differences1,10,16.
In this meta-analysis we evaluate the performance of FB and MB prostheses comparing clinical and radiological outcomes as well as complications and reported survivorship.
Results
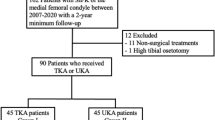
A total of 900 studies were identified in this study. After review of the titles, abstracts, full articles, and excluding unrelated articles 17 studies involving 2612 knees were eligible and selected for the final meta-analysis1,5,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22 (Fig. 1). Three of the 17 eligible studies were randomized controlled trials (RCTs). Weight or body mass index (BMI) was reported in 11 studies. The mean follow-up period ranged from 7-months to 17.2-years; the follow-up period was not stated in two studies. Additional details about study characteristics and participant demographics are shown in Table 1.

Flowchart for the identification of eligible studies. This flowchart covered the detailed selecting process, including three databases and relevant studies, the excluded reasons and number of studies, and the final studies included in the meta-analysis.
Within the 17 eligible studies the FB knee prostheses were from seven manufacturers: Miller-Galante (Zimmer), Robert Brigham (Johnson and Johnson), St Georg Sled (Waldemar Link), Preservation All Poly (DePuy), Optetrak (Exactech), Allegreto (Centerpulse), and Accuris (Smith and Nephew); the MB knee prostheses were from two manufacturers: Oxford (Biomet) and AMC (Alphanorm).
Clinical outcomes
Nine studies assessed the Knee Society Score (KSS)1,9,10,11,12,15,19,20,22; six studies assessed the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score11,16,17,18,20,22; three studies assessed the Oxford Knee Score (OKS)5,15,17; one study assessed the Italian Orthopedic UKR’s Users Group (GIUM) score9; one study assessed the Bristol knee score5; and one study assessed the International Knee Society score8. No significant statistical differences were reported between the FB and MB groups on all knee scores measured in these studies. Although statistical heterogeneity was high in the assessment of the Knee Society Score, data from the meta-analysis did not demonstrate significant statistical differences between the FB and MB groups (p = 0.22; I2 = 87%) (Fig. 2). Two studies1,20 found similar results between FB and MB groups in respect to pain (p > 0.05), however, Gleeson et al.5 reported that the total pain score, as assessed using the Bristol Knee Score, was significantly greater in the FB group at 2 years (p = 0.013). Postoperative ROM was assessed in five studies9,12,15,19,20, no significant difference was shown between the FB and MB groups (p = 0.19; WMD = − 1.53; 95% CI − 3.80 to 0.74).

Forest plot for the Knee society score following the FB and MB UKAs. Nine studies were analyzed, while only six studies were showed in the forest plot for absence of standard deviation (SD) in the other three studies. Since I2 = 87%, a random effect model was used (RevMan 5, version 5.3, URL: https://training.cochrane.org).
Radiological outcomes
According to the Kennedy and White classification, which considers correct alignment when the mechanical axis is in Zone 2 or C (central) and malalignment in Zone 1 or Zone 323. Malalignment occurred in 16 (8.0%) knees in the FB group and 22 (11%) knees in the MB group (OR = 0.70; 95% CI 0.36–1.38; p = 0.31). Two studies12,19 reported postoperative FTA and 3 studies10,19,20 reported postoperative HKA, no significant differences were found (p = 0.1; WMD = 0.60; 95% CI − 0.11 to 1.31 and p = 0.69; WMD = − 0.51; 95% CI − 3.03 to 2.01) between the FB and MB groups.
The incidence of radiolucent lines at the bone-tibial implant interface was examined in four studies. Li et al.20 reported a greater incidence of radiolucent lines at 2-years postoperatively in the FB group (37% vs. 8%; p = 0.02), while others demonstrated an increased incidence of radiolucent lines in the MB group (10.3% vs. 23.5%, p = 0.229; 69% vs. 24%, p = 0.001)10,18. Meanwhile, Andrea et al.22 revealed that no differences were found in RLLs between FM and MB group. Based on the cumulative data, no significant difference was found in the frequency of RLLs between the FB and MB groups (42.0% vs. 19.0%, OR = 0.56; 95% CI 0.10–3.05; p = 0.51).
Revisions, and survivorship
A total of 58 knees from the FB group experienced failure and underwent subsequent revisions, the time of failure ranged from 4-days to 15-years; meanwhile, a total of 43 knees from the MB group underwent subsequent revisions and the time of failure ranged from 6-weeks to 17.7-years. Meta-analysis revealed no significant difference in the incidence of revisions between the two groups (OR = 0.96; 95% CI 0.63–1.46; p = 0.85) (Fig. 3).

Forest plot for the incidence of revisions following the FB and MB UKAs. Nine studies were analyzed and showed in the forest plot. Since I2 = 24% and p = 0.23, a fixed effect model was used (RevMan 5, version 5.3, URL: https://training.cochrane.org).
In the FB group, complications consisted of progression of arthritis, polyethylene wear, aseptic loosening, and persistent pain. In the MB group, complications consisted of progression of arthritis, aseptic loosening, bearing dislocation, and persistent pain. No significant differences were found in the incidence for progression of arthritis (p = 0.33), aseptic loosening (p = 0.45), persistent pain (p = 0.84), and overall reoperation (p = 0.32) between the two groups. However, the differences in frequency of polyethylene wear (p = 0.02) and bearing dislocation (p = 0.03) were statistically significant between the two groups. In addition, the failure time for bearing dislocations was 0.6-years in the MB group and it was 8.3-years for polyethylene wear in the FB group after surgery. Additional details about complications are shown in Table 2.
Four studies demonstrated that survivorship at 5-years, 10-year, and 20-years were 95.6%, 90.9% and 83% in the FB group and 97%, 92% and 80% in the MB group respectively, with a mean follow-up ranging from 3.6 to 17.2-years (Table 3)1,10,16,18. Cumulatively these studies suggest similar implant survivorship between the two groups (OR = 1.38; 95% CI 0.83–2.30; p = 0.21). However, using the Cox regression analysis model, Bhattacharya et al.13 demonstrated better survivorship in the MB group (p < 0.05).
Publication bias
The publication bias was assessed using a funnel plot, which demonstrates the relationship between the size of the study sample and the accuracy of the estimated treatment effect. The assessment of publication bias using the incidence of revisions indicated no substantial evidence of bias (p = 0.893) (Fig. 4).

Funnel plot demonstrating minimal publication bias from revision outcome. Nine studies were analyzed, the abscissa axis showed the odds ratio, and the vertical axis showed the standard error (STATA, version 12.0, URL: https://www.stata.com).
Discussion
UKA comes in two basic prosthesis designs, FB and MB, with disagreement as to which design has superior results5,8,9. We have conducted a meta-analysis of all available studies comparing FB to MB UKA prostheses.
Only comparative studies were included in the current meta-analysis. While many studies showed favorable results with fixed or mobile bearing design, they only reported results of a single implant and were therefore excluded from this study24,25. The most important finding from our study is that FB and MB prostheses did not differ in terms of: (1) clinical outcomes; (2) radiographic outcomes; (3) revision rates, or (4) survivorship. However, the differences in modes and timing of failures were evident between the two prostheses, bearing dislocation led to earlier failures in the MB prosthesis, while later failures were related to polyethylene wear in the FB prosthesis group.
Differences in clinical outcomes between FB and MB prostheses has been reviewed with each study using different functional measurement indexes. Some studies15,19 found better results in knee functional scores with the MB group, while Inoue et al.12 and Ozcan et al.11 found higher postoperative KSS in the FB group. Interestingly, Peersman et al.24 demonstrated that there was a tendency for the KSS to deteriorate more rapidly in MB than FB prostheses between 10 and 15 years. However, none of these studies demonstrated significantly better results for one prosthesis over the other. No significant statistical differences were found between the FB and MB groups on all knee scores measured in this study (Fig. 2).
RLL have previously been reported at almost quintuple the rate in FB UKA’s compared to MB prostheses20, while other studies10,18 found the opposite results. In this meta-analysis, the incidence of RLL was higher in the MB group compared to the FB group (42.0% MB vs. 19.0% FB) based on limited sample sizes, no significant difference was found (p = 0.75). In addition, recent studies suggest that the presence of RLLs is irrelevant to knee scores and revision rates in mid- and long-term follow-up10,16,26,27. Therefore, longer-term follow-up RCTs are needed to find the true relationship between the incidence of radiolucent lines and survivorship between different prostheses.
A previous meta-analysis28 suggested that the major complications which required reoperation following UKAs consisted of aseptic loosening, progression of arthritis and wear of the polyethylene insert. Some in vitro studies6,29 based on knee simulators reported lower wear rates of FB prostheses compared to MB prostheses, while Manson et al.30 found that wear was a complication inherent to the design of FB prosthesis caused by the fatigue and sheer stress-related mechanism, secondary to higher surface deformation and delamination in comparison to MB prosthesis. In comparison, MB prostheses reduce overall polyethylene wear by increasing the contact area and congruency while minimizing constraints and maintaining normal knee motion31. In MB prostheses, wear of the polyethylene is mainly due to the abrasive and adhesive mechanism28. Bearing dislocation is a unique complication in MB prostheses. Any under correction of the deformity may play a role in the medial compartment stresses contributing to bearing dislocation. Considering this, surgeons may be inclined to choose a tight knee and risk slight overcorrection into valgus32. However, overcorrection to valgus can result in greater contact stress and significant load on the lateral compartment, thus accelerating the progression of arthritis. In contrast, FB prostheses could offload the lateral compartment and thereby slow the progression of arthritis28. In the current study, a higher incidence of polyethylene wear was clearly demonstrated in the FB group, and bearing dislocation was only present in MB group (Table 2).
Survivorship differed between prosthesis design in most studies. Whittaker et al.16 reported that the 5-year survival, with revision to TKA as the end point, was 88% for the MB implants and 96% for the FB implants. Reporting on 38 MB and 68 FB knees with a mean follow-up of 14.2-years and 11.5-years, Neufeld et al.18 demonstrated that the 10-year survivorship of the MB implants was 82.9% and the FB implants was 90.9%. In addition, a comparative study10 with a minimum 15-year follow-up reported that 20-year survivorship was 83% in the FB group and 80% in the MB group. Similar to our study, differences of survivorship between the two prostheses in these studies were not significant (Table 3). To assess the true differences in the lifespan of UKA implants, future higher quality RCTs are needed.
Several limitations should be presented in our study. First, we included 14 non-randomized controlled trials (nRCTs) of low level of evidence, which increases the risk of bias and other cofounding variables. Second, publication bias might affect the outcomes, as we did not search for unpublished studies. However, the funnel plot demonstrated minimal evidence of publication bias (Fig. 4). Finally, due to the high proportion of missing data and the observational nature of the included studies, the results should be interpreted with caution. In our study, no significant differences in knee scores were found between the two prostheses, which may be due to the limited studies and incomplete data. Therefore, future larger scale and long-term follow-up RCTs with complete data directly comparing the knee functional scores between FB and MB UKAs are needed. Theoretically, different complications mean different revision surgeries, such as replacing polyethene insert, UKA, Bi-KA or TKA, while most of present studies don’t mention it. Lacking the specific surgery of revision is another disadvantage of our study, we will analyze the tendency of the type of revision surgeries in these two designs of UKA in future study.
In conclusion, both Fixed Bearing and Mobile Bearing prostheses provide excellent knee scores, radiological outcomes, and survivorship in Unicompartmental Knee Arthroplasties. The superiority of one prosthesis over the other could not be demonstrated and each have their merits and indications. Patient selection and proper technique are required to ensure the Mobile Bearing prosthesis can survive beyond the short-term dislocation complication to enable excellent implant longevity.
Materials and methods
This meta-analysis was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement33. Relevant studies published prior to April 21, 2020 were identified by searching PubMed, Embase and the Cochrane Library with no language restrictions. The following search terms, including their variations, were used: “Arthroplasty, Replacement, Knee”, “Unicompartmental”, “Unicondylar”, “Fixed”, “Mobile”, “Bearing”, and Boolean operators (AND, OR) for various combinations. After the initial electronic search, relevant articles and their bibliographies were searched manually.
To minimize any possible selection bias, all studies that satisfied the search strategy were reviewed and included if they met the following criteria: (1) studies which compare FB and MB knee prostheses directly; (2) patients with isolated medial compartment arthritis of the knee; and (3) studies which report clinical or radiographic outcomes, revisions, or survivorship. The exclusion criteria included: (1) review articles, letter or comment; (2) studies which only describe either FB or MB knee prostheses; (3) patients with lateral compartment arthritis or patellofemoral arthritis of the knee; (4) also excluded if the results of comparison were not reported or the data could not be extracted from the published results. Two reviewers (WCZ, JPW) independently assessed each of the studies for eligibility for inclusion. All disagreements were resolved through discussion to reach a final consensus.
All information regarding relevant results were recorded. Data of participants included: number of knees/patients, demographic data (age, sex, weight, height, etc.), duration of the follow-up, and type of prosthesis. The outcome measures included knee scores, range of motion (ROM), femoral-tibial angle (FTA), hip-knee-ankle angle (HKA), incidence of radiolucent lines (RLLs), incidence and timing of revisions, and survivorship. The levels of evidence were assessed using a published rating system34.
Heterogeneity was determined by estimating the proportion of between-study inconsistencies by examining actual differences between studies identified in the data extraction tables. Heterogeneity is expressed as p and I2; if p > 0.10 and I2 < 50%, a fixed effects model was adopted; otherwise, a random effects model was chosen. Continuous data was assessed using weighted mean difference (WMD) and associated 95% CI (confidence intervals), adopting the Mantel–Haenszel method35; study-specific OR (Odds Ratio) and associated 95% CI were used to determine the value of dichotomous data.
Forest plots were used to graphically present the results of individual studies and the respective pooled estimate of effect size. Statistical significance was regarded as a p < 0.05. Publication bias was assessed using a funnel plot of the outcome measure recorded in the largest number of clinical trials36. We assessed funnel plot asymmetry using Begg and Egger tests and defined significant publication bias as a p < 0.1. Review Manager (RevMan, version 5.3) for Windows and the Cochrane collaboration were used to perform all statistical analyses. Publication bias was assessed using STATA (version 12.0).
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Emerson, R. H. Jr., Hansborough, T., Reitman, R. D., Rosenfeldt, W. & Higgins, L. L. Comparison of a mobile with a fixed-bearing unicompartmental knee implant. Clin Orthop. Relat. Res. https://doi.org/10.1097/00003086-200211000-00011 (2002).
Smith, T. O., Hing, C. B., Davies, L. & Donell, S. T. Fixed versus mobile bearing unicompartmental knee replacement: a meta-analysis. Orthop. Traumatol. Surg. Res. 95, 599–605. https://doi.org/10.1016/j.otsr.2009.10.006 (2009).
Bonutti, P. M. & Dethmers, D. A. Contemporary unicompartmental knee arthroplasty: fixed vs mobile bearing. J. Arthroplasty 23, 24–27. https://doi.org/10.1016/j.arth.2008.06.025 (2008).
O’Connor, J. J. & Goodfellow, J. W. Theory and practice of meniscal knee replacement: designing against wear. Proc. Inst. Mech. Eng. H 210, 217–222. https://doi.org/10.1243/pime_proc_1996_210_415_02 (1996).
Gleeson, R. E., Evans, R., Ackroyd, C. E., Webb, J. & Newman, J. H. Fixed or mobile bearing unicompartmental knee replacement? A comparative cohort study. Knee 11, 379–384. https://doi.org/10.1016/j.knee.2004.06.006 (2004).
Brockett, C. L., Jennings, L. M. & Fisher, J. The wear of fixed and mobile bearing unicompartmental knee replacements. Proc. Inst. Mech. Eng. H 225, 511–519. https://doi.org/10.1177/2041303310393824 (2011).
Argenson, J. N. & Parratte, S. The unicompartmental knee: design and technical considerations in minimizing wear. Clin. Orthop. Relat. Res. 452, 137–142. https://doi.org/10.1097/01.blo.0000229358.19867.60 (2006).
Catani, F. et al. Muscle activity around the knee and gait performance in unicompartmental knee arthroplasty patients: a comparative study on fixed- and mobile-bearing designs. Knee Surg. Sports Traumatol. Arthrosc. 20, 1042–1048. https://doi.org/10.1007/s00167-011-1620-z (2012).
Confalonieri, N., Manzotti, A. & Pullen, C. Comparison of a mobile with a fixed tibial bearing unicompartimental knee prosthesis: a prospective randomized trial using a dedicated outcome score. Knee 11, 357–362. https://doi.org/10.1016/j.knee.2004.01.003 (2004).
Parratte, S., Pauly, V., Aubaniac, J. M. & Argenson, J. N. No long-term difference between fixed and mobile medial unicompartmental arthroplasty. Clin. Orthop. Relat. Res. 470, 61–68. https://doi.org/10.1007/s11999-011-1961-4 (2012).
Ozcan, C. et al. Fixed-bearing unicompartmental knee arthroplasty tolerates higher variance in tibial implant rotation than mobile-bearing designs. Arch. Orthop. Trauma Surg. 138, 1463–1469. https://doi.org/10.1007/s00402-018-3005-y (2018).
Inoue, A. et al. Comparison of alignment correction angles between fixed-bearing and mobile-bearing UKA. J. Arthroplasty 31, 142–145. https://doi.org/10.1016/j.arth.2015.07.024 (2016).
Bhattacharya, R., Scott, C. E., Morris, H. E., Wade, F. & Nutton, R. W. Survivorship and patient satisfaction of a fixed bearing unicompartmental knee arthroplasty incorporating an all-polyethylene tibial component. Knee 19, 348–351. https://doi.org/10.1016/j.knee.2011.04.009 (2012).
Bini, S., Khatod, M., Cafri, G., Chen, Y. & Paxton, E. W. Surgeon, implant, and patient variables may explain variability in early revision rates reported for unicompartmental arthroplasty. J. Bone Jt. Surg. Am. 95, 2195–2202. https://doi.org/10.2106/jbjs.L.01006 (2013).
Verdini, F. et al. Assessment of patient functional performance in different knee arthroplasty designs during unconstrained squat. Muscles Ligaments Tendons J. 7, 514–523. https://doi.org/10.11138/mltj/2017.7.3.514 (2017).
Whittaker, J. P. et al. Does bearing design influence midterm survivorship of unicompartmental arthroplasty?. Clin. Orthop. Relat. Res. 468, 73–81. https://doi.org/10.1007/s11999-009-0975-7 (2010).
Biau, D. J., Greidanus, N. V., Garbuz, D. S. & Masri, B. A. No difference in quality-of-life outcomes after mobile and fixed-bearing medial unicompartmental knee replacement. J. Arthroplasty 28, 220-226.e221. https://doi.org/10.1016/j.arth.2012.05.017 (2013).
Neufeld, M. E., Albers, A., Greidanus, N. V., Garbuz, D. S. & Masri, B. A. A comparison of mobile and fixed-bearing unicompartmental knee arthroplasty at a minimum 10-year follow-up. J. Arthroplasty 33, 1713–1718. https://doi.org/10.1016/j.arth.2018.01.001 (2018).
Lu, M., Hu, G., Li, Z. & Cao, X. LINK fixed-bearing versus Oxford mobile-bearing unicompartmental knee arthroplasty for medial unicompartment knee osteoarthritis. Chin. J. Tissue Eng. Res. 35, 2095–4344. https://doi.org/10.3969/j.issn (2017).
Li, M. G. et al. Mobile vs fixed bearing unicondylar knee arthroplasty: a randomized study on short term clinical outcomes and knee kinematics. Knee 13, 365–370. https://doi.org/10.1016/j.knee.2006.05.003 (2006).
Emerson, R. H. Jr., Head, W. C. & Peters, P. C. Jr. Soft-tissue balance and alignment in medial unicompartmental knee arthroplasty. J. Bone Jt. Surg. Br 74, 807–810 (1992).
Tecame, A., Savica, R., Rosa, M. A. & Adravanti, P. Anterior cruciate ligament reconstruction in association with medial unicompartmental knee replacement: a retrospective study comparing clinical and radiological outcomes of two different implant design. Int. Orthop. 43, 2731–2737. https://doi.org/10.1007/s00264-019-04341-x (2019).
Kennedy, W. R. & White, R. P. Unicompartmental arthroplasty of the knee Postoperative alignment and its influence on overall results. Clin. Orthop. Relat. Res. 221, 278–285 (1987).
Peersman, G., Stuyts, B., Vandenlangenbergh, T., Cartier, P. & Fennema, P. Fixed- versus mobile-bearing UKA: a systematic review and meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 23, 3296–3305. https://doi.org/10.1007/s00167-014-3131-1 (2015).
Panni, A. S., Vasso, M., Cerciello, S. & Felici, A. Unicompartmental knee replacement provides early clinical and functional improvement stabilizing over time. Knee Surg. Sports Traumatol. Arthrosc. 20, 579–585. https://doi.org/10.1007/s00167-011-1613-y (2012).
Mercier, N., Wimsey, S. & Saragaglia, D. Long-term clinical results of the Oxford medial unicompartmental knee arthroplasty. Int. Orthop. 34, 1137–1143. https://doi.org/10.1007/s00264-009-0869-z (2010).
Gulati, A. et al. The incidence of physiological radiolucency following Oxford unicompartmental knee replacement and its relationship to outcome. J. Bone Jt. Surg. Br. 91, 896–902. https://doi.org/10.1302/0301-620x.91b7.21914 (2009).
Ko, Y. B., Gujarathi, M. R. & Oh, K. J. Outcome of unicompartmental knee arthroplasty: a systematic review of comparative studies between fixed and mobile bearings focusing on complications. Knee Surg. Relat. Res. 27, 141–148. https://doi.org/10.5792/ksrr.2015.27.3.141 (2015).
Kretzer, J. P. et al. Wear analysis of unicondylar mobile bearing and fixed bearing knee systems: a knee simulator study. Acta Biomater. 7, 710–715. https://doi.org/10.1016/j.actbio.2010.09.031 (2011).
Manson, T. T., Kelly, N. H., Lipman, J. D., Wright, T. M. & Westrich, G. H. Unicondylar knee retrieval analysis. J. Arthroplasty 25, 108–111. https://doi.org/10.1016/j.arth.2010.05.004 (2010).
Kendrick, B. J. et al. Polyethylene wear in Oxford unicompartmental knee replacement: a retrieval study of 47 bearings. J. Bone Jt. Surg. Br. 92, 367–373. https://doi.org/10.1302/0301-620x.92b3.22491 (2010).
Kozinn, S. C. & Scott, R. Unicondylar knee arthroplasty. J. Bone Jt. Surg. Am. 71, 145–150 (1989).
Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6, e1000097. https://doi.org/10.1371/journal.pmed.1000097 (2009).
Wright, J. G., Swiontkowski, M. F. & Heckman, J. D. Introducing levels of evidence to the journal. J. Bone Jt. Surg. Am. 85, 1–3 (2003).
Mantel, N. & Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 22, 719–748 (1959).
Egger, M., Davey Smith, G., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634. https://doi.org/10.1136/bmj.315.7109.629 (1997).
Acknowledgements
None. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
W.C.Z.: conceiving and designing the work, material preparation, data collection and analysis, writing first draft of the manuscript. J.P.W.: material preparation, data collection and analysis, writing first draft of the manuscript. H.L.: revising the manuscript. W.C.W.: writing first draft of the manuscript. D.M.G.: revising the manuscript. T.L.H.: article drafting, critical revision and final approval of the version. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhang, W., Wang, J., Li, H. et al. Fixed- versus mobile-bearing unicompartmental knee arthroplasty: a meta-analysis. Sci Rep 10, 19075 (2020). https://doi.org/10.1038/s41598-020-76124-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-76124-z
This article is cited by
-
Comparison of revision rates and epidemiological data of a single total knee arthroplasty system of different designs (cruciate retaining, posterior stabilized, mobile bearing, and fixed bearing): a meta-analysis and systematic review of clinical trials and national arthroplasty registries
Archives of Orthopaedic and Trauma Surgery (2024)
-
Impact of age on unicompartmental knee arthroplasty outcomes: a systematic review and meta-analysis
Knee Surgery, Sports Traumatology, Arthroscopy (2023)
-
No difference in mobile and fixed bearing partial knee arthroplasty in octogenarians: a clinical trial
European Journal of Orthopaedic Surgery & Traumatology (2023)
-
Unicompartmental knee arthroplasty in patients under the age of 60 years provides excellent clinical outcomes and 10-year implant survival: a systematic review
Knee Surgery, Sports Traumatology, Arthroscopy (2023)
-
Similar clinical and radiographic outcomes after two different hypoallergenic medial unicompartmental knee in patients with metal allergy
European Journal of Orthopaedic Surgery & Traumatology (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
