
Abstract
Constipation and REM sleep behaviour disorder (RBD) are the earliest non-motor manifestations of Parkinson’s disease (PD). Among non-motor symptoms of PD, it is unclear whether constipation and RBD at early stages of PD are related to cognitive outcomes at later stages. Herein, this study aims to investigate whether the presence of constipation and RBD have an impact on future cognitive outcomes in PD. Access to Parkinson’s Progression Markers Initiative (PPMI) database of 360 PD patients with longitudinal observation was requested. Constipation, probable RBD (pRBD) and neuropsychological task scores of PD patients were assessed at baseline and after 5 years. Linear mixed-effects modelling, controlling for gender, age, years of education and LEDD was used to evaluate the association between baseline constipation, pRBD and cognitive performance on follow-up. Gender differences in neuropsychological test performances were found, with men having worse global cognition, speed-attention processing, verbal learning and memory than women at early stages of the disease. We found constipation and pRBD are strongly associated with future decline in some cognitive measures among PD patients, more prominently in men. Our data suggest that early assessment of pRBD and constipation may allow better understanding of the progression of cognitive changes in later phases of PD.
Similar content being viewed by others


Introduction
Parkinson’s disease (PD) is recognised as one of the most common neurodegenerative disorders, with advancing age being its greatest risk factor1. Worldwide, PD afflicts 10 million people, and this figure is expected to double by 2030 due to our ageing population. Currently, it afflicts 1–2% of the population over the age of 602. Notably, epidemiological studies show that the risk of PD is 1.5 to 2 times greater in men than in women1,3,4.
Although PD has been classified as a movement disorder, a myriad of significant non-motor features can develop during the preclinical period, which become more prevalent with advancing disease5,6. These non-motor symptoms can antedate the onset of the prototypical motor symptoms by over a decade7,8. The causes of non-motor symptoms are multifactorial, involving neuronal loss in the dopaminergic, noradrenergic, cholinergic, and serotonergic systems. It is postulated that the manifestation of non-motor symptoms in PD is associated to the presence of Lewy bodies in specific non-nigral brainstem nuclei, which are responsible in fundamental homeostatic regulations, including gastrointestinal homeostasis, circadian rhythms and mood control9.
One of the most common and debilitating non-motor symptoms of PD is gastrointestinal dysfunction, which has a prevalence of 70–80%10. Gastrointestinal symptoms are identified as regurgitation, bloating, constipation, nausea, delayed gastric emptying, malnutrition and Helicobacter pylori infection11. Of all the gastrointestinal symptoms, constipation is recognised as the most prominent autonomic disturbance in preclinical PD as observed in 20% to 80% of PD patients12.
Recent evidence shows gastrointestinal dysfunction is present during the preclinical stages of PD, suggesting the PD pathological process could initiate in the gut13,14. Strong evidence supporting the presence of constipation during preclinical PD comes from the Honolulu Heart Program, that followed 6790 men over a 24-year period, which indicated that men with less than 1 bowel movement per day have a 4.1-fold risk of PD compared with men with 2 movements per day15. A recent preclinical study has highlighted constipation as an early feature of α-synucleinopathy which may precede the onset of motor symptoms in PD16. Although constipation has been investigated as a prodromal marker of PD17, the exact association between alterations in the gastrointestinal system and CNS in PD remains elusive.
According to the third edition of International Classification of Sleep Disorders (ICSD-3), a diagnosis of rapid eye movement sleep behaviour disorder (RBD) is a parasomnia, characterised by repeated episodes of sleep-related vocalisation and/or complex motor behaviours. These behaviours are documented by polysomnographic recordings, which demonstrate REM sleep without atonia (RWA). Finally, the disturbance is not better explained by another sleep disorder, mental disorder, medication or substance abuse18. RBD is another non-motor symptom frequently observed in all stages of PD, with a reported pooled prevalence of 42.3%19. One of the clinical manifestations observed in early PD, RBD is strongly associated with more severe motor and non-motor symptoms, including cognitive impairment20,21,22. Several recent studies have indicated that RBD represents an early phase of α-synucleinopathy23. In fact, those with idiopathic RBD have a high risk of developing PD, dementia with Lewy bodies (DLB) and multiple system atrophy (MSA)24. The concept of sleep disorder as a prodromal phase of α-synucleinopathy has attracted growing interest as early intervention and treatment of RBD could have a neuroprotective effect and subsequently modify disease progression25,26.
Mild cognitive impairment (MCI) is among the most frequently reported non-motor symptoms in PD, with a prevalence of approximately 30%27. Characteristic cognitive phenotypes observed in early PD include mild deficits in attention, executive function, verbal memory, and visuospatial domains, involving dopaminergic frontostriatal as well as non-dopaminergic posterior temporal and parietal regions of the brain28. In the early stages of PD, subtle cognitive deficits, such as bradyphrenia, mild aphasia and planning initiation difficulty are frequently observed in PD patients29. Cognitive impairment in PD is of paramount importance as it negatively affects the patient’s quality of life and independence, resulting in a great burden for caregivers, and tremendous economic costs30,31.
Identification of factors that may contribute to cognitive dysfunction is imperative given that PD patients have a sixfold higher risk for developing dementia compared to the general population32. Both constipation and RBD are identified as early signs of PD which may be associated with cognitive impairment among PD patients. Most importantly, RBD and constipation appear to be the earliest non-motor symptoms that can occur during the prodromal phase of PD33,34. However, whether constipation is linked to subsequent cognitive impairment in the course of PD remains unclear, and the possibility that constipation plays a synergistic role with RBD in cognitive performance is uncertain. By accessing the Parkinson’s Progression Markers Initiative (PPMI) database, we aimed to answer the above questions in this study.
Methods
Dataset and study participants
PPMI is an ongoing, prospective cohort study launched in 2010 funded by the Michael J. Fox Foundation to comprehensively assess the progression of clinical symptoms, advanced imaging and biologic sampling in newly diagnosed PD patients with 5 years follow-up. The aim, methodology, and study assessments have been reported elsewhere and are available on the PPMI website. Permission was granted to access the PPMI data. To our knowledge, PPMI is the largest comprehensive study of PD patients with a longitudinal design carried out to date, that is freely available.
Enrolled participants were over 30 years old, with a recent PD diagnosis. The inclusion criteria required that PD subjects had (1) at least two of the following clinical phenotypes: resting tremor, bradykinesia or rigidity (must have either resting tremor or bradykinesia), (2) a PD diagnosis made within 2 years of baseline assessment, (3) Hoehn and Yahr stage I or II at recruitment, and (4) dopamine transporter deficit on single-photon emission computed tomography (SPECT) scan. Subjects were assessed at baseline and followed for 5 years, over which some subjects commenced dopamine replacement therapy (DRT) such as levodopa, dopamine agonist and others.
The overall PPMI study was approved by the Research Subjects Review Board at the University of Rochester, and the study obtained institutional approval from all 33 participating sites in United States, Europe, Israel and Australia. Written informed consent was acquired from each participant before being included in the study. PPMI study was performed in accordance with the relevant guidelines and regulations.
Demographic characteristics
Disease duration at enrolment was calculated in months from the date of PD diagnosis. Body-mass-index (BMI) was calculated in kg/m2 using participants’ height in metres squared (m2) and weight in kilograms (kg).
Dopamine replacement therapy (DRT)
The dose of DRT prescription at year 5 follow-up visit was expressed in levodopa equivalent daily dose (LEDD) in milligrams (mg).
Constipation
Constipation was classified as occurring at least sometimes when measured using the Scale for Outcomes in PD for Autonomic Symptoms (SCOPA-AUT) questionnaire35. The specific questions relating to gastrointestinal function utilised in the current analysis were:
-
1.
Constipation is a blockage of the bowel, a condition in which someone has a bowel movement twice a week or less. In the past month, have you had problems with constipation?
-
2.
In the past months, did you have to strain hard to pass stools? In the past month, have you had involuntary loss of stools?
For each question, response options included were “never”, “sometimes”, “regularly”, and “often”. For the purpose of this evaluation, gut symptoms were defined as occurring “never”, “sometimes”, regularly” or “often”, with scores of 0, 1, 2, 3 respectively allocated. The score for constipation for each participant will be the sum of scores for questions (1) and (2).
REM sleep behaviour disorder
For the diagnosis of probable REM sleep behaviour disorder (pRBD), the REM Sleep Behaviour Disorders Screening Questionnaire (RBDSQ) was used36. An RBDSQ score of 6 and above was considered as a positive test result. A cut-off score of 6 was reported by Chahine et al. as a strong test performance with a sensitivity and specificity of 74.2% and 79.4% respectively37,38.
Neuropsychological tests
At baseline and 5 years following PD diagnosis, the following cognitive tests were administered as measures of the cognitive domain indicated:
-
1.
Montreal Cognitive Assessment (MoCA): global cognitive function39
-
2.
Symbol Digit Modalities Test (SDMT): processing speed/attention40
-
3.
Letter Number Sequencing (LNS): executive function/working memory
-
4.
Semantic fluency: executive function/working memory41
-
5.
Benton Judgment-of-Line-Orientation (JLO) 15-item (split-half) version: visuospatial function42
-
6.
Hopkins Verbal Learning Test-Revised (HVLT-R) immediate, delayed recall discrimination recognition and retention: verbal learning and memory43
Statistical methods
Statistical analyses were run using the Statistical Package for the Social Sciences (SPSS) statistics (version 25, SPSS, Inc., Chicago, IL). Statistical significance was set at p ≤ 0.01. Assumptions for statistical tests were checked and fulfilled if required. In order to incorporate missing data, the feature of approximate Bayesian bootstrap is attempted in SPSS to confirm the results44. Regarding multiple testing, we used Bonferroni correction to examine differences among different groups.
Baseline demographic characteristics of the PPMI participants were summarised using descriptive statistics. Descriptive statistics are reported as means and standard deviation (SD) with range. One-way analysis of variance (ANOVA) was applied to examine the data of male and female PD subjects at baseline and year 5 follow-up visit.
Spearman’s rank order correlation analysis was conducted to investigate the effects age, BMI and years of education on constipation score and neuropsychological test performances. Those variables of interest reaching a significance threshold of p ≤ 0.01 underwent further linear mixed-effects modelling as covariates.
Furthermore, linear mixed-effects modelling was run to evaluate longitudinal data to account for multiple testing. The independent and combined effects of baseline constipation and pRBD on cognitive outcomes in the PD cohort were assessed for each neuropsychological measure. The interaction effect of constipation and sleep disorder on cognitive outcomes of interest was analysed based on the following responses: (1) presence of probable RBD (pRBD) when RBDSQ score was ≥ 6 and (2) presence of constipation when constipation score was > 3. In each model, the follow-up year, presence or absence of pRBD and constipation at baseline were the independent variables. In order to examine the synergistic effect of baseline constipation and pRBD on cognitive outcomes, the independent variable was the constipation*pRBD interaction term. Age, years of education, gender and LEDD were treated as fixed effects in the models. The dependent variables were the repeated scores of each neuropsychological measure over 5 years. Patient identifier was incorporated as random effect in the analysis to allow for interindividual variability for baseline neuropsychological test scores. Other random effect included was the constipation*pRBD*follow-up year.
The discrimination ability of both constipation and pRBD was then assessed by area under the curve of a receiver operating characteristic (ROC) using different cut-off scores for SDMT. SDMT cut-off scores of 28 and 34 were adopted based on previous studies to capture 15% of rapid PD progressors45 and 28% PD subjects with worse SDMT scores, which was equivalent to a MoCA cut-off score of 26 in this study.
Results
Participant characteristics
The sample for this study included newly diagnosed, untreated PD patients (n = 360), who were enrolled into the PPMI study between June, 2010 and April, 2013 with 5 years follow-up assessments. Baseline characteristics of PD subjects are shown in Table 1, with a comparison of clinical variables in men and women. Participants who did not have both baseline constipation, sleep disorders and neuropsychological data were excluded. The PD cohort comprised of 238 male participants and 122 female participants. The male and female PD subjects did not differ in demographic characteristics, apart from male subjects having a greater BMI (27.82 ± 4.55) compared to the female subjects (25.45 ± 4.62) (p < 0.001, Table 1). At baseline, male subjects had a significantly lower MoCA score (males vs females: 26.94 ± 2.05 vs 27.60 ± 2.28, p = 0.008), SDMT score (males vs females: 40.32 ± 9.77 vs 44.36 ± 9.35, p < 0.001), HVLT discrimination recognition score (males vs females: 10.07 ± 1.40 vs 10.76 ± 2.17, p < 0.001), HVLT-R immediate recall score (males vs females: 23.73 ± 4.90 vs 26.36 ± 4.60, p < 0.001) and HVLT-R delayed recall score (males vs females: 8.03 ± 2.56 vs 9.35 ± 2.09, p < 0.001) (Table 1).
At year 5 follow-up, data were available on 281 PD subjects with 189 male and 92 female participants (Supplementary Table S1). Female subjects had better scores on several neuropsychological tests, such as MoCA score (males vs females: 26.24 ± 3.77 vs 27.38 ± 2.86, p = 0.01), SDMT score (males vs females: 37.80 ± 12.71 vs 43.54 ± 12.42, p < 0.001), LNS (males vs females: 9.74 ± 3.14 vs 10.67 ± 2.65, p = 0.01) and semantic fluency score (males vs females: 45.67 ± 12.56 vs 55.42 ± 12.37, p < 0.001) (Supplementary Table S1).
Effect of constipation or pRBD on cognitive outcomes in PD
At baseline, constipation, MoCA, SDMT, LNS, HVLT-R discrimination recognition, HVLT-R immediate recall and HVLT-R delayed recall were associated with age. Years of education was positively associated with baseline SDMT score (rs = 0.140, p = 0.008), HVLT discrimination recognition score (rs = 0.147, p = 0.005), HVLT-R immediate recall score (rs = 0.173, p = 0.001) and HVLT-R delayed recall score (rs = 0.193, p < 0.001). No associations were identified between baseline constipation score or cognitive outcomes and BMI at baseline observation (Supplementary Table S2).
In the linear mixed-effect model, in males, RBDSQ score at baseline was associated with SDMT (p = 0.009) over 5 years (Table 2). No associations were observed between either constipation or RBDSQ with the neuropsychological tasks, MoCA, LNS, JLO, HVLT-R and semantic fluency in both genders (Table 2).
Synergistic effect of the interaction between constipation and RBD on cognitive outcomes in PD
When constipation and RBD scores were dichotomised into those with or without those conditions, a significant interaction between the presence of constipation and pRBD at baseline was present in their association with SDMT (p < 0.001) in male subjects only (Table 2). The SDMT score amongst male PD subjects with both constipation and pRBD at baseline declined by 9.53 points more than in those without both constipation and pRBD on follow-up.
While excluding PD subjects with MoCA < 26, three neuropsychological tests, namely SDMT (p < 0.001), LNS (p = 0.003) and HVLT-R retention (p = 0.01) appeared to be significant in their interaction with both constipation and pRBD in male subjects (Supplementary Table S3). In females, presence of pRBD was associated with MoCA (p = 0.005) and semantic fluency (p = 0.005) scores respectively whereas constipation was associated with MoCA score (p = 0.003) only.
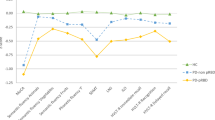
When a cut-off score of 28 for SDMT was applied, the prediction accuracy for cognitive impairment over 5 years for all parameters (constipation, pRBD, age, years of education and LEDD) (Supplementary Fig. S1A) was higher than when a SDMT cut-off of 34 was applied in male subjects (Supplementary Fig. S1B). Combining constipation and pRBD with other demographic variables (age, years of education and LEDD) resulted in a higher AUC compared with constipation or pRBD alone when a SDMT cut-off of 28 was applied (AUC 0.79 [95% CI 0.694–0.892, p < 0.001] vs constipation alone: AUC 0.63 [95% CI 0.586–0.687, p < 0.001] vs pRBD alone: AUC 0.61 [95% CI 0.561–0.662, p < 0.001]) (Supplementary Fig. S1A).
Discussion
Role of gender in cognitive outcomes
In this study of an early drug-naïve PD cohort, we observed significant gender differences in performance on cognitive tasks at the early stages of PD. At enrolment, men performed significantly worse than women on cognitive tasks that measure global cognition, speed-attention processing, verbal learning and memory.
Previous studies of PD have documented certain PD clinical characteristics that are more frequently seen in men than women, including cognitive dysfunction and rigidity, while dyskinesias and depression are more commonly observed in women46,47. The male preponderance in PD could be due to the absence of the neuroprotective role of oestrogen in men. Haaxma and coworkers48 proposed a protective role of oestrogen as hyperestrogenic factors such as parity, later age for menopause, and duration of reproductive life are associated with later age at onset of PD in women48. The possibility of sex steroid hormones underpinning these gender differences is demonstrated in animal and clinical studies. A study in primates showed that oestrogen regulates the production and metabolism of dopamine while modulating the expression and function of the dopamine receptor49. The protective role of oestrogen in women is underlined by the observation that postmenopausal oestrogen therapy was found to be associated with a lower risk of PD in women50. These data clearly suggest a key role of oestrogen in delaying loss of dopaminergic neurons while preserving a functional nigrostriatal dopaminergic pathway49. In conjunction with these observations, our findings suggest that cognition in men deteriorates more rapidly and that the impact of PD on men is more prominent than in women.
Regardless of the large body of research findings, the neuroprotective effect of oestrogen on the nigrostriatal dopaminergic pathway alone is not adequate to explain a more severe clinical phenotype in men with PD. Not all studies investigating the role of oestrogen in PD have found beneficial effect of oestrogen, such as a large prospective cohort study in Denmark, which comprised 27,466 women shows that oestrogen does not alter the risk of PD in women51. The conflicting findings suggest that other factors, such as genetics and environmental factors may also be responsible for the gender differences reported in this study52. We also note that there were great numbers of male than female patients in this data set, so it is possible that statistical power may have influenced the findings to some degree.
Influence of pRBD on cognitive outcomes
Our study has shown that baseline RBDSQ score was strongly associated with measures of processing speed and attention in male subjects. In agreement with our findings, a study based on the Oxford Parkinson’s disease center (OPDC) cohort found that pRBD was significantly associated with cognitive impairment (p = 0.006)53. Previous studies have indicated pRBD as a risk factor for cognitive impairment and deterioration in advanced PD54,55,56. However, more recent studies have shown that pRBD is associated with worse motor and cognitive performances, indicating a more extensive spread of α-synucleinopathy in patients diagnosed with pRBD57,58.
Previous work on the PPMI dataset up to the year 3 follow-up visit demonstrated pRBD at baseline was associated with a greater rate of cognitive decline, specifically in attention and memory domains38. The present study, investigating this association over a 5-year period following PD diagnosis reports similar findings. Interestingly, our further analysis revealed that this association was only present in men—an important finding that was not reported previously, which suggests there may be a gender difference in progression of cognitive decline.
Synergistic effect of the interaction between constipation and RBD on cognitive outcomes
Our study revealed that constipation and pRBD at baseline, in combination, had a significant effect on cognitive performance after 5 years following diagnosis of PD. We observed a synergistic effect of the interaction between constipation and pRBD at baseline on measures of processing speed/attention, verbal learning and memory in men. However, the synergistic effect of constipation and pRBD did not impact any neuropsychological test measure in women. These observations indicate the synergistic effect of constipation and pRBD on cognitive performance was more prominent in men than in women. The synergistic effect of constipation and pRBD produced good discrimination for the prediction of cognitive impairment, particularly measure of processing speed/attention while the addition of demographic variables such as age, years of education and LEDD further improved the predictive value. Demographic variables such as age and educational level are known to be associated with cognitive decline in the PD cohort as demonstrated in a cross-sectional study that utilized the Parkinson’s disease cognitive study (PACOS) data27. Further validation of this finding is warranted to determine whether constipation and pRBD scores can be utilised to predict future attention, motor speed, verbal learning and memory performance in men with PD.
Our results reported that pRBD, independently and in combination with constipation, was related with the cognitive domains, namely processing speed and attention in men, suggesting that pRBD, constipation and cognitive impairment affecting processing speed and attention domains may be attributed to a similar neurodegenerative process, particularly in men. In contrast, LNS, JLO and semantic fluency, which are measures of visuospatial function, executive function and working memory did not seem to relate to either baseline constipation or pRBD in both genders. Our result shows that these specific cognitive domains are less likely to be impacted as PD progresses.
On the other hand, the concept of the gut-brain axis has long been investigated to describe the connection between the gastrointestinal tract and the CNS for a better understanding of the pathogenesis of PD59,60,61. A dual-hit hypothesis was postulated by Braak and colleagues, whereby evaluation of 413 brain autopsies led Braak and colleagues to propose that a neurotropic pathogen initiates PD pathology in the gut, which then spreads to the brain via both nasal and gastric routes62. The gut-originated pathogen appears to propagate to the cortical regions of the brain to cause cognitive dysfunction in PD63. Pan-Montojo and coworkers successfully induced PD-like pathology in mice by oral administration of rotenone, a mitochondrial complex I inhibitor in their Dresden Parkinson Model64. In addition, post-mortem observations of PD patients suggest that the degenerative process in PD may begin in the peripheral autonomic nervous system before affecting the CNS65. Our speculation that there might be a connection between gastrointestinal dysfunction and cognitive impairment in PD is supported by the association between baseline constipation and RBD scores with cognitive performance on follow-up, particularly in men.
In short, the non-motor symptoms of PD, specifically constipation and REM sleep disorder have an association with future cognitive impairment in PD, where gender may play a role in modifying this association. The findings of this study require further validation and extension by screening a larger cohort to allow assessment of the utility of constipation and sleep disorder scores as a tool to predict future cognitive impairment in PD.
Limitations and study improvement
There are a number of limitations in this study. Most importantly, the PPMI cohort generally comprised highly educated and Caucasian volunteers, which reduces the generalisability of the study outcomes. While there are multiple approaches to measure the episodes and severity of constipation, SCOPA-AUT relies on self-reported constipation. Sufferers’ definition and interpretation of constipation vary widely, which makes constipation a subjective experience, thus it can be difficult to understand what symptoms are considered as “real” constipation66. The answer choices for SCOPA-AUT: “never”, “sometimes”, “regularly” and “often” are also subjective to the participants and may not accurately represent the frequency of episodes or severity of constipation. Another study that utilised a variety of questionnaires to evaluate self-reported constipation found that generally PD subjects suffered objective colonic dysfunction more frequently than they reported constipation67. Furthermore, according to the International Classification of Sleep Disorders (ICSD), the gold standard for measuring sleep disorders is polysomnography. However, there was no access to polysomnography data in the PPMI cohort. Therefore, our study might require better measures to quantify or define constipation and pRBD for the administration of self-assessment questionnaires such as SCOPA-AUT and RBDSQ.
Furthermore, studies have indicated there is a possible practice effect from previous exposure to a neuropsychological assessment, resulting in an increasing familiarity on the administration of the neuropsychological assessment68,69. Repeated administration of the same neuropsychological assessments in this study might result in an improvement on scores across the 5-year period, which subsequently reduce the accuracy and reliability of our analyses. This emphasises the need to take into consideration the practice effect that might arise when interpreting cognitive changes across time.
The statistical method, linear mixed-effect modelling, does not account for the varying sample size of the PD cohort at different annual follow-up visits. Attrition during follow-up is often inevitable and could lead to a biased result70. Despite the lower number of PD participants at follow-up visits, the correlation between baseline constipation, pRBD and cognitive performance over 5 years period remained significant. In order to better comprehend the true effects of baseline constipation and pRBD on future cognitive outcomes, this study has included sub-analysis, such as gender-stratified model. The cognitive outcomes were measured by nine neuropsychological scores and they represent a set of inferences simultaneously, which are likely to incur erroneous inferences. Thus, stringent significance threshold, p value no more than 0.01 in this study, is required to compensate for the possible uncertainty in results due to multiple comparisons.
Conclusion
Despite the limitations of this study, our analysis showed that constipation and pRBD are strongly associated with worse cognitive outcomes in PD, while specific cognitive features appear to be more affected in males. Therefore, future work should address whether screening for constipation and sleep disorder might assist with early detection of cognitive impairment in men, to allow a more thorough understanding of the progression and prognosis of cognitive impairment among this sub-group of PD patients.
Ethics approval and consent to participate
Permission and approval for conducting this study was received from the Human Research Advisory Panel (HREAP) Executive of UNSW Sydney, under approval number of HC180099.
Availability of data and materials
Data used in the preparation of this article were obtained from the Parkinson’s Progression Markers Initiative (PPMI) database (www.ppmi-info.org/data). For up-to-date information on the database, visit www.ppmi-info.org. All data generated or analysed during this study are included in this published article and its supplementary information files.
References
de Lau, L. M. & Breteler, M. M. Epidemiology of Parkinson’s disease. Lancet Neurol. 5, 525–535. https://doi.org/10.1016/S1474-4422(06)70471-9 (2006).
Tysnes, O. B. & Storstein, A. Epidemiology of Parkinson’s disease. J. Neural Trans. (Vienna, Austria: 1996) 124, 901–905. https://doi.org/10.1007/s00702-017-1686-y (2017).
Van Den Eeden, S. K. et al. Incidence of Parkinson’s disease: variation by age, gender, and race/ethnicity. Am. J. Epidemiol. 157, 1015–1022. https://doi.org/10.1093/aje/kwg068 (2003).
Schrag, A., Ben-Shlomo, Y. & Quinn, N. P. Cross sectional prevalence survey of idiopathic Parkinson’s disease and Parkinsonism in London. BMJ 321, 21–22. https://doi.org/10.1136/bmj.321.7252.21 (2000).
Poewe, W. Non-motor symptoms in Parkinson’s disease. Eur. J. Neurol. 15(Suppl 1), 14–20. https://doi.org/10.1111/j.1468-1331.2008.02056.x (2008).
Rybicki, B. A., Johnson, C. C., Peterson, E. L., Kortsha, G. X. & Gorell, J. M. A family history of Parkinson’s disease and its effect on other PD risk factors. Neuroepidemiology 18, 270–278. https://doi.org/10.1159/000026222 (1999).
Serra, M. C. et al. Increased odds of bladder and bowel symptoms in early Parkinson’s disease. Neurourol. Urodyn. https://doi.org/10.1002/nau.23443 (2017).
Hawkes, C. H., Del Tredici, K. & Braak, H. A timeline for Parkinson’s disease. Parkinsonism Relat. Disord. 16, 79–84. https://doi.org/10.1016/j.parkreldis.2009.08.007 (2010).
Grinberg, L. T., Rueb, U., Alho, A. T. & Heinsen, H. Brainstem pathology and non-motor symptoms in PD. J. Neurol. Sci. 289, 81–88. https://doi.org/10.1016/j.jns.2009.08.021 (2010).
Martinez-Martin, P. et al. Prevalence of nonmotor symptoms in Parkinson’s disease in an international setting; study using nonmotor symptoms questionnaire in 545 patients. Mov. Disord. 22, 1623–1629. https://doi.org/10.1002/mds.21586 (2007).
Edwards, L. L., Pfeiffer, R. F., Quigley, E. M., Hofman, R. & Balluff, M. Gastrointestinal symptoms in Parkinson’s disease. Mov. Disord. 6, 151–156. https://doi.org/10.1002/mds.870060211 (1991).
Palma, J. A. & Kaufmann, H. Autonomic disorders predicting Parkinson disease. Parkinsonism Relat. Disord. 20, S94-98. https://doi.org/10.1016/s1353-8020(13)70024-5 (2014).
Klingelhoefer, L. & Reichmann, H. Pathogenesis of Parkinson disease—the gut-brain axis and environmental factors. Nat. Rev. Neurol. 11, 625–636. https://doi.org/10.1038/nrneurol.2015.197 (2015).
Winge, K., Rasmussen, D. & Werdelin, L. Constipation in neurological diseases. J. Neurol. Neurosurg. Psychiatry 74, 13–19. https://doi.org/10.1136/jnnp.74.1.13 (2003).
Abbott, R. D. et al. Frequency of bowel movements and the future risk of Parkinson’s disease. Neurology 57, 456–462 (2001).
Rota, L. et al. Constipation, deficit in colon contractions and alpha-synuclein inclusions within the colon precede motor abnormalities and neurodegeneration in the central nervous system in a mouse model of alpha-synucleinopathy. Transl. Neurodegen. 8, 5. https://doi.org/10.1186/s40035-019-0146-z (2019).
Berg, D. et al. MDS research criteria for prodromal Parkinson’s disease. Mov. Disord. 30, 1600–1611. https://doi.org/10.1002/mds.26431 (2015).
Sateia, M. J. International classification of sleep disorders-third edition: highlights and modifications. Chest 146, 1387–1394. https://doi.org/10.1378/chest.14-0970 (2014).
Zhang, X., Sun, X., Wang, J., Tang, L. & Xie, A. Prevalence of rapid eye movement sleep behavior disorder (RBD) in Parkinson’s disease: a meta and meta-regression analysis. Neurological. Sci. Off. J. Italian Neurolog. Soc. Italian Soc. Clin. Neurophysiol. 38, 163–170. https://doi.org/10.1007/s10072-016-2744-1 (2017).
Anang, J. B. et al. Predictors of dementia in Parkinson disease: a prospective cohort study. Neurology 83, 1253–1260. https://doi.org/10.1212/wnl.0000000000000842 (2014).
Bohnen, N. I. & Hu, M. Sleep disturbance as potential risk and progression factor for Parkinson’s disease. J. Parkinson’s Dis. https://doi.org/10.3233/jpd-191627 (2019).
Hansen, I. H., Marcussen, M., Christensen, J. A., Jennum, P. & Sorensen, H. B. Detection of a sleep disorder predicting Parkinson's disease. Conference proceedings: Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society. Annual Conference, 2013, 5793–5796, https://doi.org/10.1109/embc.2013.6610868 (2013).
Hogl, B., Stefani, A. & Videnovic, A. Idiopathic REM sleep behaviour disorder and neurodegeneration—an update. Nat. Rev. Neurol. 14, 40–55. https://doi.org/10.1038/nrneurol.2017.157 (2018).
Postuma, R. B. et al. Risk and predictors of dementia and parkinsonism in idiopathic REM sleep behaviour disorder: a multicentre study. Brain 142, 744–759. https://doi.org/10.1093/brain/awz030 (2019).
Schrempf, W., Brandt, M. D., Storch, A. & Reichmann, H. Sleep disorders in Parkinson’s disease. J. Parkinson’s Dis. 4, 211–221. https://doi.org/10.3233/jpd-130301 (2014).
Iranzo, A. et al. Neurodegenerative disease status and post-mortem pathology in idiopathic rapid-eye-movement sleep behaviour disorder: an observational cohort study. Lancet Neurol. 12, 443–453. https://doi.org/10.1016/s1474-4422(13)70056-5 (2013).
Monastero, R. et al. Mild cognitive impairment in Parkinson’s disease: the Parkinson’s disease cognitive study (PACOS). J. Neurol. 265, 1050–1058. https://doi.org/10.1007/s00415-018-8800-4 (2018).
Janvin, C. C. et al. Cognitive profiles of individual patients with Parkinson’s disease and dementia: comparison with dementia with lewy bodies and Alzheimer’s disease. Mov. Disord. 21, 337–342. https://doi.org/10.1002/mds.20726 (2006).
Truong, D. D., Bhidayasiri, R. & Wolters, E. Management of non-motor symptoms in advanced Parkinson disease. J. Neurol. Sci. 266, 216–228. https://doi.org/10.1016/j.jns.2007.08.015 (2008).
Olesen, J., Gustavsson, A., Svensson, M., Wittchen, H. U. & Jonsson, B. The economic cost of brain disorders in Europe. Eur. J. Neurol. 19, 155–162. https://doi.org/10.1111/j.1468-1331.2011.03590.x (2012).
Tomic, S., Rajkovaca, I., Pekic, V., Salha, T. & Misevic, S. Impact of autonomic dysfunctions on the quality of life in Parkinson’s disease patients. Acta Neurol. Belg. 117, 207–211. https://doi.org/10.1007/s13760-016-0739-6 (2017).
Aarsland, D. et al. Risk of dementia in Parkinson’s disease: a community-based, prospective study. Neurology 56, 730–736 (2001).
Poewe, W. et al. Parkinson disease. Nat. Rev. Dis. Prim. 3, 17013. https://doi.org/10.1038/nrdp.2017.13 (2017).
Kalia, L. V. & Lang, A. E. Parkinson’s disease. Lancet (London, England) 386, 896–912. https://doi.org/10.1016/s0140-6736(14)61393-3 (2015).
Visser, M., Marinus, J., Stiggelbout, A. M. & Van Hilten, J. J. Assessment of autonomic dysfunction in Parkinson’s disease: the SCOPA-AUT. Mov. Disord. 19, 1306–1312. https://doi.org/10.1002/mds.20153 (2004).
Stiasny-Kolster, K. et al. The REM sleep behavior disorder screening questionnaire–a new diagnostic instrument. Mov. Disord. 22, 2386–2393. https://doi.org/10.1002/mds.21740 (2007).
Chahine, L. M. et al. Questionnaire-based diagnosis of REM sleep behavior disorder in Parkinson’s disease. Mov. Disord. 28, 1146–1149. https://doi.org/10.1002/mds.25438 (2013).
Chahine, L. M. et al. Longitudinal changes in cognition in early Parkinson’s disease patients with REM sleep behavior disorder. Parkinsonism Relat. Disord. 27, 102–106. https://doi.org/10.1016/j.parkreldis.2016.03.006 (2016).
Nasreddine, Z. S. et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 53, 695–699. https://doi.org/10.1111/j.1532-5415.2005.53221.x (2005).
Smith, A. Symbol digits modalities test Los Angeles: western psychological services. Los Angeles Western Psychol. Serv. 83–91 (1968).
Gladsjo, J. A. et al. Norms for letter and category fluency: demographic corrections for age, education, and ethnicity. Assessment 6, 147–178. https://doi.org/10.1177/107319119900600204 (1999).
Benton, A. L., Sivan, A. B., Hamsher, K. D., Varney, N. R. & Spreen, O. Contributions to neuropsychological assessment: a clinical manual (Oxford University Press, Oxford, 1994).
Brandt, J. & Benedict, R. H. Hopkins verbal learning test-revised: professional manual. (Psychological Assessment Resources, 2001).
Dong, Y. & Peng, C. Y. Principled missing data methods for researchers. SpringerPlus 2, 222. https://doi.org/10.1186/2193-1801-2-222 (2013).
Huang, Y., Rowe, D. B. & Halliday, G. M. Interaction between α-synuclein and tau genotypes and the progression of Parkinson’s disease. J. Parkinson’s Dis. 1, 271–276. https://doi.org/10.3233/jpd-2011-11027 (2011).
Baldereschi, M. et al. Parkinson’s disease and Parkinsonism in a longitudinal study: two-fold higher incidence in men. ILSA Working Group. Italian longitudinal study on aging. Neurology 55, 1358–1363. https://doi.org/10.1212/wnl.55.9.1358 (2000).
Bower, J. H., Maraganore, D. M., McDonnell, S. K. & Rocca, W. A. Incidence and distribution of parkinsonism in Olmsted County, Minnesota, 1976–1990. Neurology 52, 1214–1220. https://doi.org/10.1212/wnl.52.6.1214 (1999).
Haaxma, C. A. et al. Gender differences in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 78, 819–824. https://doi.org/10.1136/jnnp.2006.103788 (2007).
Leranth, C. et al. Estrogen is essential for maintaining nigrostriatal dopamine neurons in primates: implications for Parkinson’s disease and memory. J. Neurosci. Off. J. Soc. Neurosci. 20, 8604–8609 (2000).
Currie, L. J., Harrison, M. B., Trugman, J. M., Bennett, J. P. & Wooten, G. F. Postmenopausal estrogen use affects risk for parkinson disease. JAMA Neurol. 61, 886–888. https://doi.org/10.1001/archneur.61.6.886 (2004).
Rugbjerg, K., Christensen, J., Tjonneland, A. & Olsen, J. H. Exposure to estrogen and women’s risk for Parkinson’s disease: a prospective cohort study in Denmark. Parkinsonism Relat. Disord. 19, 457–460. https://doi.org/10.1016/j.parkreldis.2013.01.008 (2013).
Wooten, G. F., Currie, L. J., Bovbjerg, V. E., Lee, J. K. & Patrie, J. Are men at greater risk for Parkinson’s disease than women?. J. Neurol. Neurosurg. Psychiatry 75, 637–639. https://doi.org/10.1136/jnnp.2003.020982 (2004).
Rolinski, M. et al. REM sleep behaviour disorder is associated with worse quality of life and other non-motor features in early Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 85, 560–566. https://doi.org/10.1136/jnnp-2013-306104 (2014).
Jozwiak, N. et al. REM sleep behavior disorder and cognitive impairment in Parkinson’s disease. Sleep https://doi.org/10.1093/sleep/zsx101 (2017).
Gagnon, J. F. et al. REM sleep behavior disorder and REM sleep without atonia in Parkinson’s disease. Neurology 59, 585–589. https://doi.org/10.1212/wnl.59.4.585 (2002).
Postuma, R. B. et al. Rapid eye movement sleep behavior disorder and risk of dementia in Parkinson’s disease: a prospective study. Mov. Disord. 27, 720–726. https://doi.org/10.1002/mds.24939 (2012).
Pagano, G. et al. REM behavior disorder predicts motor progression and cognitive decline in Parkinson disease. Neurology 91, e894–e905. https://doi.org/10.1212/wnl.0000000000006134 (2018).
Pilotto, A. et al. Orthostatic hypotension and REM sleep behaviour disorder: impact on clinical outcomes in α-synucleinopathies. J. Neurol. Neurosurg. Psychiatry 90, 1257–1263. https://doi.org/10.1136/jnnp-2019-320846 (2019).
Pretorius, E., Bester, J. & Kell, D. B. A bacterial component to Alzheimer’s-type dementia seen via a systems biology approach that links iron dysregulation and inflammagen shedding to disease. J. Alzheimers Dis. 53, 1237–1256. https://doi.org/10.3233/JAD-160318 (2016).
Sampson, T. R. et al. Gut microbiota regulate motor deficits and neuroinflammation in a model of Parkinson’s disease. Cell 167, 1469–1480. https://doi.org/10.1016/j.cell.2016.11.018 (2016).
Mamikonyan, E. et al. Mild cognitive impairment is common in Parkinson’s disease patients with normal mini-mental state examination (MMSE) scores. Parkinsonism Relat. Disord. 15, 226–231. https://doi.org/10.1016/j.parkreldis.2008.05.006 (2009).
Braak, H. et al. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol. Aging 24, 197–211 (2003).
Kim, S. et al. Transneuronal propagation of pathologic alpha-synuclein from the gut to the brain models Parkinson’s disease. Neuron https://doi.org/10.1016/j.neuron.2019.05.035 (2019).
Pan-Montojo, F. et al. Progression of Parkinson’s disease pathology is reproduced by intragastric administration of rotenone in mice. PLoS ONE 5, e8762. https://doi.org/10.1371/journal.pone.0008762 (2010).
Kaufmann, H., Nahm, K., Purohit, D. & Wolfe, D. Autonomic failure as the initial presentation of Parkinson disease and dementia with Lewy bodies. Neurology 63, 1093–1095. https://doi.org/10.1212/01.wnl.0000138500.73671.dc (2004).
Frank, L., Flynn, J. & Rothman, M. Use of a self-report constipation questionnaire with older adults in long-term care. Gerontologist 41, 778–786. https://doi.org/10.1093/geront/41.6.778 (2001).
Knudsen, K. et al. Objective colonic dysfunction is far more prevalent than subjective constipation in Parkinson’s disease: a colon transit and volume study. J. Parkinson’s Dis. 7, 359–367. https://doi.org/10.3233/jpd-161050 (2017).
McCaffrey, R. J., Ortega, A., Orsillo, S. M., Nelles, W. B. & Haase, R. F. Practice effects in repeated neuropsychological assessments. Clin. Neuropsychol. 6, 32–42. https://doi.org/10.1080/13854049208404115 (1992).
Calamia, M., Markon, K. & Tranel, D. Scoring higher the second time around: meta-analyses of practice effects in neuropsychological assessment. Clin. Neuropsychol. 26, 543–570. https://doi.org/10.1080/13854046.2012.680913 (2012).
Howe, C. J., Cole, S. R., Lau, B., Napravnik, S. & Eron, J. J. Jr. Selection Bias Due to Loss to Follow Up in Cohort Studies. Epidemiology (Cambridge, Mass) 27, 91–97. https://doi.org/10.1097/ede.0000000000000409 (2016).
Acknowledgements
We thank S Leigh for assistance with statistics.
Funding
PPMI, a public-private partnership, is funded by the Michael J. Fox Foundation for Parkinson’s Research and funding partners, including AbbVie, Allergan, Avid Radiopharmaceuticals, Biogen Idec, Bio-Legend, Bristol-Meyers Squibb, Celgene, Jenali, GE Healthcare, Genentech, GlaxoSmithKline, Lilly, Lundbeck, Merck, Meso Scale Discovery, Pfizer, Piramal, Prevail Therapeutics, Roche, Sanofi Genzyme, Servier, Takeda, Teva, UCB, Verily, Voyager Therapeutics and Golub Capital. This project is funded by UNSW Sydney, Australia, the National Natural Science Foundation of China (Grant No. 82071417), and PI start-up fund, Beijing Tiantan Hospital, Capital Medical University, China. The funders of this project had no role in the design of the study and collection, analysis, and interpretation of data nor in writing the manuscript.
Author information
Authors and Affiliations
Contributions
M.J.M. and Y.H. designed the study. W.L.K., M.J.M. and Y.H. acquired and analysed data for the study. W.L.K. drafted the tables and original report, which was edited and revised by M.J.M. and Y.H. E.Q. assisted with data cleaning.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kong, W.L., Huang, Y., Qian, E. et al. Constipation and sleep behaviour disorder associate with processing speed and attention in males with Parkinson’s disease over five years follow-up. Sci Rep 10, 19014 (2020). https://doi.org/10.1038/s41598-020-75800-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-75800-4
This article is cited by
-
Application of non-invasive neuromodulation in children with neurodevelopmental disorders to improve their sleep quality and constipation
BMC Pediatrics (2023)
-
The brain-first vs. body-first model of Parkinson’s disease with comparison to alternative models
Journal of Neural Transmission (2023)
-
A postmortem study suggests a revision of the dual-hit hypothesis of Parkinson’s disease
npj Parkinson's Disease (2022)
-
Early constipation predicts faster dementia onset in Parkinson’s disease
npj Parkinson's Disease (2021)
-
Diagnostic value of skin RT-QuIC in Parkinson’s disease: a two-laboratory study
npj Parkinson's Disease (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
