
Abstract
Age estimation is a major step in forensic and legal procedures. Its relevance has been increasing due to growing society issues, such as identification of missing people, crimes against minors or lack of valid identification papers from locals or foreigners. Evaluation of the cut-off value of the Third Molar Maturation Index (I3M) = 0.08 for discriminating minors from adults in the Portuguese population. The left lower third molars were analysed by applying a specific cut-off value of 0.08 determined by Cameriere et al. in 2008. A sample of 778 digital panoramic radiographs of a representative Portuguese sample (442 females and 336 males), in the age range of 12–24 years (mean age 17.7 ± 2.98 years in females and 18.1 ± 3.0 years in males), was retrospectively evaluated. I3M decreased as the real age gradually increased in both sexes. The 0.08 cut-off score was valuable in discriminating adults from minors. According to the pooled results, the accuracy, by means of area under the curve, was 92.8% (95% confidence interval (CI) 91.0–94.6%). The proportion of correctly classified subjects (sensitivity) was 90.7% (95% CI 88.7–92.8%) and the specificity was 94.9% (95% CI 93.3–96.4%). The results show that I3M is a valuable method to differentiate minors from adults in the Portuguese population.
Similar content being viewed by others


Introduction
Age estimation is a key step in human identification, legal practice and clinical research. Some areas of interest are in the aid of identification of missing people, crimes against minors, adoption procedures, invalid identification documents and mass migration1,2,3,4. For such reasons, a reliable standardized age estimation tool to differentiate minors from adults is of great interest1,5.
Based on research on the distinguishable features of skull bones, symphysis pubis, long bones, hand bones and permanent dentition2,6,7,8,9,10, the Study Group on Forensic Age Diagnostics of the German Society of Legal Medicine (AGFAD) presented the criteria for age estimation in lawsuits. Dental examination is highly reliable because dental development is less influenced by both internal and external factors1,4. With the exception of the third molars, permanent dentition completed its development between 12 and 14 years of age. Third molars are estimated to develop between the ages of 15.7 and 23.3 years, and because this timeframe intercrosses the legal age of 18, they can serve as a discriminant tool to distinguish adults from minors1,2,3,5.
In Portugal, the age of criminal and legal responsibility is 14 years old. If a crime is committed by an individual between 12 and 16 years old, he will be tried in a juvenile court. In the event of a conviction, the individual may be condemned to serve time in a closed educational center. On the other hand, if the person who commits the crime has between 16 and 18 years of age, may be considered adult and will be judged under general criminal laws. For all purposes, the legal age of adulthood in Portugal is 18 years old11,12.
In 2008, Cameriere et al.13 proposed the Third Molar Maturation Index (I3M) as a predictive tool to discriminate adult age. The I3M relies on the relationship between chronological age and the measures of the open apices of the lower left third molar. The bidimensional widths of the apical and tooth lengths are measured and used to calculate the I3M. Then, a cutoff value (0.08) is set to differentiate minors from adults13.
Over the last years, I3M was successfully validated worldwide, in Europe2,13,14,15,16,17,18,19,20,21,22,23, Africa1,24,25,26,27, Asia5,28,29,30,31, America3,32,33,34,35,36 and Oceania37. Overall, I3M had considerable reliability among all countries, however, to date, this method is not validated for a Portuguese sample. Therefore, investigating if the I3M is suitable for the Portuguese population would be of great interest.
Given the evidence on high population movements in the Portuguese population, contributing to a higher level of diversity than some neighboring populations38,39, we aimed to test the validity of the I3M in a Portuguese representative sample, by using panoramic radiographs (PRs).. Secondly, we looked for the influence of sex on its validity. Our null hypothesis was that the I3M has no validity to discriminate adult age in this Portuguese sample.
Materials and methods
Source of data and sample size
This retrospective observational study has received approval from the Egas Moniz Ethics Committee (ID 887). Written informed consent was obtained for each participant, during the first appointment at the Egas Moniz Dental Clinic (EMDC), (Almada, Portugal). Regarding participants under 18, a parent and/or legal guardian and this study gave and signed the informed consent. This research was conducted in accordance with the Declaration of Helsinki, as revised in 2013.
The present study follows the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD) reporting guidelines40 for validation of prediction models. This study was conducted on a triple-blind basis with respect to: (1) diagnosis and clinical outcome; (2) data collection; and (3) analysis.
Participants
A consecutive sample of 1267 digital PRs, taken between September 2017 and January 2020, were considered for this study.
The inclusion criteria were: the presence of the lower third molar; known chronological age between 12 and 24 years old5,13,36; and absence of evident bone pathologies or systemic diseases that may affect tooth development. Exclusion criteria included spatial orientation of the third molar that prevents correct measuring, endodontic treatment and/or coronary restoration on the third molar, extensive cavities or abnormal dental anatomy, congenital anomalies and poor-quality or distorted X-rays41.
Outcome, predictors and measurement reproducibility
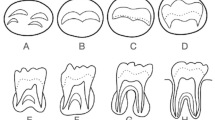
All digital PRs were converted to JPEG documents for the examination with ImageJ image processing software (Graphics Suite X7, Ottawa, Canada) by one trained and calibrated observer (JAN). The I3M index of each evaluated third molar was performed according to the Cameriere et al. method13. If the root development of the third molar is complete, then I3M = 0.0. If not, I3M was calculated as the distance between the inner sides of the open apex (A and B) divided by the tooth length (C) (Fig. 1). In case of I3M < 0.08, the individual is classified as 18 years old or older and if I3M ≥ 0.08, the individual as considered a minor.

Measurement of the third molar index.
The Kappa correlation index was used to test the agreement of classification of individuals younger than 18 years, aged 18 years or older. The Intraclass Correlation Coefficient (ICC) was used to analyze the measurements of open apices. Previously, twelve PRs were randomly chosen from the total sample, measured and remeasured one week later by the same researcher (JAN). Kappa index indicated a perfect agreement for the inter-examiner analysis (κ = 1.00). Intraclass correlation coefficient (ICC) showed absolute agreement (ICC = 0.96), according to Landis and Koch42.
Statistical analysis
Data analysis was performed using SPSS Statistics v. 25.0 for Windows (IBM; Armonk, New York, USA). The estimated I3M index result was compared against the actual chronological age to determine the method’s performance in global and according to sex (females and males). For this purpose, contingency tables were used to calculate true positive (TP), true negative (TN), false positive (FP) and false negative (FN) values (Table 1). Then, several performance indicators were determined and detailed in Table 143. Performance measurement was assessed through binary and multiclass area under the curve (AUC), through receiver operating characteristics (ROC) analysis. The correspondent 95% confidence intervals (95% CI) were also determined. Bayes post-test probability (p) of being 18 years or older is computed to discriminate between those who are or are not aged 18 years or more. According to Bayes’ theorem, p may be written as:
In the post-test probability p, p0 defines the probability that a participant is 18 years or older given that he or she is aged between 12 and 24 years, in the target population. In this study, we calculated the probability p0 as the proportion of participants between 18 and 24 years of age who live in Portugal and those who are aged between 12 and 24 years. This value (p0) was considered to be 0.55 (global, males and females) according to the Portuguese National Statistics Institute - Instituto Nacional de Estatística (INE) (https://www.ine.pt/xportal).
Results
Participants
A total of 778 digital PRs (336 males and 442 females) met the inclusion criteria, with 489 being excluded due to absence of third molars. The distribution of age and sex is depicted in Table 2. The mean ages of the males and females, aged between 12 and 24 years, were 18.1 ± 3.0 years old and 17.7 ± 3.0, respectively, without statistically significant difference (p = 0.078).
Model performance
The estimated age of majority was correlated with the chronological age (p < 0.001). The I3M values decreased as age increased across all age groups in both sexes, showing that the lower third molar mineralization occurred earlier in females than in males (Fig. 2).

Boxplot of relationship between chronological age and I3M of open apices of lower left third molar, according to females and males.
Then, pooled data of both sexes as well as separately was analysed (Table 3). The overall results were 92.8% (95% CI 91–94.6%), 90.7% (95% CI 88.7–92.8%) and 94.9% (95% CI 93.3–96.4%) for accuracy, sensitivity and specificity, respectively. Concerning the LR+ and the LR−, their values were as follows: 17.7 (95% CI 12.5–20.3) and 0.10 (95% CI 0.08–0.12). Global post-test probability was 95.6% (95% CI 94.1–97.0%).
Males were better classified into adults or minors (94%; 95% CI 92.4–95.7%) than females (91.2%; 95% CI 89.9–93.8%). Specificity was better for females (95.7%; 95% CI 94.3–97.1%) compared to males (93.5%; 95% CI 91.8–95.3%) while sensitivity was better for males (94.9%; 95% CI 93.3–96.4%) compared to females (87.5%; 95% CI 85.2–89.8%). Both estimating post-test probability results were excellent; in males was 94.7% (95% CI 93.1–96.3%) and 96.2% (95% CI 94.2–97.5%) in females. The LR+ and LR− were 20.5 (95% CI 15.0–23.3) and 0.13 (95% CI 0.11–0.15), respectively, in females and 14.6 (95% CI 9.9–17.1) and 0.06 (95% CI 0.04–0.08), respectively, in males.
Data from articles showing results with cutoff value 0.08 in various European samples
Also, we compared the results of the present study with previous European studies (Tables 4 and 5 present).
Discussion
The present study is the first to test the validity of I3M in a Portuguese sample. Overall, the null hypothesis was rejected, that is, the I3M is a reliable tool to discriminate adult age in this Portuguese population. Further, I3M was more accurate in male participants. These results have important implications because this tool has potential to be used in legal and criminal settings.
Discriminating minors from adults is important to prevent legal wrongful procedures, specially in cases where valid identification documents are lacking, in order to prevent legal wrongful procedures4,32. Notwithstanding, age estimation is challenging, particularly in the differentiation teens from young adults (aged 15 years old to early 20 s), as the physical appearance and characterization are not clearly related of being an adult1,4. From 15 years of age, the third molars are only teeth not fully developed, as this clinical circumstance is useful in forensic sciences44.
In the Portuguese context, age estimation methods involving dental measures were reported in previous studies45,46,47,48,49,50. Caldas et al. (2011)46 have evaluated third molars, however the method and the age range of these participants were not comparable. Thus, to the best of our knowledge, this is the first study that validates the use of the I3M cutoff value of 0.08 in the Portuguese population.
Cameriere et al. (2008)13 introduced a new methodology for age estimation based on the ratio between measures of the open apices and height of the third molar. Since then, the I3M has been validated in every continent with very strong results, showing only slight variations among different ethnicities.
The sensibility indicates the I3M ability to correctly identify individuals who are 18 years or older (I3M < 0.08). On the other hand, specificity is the ability to discriminate individuals younger than 18 years old (I3M ≥ 0.08). Santiago et al. (2018)41 reported that I3M outperforms in individuals younger than 18 years due to the higher specificity of this tool. This is key in forensic science because if a minor is wrongly processed as an adult it would violate its rights23,41.
To better integrate the results of our study within the European scenario, we analyzed every European study that have analyzed the validity of I3M (Fig. 3). Our pooled overall results on accuracy (92.8%; 95% CI 91.0–94.6%) outperformed all previous studies that presented pooled data2,13,17,22,23 . Both sensitivity and specificity pooled results also surpassed most previous European studies2,22,23 except for Cameriere et al.13 (98%) and De Luca et al.17 (95.7%; 95% CI 92.1–98.0%). The estimated post-test probability of the pooled data (95.6%; 95% CI 94.1–97.0%) showed similar results with previous studies.

Pooled results from different European populations.
When analysing our data regarding males and females (Fig. 4), we demonstrated alike maturation of third molars in both males and females, which is in line with similar studies14,15,16,19,20,21,22,23,44,51. Previous European studies present slightly better accuracy and sensibility in males than in females14,15,16,19,20,21,22,23,44,51. Contrary, females presented better specificity than males14,15,16,19,20,21,22,23,44,51. Therefore, I3M seems to be slightly more accurate in males, although it is equivalent to the female participants in this Portuguese population. The effect of age on I3M performance is proposed to rely on the maturation development according to sex as women tend to develop at a younger ages than men52. This maturation difference is suggested to explain the I3M results discrepancies between both sexes, however more studies are needed to fully understand the biological reasons upon this subject19,41,51.

Discriminated results by sex, from different European populations.
Estimated post-test probability of both male (94.7%; 95% CI 93.1–96.3%) and female (96.2%; 95% CI 94.8–97.5%) demonstrated results compatible with other European studies2,14,15,19,20,21,22,23,44,51. It is important to refer that Zelic et al.20 and Kelmendi et al.21 reported results very close to 100% in females, and Gulsahi et al.19 reported results of 100% in both sexes, although the sample size was one of the smallest in all European studies (n = 293), which may influence these results.
The likelihood ratio is a practical measure of diagnostic accuracy. The higher the value of LR + , more the test has the capability of establishing the tested condition; an LR + value greater than 10 defines it as a good diagnostic test. In our study, balanced values of LR + and LR − have been achieved. Although I3M presented higher LR + in females (20.5; 95% CI 15–23.3) then males (14.6; 95% CI 9.9–17.1), I3M is an excellent prediction of the probability of majority; and lower LR − (0.06; 95% CI 0.04–0.08) in males than (0.13; 95% CI 0.11–0.15) in females, prove that the test is also an excellent tool at classifying individuals younger than 18 years of age, despite the sex of the individuals19,23.
In conclusion, I3M is a suitable method in legal and forensic purposes to identify minors from adults in the Portuguese population. Further, the cut-off value used (0.08) is predictable and useful to discriminating individuals younger than 18 years of age (high specificity in both sexes).
References
Angelakopoulos, N. et al. Third molar maturity index (I 3M ) for assessing age of majority: study of a black South African sample. Int. J. Legal Med. 132, 1457–1464 (2018).
Cameriere, R. et al. Assessment of legal adult age of 18 by measurement of open apices of the third molars: Study on the Albanian sample. Forensic Sci. Int. 245(205), e1-205.e5 (2014).
da Nóbrega, J. B. M. et al. Validation of the Third Molar Maturation Index to estimate the age of criminal responsibility in Northeastern Brazil. Forensic Sci. Int. 304, 109917 (2019).
Cunha, E. et al. The problem of aging human remains and living individuals: a review. Forensic Sci. Int. 193, 1–13 (2009).
Chu, G. et al. Third molar maturity index (I3M) for assessing age of majority in northern Chinese population. Int. J. Legal Med. 132, 1759–1768 (2018).
Ozveren, N., Serindere, G., Meric, P. & Cameriere, R. A comparison of the accuracy of Willems’ and Cameriere’s methods based on panoramic radiography. Forensic Sci. Int. 302, 109912 (2019).
Cameriere, R., Cingolani, M., Giuliodori, A., De Luca, S. & Ferrante, L. Radiographic analysis of epiphyseal fusion at knee joint to assess likelihood of having attained 18 years of age. Int. J. Legal Med. 126, 889–899 (2012).
Liversidge, H. M., Speechly, T. & Hector, M. P. Dental maturation in British children: are Demirjian’s standards applicable?. Int. J. Paediatr. Dent. 9, 263–269 (1999).
Garamendi, P. M., Landa, M. I., Ballesteros, J. & Solano, M. A. Reliability of the methods applied to assess age minority in living subjects around 18 years old: a survey on a Moroccan origin population. Forensic Sci. Int. 154, 3–12 (2005).
Garamendi, P. M., Landa, M. I., Botella, M. C. & Alemán, I. Forensic age estimation on digital X-ray images: medial epiphyses of the clavicle and first rib ossification in relation to chronological age. J. Forensic Sci. 56, 3–12 (2011).
Cipriani, D. Children’s rights and the minimum age of criminal responsibility: a global perspective. Br. J. Criminol. 50, 990–991 (2010).
Justiça, M. da. Diário da República no273. Decreto de Lei no496/77 (1977).
Cameriere, R., Ferrante, L., De Angelis, D., Scarpino, F. & Galli, F. The comparison between measurement of open apices of third molars and Demirjian stages to test chronological age of over 18 year olds in living subjects. Int. J. Legal Med. 122, 493–497 (2008).
Tafrount, C., Galić, I., Franchi, A., Fanton, L. & Cameriere, R. Third molar maturity index for indicating the legal adult age in southeastern France. Forensic Sci. Int. 294(218), e1-218.e6 (2019).
Boyacıoğlu Doğru, H. et al. Age of majority assessment in Dutch individuals based on Cameriere’s third molar maturity index. Forensic Sci. Int. 282, 231.e1-231.e6 (2018).
Cameriere, R. et al. Adult or not? Accuracy of Cameriere’s cut-off value for third molar in assessing 18 years of age for legal purposes. Minerva Stomatol. 63, 283–294 (2014).
De Luca, S. et al. Accuracy of Cameriere’s cut-off value for third molar in assessing 18 years of age. Forensic Sci. Int. 235(102), e1-102.e6 (2014).
Galić, I. et al. Cameriere’s third molar maturity index in assessing age of majority. Forensic Sci. Int. 252, 191 e1-191.e5 (2015).
Gulsahi, A., De Luca, S., Cehreli, S. B., Tirali, R. E. & Cameriere, R. Accuracy of the third molar index for assessing the legal majority of 18 years in Turkish population. Forensic Sci. Int. 266, 584 e1-584.e6 (2016).
Zelic, K. et al. Accuracy of Cameriere’s third molar maturity index in assessing legal adulthood on Serbian population. Forensic Sci. Int. 259, 127–132 (2016).
Kelmendi, J. et al. The third molar maturity index in indicating the legal adult age in Kosovar population. Int. J. Legal Med. 132, 1151–1159 (2018).
Różyło-Kalinowska, I., Kalinowski, P., Kozek, M., Galić, I. & Cameriere, R. Validity of the third molar maturity index I3M for indicating the adult age in the Polish population. Forensic Sci. Int. 290(352), e1-352.e6 (2018).
Spinas, E., De Luca, S., Lampis, L., Velandia Palacio, L. A. & Cameriere, R. Is the third molar maturity index (I3M) useful for a genetic isolate population? Study of a Sardinian sample of children and young adults. Int. J. Legal Med. 132, 1787–1794 (2018).
Cavrić, J. et al. Third molar maturity index (I3M) for assessing age of majority in a black African population in Botswana. Int. J. Legal Med. 130, 1109–1120 (2016).
Dardouri, A. A. K., Cameriere, R., De Luca, S. & Vanin, S. Third molar maturity index by measurements of open apices in a Libyan sample of living subjects. Forensic Sci. Int. 267, 230 e1-230.e6 (2016).
AlQahtani, S., Kawthar, A., AlAraik, A. & AlShalan, A. Third molar cut-off value in assessing the legal age of 18 in Saudi population. Forensic Sci. Int. 272, 64–67 (2017).
El-Bakary, A. A., El-Azab, S. M., Abou El Atta, H. M., Palacio, L. A. V. & Cameriere, R. Accuracy of the cutoff value of the third molar maturity index: an Egyptian study. Egypt. J. Forensic Sci. 9, 52 (2019).
Balla, S. B. et al. Validation of third molar maturity index (I3M) for discrimination of juvenile/adult status in South Indian population. J. Forensic Leg. Med. 49, 2–7 (2017).
Sharma, P., Wadhwan, V., Ravi Prakash, S., Aggarwal, P. & Sharma, N. Assessment of age of majority by measurement of open apices of the third molars using Cameriere′s third molar maturity index. J. Forensic Dent. Sci. 9, 96 (2017).
Kumagai, A. et al. Accuracy of the third molar index cut-off value for estimating 18 years of age: validation in a Japanese samples. Leg. Med. 38, 5–9 (2019).
Jiménez, L. G. et al. Validation of the third molar maturity index (I3M): study of a Dominican Republic sample. J. Forensic Odontostomatol. 37, 27–33 (2019).
Deitos, A. R. et al. Age estimation among Brazilians: Younger or older than 18?. J. Forensic Leg. Med. 33, 111–115 (2015).
De Luca, S. et al. Accuracy of cut-off value by measurement of third molar index: study of a Colombian sample. Forensic Sci. Int. 261(160), e1-160.e5 (2016).
Quispe Lizarbe, R. J., Solís Adrianzén, C., Quezada-Márquez, M. M., Galić, I. & Cameriere, R. Demirjian’s stages and Cameriere’s third molar maturity index to estimate legal adult age in Peruvian population. Leg. Med. 25, 59–65 (2017).
Khare, P. et al. Validation of the third molar maturity index cut-off value of <0.08 for indicating legal age of 18 years in Eastern Chinese region. Leg. Med. 42, 101645 (2020).
Cameriere, R. et al. Assessment of second (I2M) and third (I3M) molar indices for establishing 14 and 16 legal ages and validation of the Cameriere’s I3M cut-off for 18 years old in Chilean population. Forensic Sci. Int. 285(205), e1-205.e5 (2018).
Franklin, D. et al. Accuracy of a cut-off value based on the third molar index: validation in an Australian population. Forensic Sci. Int. 266(575), e1-575.e6 (2016).
Pereira, L., Prata, M. J. & Amorim, A. Diversity of mtDNA lineages in Portugal: Not a genetic edge of European variation. Ann. Hum. Genet. 64, 491–506 (2000).
Pimenta, J. et al. Spatially explicit analysis reveals complex human genetic gradients in the Iberian Peninsula. Sci. Rep. 9, 1–9 (2019).
Collins, G. S. et al. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): explanation and elaboration. Ann. Intern. Med. 162, W1–W73 (2015).
Santiago, B. M., Almeida, L., Cavalcanti, Y. W., Magno, M. B. & Maia, L. C. Accuracy of the third molar maturity index in assessing the legal age of 18 years: a systematic review and meta-analysis. Int. J. Legal Med. 132, 1167–1184 (2018).
Landis, J. R. & Koch, G. G. The measurement of observer agreement for categorical data. Biometrics 33, 159 (1977).
Glas, A. S., Lijmer, J. G., Prins, M. H., Bonsel, G. J. & Bossuyt, P. M. M. The diagnostic odds ratio: a single indicator of test performance. J. Clin. Epidemiol. 56, 1129–1135 (2003).
Galić, I. et al. Dental age estimation on Bosnian–Herzegovinian children aged 6–14 years: evaluation of Chaillet’s international maturity standards. J. Forensic Leg. Med. 20, 40–45 (2013).
Tomás, L. F., Mónico, L. S. M., Tomás, I., Varela-Patiño, P. & Martin-Biedma, B. The accuracy of estimating chronological age from Demirjian and Nolla methods in a Portuguese and Spanish sample. BMC Oral Health 14, 1–12 (2014).
Caldas, I. M. et al. Chronological age estimation based on third molar development in a Portuguese population. Int. J. Legal Med. 125, 235–243 (2011).
Cameriere, R., Cunha, E., Sassaroli, E., Nuzzolese, E. & Ferrante, L. Age estimation by pulp/tooth area ratio in canines: study of a Portuguese sample to test Cameriere’s method. Forensic Sci. Int. 193(128), e1-128.e6 (2009).
Anastácio, A. C., Serras, C., Vargas Sousa de Santos, R. F. & Palmela Pereira, C. Validation of Cameriere’s medical-legal age estimation method using seconds premolars in a Portuguese population. J. Forensic Leg. Med. 60, 30–34 (2018).
Pavlović, S., Palmela Pereira, C. & Vargas Sousa de Santos, R. F. Age estimation in Portuguese population: the application of the London atlas of tooth development and eruption. Forensic Sci. Int. 272, 97–103 (2017).
Pereira, C. P., Caldas, R. & Pestana, D. Legal medical age estimation in Portuguese adult cadavers: evaluation of the accuracy of forensic dental invasive and non-invasive methods. J. Forensic Sci. Criminol. 1, 1–6 (2013).
Antunovic, M. et al. The third molars for indicating legal adult age in Montenegro. Leg. Med. 33, 55–61 (2018).
Veldhuis, J. D., Roemmich, J. N. & Rogol, A. D. Gender and sexual maturation-dependent contrasts in the neuroregulation of growth hormone secretion in prepubertal and late adolescent males and females: a general clinical research center-based study. J. Clin. Endocrinol. Metab. 85, 2385–2394 (2000).
Author information
Authors and Affiliations
Contributions
Conceptualization, V.M, J.B and R.C.; methodology, J.N.; validation, J.B., V.M. and L.P.; formal analysis, L.P.; investigation, J.N.; resources, A.D. and J.J.M.; writing—original draft preparation, J.N.; writing—review and editing, J.J.M., N.A.F., A.Q. and R.C.; supervision, J.J.M, A.D, N.A.F and A.Q.; project administration, J.J.M, A.D. and R.C. . All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Albernaz Neves, J., Antunes-Ferreira, N., Machado, V. et al. Validation of the Third Molar Maturation Index (I3M) to assess the legal adult age in the Portuguese population. Sci Rep 10, 18466 (2020). https://doi.org/10.1038/s41598-020-75324-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-75324-x
This article is cited by
-
Third molar maturity index (I3M) assessment according to different geographical zones: a large multi-ethnic study sample
International Journal of Legal Medicine (2023)
-
Demirjian and Cameriere methods for age estimation in a Spanish sample of 1386 living subjects
Scientific Reports (2022)
-
Diagnostic accuracy of the third molar maturity index (I3M) to assess the age of legal majority in Northern Brazil—population-specific cut-off values
International Journal of Legal Medicine (2022)
-
Comparison of the third molar maturity index (I3M) between left and right lower third molars to assess the age of majority: a multi-ethnic study sample
International Journal of Legal Medicine (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
