
Abstract
The objective of this study was to investigate associations between education in early life and cognitive impairment in later life in Colombia. Participants were community-dwelling adults aged 60 years or older from the National Study of Health, Wellbeing and Ageing. Trained interviewers administered a shorter version of the mini-mental state examination. Cognitive impairment was defined as the lowest tertile in the main analysis and as a score of 12 or less out of 19 in the sensitivity analysis. Logistic regression models were adjusted for education, other early life characteristics, and later life characteristics. The prevalence of cognitive impairment was 17.93% in the main analysis (n = 16,505). Compared with participants with no education, the fully adjusted odds ratio for cognitive impairment was 0.57 (95% confidence interval: 0.52, 0.63) in those with some primary education and 0.29 (95% confidence interval: 0.25, 0.34) in those with some secondary education or more. The population attributable fraction for education suggests that at least 10% of cases of cognitive impairment would be eliminated if all children received an education. Similar results were observed in the sensitivity analysis (n = 20,174). This study suggests that education in early life markedly reduces the probability of cognitive impairment in late life in Colombia.
Similar content being viewed by others


Introduction
The global burden of disease attributable to mental disorders is rising to such an extent that poor mental health is regarded as a threat to sustainable development1. Mental health is a fundamental human right for all people, yet the burden of mental and substance use disorders is high in young people and the burden of Alzheimer’s disease and other dementias is high in older people1,2. In the Lancet Commission on global mental health and sustainable development, it is proposed that mental health in adults be understood from a life course perspective, with education in early life playing an important role in building cognitive reserve and reducing the risk of dementia in later life1. It is plausible that education reduces the risk of mild cognitive impairment and dementia3,4; however, more research is required to understand the association between education in early life and mild cognitive impairment in later life in Colombia and elsewhere in Latin America5,6. Inverse associations between education and cognitive impairment have been observed in older adults in Bogotá and five other cities in Colombia7,8,9; however, these analyses were not adjusted for early life characteristics or later life characteristics that may be associated with mental health such as nutrition, physical activity and socioeconomic status1,6,10,11,12. The studies in Bogotá and elsewhere in Colombia included between 1235 and 2000 participants7,8,9 and were too small to estimate the population attributable fraction for education, which is the proportion of cases of cognitive impairment that would be eliminated if all children received an education13. The National Survey of Health, Wellbeing and Ageing in Colombia (SABE Colombia, according to its initials in Spanish) is a nationwide study of adults older than 60 years of age14. The main objective of the present study is to investigate whether education in early life reduces the probability of cognitive impairment in participants in SABE independent of a range of early life and later life characteristics that may be associated with mental health. The secondary objective is to estimate the proportion of cases of cognitive impairment that are attributable to education.
Methods
This study was conducted in accordance with the STROBE Statement and includes the items that should be included in reports of observational studies15.
Participants
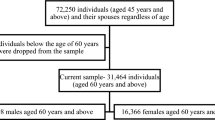
The National Survey of Health, Wellbeing and Ageing in Colombia is described in detail elsewhere14. Briefly, the target population was all adults aged 60 years or older living in households. Participants were selected using a multistage area probability sampling design and there were four selection stages: municipalities, blocks, housing units, and households. The response rate was around 62% in urban areas, around 77% in rural areas, and around 70% overall14. Data were collected across all departments (that is, states) and the final sample was deemed to be representative of the population of older adults living in households in Colombia14. Standard operating procedures were written for all procedures in the protocol and a study manual was written to guide fieldwork. Research and field staff were trained in all aspects of data collection and the core research staff trained the interviewers using role-playing14. The trained interviewers conducted face-to-face interviews in the participant’s home between April and September 201514. Volunteers completed the shorter version of the Folstein Mini-Mental State Examination (MMSE) described below and were invited to participate in the interview if they had a score of 13 or more14. Otherwise, a friend or family member was invited to complete the interview on behalf of the participant. Such a proxy obtained a score of 13 or more and completed the interview in 17.5% of cases14. Institutional review boards of Universidad de Caldas and Universidad del Valle approved the study and all participants gave written informed consent.
Dependent variable
The dependent variable was cognitive impairment. The versions of the MMSE used in Latin America and the Caribbean are shorter than the original version in an attempt to reduce the low literacy bias16. The shorter version of the MMSE used in SABE Colombia has six questions and participants were asked: to state the date and the day of week (4 points); to repeat and remember three words (3 points); to state in reverse order the numbers 1, 3, 5, 7, 9 (5 points); to take a piece of paper in their right hand, fold it in half using both hands, and put it on their lap (3 points); to reiterate the three words given earlier (3 points); and, to copy a drawing of two overlapping circles (1 point). Many English versions and several Spanish versions of the MMSE have been used to screen for mild cognitive impairment in older adults17, with sensitivity of 45% (95% confidence interval (CI): 39, 52) and specificity of 80% (95% CI: 75, 84) in the good quality studies17,18. Sensitivity and specificity may be higher when lower thresholds are used to screen for mild cognitive impairment in Spanish speaking populations with lower levels of education19,20. A score of 12 or less out of 19 was used to screen for mild cognitive impairment in SABE Colombia14. The shorter version of the MMSE used in SABE Colombia has been validated in a study of 1,301 adults aged 60 years or older living in households in Chile21. The prevalence of mild cognitive impairment was 10.7% using the threshold of 12 or less out of 19 in the shorter version of the MMSE and 8.1% using the threshold of 6 or more out of 33 in the criterion measure21, which was the Short Portable Mental Status Questionnaire22.
Independent variables
The trained interviewers followed a questionnaire and asked about age, sex, education, the economic situation of the family during childhood, self-rated health during childhood, current income, civil status, cigarette smoking, alcohol drinking, self-rated nutritional status, and physical activity. Participants were asked about the highest level of education they had achieved, and three groups were created: no education; some primary education; and, some secondary education or more. Interviewees were asked to state whether the economic situation of their family during their first 15 years of life was bad, normal or good. Interviewees were asked to state whether their health during their first 15 years of life was bad, normal or good. Participants were asked about their current individual income according to multiples of the minimum wage. Participants were asked about their current civil status, and two groups were created: not married or with partner; and, married or with partner. Participants were asked about cigarette smoking, and two groups were created: never smoker; and, current or ex-smoker. Participants were asked about alcohol drinking in the last month, and two groups were created: non-drinker; and, drinker. Interviewees were asked to rate their current state of nutrition as serious malnutrition, moderate malnutrition, or good nutrition. Participants were categorized as physically active if they reported taking part in sport or exercise at least three times per week or if they reported walking between 9 and 20 blocks (1.6 km) at least three times per week. The trained interviewers also measured height. The proxy was not asked about the economic situation of the family during childhood, self-rated health during childhood, or self-rated nutritional status.
Statistical analysis
All analyses were performed using Stata MP version 15.1 for Mac (StataCorp, Texas, USA). Logistic regression was used to investigate associations between education and cognitive impairment. In other studies, many thresholds have been used to screen for mild cognitive impairment17. In the present study, the threshold for mild cognitive impairment was the lowest tertile of the shorter version of the MMSE in the main analysis and a score of 12 or less in the sensitivity analysis. Logistic regression models were adjusted for age, sex, height quintile, education, economic situation of the family during childhood, self-rated health during childhood, current individual income, civil status, cigarette smoking, alcohol drinking, self-related nutritional status, and physical activity. Age was modelled as a continuous variable. All other covariates were modelled as categorical variables. The margins and atmeans commands in Stata were used to investigate the probability of cognitive impairment according to education level, with the covariates fixed at their means. The punaf command in Stata was used to estimate the population attributable fraction for education, adjusting for the covariates13.
Results
There were 23,694 participants in SABE; 16,505 were included in the main analysis and 20,174 were included in the sensitivity analysis in the present study. Table S1 in the online supplement shows selected participants’ characteristics in SABE and in the sub-samples. For example, the score on the shorter version of the MMSE was 14.9 ± 3.9 in SABE (mean ± SD), 16.6 ± 1.9 in the main analysis (p < 0.001 vs. SABE), and 15.4 ± 3.5 in the sensitivity analysis (p < 0.001 vs. SABE); Age was 70.8 ± 8.2 years in SABE, 68.9 ± 6.9 years in the main analysis (p < 0.0.01 vs. SABE), and 70.0 ± 7.7 years in the sensitivity analysis (p < 0.001 vs. SABE); And, the proportion of males was 42.68% in SABE, 45.27% in the main analysis (p < 0.001 vs. SABE), and 44.18% in the sensitivity analysis (p < 0.001 vs. SABE). The proportion of participants who reported some primary education was 57.04% in SABE, 59.02% in the main analysis (p < 0.001 vs. SABE), and 57.47% in the sensitivity analysis (p = 0.22 vs. SABE). The number of years of education was 3.59 ± 3.82 in SABE, 4.07 ± 4.00 in the main analysis (p < 0.001 vs. SABE), and 3.68 ± 3.85 in the sensitivity analysis (p < 0.05 vs. SABE).
Table 1 shows the score on the shorter version of the MMSE, age, proportion of males, level of education and all other variables in the sub-samples in the present study. The economic situation of the family during childhood was “bad” in 16.85% of participants, self-rated health during childhood was “good” in 89.7% of participants, and nutritional status was “good” in 72.28% of participants in the main analysis. These variables were not included in the sensitivity analysis because the proxy interviewee was not asked such questions. Current income was less than minimum wage in 55.64% of participants in the main analysis and 57.60% of participants in the sensitivity analysis. The proportion of participants married or with partner was 57.60% in the main analysis and 54.93% in the sensitivity analysis. The proportion of current or ex-smokers was 52.61% in the main analysis and 52.60% in the sensitivity analysis. Some 14% of participants in the main analysis and 12.74% of participants in the sensitivity analysis reported drinking alcohol. More than 50% of the participants in each of the sub-samples reported being physically active. Table S2 and Table S3 in the online supplement show participants’ characteristics in the sub-samples according to education levels. Compared with participants with no education, the score on the shorter version of the MMSE was higher and age was lower in those with some primary or some secondary education in both the main analysis and the sensitivity analysis. There were favourable differences in early life characteristics according to education level in the main analysis. And, there were favourable differences in later life characteristics according to education level in both the main analysis and the sensitivity analysis. For example, the proportion of physically active individuals in the main analysis was 55.30% in those with no education, 57.75% in those with some primary education (p < 0.001 vs. those with no education), and 66.88% in those with some secondary education or more (p < 0.001 vs. those with no education and those with some primary education).
The prevalence of cognitive impairment was 17.93% in the main analysis, where the threshold for mild cognitive impairment was the lowest tertile of the shorter version of the MMSE. Table 2 shows the probability of cognitive impairment in the 16,505 older adults in the main analysis. The fully adjusted odds ratio (95% confidence interval) was 1.03 (1.03, 1.04) for age and 1.06 (0.93, 1.20) for female sex. Compared with participants with no education, the fully adjusted odds ratio for cognitive impairment was 0.57 (0.52, 0.63) in those with some primary education and 0.29 (0.25, 0.34) in those with some secondary education or more. Greater income, good nutrition and physical activity were also associated with lower probability of cognitive impairment. The prevalence of cognitive impairment was 16.16% in the sensitivity analysis, where the threshold for mild cognitive impairment was a score of 12 or less on the shorter version of the MMSE. Table 2 also shows the probability of cognitive impairment in the 20,174 older adults in the sensitivity analysis. The fully adjusted odds ratio was 1.09 (1.09, 1.10) for age and 0.82 (0.72, 0.93) for female sex. Compared with participants with no education, the fully adjusted odds ratio for cognitive impairment was 0.33 (0.30, 0.36) in those with some primary education and 0.12 (0.10, 0.14) in those with some secondary education or more. Greater income, being married or with partner, being a smoker or ex-smoker, drinking alcohol, and being physically active were also associated with lower probability of cognitive impairment.
Figure 1 shows the probability of cognitive impairment according to education level, with the covariates fixed at their means. In the main analysis, the probability of cognitive impairment was 0.27 (0.25, 0.29) in those with no education, 0.17 (0.17, 0.18) in those with some primary education, and 0.10 (0.09, 0.11) in those with some secondary education or more. In the sensitivity analysis, the probability of cognitive impairment was 0.26 (0.24, 0.27) in those with no education, 0.10 (0.10, 0.11) in those with some primary education, and 0.04 (0.03, 0.05) in those with some secondary education or more.

The probability of cognitive impairment according to education level, with the covariates fixed at their means. 0 is no education. 1 is some primary education. 2 is some secondary education or more. Sample size was 16,505 in the main analysis and cognitive impairment was defined as the lowest tertile of the shorter version of the mini-mental state examination. Sample size was 20,174 in the sensitivity analysis and cognitive impairment was defined as a score of 12 or less out of 19.
In the main analysis, the population attributable fraction for education was estimated while adjusting for age, sex, height, education, economic situation of the family during childhood, self-rated health during childhood, current individual income, civil status, cigarette smoking, alcohol drinking, self-related nutritional status, and physical activity (n = 16,505). Theoretically, 10% (9, 12) of cases of cognitive impairment would be eliminated if all children received an education (i.e., some primary education or some secondary education or more). Some 43% (37, 48) of cases would be eliminated if all children received an education that was secondary education or more. In the sensitivity analysis, the population attributable fraction was estimated while adjusting for age, sex, height, education, current individual income, civil status, cigarette smoking, alcohol drinking, and physical activity (n = 20,174). Theoretically, 25% (23, 27) of cases would be eliminated if all children received an education and 65% (59, 70) of cases would be eliminated if that education was secondary education or more.
Discussion
The main objective of this study was to investigate whether education in early life reduced the probability of cognitive impairment in older adults in Colombia. We found that, compared with participants with no education, the probability of cognitive impairment was lower in those with some primary education and lower still in those with some secondary education or more. Any education markedly reduced the probability of cognitive impairment, whether cognitive impairment was defined as the lowest tertile of the mental state examination or as a score of 12 or less. Magnetic resonance imaging studies suggest that it is plausible that education reduces the risk of dementia because greater education in early life is associated with greater grey matter volume in middle age3 and greater lifespan mental activity is associated with lower hippocampal atrophy in older age4. The secondary objective of this study was to estimate the proportion of cases of cognitive impairment that were attributable to education. We found that at least 10% of cases of cognitive impairment would be eliminated if all children received an education.
To the best of our knowledge, this is the largest and most robust study of education and cognitive impairment in older adults in Colombia7,8,9. Inverse associations between education and cognitive impairment have been reported in 1,611 older adults in five cities of Colombia7, in 1,235 older adults in the city of Bogotá in Colombia8, and in 2,000 older adults in the city of Bogotá in Colombia9; However, these analyses were only adjusted for age and sex7,9, and for age, sex and “comorbidities”8. The present study is also one of the largest studies of its kind in Latin America6,23,24,25,26,27. The 10/66 Dementia Research Group includes data from “representative populations” from Cuba, Dominican Republic, Mexico, Peru, Puerto Rico and Venezuela (the Latin American sample) and from China and India28. The data from the 12,865 older adults in the Latin American sample suggest that the prevalence of low education is around 70% and the population attributable fraction for dementia is around 11%6. In the present study, the prevalence of low education in Colombia was around 75–80% and the population attributable fraction for cognitive impairment was around 10–25%. These studies suggest that there should be more emphasis on education in early life in subsequent iterations of the mental health act of Colombia as part of a policy to improve mental health across the life course29,30. While it is plausible that education reduces the risk of dementia3,4, it is also possible that people with more education in early life adopt lifestyles that are conducive to brain health in later life1. Indeed, compared with participants in the present study with no education, the proportion of smokers was lower in those with some primary education and lower still in those with some secondary education or more. And, compared with participants with no education, the proportion of physically active individuals was higher in those with some primary education and higher still in those with some secondary education or more.
The present analysis was adjusted for a range of covariates that may be associated with mental health1,6,10,11,12. The observed associations were in the expected directions, except cigarette smoking6. More research is needed to understand the association between alcohol and dementia31. There is growing evidence that cardiovascular disease risk factors deteriorate many years before the onset of dementia and that cardiovascular disease risk factors are not associated with cognitive decline in older adults32,33,34. In the present sample, 2088 participants reported a diagnosis of heart disease and the fully adjusted odds ratio for cognitive impairment was 0.97 (0.86, 1.10). In the present sample, body mass index was measured in 20,124 participants, and body mass index was not associated with cognitive impairment in the fully adjusted model (data not shown). In the present sample, blood samples were obtained from 3530 participants after an overnight fast, and total cholesterol concentration, HDL-cholesterol concentration, and LDL-cholesterol concentration were not associated with cognitive impairment in the fully adjusted model (data not shown).
This study has some limitations. Longitudinal studies are needed to clarify the associations between early life characteristics, later life characteristics, and cognitive impairment; however, it is reasonable to assume that education preceded cognitive impairment even in this cross-sectional study. The thresholds used in screening tests of cognitive impairment are often arbitrary17; however, we used a sensitivity analysis to demonstrate the robustness of the assessment. The shorter version of the MMSE used in SABE Colombia is a valid screening tool21, but it is not a clinical diagnosis of cognitive impairment. Some variables were self-reported and are subject to biases. There was no measure of the genetic factors that may play a role in determining individual risk of dementia35. There was no measure of quality of education in the present study; however, it is encouraging that any amount of education markedly reduced the probability of cognitive impairment.
Conclusion
Little was known about the association between education in early life and cognitive impairment in later life in Colombia because there were no nationwide surveys, only small studies in different cities. The National Survey of Health, Wellbeing and Ageing in Colombia is a representative study of 23,694 older adults. To the best of our knowledge, the present study is the largest report of an inverse association between education and cognitive impairment in older adults in Colombia and elsewhere in Latin America & the Caribbean. There should be more emphasis on education in early life in subsequent iterations of the mental health act of Colombia as part of a policy to improve mental health across the life course.
References
Patel, V. et al. The Lancet Commission on global mental health and sustainable development. Lancet 392, 1553–1598 (2018).
2Institute for Health Metrics and Evaluation. GBD Compare | Viz Hub. https://vizhub.healthdata.org/gbd-compare/ (2019).
Gazzina, S. et al. Education modulates brain maintenance in presymptomatic frontotemporal dementia. J. Neurol. Neurosurg. Psychiatry. 90, 1124–1130 (2019).
Valenzuela, M. J., Sachdev, P., Wen, W., Chen, X. & Brodaty, H. Lifespan mental activity predicts diminished rate of hippocampal atrophy. PLoS ONE 3, e2598 (2008).
5Patterson, C. The World Alzheimer Report 2018, The state of the art of dementia research: New frontiers. https://www.alz.co.uk/research/world-report-2018 (2018).
Mukadam, N., Sommerlad, A., Huntley, J. & Livingston, G. Population attributable fractions for risk factors for dementia in low-income and middle-income countries: an analysis using cross-sectional survey data. Lancet Glob. Health. 7, e596–e603 (2019).
Rosselli, D. et al. The Mini-Mental State Examination as a selected diagnostic test for dementia: a Colombian population study. GENECO. Rev Neurol. 30, 428–432 (2000).
Pedraza, O. L. et al. Mild cognitive impairment (MCI) and dementia in a sample of adults in the city of Bogota. Dement Neuropsychol. 11, 262–269 (2017).
9Borda, M. G. et al. Educational level and its association with the domains of the Montreal Cognitive Assessment Test. Aging Ment Health. 1–7 (2018).
Engeroff, T., Ingmann, T. & Banzer, W. Physical activity throughout the adult life span and domain-specific cognitive function in old age: a systematic review of cross-sectional and longitudinal data. Sports Med. 48, 1405–1436 (2018).
Kobayashi, L. C. et al. Education modifies the relationship between height and cognitive function in a cross-sectional population-based study of older adults in Rural South Africa. Eur. J. Epidemiol. 34, 131–139 (2019).
Sommerlad, A., Ruegger, J., Singh-Manoux, A., Lewis, G. & Livingston, G. Marriage and risk of dementia: systematic review and meta-analysis of observational studies. J. Neurol. Neurosurg. Psychiatry. 89, 231–238 (2018).
Newson, R. B. Attributable and unattributable risks and fractions and other scenario comparisons. Stata J. 13, 672–698 (2013).
Gomez, F., Corchuelo, J., Curcio, C. L., Calzada, M. T. & Mendez, F. SABE Colombia: survey on health, well-being, and aging in Colombia-study design and protocol. Curr. Gerontol. Geriatr. Res. 2016, 7910205 (2016).
15STROBE. STROBE Statement. https://www.strobe-statement.org.
Pelaez, M. et al. Inter-university Consortium for Political and Social Research [distributor], Ann Arbor (MI, USA, 2006).
17Lin, J. S. et al. Screening for Cognitive Impairment in Older Adults: An Evidence Update for the U.S. Preventive Services Task Force. Evidence Report No. 107. AHRQ Publication No. 14-05198-EF-1. (Agency for Healthcare Research and Quality, 2013).
Saxton, J. et al. Computer assessment of mild cognitive impairment. Postgrad. Med. 121, 177–185 (2009).
Morales, J. M., Bermejo, F., Romero, M. & Del-Ser, T. Screening of dementia in community-dwelling elderly through informant report. Int. J. Geriatr. Psychiatry. 12, 808–816 (1997).
Cruz-Orduna, I. et al. Detecting MCI and dementia in primary care: effectiveness of the MMS, the FAQ and the IQCODE [corrected]. Fam. Pract. 29, 401–406 (2012).
21Organización Panamericana de la Salud. Salud, bienestar y envejecimiento en Santiago, Chile [Health, wellbeing and ageing in Santiago, Chile]. https://iris.paho.org/bitstream/handle/10665.2/741/9275316090.pdf?sequence=1 (2005).
Pfeiffer, E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 23, 433–441 (1975).
Johansson, L. et al. Associations between depression, depressive symptoms, and incidence of Dementia in Latin America: A 10/66 Dementia Research Group Study. J. Alzheimers Dis. 69, 433–441 (2019).
Ashby-Mitchell, K., Jagger, C., Fouweather, T. & Anstey, K. J. Life expectancy with and without cognitive impairment in seven Latin American and Caribbean countries. PLoS ONE 10, e0121867 (2015).
Maurer, J. Education and male-female differences in later-life cognition: international evidence from Latin America and the Caribbean. Demography 48, 915–930 (2011).
Nguyen, C. T., Couture, M. C., Alvarado, B. E. & Zunzunegui, M. V. Life course socioeconomic disadvantage and cognitive function among the elderly population of seven capitals in Latin America and the Caribbean. J. Aging Health. 20, 347–362 (2008).
Zeki Al Hazzouri, A., Haan, M. N., Galea, S. & Aiello, A. E. (2011) Life-course exposure to early socioeconomic environment, education in relation to late-life cognitive function among older Mexicans and Mexican Americans. J. Aging Health. 23, 1027–1049 (2011).
Prince, M. et al. The protocols for the 10/66 dementia research group population-based research programme. BMC Public Health. 7, 165 (2007).
29República de Colombia - Gobierno Nacional. Ley de Salud Mental (Ley 1616) [Mental Health Act (Law 1616)]. https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/ley-1616-del-21-de-enero-2013.pdf (2013).
30Gobierno de Colombia. Estrategia para la Promoción de la Salud Mental en Colombia (CONPES 3992) [Strategy for the Promotion of Mental Health in Colombia (CONPES 3992)]. https://www.dnp.gov.co/CONPES/documentos-conpes/Paginas/documentos-conpes.aspx (2020).
Livingston, G. et al. Dementia prevention, intervention, and care. Lancet 390, 2673–2734 (2017).
Peters, R., Peters, J., Booth, A. & Anstey, K. J. Trajectory of blood pressure, body mass index, cholesterol and incident dementia: systematic review. Br. J. Psychiatry. 216, 16–28 (2020).
Fitzpatrick, A. L. et al. Midlife and late-life obesity and the risk of dementia: cardiovascular health study. Arch. Neurol. 66, 336–342 (2009).
Armstrong, N. M., Bangen, K. J., Au, R. & Gross, A. L. Associations between midlife (but not late-life) elevated coronary heart disease risk and lower cognitive performance: results from the Framingham offspring study. Am. J. Epidemiol. 188, 2175–2187 (2019).
Lourida, I. et al. Association of lifestyle and genetic risk with incidence of dementia. JAMA https://doi.org/10.1001/jama.2019.9879 (2019).
Author information
Authors and Affiliations
Contributions
G.O.D conceived the study, analysed and interpreted the data, and approved the final submission. M.H. helped to design the study, helped to interpret the data, and approved the final submission. O.L.S. helped to interpret the data and approved the final submission. PH obtained the data and approved the final submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
O’Donovan, G., Hamer, M., Sarmiento, O.L. et al. Education in early life markedly reduces the probability of cognitive impairment in later life in Colombia. Sci Rep 10, 17685 (2020). https://doi.org/10.1038/s41598-020-74822-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-74822-2
This article is cited by
-
The impacts of social determinants of health and cardiometabolic factors on cognitive and functional aging in Colombian underserved populations
GeroScience (2023)
-
The burden of mild cognitive impairment attributable to physical inactivity in Colombia
European Review of Aging and Physical Activity (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
