
Abstract
Olanzapine-induced dyslipidemia significantly increases the risk of cardiovascular disease in patients with schizophrenia. However, the clinical features of olanzapine-induced dyslipidemia remain hitherto unclear because of inconsistencies in the literature. This meta-analysis thus investigated the effects of olanzapine treatment on lipid profiles among patients with schizophrenia. Studies of the effects of olanzapine on lipids were obtained through the PubMed, Web of science, The Cochrane Library and Embase databases (up to January 1, 2020). Twenty-one studies and 1790 schizophrenia patients who received olanzapine therapy were included in our analysis. An olanzapine-induced increase was observed in plasma triglyceride (TG), total cholesterol (TC), and low-density lipoprotein cholesterol (LDL-C) levels in patients with schizophrenia (all P < 0.05). Moreover, the time points analyzed included the following: baseline, 4 weeks, 6 weeks, 8 weeks, 12 weeks, and ≥ 24 weeks (data of ≥ 24 weeks were integrated). The significant elevation of TG, TC, and LDL-C was observed in patients with schizophrenia already by 4 weeks of olanzapine therapy (all P < 0.05), with no obvious changes observed in high-density lipoprotein cholesterol (HDL-C) (P > 0.05). In conclusion, olanzapine-induced dyslipidemia, characterized by increased TG, TC, and LDL-C levels, was observed in patients with schizophrenia already by 4 weeks of olanzapine treatment.
Similar content being viewed by others
Introduction
Schizophrenia is a severe neuropsychiatric illness that threatens approximately 1% of the global population1. High morbidity and mortality caused by dyslipidemia concomitant with cardiovascular disease (CVD) have been documented among patients with schizophrenia2,3. It has been shown that olanzapine, a second-generation antipsychotic drug, is a major contributor to dyslipidemia among patients with schizophrenia4,5,6. However, the clinical features of olanzapine-induced dyslipidemia remain unclear because of inconsistent data among studies. Although some clinical randomized trials have reported increased serum triglyceride (TG) levels in schizophrenic patients on olanzapine therapy, the changes in total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) remain a matter of dispute7,8,9,10,11.
Dyslipidemia is a well-established risk factor in the pathogenesis of CVD, including coronary heart disease (CAD), and acute coronary syndrome12. In fact, it is thought to account for more than half of the worldwide cases of CAD. Importantly, high plasma TG and LDL-C levels and/or low serum HDL-C levels have been implicated in the pathophysiology of CVD13. Accordingly, understanding the characteristics of olanzapine-induced dyslipidemia is critical to the assessment and control of cardiovascular risk in schizophrenic patients. We therefore conducted a systematic review and meta-analysis of published literature to determine olanzapine-associated lipid profiles in patients with schizophrenia. In addition, we further analyzed the influence of clinical characteristics and treatment duration on olanzapine-induced dyslipidemia in patients with schizophrenia.
Methods
Search strategy and study identification
This systematic literature review and meta-analysis was strictly subject to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (see PRISMA Checklist in Supplementary table S1)14. We performed a comprehensive literature search in the following electronic databases to obtain eligible studies published by January 1, 2020: PubMed, Web of science, The Cochrane Library and Embase. The search terms were [‘schizophrenia’] AND [‘olanzapine’] AND [‘dyslipidemias’ OR ‘triglycerides’ OR ‘Cholesterol’ OR ‘Cholesterol, LDL’ OR ‘Cholesterol, HDL’]. We also adopted Medical Subject Headings (MeSH) and related keywords in our analysis to increase the number of studies in our search. Moreover, a manual search of reference lists was undertaken for additional relevant articles. English was the only standard language that was applied in the search strategy. If relevant data of published studies were not available, we contacted the corresponding author(s) to obtain them via email.
Study selection
The inclusion and exclusion criteria of the obtained reports are described in reference to population, interventions, outcomes, and study design as follows.
Population
People with schizophrenia diagnosed according to the criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders—Fourth Edition (DSM-IV), the International Statistical Classification of Diseases and Related Health Problems—Tenth Revision (ICD-10), or the 3rd edition of the Chinese Classification of Mental Disorders (CCMD-3) (the diagnostic criteria commonly used in China). No limitations were defined by sex, race, or age. Women were excluded if they were planning to be pregnant or were undergoing pregnancy or lactation. Moreover, patients with chronic physical illness were also excluded, including those with atherosclerotic CVD, hepatic diseases, renal diseases, and diabetes.
Interventions
Only studies that administered olanzapine alone were considered. Moreover, all of the included studies were required to have provided detailed descriptions of the durations of administration. The dosage of olanzapine was further required to have been within the maximum dose range.
Outcomes
The mean and standard deviation (SD) of the plasma levels of TG, TC, LDL-C, and HDL-C at baseline and the end of olanzapine therapy. It's important to note that TG levels are susceptible to the quality of the meals slightly before bloodwork.
Study design
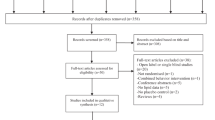
Randomized controlled clinical trials and cohort studies were included. Furthermore, other non-randomized controlled studies such as self-controlled studies concerning the effects of olanzapine on plasma lipids were also included. Indeed, not only schizophrenia itself may affect the metabolic state including blood lipid metabolism in patients, but the eating habits and exercise in each of individuals is quite different, hence, we conducted a single-arm meta-analysis rather than a pairwise meta-analysis of olanzapine against various control groups. We excluded studies that satisfied one of the following criteria: (1) non-clinical studies, such as animal, cell, genetic and drug metabolism studies; (2) unpublished papers, letters, case reports, reviews, and meta-analyses; (3) the full text not available; (4) the statistical methods were misapplied. A flow chart concerning the process of the identification, inclusion, and exclusion of studies is shown in Fig. 1.

Flowchart of included and excluded reports. This flowchart summarizes the process of document retrieval and selection according to the inclusion criteria.
Data extraction
Data from studies were entered in a pre-specified spreadsheet in Microsoft Excel 2019 and EndNote 8.1. The following details of patients were extracted from each of the included reports: (1) surname name of the first author and the year of publication; (2) institution and country of each study; (3) characteristics about the subjects, including mean age, body mass index (BMI), medication times, sample sizes of the olanzapine and control groups; (4) the plasma levels of TG, TC, LDL-C, and HDL-C at baseline and different time points of olanzapine treatment.
Quality assessment
The quality of each of the included studies was accessed and scored by two independent reviewers to determine the quality of participant selection, comparability, exposures, and outcomes. The methodological biases of the RCTs were judged according to the Cochrane criteria guidelines, and the researchers were required to make judgments of "yes", "no", and "unclear" for each evaluation item. Recommended by the Agency for Healthcare Research and Quality (AHRQ), the Newcastle–Ottawa Quality (NOS) Assessment Scale, was used to evaluate the quality of cohort studies15. We also integrated the methodological index for non-randomized studies (MINORS) in our investigation because of its suitability for evaluating the quality of self-controlled studies16. The MINORS is composed of 12 evaluation indices, each of which is awarded scores of 0–2 points: a score of 0 indicates unreported information; a score of 1, insufficiently reported information; and a score of 2, sufficiently reported information. Disagreements were discussed, and adjudication was resolved by a third reviewer.
Statistical analysis
The data pooled from the selected studies were divided into four groups on the basis of the main serum lipid components (TG, TC, LDL-C and HDL-C), and provided the data source for the primary results. Analysis of the relationship between olanzapine treatment duration and serum lipid changes was achieved from the integrated lipids data of different olanzapine intervention duration. Additionally, a potential source of heterogeneity in serum lipids can be the age of the patient. Indeed, numerous reports have concluded that as people age, their plasma lipid levels tend to also increase. Additionally, epidemiologic studies have shown that a greater proportion of the elderly population is dyslipidemic17. Hence, in order to avoid the confounding role of age in our assessment and determine the possible source of heterogeneity, we performed an age subgroup analysis as a function of time.
The effect size of the mean differences of TG, TC, LDL-C, and HDL-C between baseline and endpoint in schizophrenia patients was computed using weighted-mean difference (WMD). A forest plot using α = 0.05 to indicate significance was generated to estimate the WMD and its 95% CI. Heterogeneity of the included studies was tested with the Q-statistic and quantified using I2 = 100% × [(Q – degree of freedom)/Q]. An I2 of > 50% was considered to reflect significant statistical heterogeneity. The random-effects model using the inverse variance heterogeneity method was adopted with I2 > 50%18.
A sensitivity analysis was performed by excluding one study at a time to explore the sources of heterogeneity. Evidence of publication bias was assessed by a visual funnel plot and Egger’s regression asymmetry test. Subgroup analysis was performed to detect the underlying sources of heterogeneity. All analytic processes were conducted with Stata-SE 15.1 statistical software (STATA Corp, College Station, TX, USA).
Results
Search results and study characteristics
Our initial search yielded 1445 studies from the PubMed, Web of Science, The Cochrane Library and Embase databases. Of these studies, 1424 articles were excluded on account of the following: (1) duplicated literature, (2) non-experimental literature, (3) animal experiments, (4) unavailability of the full text, (5) unrelated to olanzapine or plasma lipid levels, (6) unrelated to schizophrenia, and (7) unavailability of the originally relevant data (Fig. 1). All included studies were published in English. Our analysis thus included 21 studies and 1790 schizophrenia patients in the olanzapine arm. We also included the randomized open-label trial by Kusumi et al.19 to compare the effect of olanzapine orally disintegrating tablet and oral standard tablet on body weight and lipid metabolism in patients with schizophrenia. Since both arms were treated with olanzapine, all patients were included in this meta-analysis. The main characteristics of these studies are listed in Tables 1 and 2.
Methodological quality of the included studies
We used the data extracted from the olanzapine arm (not included control arm) of 16 included RCTs. Our analysis, therefore, was primarily concerned with the bias resulting from the integrity of the lipid data at different time points and selective publication of lipid data inconsistent with the hypothesis. The only cohort study assessed medium quality according to NOS Assessment Scale, and most RCTs (94%) provided complete outcome data instead of selective data (Table 3). Moreover, four self-controlled studies provided sufficient information (Table 4). Thus, the quality of the included literature was generally high.
Primary outcomes
The random effect model pooled the WMD of lipid levels from the baseline to the termination of their respective study periods as follows: TG = 0.41 mmol/l (95% confidence interval [CI], 0.30 to 0.52; P < 0.001; I2 = 74.6%; n = 1569; 21 studies), TC = 0.37 mmol/l (95% CI, 0.19 to 0.55; P < 0.001; I2 = 85.4%; n = 1185; 18 studies), LDL-C = 0.14 mmol/l (95% CI, 0.04 to 0.24; P = 0.005; I2 = 49.6%; n = 1159; 16 studies). All the WMD of TG, TC, and LDL-C featured significant heterogeneity. However, no obvious changes were observed in HDL-C (WMD = – 0.02 mmol/l; Figs. 2, 3, 4, 5). Taken together, the analysis indicated that olanzapine-induced dyslipidemia is characterized by increases of TG, TC, and LDL-C and no changes in HDL-C.

Forest plot and meta-analysis of olanzapine's effects on TG. WMD weighted-mean difference; CI confidence interval.

Forest plot and meta-analysis of olanzapine's effects on TC. WMD weighted-mean difference; CI confidence interval.

Forest plot and meta-analysis of olanzapine's effects on LDL-C. WMD weighted-mean difference; CI confidence interval.

Forest plot and meta-analysis of olanzapine's effects on HDL-C. WMD weighted-mean difference; CI confidence interval.
Secondary outcomes-changes of lipid profiles depending on the duration of treatment
The effects of olanzapine intervention duration on lipid levels were further analyzed because the accumulation effect of the drug may influence the final detected serum lipid level. The time points analyzed included the following: baseline, 4 weeks, 6 weeks, 8 weeks, 12 weeks, and ≥ 24 weeks (data of ≥ 24 weeks were integrated).
The WMDs of plasma TG changes from baseline to the five end time points were as follows: 4 weeks = 0.57 mmol/l (95% CI, 0.28 to 0.87; I2 = 67.4%), 6 weeks = 0.36 mmol/l (95% CI, 0.18 to 0.54; I2 = 39.7%), 8 weeks = 0.48 mmol/l (95% CI, 0.30 to 0.66; I2 = 67.7%), 12 weeks = 0.55 mmol/l (95% CI, 0.09 to 1.00; I2 = 92.3%), and ≥ 24 weeks = 0.30 mmol/l (95% CI, 0.20 to 0.40; I2 = 0.0%). All WMDs of the above TG changes were significant (P < 0.05 for all) (Table 5), showing that olanzapine therapy will increase plasma TG levels in patients with schizophrenia after 4 weeks and that this effect will persist across the remaining period of medication.
The WMDs of TC changes at 4, 6, 8 and 12 weeks were 0.34 mmol/l (95% CI, 0.10 to 0.58; I2 = 31.3%), 0.36 mmol/l (95% CI, 0.19 to 0.54; I2 = 22.3%), 0.44 mmol/l (95% CI, 0.19 to 0.69; I2 = 73.1%), and 0.62 mmol/l (95% CI, 0.41 to 0.83; I2 = 0.0%), respectively. All WMDs at the four end time points mentioned were significant (P < 0.05 for all). Interestingly, no significant changes were found at ≥ 24 weeks (WMD = 0.20 mmol/l; 95% CI = – 0.04 to 0.44; P = 0.10; I2 = 66.2%) (Table 5).
For LDL-C, the significant WMDs were obtained at four end time points as follows: 4 weeks = 0.14 mmol/l (95% CI, 0.03 to 0.25; I2 = 1.8%), 6 weeks = 0.19 mmol/l (95% CI, 0.08 to 0.29; I2 = 0.0%), 8 weeks = 0.18 mmol/l (95% CI, 0.07 to 0.29; I2 = 8.1%), and 12 weeks = 0.39 mmol/l (95% CI, 0.21 to 0.56; I2 = 0.0%) (P < 0.05 for all). Interestingly, similar to the data concerning TC, no significant LDL-C changes were found at ≥ 24 weeks (WMD = – 0.02 mmol/l; 95% CI, – 0.17 to 0.13; P = 0.81; I2 = 31.0%) (Table 5).
As shown in Table 5, the WMDs of HDL-C at all end time points were as follows: 4 weeks = – 0.02 mmol/l (95% CI, – 0.09 to 0.05; I2 = 0.0%), 6 weeks = 0.01 mmol/l (95% CI, – 0.06 to 0.08; I2 = 31.5%), 8 weeks = – 0.03 mmol/l (95% CI, – 0.13 to 0.07; I2 = 61.5%), 12 weeks = – 0.00 mmol/l (95% CI, – 0.05 to 0.05; I2 = 0.0%), and ≥ 24 weeks = – 0.03 mmol/l (95% CI, – 0.06 to 0.00; I2 = 0.0%). Of note, no significant changes in HDL-C were found after olanzapine treatment (P > 0.05 for all).
Subgroup analysis according to age
Considering the potential heterogeneity among included studies, an age subgroup analysis was performed (Table 6). The age subgroup analysis was only conducted in groups with an I2 of ≥ 50%. Meta-analyses could not be conducted in subgroups for which data from only one study was available. The WMD of TG changes from baseline to 12 weeks among patients with schizophrenia (mean age < 40 years) was 0.30 mmol/l (95% CI, 0.16 to 0.45; I2 = 0.0%). For HDL-C, the WMD was 0.02 mmol/l (95% CI, – 0.05 to 0.09; I2 = 0.0%) in patients with schizophrenia (mean age < 40 years) that had undergone an 8-week olanzapine intervention. The groups including TG at 4 weeks, 8 weeks, TC at 8 weeks, and TC ≥ 24 weeks with an I2 that exceeded 50% after age subgroup analyses required further analysis (see “Sensitivity analysis and potential sources of heterogeneity”).
Our findings suggest that the age of the patients is an important characteristic in determining the effects of olanzapine on TG and HDL-C. However, we could not analyze the magnitude of the variations in serum lipids and therefore, could not establish a link between the magnitude of the change in serum lipids and the age of the patients from this meta-analysis.
Sensitivity analysis and potential sources of heterogeneity
A sensitivity analysis was required to identify the sources of heterogeneity in our findings. Our analysis revealed that the studies by Chen et al.20, Wu et al.21 and McDonnell et al.22 were the main causes of heterogeneity (Supplementary Figure S1, S2, S3 and S4) and their exclusion effectively removed or decreased the variations (TG at 4 weeks: I2 = 17.2%; TG at 8 weeks: I2 = 59.4%; TC at 8 weeks: I2 = 35.4%; TC ≥ 24 weeks: I2 = 20.5%). Notably, the stability of our results was substantiated by the consistency of the statistical significance obtained after their exclusion (TG at 4 weeks: P < 0.001; TG at 8 weeks: P < 0.001; TC at 8 weeks: P = 0.002). Finally, the P value of TC ≥ 24 weeks group changed to 0.005 (statistically significant) after the exclusion, revealing that the accuracy of the results in the study of McDonnell et al.22 was debatable.
Publication bias
Most studies were located within the 95% CIs of a symmetrical distribution (Fig. 6). In addition, P values for the Egger tests were > 0.05, indicating no significant publication bias.

Funnel plots illustrating the publication bias of the four groups of different lipid components. WMD weighted mean difference; se standard error.
Discussion
In this current meta-analysis of 21 studies on the effects of olanzapine on lipid profiles in patients with schizophrenia, we demonstrated that the clinical features of dyslipidemia were characterized by an elevation of TG, TC, and LDL-C, with no significant changes in HDL-C. Furthermore, we analyzed the effects of the duration of olanzapine treatment on lipid profiles in patients with schizophrenia, revealed that 4 weeks of olanzapine treatment resulted in abnormal serum lipid levels. Even if the duration of olanzapine-therapy was prolonged, the effect of olanzapine on modulating serum levels of lipid could persist synchronously.
Interestingly, following the exclusion of the findings by McDonnell et al.22, there was a significant increase in TC level in the TC ≥ 24 weeks group (P = 0.005). A review of the research revealed significant decreases in the mean fasting serum TC levels from baseline to end point22. The conclusion of McDonnell’s group might be debatable because the long-term diet control was not discussed in the study, and its design included an acute period of stabilization on oral olanzapine before random assignment to therapy22. Meanwhile, there were no significant changes in the LDL-C levels after 24-week treatment. We postulate that it might be due to the variations in the sample sizes, ethnicities, and clinical characteristics of the populations in the selected studies. Alternately, the return to baseline levels could have been caused by some form of tolerance to olanzapine. Moreover, the studies were found to have relatively significant heterogeneity (I2 ≥ 50% and P < 0.05) in TG, TC and LDL-C but not HDL-C (I2 = 36.3%, P = 0.058). The heterogeneity could partly be explained by the different age groups included as a decrease in heterogeneity was observed after age subgroup analyses. Other sources of heterogeneity could be the discordant measurements and results between different studies, resulting in impaired validity of the conclusions. Nevertheless, no publication bias of the literature was detected, further suggesting that the heterogeneity did not result from publication bias. To the best of our knowledge, previous meta-analyses mostly focused on lipid comparison between different antipsychotics, this is the first meta-analysis to investigate the correlation of olanzapine and dyslipidemia in patients with schizophrenia, especially the effect of olanzapine intervention duration on lipid metabolism. Our findings could contribute to the monitoring and management of dyslipidemia in patients with schizophrenia undergoing olanzapine treatment.
Currently, growing evidence suggests that olanzapine treatment can promote several cardio-metabolic disorders such as dyslipidemia in schizophrenic patients, contributing to markedly shorter longevities as compared to the general population23. In the first published cases of olanzapine-associated hypertriglyceridemia, Sheitman et al.24 followed nine patients on olanzapine for an average of 16 months and observed an increase in serum TG from the baseline mean of 170 mg/dl (range 25–200 mg/dl) to the mean of 240 mg/dl (range 135–369 mg/dl), with five patients sustaining > 50% increase in serum TG. Further research associated olanzapine with a roughly five-time increased risk of developing hyperlipidemia as compared with no antipsychotic exposure25. As the role of dyslipidemia in CVD development has been well-documented, the increased risk of CVD attributed to olanzapine-induced dyslipidemia is likewise clear12: with each 1 mmol/l increase in TG, the risk of CVD increases by ≈ 12% and 37% in men and women, respectively26. Furthermore, a meta-analysis of 90,056 individuals in 14 randomized trials showed that each 1 mmol/L drop of LDL-C reduces the risk of CVD by 23%27. The WMD of lipid levels from the baseline to endpoint were 0.41 mmol/l of TG, 0.37 mmol/l of TC, and 0.14 mmol/l of LDL-C, respectively. These figures stress the importance of managing olanzapine-induced dyslipidemia especially TG and LDL-C in patients with schizophrenia to the prevention of CVD in this population28. Besides, the fibrates and the statins are recommended to effectively control the TG and LDL-C levels, which may be also used to treat olanzapine-associated hypertriglyceridemia and reduce the plasma level of LDL-C. Therefore, it has been well-established that olanzapine treatment—specifically, olanzapine-induced dyslipidemia—contributes to high cardiovascular risk among patients with schizophrenia7,29.
Notably, regular lipid monitoring and physical health care for schizophrenic patients are usually suboptimal and may contribute to the high prevalence of CVD and increased mortality30,31. However, to date, the clinical features of olanzapine-induced dyslipidemia have remained controversial because of inconsistent data between studies7,8,9,10,11. In an early study, Osser et al. observed an elevation of plasma TG levels after olanzapine treatment32. The CATIE Schizophrenia Trial observed higher TG levels in patients with schizophrenia who were treated with olanzapine for 3 months than in those treated with ziprasidone33. This finding is supported by two recent studies that have also demonstrated an olanzapine-induced elevation of TG in patients with schizophrenia34,35. However, the data about the effects of olanzapine on plasma cholesterol (TC, HDL-C and LDL-C) levels were inconsistent. A meta-analysis in 2010 observed an increase of TC after olanzapine treatment36, but no significant TC elevation was shown in another meta-analysis of 18 studies37. Additionally, the data obtained from Chinese populations of individuals with schizophrenia also remain controversial. The studies by Lin et al.38 and Chiu et al.10 revealed that olanzapine increased TC and LDL-C in this population, with no obvious changes in HDL-C10,38. By contrast, no effects of olanzapine on TC and LDL-C were found by Huang et al.7. Concerning HDL-C, Ou et al. observed an increase after olanzapine therapy8, whereas an olanzapine-induced reduction of HDL-C was detected in another study11. Our meta-analysis demonstrates that olanzapine-induced dyslipidemia is characterized by elevations of TG, TC, and LDL-C, with no significant changes in HDL-C.
Our study also characterized the influence of olanzapine on serum lipids after 4 weeks of treatment and may be beneficial clinically to monitor the plasma lipid levels in a timely manner and help guide appropriate interventions if necessary. Of note, two studies concluded that TG levels increased significantly after 2–3 weeks of olanzapine treatment and found the increase in TG levels to occur before the weight gain and other lipid levels changes7,39. However, their relatively small sample sizes of 13 and 15 patients, make it difficult to generalize their findings to a broader clinical population of patients on olanzapine. More extensive studies will be required to validate the findings.
While the mechanism of olanzapine-induced dyslipidemia remains unknown, several factors have been implicated. First, olanzapine antagonizes the 5-hydroxytryptamine and histamine H1 receptors in the hypothalamus40,41, and promotes adenosine monophosphate activated protein kinase (AMPK) phosphorylation in the central nervous system42. This in turn results in increased food intake, dyslipidemia and obesity43. Dyslipidemia may be a secondary reaction to olanzapine-induced weight gain or obesity. Our study only revealed changes in four lipid parameters and did not explore the relationship between lipid profile and body weight. More studies such as meta-analyses or large-scale clinical trials could be conducted to discuss this issue in the future. Besides, the concentrations of circulating leptin and ghrelin were also significantly increased in schizophrenic patients on olanzapine and correlated with increased food intake44,45. Second, olanzapine-induced insulin resistance inhibits the activity of lipoprotein lipase, thereby slowing the catabolism of LDL and increasing plasma LDL-C levels46,47. In addition, insulin resistance stimulates sterol regulatory element binding protein-1c (SREBP-1c), which enhances the production of very low density lipoprotein in the liver and consequently increases plasma TG levels48,49. Third, the molecular mechanisms underlying olanzapine-associated lipid dysregulation are partly understood. Olanzapine enhances lipogenesis directly in the liver by regulating the expression of AMPK, SREBP-1c or peroxisome proliferation-activated receptor in the liver and disturbing the transcription of genes regulating lipid metabolism50,51,52.
Of note, this meta-analysis is subject to several limitations. First, the variance in the reagents and instruments for lipid measurement used among the included studies contributed to heterogeneity. Second, the inclusion of several studies with small samples might impair the authority of our conclusions. Third, this manuscript was marred by currently inefficient resource sharing.
Conclusion
The present analysis demonstrated that olanzapine-induced dyslipidemia in patients with schizophrenia is characterized by elevated plasma TG, TC, and LDL-C levels, with no significant changes in HDL-C. Dyslipidemia always occurs already by 4 weeks of treatment and, to some extent, exhibits a time-dependent effect. Hence, there is an urgent need for physicians to manage olanzapine-induced dyslipidemia in patients with schizophrenia to prevent the development of CVD in this population. However, a more comprehensive meta-analysis, with unlimited access to the literature, will be required to validate our findings. In addition, further long-term studies that allow the use of lipid-lowering medications upon the emergence of hyperlipidemia will be needed.
References
Owen, M. J., Sawa, A. & Mortensen, P. B. Schizophrenia. Lancet 388, 86–97. https://doi.org/10.1016/s0140-6736(15)01121-6 (2016).
Curkendall, S. M., Mo, J., Glasser, D. B., Rose Stang, M. & Jones, J. K. Cardiovascular disease in patients with schizophrenia in Saskatchewan, Canada. J. Clin. Psychiatry65, 715–720, https://doi.org/10.4088/jcp.v65n0519 (2004).
Ryan, M. C. & Thakore, J. H. Physical consequences of schizophrenia and its treatment: The metabolic syndrome. Life Sci. 71, 239–257. https://doi.org/10.1016/s0024-3205(02)01646-6 (2002).
Henderson, D. C., Vincenzi, B., Andrea, N. V., Ulloa, M. & Copeland, P. M. Pathophysiological mechanisms of increased cardiometabolic risk in people with schizophrenia and other severe mental illnesses. Lancet Psychiatry 2, 452–464. https://doi.org/10.1016/s2215-0366(15)00115-7 (2015).
Reynolds, G. P. & Kirk, S. L. Metabolic side effects of antipsychotic drug treatment–pharmacological mechanisms. Pharmacol. Ther. 125, 169–179. https://doi.org/10.1016/j.pharmthera.2009.10.010 (2010).
Misawa, F. et al. Is antipsychotic polypharmacy associated with metabolic syndrome even after adjustment for lifestyle effects?: A cross-sectional study. BMC Psychiatry 11, 118. https://doi.org/10.1186/1471-244x-11-118 (2011).
Huang, T. L. & Chen, J. F. Serum lipid profiles and schizophrenia: Effects of conventional or atypical antipsychotic drugs in Taiwan. Schizophr. Res. 80, 55–59. https://doi.org/10.1016/j.schres.2005.05.001 (2005).
Ou, J. J. et al. Comparison of metabolic effects of ziprasidone versus olanzapine treatment in patients with first-episode schizophrenia. Psychopharmacology 225, 627–635. https://doi.org/10.1007/s00213-012-2850-6 (2013).
9Salviato Balbao, M. et al. Olanzapine, weight change and metabolic effects: A naturalistic 12-month follow up. Ther. Adv. Psychopharmacol.4, 30–36, https://doi.org/10.1177/2045125313507738 (2014).
Chiu, C. C., Chen, C. H., Chen, B. Y., Yu, S. H. & Lu, M. L. The time-dependent change of insulin secretion in schizophrenic patients treated with olanzapine. Prog. Neuropsychopharmacol. Biol. Psychiatry 34, 866–870. https://doi.org/10.1016/j.pnpbp.2010.04.003 (2010).
Gautam, S. & Meena, P. S. Drug-emergent metabolic syndrome in patients with schizophrenia receiving atypical (second-generation) antipsychotics. Indian J. Psychiatry 53, 128–133. https://doi.org/10.4103/0019-5545.82537 (2011).
Raal, F. J., Hovingh, G. K. & Catapano, A. L. Familial hypercholesterolemia treatments: Guidelines and new therapies. Atherosclerosis 277, 483–492. https://doi.org/10.1016/j.atherosclerosis.2018.06.859 (2018).
Mach, F. et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 41(1), 111–188. https://doi.org/10.1093/eurheartj/ehz455 (2019).
Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 62, 1006–1012. https://doi.org/10.1016/j.jclinepi.2009.06.005 (2009).
Margulis, A. V. et al. Quality assessment of observational studies in a drug-safety systematic review, comparison of two tools: The Newcastle-Ottawa Scale and the RTI item bank. Clin. Epidemiol. 6, 359–368. https://doi.org/10.2147/clep.s66677 (2014).
Slim, K. et al. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 73, 712–716 (2003).
Liu, H. H. & Li, J. J. Aging and dyslipidemia: A review of potential mechanisms. Ageing Res. Rev. 19, 43–52. https://doi.org/10.1016/j.arr.2014.12.001 (2015).
Higgins, J. P., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. BMJ (Clin. Res. Ed.) 327, 557–560. https://doi.org/10.1136/bmj.327.7414.557 (2003).
Kusumi, I. et al. Effect of olanzapine orally disintegrating tablet versus oral standard tablet on body weight in patients with schizophrenia: A randomized open-label trial. Prog. Neuropsychopharmacol. Biol. Psychiatry 36, 313–317. https://doi.org/10.1016/j.pnpbp.2011.11.004 (2012).
Chen, J., Pan, X., Qian, M. & Yang, S. Efficacy and metabolic influence on blood-glucose and serum lipid of ziprasidone in the treatment of elderly patients with first-episode schizophrenia. Shanghai Arch. Psychiatry 29, 104–110. https://doi.org/10.11919/j.issn.1002-0829.217005 (2017).
Wu, R.-R. et al. Effects of typical and atypical antipsychotics on glucose-insulin homeostasis and lipid metabolism in first-episode schizophrenia. Psychopharmacology 186, 572–578. https://doi.org/10.1007/s00213-006-0384-5 (2006).
McDonnell, D. P., Kryzhanovskaya, L. A., Zhao, F., Detke, H. C. & Feldman, P. D. Comparison of metabolic changes in patients with schizophrenia during randomized treatment with intramuscular olanzapine long-acting injection versus oral olanzapine. Hum. Psychopharmacol. 26, 422–433. https://doi.org/10.1002/hup.1225 (2011).
Correll, C. U. et al. Cardiometabolic risk in patients with first-episode schizophrenia spectrum disorders: Baseline results from the RAISE-ETP study. JAMA Psychiatry 71, 1350–1363. https://doi.org/10.1001/jamapsychiatry.2014.1314 (2014).
Sheitman, B. B., Bird, P. M., Binz, W., Akinli, L. & Sanchez, C. Olanzapine-induced elevation of plasma triglyceride levels. Am. J. Psychiatry 156, 1471–1472 (1999).
Koro, C. E. et al. An assessment of the independent effects of olanzapine and risperidone exposure on the risk of hyperlipidemia in schizophrenic patients. Arch. Gen. Psychiatry 59, 1021–1026. https://doi.org/10.1001/archpsyc.59.11.1021 (2002).
Abdel-Maksoud, M. F. & Hokanson, J. E. The complex role of triglycerides in cardiovascular disease. Semin. Vasc. Med. 2, 325–333. https://doi.org/10.1055/s-2002-35403 (2002).
Silverman, M. G. et al. Association between lowering LDL-C and cardiovascular risk reduction among different therapeutic interventions: A systematic review and meta-analysis. JAMA 316, 1289–1297. https://doi.org/10.1001/jama.2016.13985 (2016).
Reiner, Z. et al. Lipid lowering drug therapy in patients with coronary heart disease from 24 European countries–Findings from the EUROASPIRE IV survey. Atherosclerosis 246, 243–250. https://doi.org/10.1016/j.atherosclerosis.2016.01.018 (2016).
Casey, D. E. Metabolic issues and cardiovascular disease in patients with psychiatric disorders. Am. J. Med. 118(Suppl 2), 15s–22s. https://doi.org/10.1016/j.amjmed.2005.01.046 (2005).
Saxena, S. & Maj, M. Physical health of people with severe mental disorders: Leave no one behind. World Psychiatry 16, 1–2. https://doi.org/10.1002/wps.20403 (2017).
Mitchell, A. J., Delaffon, V., Vancampfort, D., Correll, C. U. & De Hert, M. Guideline concordant monitoring of metabolic risk in people treated with antipsychotic medication: Systematic review and meta-analysis of screening practices. Psychol. Med. 42, 125–147. https://doi.org/10.1017/s003329171100105x (2012).
Osser, D. N., Najarian, D. M. & Dufresne, R. L. Olanzapine increases weight and serum triglyceride levels. J. Clin. Psychiatry 60, 767–770. https://doi.org/10.4088/jcp.v60n1109 (1999).
Meyer, J. M. et al. Change in metabolic syndrome parameters with antipsychotic treatment in the CATIE Schizophrenia Trial: Prospective data from phase 1. Schizophr. Res. 101, 273–286. https://doi.org/10.1016/j.schres.2007.12.487 (2008).
Xiong, Z. et al. Association of blood cell counts with the risk of olanzapine- or clozapine-induced dyslipidemia in Chinese schizophrenia patients. Hum. Psychopharmacol. 34, e2699. https://doi.org/10.1002/hup.2699 (2019).
Albaugh, V. L., Singareddy, R., Mauger, D. & Lynch, C. J. A double blind, placebo-controlled, randomized crossover study of the acute metabolic effects of olanzapine in healthy volunteers. PLoS ONE 6, e22662. https://doi.org/10.1371/journal.pone.0022662 (2011).
Rummel-Kluge, C. et al. Head-to-head comparisons of metabolic side effects of second generation antipsychotics in the treatment of schizophrenia: A systematic review and meta-analysis. Schizophr. Res. 123, 225–233. https://doi.org/10.1016/j.schres.2010.07.012 (2010).
Buhagiar, K. & Jabbar, F. Association of first- vs. second-generation antipsychotics with lipid abnormalities in individuals with severe mental illness: A systematic review and meta-analysis. Clin. Drug Invest.39, 253–273, https://doi.org/10.1007/s40261-019-00751-2 (2019).
Lin, Y. et al. Serum IL-1ra, a novel biomarker predicting olanzapine-induced hypercholesterolemia and hyperleptinemia in schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 84, 71–78. https://doi.org/10.1016/j.pnpbp.2018.01.020 (2018).
Chiu, C.-C., Chen, K.-P., Liu, H.-C. & Lu, M.-L. The early effect of olanzapine and risperidone on insulin secretion in atypical-naive schizophrenic patients. J. Clin. Psychopharmacol. 26, 504–507. https://doi.org/10.1097/01.jcp.0000237947.80764.d9 (2006).
Martin-Gronert, M. S. et al. 5-HT2A and 5-HT2C receptors as hypothalamic targets of developmental programming in male rats. Dis. Models Mech. 9, 401–412. https://doi.org/10.1242/dmm.023903 (2016).
Kirk, S. L., Glazebrook, J., Grayson, B., Neill, J. C. & Reynolds, G. P. Olanzapine-induced weight gain in the rat: role of 5-HT2C and histamine H1 receptors. Psychopharmacology 207, 119–125. https://doi.org/10.1007/s00213-009-1639-8 (2009).
Manu, P. et al. Weight gain and obesity in schizophrenia: Epidemiology, pathobiology, and management. Acta Psychiatr. Scand. 132, 97–108. https://doi.org/10.1111/acps.12445 (2015).
Lopez, M. & Tena-Sempere, M. Estradiol effects on hypothalamic AMPK and BAT thermogenesis: A gateway for obesity treatment?. Pharmacol. Ther. 178, 109–122. https://doi.org/10.1016/j.pharmthera.2017.03.014 (2017).
Sentissi, O., Epelbaum, J., Olie, J. P. & Poirier, M. F. Leptin and ghrelin levels in patients with schizophrenia during different antipsychotics treatment: A review. Schizophr. Bull. 34, 1189–1199. https://doi.org/10.1093/schbul/sbm141 (2008).
Murashita, M. et al. Olanzapine increases plasma ghrelin level in patients with schizophrenia. Psychoneuroendocrinology 30, 106–110. https://doi.org/10.1016/j.psyneuen.2004.05.008 (2005).
Melkersson, K. Clozapine and olanzapine, but not conventional antipsychotics, increase insulin release in vitro. Eur. Neuropsychopharmacol. 14, 115–119. https://doi.org/10.1016/s0924-977x(03)00072-5 (2004).
Yan, H., Chen, J. D. & Zheng, X. Y. Potential mechanisms of atypical antipsychotic-induced hypertriglyceridemia. Psychopharmacology 229, 1–7. https://doi.org/10.1007/s00213-013-3193-7 (2013).
Postic, C. & Girard, J. Contribution of de novo fatty acid synthesis to hepatic steatosis and insulin resistance: Lessons from genetically engineered mice. J. Clin. Invest. 118, 829–838. https://doi.org/10.1172/jci34275 (2008).
Ferre, P. & Foufelle, F. SREBP-1c transcription factor and lipid homeostasis: Clinical perspective. Horm. Res. 68, 72–82. https://doi.org/10.1159/000100426 (2007).
Polymeropoulos, M. H. et al. Common effect of antipsychotics on the biosynthesis and regulation of fatty acids and cholesterol supports a key role of lipid homeostasis in schizophrenia. Schizophr. Res. 108, 134–142. https://doi.org/10.1016/j.schres.2008.11.025 (2009).
Jassim, G. et al. Acute effects of orexigenic antipsychotic drugs on lipid and carbohydrate metabolism in rat. Psychopharmacology 219, 783–794. https://doi.org/10.1007/s00213-011-2397-y (2012).
Oh, K. J. et al. Atypical antipsychotic drugs perturb AMPK-dependent regulation of hepatic lipid metabolism. Am. J. Physiol. Endocrinol. Metab.300, E624–E632, https://doi.org/10.1152/ajpendo.00502.2010 (2011).
Berg, P. H. et al. Olanzapine versus ziprasidone: Results of a 28-week double-blind study in patients with schizophrenia. Am. J. Psychiatry 162, 1879–1887. https://doi.org/10.1176/appi.ajp.162.10.1879 (2005).
Kane, J. et al. Treatment of schizophrenia with paliperidone extended-release tablets: A 6-week placebo-controlled trial. Schizophr. Res. 90, 147–161. https://doi.org/10.1016/j.schres.2006.09.012 (2007).
Saddichha, S., Manjunatha, N., Ameen, S. & Akhtar, S. Metabolic syndrome in first episode schizophrenia—A randomized double-blind controlled, short-term prospective study. Schizophr. Res. 101, 266–272. https://doi.org/10.1016/j.schres.2008.01.004 (2008).
Kryzhanovskaya, L. et al. Olanzapine versus placebo in adolescents with schizophrenia: A 6-week, randomized, double-blind, placebo-controlled trial. J. Am. Acad. Child Adolesc. Psychiatry 48, 60–70. https://doi.org/10.1097/CHI.0b013e3181900404 (2009).
Bushe, C., Sniadecki, J., Bradley, A. J. & Poole Hoffmann, V. Comparison of metabolic and prolactin variables from a six-month randomised trial of olanzapine and quetiapine in schizophrenia. J. Psychopharmacol. (Oxford, England)24, 1001–1009, https://doi.org/10.1177/0269881108101783 (2010).
Narula, P. K., Rehan, H. S., Unni, K. E. & Gupta, N. Topiramate for prevention of olanzapine associated weight gain and metabolic dysfunction in schizophrenia: A double-blind, placebo-controlled trial. Schizophr. Res. 118, 218–223. https://doi.org/10.1016/j.schres.2010.02.001 (2010).
Schreiner, A. et al. Metabolic effects of paliperidone extended release versus oral olanzapine in patients with schizophrenia: A prospective, randomized, controlled trial. J. Clin. Psychopharmacol. 32, 449–457. https://doi.org/10.1097/JCP.0b013e31825cccad (2012).
Hu, S. et al. A randomized, 12-week study of the effects of extended-release paliperidone (paliperidone ER) and olanzapine on metabolic profile, weight, insulin resistance, and beta-cell function in schizophrenic patients. Psychopharmacology 230, 3–13. https://doi.org/10.1007/s00213-013-3073-1 (2013).
Modabbernia, A. et al. Melatonin for prevention of metabolic side-effects of olanzapine in patients with first-episode schizophrenia: Randomized double-blind placebo-controlled study. J. Psychiatr. Res. 53, 133–140. https://doi.org/10.1016/j.jpsychires.2014.02.013 (2014).
Zhang, S. & Lan, G. Prospective 8-week trial on the effect of olanzapine, quetiapine, and aripiprazole on blood glucose and lipids among individuals with first-onset schizophrenia. Shanghai Arch. Psychiatry 26, 339–346. https://doi.org/10.11919/j.issn.1002-0829.214037 (2014).
Kumar, P. N. S., Anish, P. K. & Rajmohan, V. Olanzapine has better efficacy compared to risperidone for treatment of negative symptoms in schizophrenia. Indian J. Psychiatry 58, 311–316. https://doi.org/10.4103/0019-5545.192016 (2016).
Tanaka, K. et al. Decreased levels of ghrelin, cortisol, and fasting blood sugar, but not n-octanoylated ghrelin, in Japanese schizophrenic inpatients treated with olanzapine. Prog. Neuropsychopharmacol. Biol. Psychiatry 32, 1527–1532. https://doi.org/10.1016/j.pnpbp.2008.05.013 (2008).
Gilles, M. et al. Visceral and subcutaneous fat in patients treated with olanzapine: A case series. Clin. Neuropharmacol. 33, 248–249. https://doi.org/10.1097/WNF.0b013e3181f0ec33 (2010).
Acknowledgements
This work was supported by the National Natural Science Foundation of China (Grant number 81974281), the National Natural Science Foundation for Young Programs of China (Grant number 81700999), and the Natural Science Foundation of Hunan Province (Grant number 2018JJ3741).
Author information
Authors and Affiliations
Contributions
Y.Z. and W.Z. reviewed literature and designed the review, Y.Z. and R.L. conducted the search for the systematic review, C.D. and R.L. interpreting the data, X.S., W.J. D. and W.D. conducted the statistical analysis, J.X. and Z.X. prepared the figures and tables, X.H. revising the manuscript, and all authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, R., Zhang, Y., Zhu, W. et al. Effects of olanzapine treatment on lipid profiles in patients with schizophrenia: a systematic review and meta-analysis. Sci Rep 10, 17028 (2020). https://doi.org/10.1038/s41598-020-73983-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-73983-4
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
