
Abstract
Treatment of rheumatoid arthritis (RA) is aimed at long-term remission and inhibition of joint destruction by different biologic drugs. However, the choice of a particular biologic agent based on individual cases of RA remains unestablished. Interleukin-6 (IL-6) inhibitor and tumor necrosis factor (TNF) inhibitor are common biologics used for the treatment of RA. This study aimed to investigate predictive factors for effective selection of tocilizumab (IL-6 inhibitor) and etanercept (TNF inhibitor) in patients with RA. This is a retrospective cohort study. The 196 patients analyzed in this study were divided into four groups: tocilizumab treatment as the first biologic group (TCZ first, 42 patients), tocilizumab as second/ third biologic group (TCZ second, 34 patients), etanercept as the first biologic group (ETN first, 103 patients) and etanercept as second/third group (ETN second, 17 patients). Visual analog scale (VAS), clinical disease activity index (CDAI), and modified health assessment questionnaire (mHAQ) scores at the initiation of biologic treatment and after 6 months of tocilizumab and etanercept therapy were measured and compared to clinical parameters and radiographical parameters among the four groups. CRP, MMP-3, VAS, CDAI, and HAQ were improved after 6 months of treatment in all groups. Improvement of clinical outcomes was correlated with CRP value, duration of RA, and Sharp scores at the initiation of treatment. Multivariate analysis demonstrated improvement in CDAI was significantly associated with the yearly progression of erosion according to the Sharp score in TCZ first group (OR, 1.5; 95% CI, 1.03–2.07) and was negatively associated with the duration of RA (OR, 0.49; 95% CI, 0.29–0.86) at the initiation of treatment with ETN first group. We identified the predictive factors for effective selection of tocilizumab and etanercept treatment and established the effectiveness of tocilizumab for the patients with rapid progressive joint erosion and etanercept for the early administration from diagnosis of RA.
Similar content being viewed by others


Introduction
Rheumatoid arthritis (RA) is an autoimmune disease characterized by chronic inflammation of the synovial lining of the joint1, commonly observed with progressive joint destruction and systemic complications2. Joint inflammation causes bone erosions and cartilage loss, leading to the narrowing of the joint space, thereby resulting in joint deformities and functional impairments2. The treatment of RA has progressed with the introduction of biologic disease-modifying antirheumatic drugs (DMARDs) and standard implementation of the treat-to-target approach aimed at clinical remission, which has had a remarkable benefit in preventing joint damage and thereby improving the long-term outcomes in these patients3.
TNF plays a main role in RA, and many TNF inhibitors have been developed for the RA treatment4,5,6. TNF-α induces the secretion of multiple proinflammatory cytokines such as IL-1, -6, -8, granulocyte-macrophage colony-stimulating factor (GCS-F), and dickkopf (DKK)-1 which regulates Wnt pathway7,8. Previous reports showed that TNF inhibitor decreases serum DKK-1 levels in RA patients8, and DKK-1 levels correlated with destruction of radiographic change9. Therefore, the role of the Wnt pathway molecules including DKK-1 and sclerostin were important, however in vivo effect of TNF-α inhibitor on bone loss in RA patients are limited10,11.
IL-6, another pleiotropic cytokine with proinflammatory and immune stimulatory actions, plays a significant role in the pathogenesis of RA and disease activity12. The expression of serum IL-6 and IL-6 receptor is correlated with inflammation, clinical signs and symptoms, and radiographic signs of joint destruction13,14. IL-6 affects the function of neutrophils, T cells, B cells, monocytes, and osteoclasts that are highly activated in RA. IL-6 also affects the hepatic acute phase response, which is a key feature of RA15. As a key regulator in osteoclast differentiation, IL-6 may promote erosive joint changes by activating osteoclast formation and accelerating bone resorption14.
Etanercept is a fully human soluble TNF receptor Fc fusion protein that inhibits the binding of TNF receptors, blocking the proinflammatory activities of TNF receptor signaling16, and several studies demonstrated therapy with etanercept could inhibit the progression of joint destruction and repair bone erosion17,18. Tocilizumab is a humanized monoclonal antibody that inhibits the binding of IL-6 to the soluble- and membrane-expressed IL-6 receptors, blocking the proinflammatory activities of IL-6/IL-6 receptor signaling19,20,21. In a study involving patients with RA, tocilizumab monotherapy was found to be superior to conventional DMARDs for radiographic progression22. Similarly, tocilizumab treatment with methotrexate (MTX) considerably reduced cartilage degradation markers26.
Thus, rheumatologists can choose from several different types of biological DMARDs, including IL-6 and TNF inhibitors, for the treatment of RA. However, there are no established treatment guidelines for the selection of biologic drugs in individual patients based on their effectiveness. Tocilizumab and etanercept are commonly used as biological drugs for the treatment of RA23,24. Further, several reports showed the response to biological drugs was changed between the biologic treatment as the first drug and the treatment as the second drug because the immune response of the patient receiving second biologics may be altered after the first biological drug25,26. Therefore, the purpose of the present study was to evaluate the association between the patient factors and clinical outcome for the four groups (TCZ first, TCZ second, ETN first, and ETN second) to investigate the effective selection of biological drugs for the treatment of RA patients.
Patients and methods
Patient selection
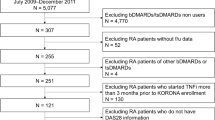
This was a retrospective cohort study. Medical records of 196 patients with RA who were treated with tocilizumab at Matsubara Mayflower Hospital and Kobe University Hospital between October 2004 and September 2018 were analyzed. All patients included in the study were qualified according to the 1987 American College of Rheumatology RA criteria27. The inclusion criteria of this study were the patient who was treated with tocilizumab or etanercept for at least 6 months, and the administration of tocilizumab or etanercept treatment in the last 5 years of diagnosis as RA. The exclusion criteria of this study were the patient who was overlapped with tocilizumab and etanercept treatment. All the patients were treated with RA within three biological drugs. Finally, the 196 patients analyzed in this study were divided into four groups: tocilizumab treatment as the first biologic group (TCZ first, 42 patients), tocilizumab as second/third biologic group (TCZ second, 34 patients), etanercept as the first biologic group (ETN first, 103 patients) and etanercept as second/ third group (ETN second, 17 patients).
Clinical evaluation
Collected data included the age, duration of RA, Steinbrocker class and stage, MTX dose (mg/week), glucocorticoid doses (mg/day), CRP, and MMP-3 at the time of introduction of the tocilizumab or etanercept therapy. The duration of RA was determined between the time of diagnosis as RA and the time of administration of tocilizumab or etanercept treatment. Data of modified HAQ (mHAQ), patients’ visual analog scale (VAS), and clinical disease activity index (CDAI) were obtained as clinical outcomes at the initiation of treatment and after 6 months of tocilizumab or etanercept therapy. Delta mHAQ, delta VAS, and delta CDAI were values of improvement between initiation of treatment and after 6 months of tocilizumab or etanercept therapy (values at the initiation of treatment-values at 6 M).
Radiographic evaluation
Radiographs of the hands and feet were assessed according to the Sharp method28. All radiographic follow-up data included in the analysis were obtained within 5 years of the diagnosis of RA. In total, scores for the 196 radiographs (from 196 patients) were determined by a single experienced rheumatologist who was blinded to the clinical data. Sixteen and six areas were considered for assessing erosions and joint space narrowing (JSN) for the hands and feet, respectively. The maximum erosion score of the hands and wrists was 160, and that of the feet is 120 (maximum total erosion score: 280). Accordingly, the maximum JSN score of the hands and wrists was 120, and that of the feet is 48 (maximum total JSN score: 168). The sum of the erosion and JSN scores is the total Sharp/van der Heijde score (SHS) (maximum: 448). Therefore, radiographic joint destruction was quantified as the total SHS score divided by the duration of RA.
Statistical analysis
Demographic and clinical characteristics of patients of TCZ first, TCZ second, ETN first, and ETN second with the statistical analysis are provided in Tables 1, 2, 3, 4 and 5. All data are expressed as mean ± standard deviation unless otherwise indicated. Patients' backgrounds were compared among four groups using one-way (Table 1) analysis of variance, with Tukey’s post hoc test for multiple comparisons of paired samples. To assess the improvement in laboratory data (CRP and MMP-3) and clinical scores (mHAQ, VAS, and CDAI), we compared values between initiation of treatment and 6 M using paired t-test (Table 2). Post-hoc power analysis was performed using G*Power 329. For Pearson’s correlation analysis, the study is expected to provide a power (1 − β) of 0.87, 0.80, 0.99, and 0.55 for detecting an effect size q (H1) of 0.4, in TCZ first (n = 42), TCZ second (n = 34), ETN first (n = 103) and ETN second (n = 17) groups, respectively. In addition, for paired t-test, we calculated the effect size by means and SDs based on the Hedges’g for each parameter and the 95% confidence interval (CI) for effect sizes30.
Correlations between predictive factors (clinical and radiographic parameters) and clinical outcomes in each of the four groups were analyzed using Pearson’s correlation value (Tables 3, 4). To identify predictive factors of the effective selection of tocilizumab or etanercept therapy, we performed a multivariate analysis in the four groups to test the association among CRP, duration of RA, and radiographic parameters (TSS/year, Sharp score erosion/year, and Sharp score joint narrow/year) with the improvement in CDAI (Table 5). Improvement in CDAI was determined as following; patients were classified as remission (CDAI < 2.8), low activity (2.8 ≤ CDAI < 10), moderate activity (10 ≤ CDAI < 22), and high activity (CDAI ≥ 22) based on predefined cutoff values for CDAI, and we defined improvement of CDAI when disease activity class of the patient was changed to lower activity class after 6 months of tocilizumab or etanercept treatment. Predictive factors were identified using multivariate analysis. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were calculated for multivariate analysis. Data were analyzed using SPSS version 19 J (IBM Japan, Tokyo, Japan).
Ethics statement and patient consent
This study complies with the Declaration of Helsinki, and study protocols were approved by the ethics committee of the Research Institute of Joint Disease Kobe and Kobe University Graduate School of Medicine, and all participants provided informed consent for participation.
Results
Patient characteristics
The 196 patients analyzed in this study were divided into four groups. Patient characteristics of the four groups including age, duration of RA, Steinbrocker classification stage and class, weekly MTX and daily glucocorticoid dosages, and TSS including the Sharp score for erosion, Sharp for joint space narrowing, total Sharp score/year, sharp score for erosion/year, and Sharp score for joint space narrowing/year at initiation of biologics are provided in Table 1. One-way analysis of variance demonstrated significant differences of patient radiographic parameters of Total Sharp score, Sharp score for joint narrow, and sharp score for erosion/year were found among the four groups (Table 1). Post hoc analysis demonstrated significant differences and were found between TCZ first group and TCZ second group in Total Sharp score (p = 0.027), TCZ second group and ETN first in Sharp score for joint narrow (p = 0.022), and TCZ first and TCZ second in sharp score for erosion/year (p = 0.046), respectively.
Biological drugs treatment improved laboratory data and clinical outcomes
Laboratory data and clinical outcomes of our study are provided in Table 2. Both tocilizumab and etanercept treatment for 6 months significantly improved laboratory data (CRP, MMP-3) and clinical outcomes (mHAQ, VAS, CDAI) except mHAQ in TCZ second group (Table 2).
Improvement of clinical outcomes was correlated with CRP value and duration of RA at the initiation of treatment
The correlation between clinical outcomes and clinical parameters in tocilizumab or etanercept patients are provided in Table 3. There was no significant correlation between clinical parameters including age, Steinbrocker classification stage and class, weekly MTX dose, daily glucocorticoid dose, or MMP-3 and clinical outcomes (delta mHAQ, delta VAS, delta CDAI). However, there was a significant correlation between CRP value at initiation of treatment and the improvement of patients VAS or CDAI (delta VAS: rr = 0.40, p = 0.017; delta CDAI: rr = 0.44, p = 0.016) with tocilizumab first treatment and between CRP value and the improvement of patients mHAQ and CDAI (delta mHAQ: rr = 0.36, p = 0.007; delta CDAI: rr = 0.31, p = 0.038) with etanercept first treatment (Table 3). Further, significant correlation was found between RA duration and the improvement of patients VAS or CDAI (delta VAS: rr = 0.25, p = 0.040; delta CDAI: rr = 0.40, p = 0.002) with etanercept first treatment or the improvement of patients VAS or CDAI (delta VAS: rr = 0.78, p = 0.0001; delta CDAI: rr = 0.65, p = 0.012) with etanercept second/ third treatment (Table 3). Here, we demonstrated two clinical predictive factors (CRP, duration of RA) related to effective selection for tocilizumab and etanercept treatment by Pearson’s correlation analysis.
Improvement of clinical outcomes was correlated with radiographic parameters at the initiation of treatment
The correlation between clinical outcomes and radiographic parameters, including yearly progression of TSS, erosion Sharp score, and joint narrow Sharp score, are shown in Table 4. A significant correlation between the yearly progression of erosion Sharp score and improvement in CDAI (delta CDAI) were found in TCZ first and second group (TCZ first: rr = 0.44, p = 0.034; TCZ second: rr = 0.58, p = 0.032) (Table 4). A significant correlation between improvement of HAQ (delta HAQ) and three radiographic parameters were found in ETN second group (TSS/year: rr = 0.66, p = 0.005, erosion Sharp score/year: rr = 0.63, p = 0.009, joint narrow Sharp score/year: rr = 0.56, p = 0.025). There was no significant correlation between clinical outcomes and radiographic parameters in ETN first group (Table 4). Here, we demonstrated three radiographic predictive factors (TSS/year, erosion Sharp score/year, joint narrow Sharp score/year) related to effective selection for tocilizumab and etanercept treatment by Pearson’s correlation analysis.
Predictive factors of good response to tocilizumab and etanercept treatment
We demonstrated five significant predictive factors (CRP, duration of RA, TSS/year, erosion Sharp score/year, joint narrow Sharp score/year) related to effective selection for tocilizumab and etanercept treatment by Pearson’s correlation analysis. However, predictive factors might be dependent on multiple confounders. Therefore, these five significant predictive factors were used as covariates for multivariate analysis. We demonstrated that the improvement of CDAI was significantly associated with the yearly progression of erosion Sharp score (OR, 1.5; 95% CI, 1.03–2.07) at the initiation of treatment with TCZ first group and was negatively associated with duration of RA (OR, 0.49; 95% CI, 0.29–0.86) at the initiation of treatment with ETN first group (Table 5). There was no significant association between clinical factors or radiographic parameters and clinical outcomes in the patients with TCZ second group or ETN second group.
Discussion
In the present study, we identified the predictive factors related to the effective selection of tocilizumab and etanercept treatment in RA. Improvement in CDAI was associated with the rapid progression of joint erosion before tocilizumab treatment as first biologic patients. The high correlation coefficients between improvement of CDAI and rapid progression of joint erosion was found in patients with tocilizumab treatment as second biologic, but the multivariate analysis did not show significant association. Recently, several reports demonstrated tocilizumab treatment to be more effective for the inhibition of bone erosion than inhibition of JSN31,32,33. Teitsma and colleagues reported that tocilizumab treatment with or without MTX in DMARD naïve patients with early RA is more effective in preventing progression of bone erosion compared to patients on MTX monotherapy; however, no significant difference in JSN was observed between the two groups31. FUNCTION study also showed that more progression of erosion was observed in patients with early RA on treatment with MTX alone compared to those treated with tocilizumab and MTX, but no significant difference in JSN was observed at 52 weeks32,33. From the point of cellular and molecular aspects, several studies demonstrated that the main activity of IL-6 on bone is its effect on osteoclastogenesis and bone resorption34,35,36. IL-6 stimulates osteoclast-like formation in long-term human marrow cultures by inducing IL-1 release36. IL-6 also mediates the stimulatory effects of TNF37 and enhances PTHrp-mediated hypercalcemia and bone resorption by increasing the pool of osteoclastic progenitors and their differentiation into mature osteoclasts38. TNF-a induces the production of RANKL both by indirectly influencing osteoclastogenesis supporting mesenchymal cells, and by directly influencing osteoclast precursor cells through the expression or the activation of factors such as RANK, TRAF6, and NF-kB, which are activated in the early phase of osteoclast differentiation39. However, the TNF-alpha may not directly induce osteoclastogenesis38, and TNF inhibitor therapy will not provide a complete reduction of bone damage in vivo study40. These studies supported our finding that improvement in CDAI was associated with the progression of joint erosion before initiation of tocilizumab treatment but not etanercept treatment.
We showed that the expression levels of MMP-3 was inhibited by tocilizumab and etanercept treatment in RA patients, and the expression levels at initiation of biologic treatment did not affect clinical outcomes between tocilizumab and etanercept treatment. Cartilage is mainly composed of collagen type II (70%) and proteoglycans, including aggrecan, and MMPs and aggrecanases are mediators of cartilage degradation41. MMP-3 is present in RA synovial fluid and overexpressed in rheumatoid synovium37. The expression levels of MMP-3 is associated with higher joint destruction in RA38. TNF blocker treatment decreased serum MMP-3 expression in RA patients42. We previously demonstrated that tocilizumab (IL-6 blocker) also inhibited serum MMP-3 expression through a similar mechanism as TNF inhibitor43. Therefore, the MMP-3 expression may not affect clinical outcomes between tocilizumab and etanercept treatment.
We also demonstrated that the duration of RA was negatively associated with improvement in CDAI in response to etanercept treatment as the first biologic. In other words, etanercept treatment is more effective for patients with early RA. Previous reports demonstrated aggressive treatment after the first 3 months of symptoms, with either conventional DMARD (csDMARD) or biologic DMARD (bDMARD) reducing the rate of disease progression44. Several studies attempt to evaluate the priority of bDMARD treatment as first-line for early RA patients45,46,47. However, bDMARD-naïve and MTX- naïve cohorts did not show a clear benefit of bDMARD as first-line45,46,47. Therefore, bDMARDs are still restricted to MTX- inadequate response, which avoids overtreatment. In our study, the average duration of RA in the etanercept first group was 1.8 years, and all the patients were treated with csDMARD prior to etanercept therapy. However, etanercept treatment was more effective for patients with shorter duration of RA. Therefore, we recommend the decision of switching from initial csDMARD to etanercept maybe earlier from initiation of RA treatment.
The limitation of this study is that the sample sizes in subgroups of the cohort were not large, and power is limited, especially in the ETN second group. Therefore, the data of ETN second has to be increased and re-analyzed in the future. Second, the patients’ radiographic background of Sharp score was different among the four groups. Sharp scores of tocilizumab as second/third biologic patients at initiation of treatment were higher than other groups because tocilizumab treatment was not recommended as a second biologic drug until EULAR 2013 recommendations presentation48. Although tocilizumab was used for more patients after the radiographic change, the study showed a significant correlation between improvement of CDAI and Sharp scores for erosion.
In conclusion, we identified the predictive factors related to the effective selection of tocilizumab and etanercept treatment. We propose the use of tocilizumab for the patients with rapid progressive joint erosion and etanercept for the early initiation of RA treatment.
References
Klareskog, L., Catrina, A. I. & Paget, S. Rheumatoid arthritis. Lancet 373(9664), 659–672 (2009).
Radner, H., Smolen, J. S. & Aletaha, D. Comorbidity affects all domains of physical function and quality of life in patients with rheumatoid arthritis. Rheumatology (Oxford) 50(2), 381–388 (2011).
Balanescu, A. & Wiland, P. Maximizing early treatment with biologics in patients with rheumatoid arthritis: the ultimate breakthrough in joints preservation. Rheumatol. Int. 33(6), 1379–1386 (2013).
Feldmann, M. & Maini, S. R. Role of cytokines in rheumatoid arthritis: an education in pathophysiology and therapeutics. Immunol. Rev. 223, 7–19 (2008).
Emery, P. et al. Golimumab, a human anti-tumor necrosis factor alpha monoclonal antibody, injected subcutaneously every four weeks in methotrexate-naive patients with active rheumatoid arthritis: twenty-four-week results of a phase III, multicenter, randomized, double-blind, placebo-controlled study of golimumab before methotrexate as first-line therapy for early-onset rheumatoid arthritis. Arthritis Rheum. 60(8), 2272–2283 (2009).
Smolen, J. S. et al. Evidence of radiographic benefit of treatment with infliximab plus methotrexate in rheumatoid arthritis patients who had no clinical improvement: a detailed subanalysis of data from the anti-tumor necrosis factor trial in rheumatoid arthritis with concomitant therapy study. Arthritis Rheum. 52(4), 1020–1030 (2005).
Butler, D. M., Maini, R. N., Feldmann, M. & Brennan, F. M. Modulation of proinflammatory cytokine release in rheumatoid synovial membrane cell cultures. Comparison of monoclonal anti TNF-alpha antibody with the interleukin-1 receptor antagonist. Eur. Cytokine Netw. 6(4), 225–230 (1995).
Haworth, C. et al. Expression of granulocyte-macrophage colony-stimulating factor in rheumatoid arthritis: regulation by tumor necrosis factor-alpha. Eur. J. Immunol. 21(10), 2575–2579 (1991).
Chin, J. E., Winterrowd, G. E., Krzesicki, R. F. & Sanders, M. E. Role of cytokines in inflammatory synovitis. The coordinate regulation of intercellular adhesion molecule 1 and HLA class I and class II antigens in rheumatoid synovial fibroblasts. Arthritis Rheum. 33(12), 1776–1786 (1990).
Choy, E. H. & Panayi, G. S. Cytokine pathways and joint inflammation in rheumatoid arthritis. N. Engl. J. Med. 344(12), 907–916 (2001).
Bazzoni, F. & Beutler, B. The tumor necrosis factor ligand and receptor families. N. Engl. J. Med. 334(26), 1717–1725 (1996).
Walsh, N. C., Crotti, T. N., Goldring, S. R. & Gravallese, E. M. Rheumatic diseases: the effects of inflammation on bone. Immunol. Rev. 208, 228–251 (2005).
Dasgupta, B., Corkill, M., Kirkham, B., Gibson, T. & Panayi, G. Serial estimation of interleukin 6 as a measure of systemic disease in rheumatoid arthritis. J. Rheumatol. 19(1), 22–25 (1992).
Kotake, S. et al. Interleukin-6 and soluble interleukin-6 receptors in the synovial fluids from rheumatoid arthritis patients are responsible for osteoclast-like cell formation. J. Bone Miner. Res. 11(1), 88–95 (1996).
Naka, T., Nishimoto, N. & Kishimoto, T. The paradigm of IL-6: from basic science to medicine. Arthritis Res. 4(Suppl 3), S233–S242 (2002).
Moreland, L. W. et al. Treatment of rheumatoid arthritis with a recombinant human tumor necrosis factor receptor (p75)-Fc fusion protein. N. Engl. J. Med. 337(3), 141–147 (1997).
Emery, P. et al. Comparison of methotrexate monotherapy with a combination of methotrexate and etanercept in active, early, moderate to severe rheumatoid arthritis (COMET): a randomised, double-blind, parallel treatment trial. Lancet 372(9636), 375–382 (2008).
van der Heijde, D. et al. Comparison of etanercept and methotrexate, alone and combined, in the treatment of rheumatoid arthritis: two-year clinical and radiographic results from the TEMPO study, a double-blind, randomized trial. Arthritis Rheum. 54(4), 1063–1074 (2006).
Mihara, M. et al. Tocilizumab inhibits signal transduction mediated by both mIL-6R and sIL-6R, but not by the receptors of other members of IL-6 cytokine family. Int. Immunopharmacol. 5(12), 1731–1740 (2005).
Nakahara, H. et al. Anti-interleukin-6 receptor antibody therapy reduces vascular endothelial growth factor production in rheumatoid arthritis. Arthritis Rheum. 48(6), 1521–1529 (2003).
Rose-John, S., Scheller, J., Elson, G. & Jones, S. A. Interleukin-6 biology is coordinated by membrane-bound and soluble receptors: role in inflammation and cancer. J. Leukoc. Biol. 80(2), 227–236 (2006).
Nishimoto, N. et al. Study of active controlled monotherapy used for rheumatoid arthritis, an IL-6 inhibitor (SAMURAI): evidence of clinical and radiographic benefit from an x ray reader-blinded randomised controlled trial of tocilizumab. Ann. Rheum. Dis. 66(9), 1162–1167 (2007).
Best, J. H., Vlad, S. C., Tominna, L. & Abbass, I. Real-World Persistence with tocilizumab compared to other subcutaneous biologic disease-modifying antirheumatic drugs among patients with rheumatoid arthritis switching from another biologic. Rheumatol. Ther. 7(2), 345–355 (2020).
Kilcher, G. et al. Rheumatoid arthritis patients treated in trial and real world settings: comparison of randomized trials with registries. Rheumatology (Oxford) 57(2), 354–369 (2018).
Codullo, V. et al. Comparison of efficacy of first- versus second-line adalimumab in patients with rheumatoid arthritis: experience of the Italian biologics registries. Clin. Exp. Rheumatol. 35(4), 660–665 (2017).
Gottenberg, J. E. et al. Non-TNF-targeted biologic vs a second anti-TNF drug to treat rheumatoid arthritis in patients with insufficient response to a first anti-TNF drug: a randomized clinical trial. JAMA 316(11), 1172–1180 (2016).
Arnett, F. C. et al. The American-rheumatism-association 1987 revised criteria for the classification of rheumatoid-arthritis. Arthritis Rheum. Us. 31(3), 315–324 (1988).
Sharp, J. T. et al. How many joints in the hands and wrists should be included in a score of radiologic abnormalities used to assess rheumatoid arthritis?. Arthritis Rheum. 28(12), 1326–1335 (1985).
Faul, F., Erdfelder, E., Buchner, A. & Lang, A. G. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav. Res. Methods 41(4), 1149–1160 (2009).
Durlak, J. A. How to select, calculate, and interpret effect sizes. J. Pediatr. Psychol. 34(9), 917–928 (2009).
Teitsma, X. M. et al. Radiographic joint damage in early rheumatoid arthritis patients: comparing tocilizumab- and methotrexate-based treat-to-target strategies. Rheumatology 57(2), 309–317 (2018).
Burmester, G. R. et al. Tocilizumab in early progressive rheumatoid arthritis: FUNCTION, a randomised controlled trial. Ann. Rheum. Dis. 75(6), 1081–1091 (2016).
Burmester, G. R. et al. Tocilizumab combination therapy or monotherapy or methotrexate monotherapy in methotrexate-naive patients with early rheumatoid arthritis: 2-year clinical and radiographic results from the randomised, placebo-controlled FUNCTION trial. Ann. Rheum. Dis. 76(7), 1279–1284 (2017).
Taguchi, Y. et al. Interleukin-6-type cytokines stimulate mesenchymal progenitor differentiation toward the osteoblastic lineage. Proc. Assoc. Am. Physicians 110(6), 559–574 (1998).
Kurihara, N., Bertolini, D., Suda, T., Akiyama, Y. & Roodman, G. D. IL-6 stimulates osteoclast-like multinucleated cell formation in long term human marrow cultures by inducing IL-1 release. J. Immunol. 144(11), 4226–4230 (1990).
Abe, K. et al. The usefulness of wide excision assisted by a computer navigation system and reconstruction using a frozen bone autograft for malignant acetabular bone tumors: a report of two cases. BMC Cancer 18(1), 1036 (2018).
Amimoto, H. et al. Force plate gait analysis and clinical results after tibial plateau levelling osteotomy for cranial cruciate ligament rupture in small breed dogs. Vet. Comp. Orthop. Traumatol. 33, 183–188 (2020).
Abdelmegeed, M. A., Ha, S. K., Choi, Y., Akbar, M. & Song, B. J. Role of CYP2E1 in mitochondrial dysfunction and hepatic injury by alcohol and non-alcoholic substances. Curr. Mol. Pharmacol. 10(3), 207–225 (2017).
Andersson-Sjoland, A. et al. Fibrocytes are a potential source of lung fibroblasts in idiopathic pulmonary fibrosis. Int. J. Biochem. Cell Biol. 40(10), 2129–2140 (2008).
Maruotti, N., d’Onofrio, F., Corrado, A. & Cantatore, F. P. Why TNF-alpha inhibition is not sufficient to avoid juxta-articular erosions in chronic arthritis?. Intern. Emerg. Med. 7(1), 15–20 (2012).
Goldring, M. B. & Marcu, K. B. Cartilage homeostasis in health and rheumatic diseases. Arthritis Res. Ther. 11(3), 224 (2009).
Ciatto, S. et al. Computer-aided detection (CAD) of cancers detected on double reading by one reader only. Breast 15(4), 528–532 (2006).
Bongartz, T. et al. Incidence and mortality of interstitial lung disease in rheumatoid arthritis: a population-based study. Arthritis Rheum. 62(6), 1583–1591 (2010).
Raza, K., Buckley, C. E., Salmon, M. & Buckley, C. D. Treating very early rheumatoid arthritis. Best Pract. Res. Clin. Rheumatol. 20(5), 849–863 (2006).
Nam, J. L. et al. Remission induction comparing infliximab and high-dose intravenous steroid, followed by treat-to-target: a double-blind, randomised, controlled trial in new-onset, treatment-naive, rheumatoid arthritis (the IDEA study). Ann. Rheum. Dis. 73(1), 75–85 (2014).
van Vollenhoven, R. F. et al. Addition of infliximab compared with addition of sulfasalazine and hydroxychloroquine to methotrexate in patients with early rheumatoid arthritis (Swefot trial): 1-year results of a randomised trial. Lancet 374(9688), 459–466 (2009).
Smolen, J. S. et al. Adjustment of therapy in rheumatoid arthritis on the basis of achievement of stable low disease activity with adalimumab plus methotrexate or methotrexate alone: the randomised controlled OPTIMA trial. Lancet 383(9914), 321–332 (2014).
Smolen, J. S. et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update. Ann. Rheum. Dis. 73(3), 492–509 (2014).
Funding
The authors have not received any financial support for this study.
Author information
Authors and Affiliations
Contributions
S.H., T.M., K.F., K.F., T.M. and M.H. contributed to study design. Hayashi wrote the main manuscript text. Kamenaga, Takashima, and Matsumoto contributed to acquisition and analysis of data. Niikura and Kuroda contributed to critical review of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hayashi, S., Matsubara, T., Fukuda, K. et al. Predictive factors for effective selection of Interleukin-6 inhibitor and tumor necrosis factor inhibitor in the treatment of rheumatoid arthritis. Sci Rep 10, 16645 (2020). https://doi.org/10.1038/s41598-020-73968-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-73968-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
