
Abstract
To determine levels of change in risk factors for cardiovascular disease among people with and without a previous diagnosis of diabetes from 2007 to 2016 in Iran. Data were obtained from five rounds of the World Health Organization STEPwise approach to Surveillance (STEPS) cross-sectional surveys. Participants were 7665 and 93,733 adults with and without known diabetes, respectively, aged 25–65 years. We used logistic and linear regressions to assess the trends of risk factors. Individuals with known diabetes compared to those without the condition, experienced greater reductions in mean levels of systolic blood pressure (3.0 vs. 0.5 mmHg among women and 3.9 vs. 1.6 mmHg among men), diastolic blood pressure (6.4 vs. 5.11 mmHg in women and 3.3 vs. 1.8 mmHg in men), and non-HDL cholesterol (42.4 vs. 27.2 mg/dL among women and 30.3 vs. 21.0 mg/dL among men) throughout these years. Men with diabetes also showed a greater reduction in the prevalence of daily cigarette smoking compared to their non-diabetic counterparts (7.3% vs. 2.3%). Fasting plasma glucose decreased among subjects with diabetes but increased among those without diabetes. Significant increases were observed in proportions who met goals for blood pressure, triglycerides, non-HDL cholesterol and LDL cholesterol in both groups; however, almost half of diabetic subjects did not achieve risk factor goals in 2016. Secondary prevention in diabetic patients was more effective than primary prevention in the general population; however, the rate of diabetic patients who met the designated goals for each risk factor was still suboptimal.
Similar content being viewed by others

Introduction
Diabetes is associated with premature mortality from different causes, including cardiovascular diseases (CVD)1. Previous studies have demonstrated the vitality of CVD risk factor control to decrease the fast-rising trend of this mortality and CVD events in people with diabetes2,3,4. Furthermore, evidence suggests that the use of more intensive targets for blood pressure and cholesterol in individuals with diabetes results in a more significant reduction in the incidence of CVD events5,6,7. However, several studies report that people with diabetes are less likely to achieve target goals for control of CVD risk factors than those without diabetes8,9.
Nationally representative data that investigate trends in CVD risk factors in both the general population and people with diabetes in Middle Eastern countries such as Iran are scarce. Moreover, due to the lack of proper investigations that compare secular trends for CVD risk factors in individuals with and without diabetes in this region, it is difficult to illustrate the impact of preventative programs on this population and also prioritize strategies for primary and secondary preventions.
The primary goal of this analysis is to characterize and compare the trends of body mass index (BMI), waist circumference (WC), blood pressure, smoking, plasma glucose and lipid measures among adults with known diabetes (as indicators of secondary prevention impacts) and those without known diabetes (as indicators of primary prevention impacts) in a nationally representative study from 2007 through 2016.
Results
Age and sex distribution of participants with and without known diabetes are presented in Table 1. The proportion of women was higher among those with known diabetes. The mean age for participants was approximately 44 years in all study years; however, for those with known diabetes, the mean age was almost ten years higher.
Trends of risk factors in persons with known diabetes
Among those with diabetes, there were significant reductions of mean SBP (from 134 to 131 mmHg in women and 134 to 130 mmHg in men), DBP (from 86 to 79 mmHg in women and 84 to 81 mmHg in men), LDL cholesterol (from 132 to 99 mg/dL in women and 121 to 97 mg/dL in men), non-HDL cholesterol (from 168 to 126 mg/dL in women and 155 to 125 mg/dL in men) and triglycerides (from 177 to 127 mg/dL in women and 171 to 146 mg/dL in men) in both sexes. Furthermore, there were significant reductions in FPG among women (from 147 to 139 mg/dL) and HDL cholesterol among men (from 40 to 35 mg/dL) (Figs. 1 and 2). There was not enough evidence supporting a significant trend for BMI and waist circumference.

Trends of CVD risk factor levels among women with (red dotted line) and without diabetes (black dashed line) through 2007–2016. Changes in mean levels Body Mass Index (BMI), Waist Circumference (WC), Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP) and Daily cigarette smoking are preented for five STEPS surveys in 2007, 2008, 2009, 2011 and 2016. Changes in Fasting Plasma Glucose FPG), Triglycerides (TGs), HDL cholesterol (HDL-C), non-HDL cholesterol (non-HDL-C) and LDL cholesterol throughout are presented for three STEPS surveys in 2007, 2011 and 2016.

Trends of CVD risk factor levels among men with (red dotted line) and without diabetes (black dashed line) through 2007–2016. Changes in mean levels Body Mass Index (BMI), Waist Circumference (WC), Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP) and Daily cigarette smoking are preented for five STEPS surveys in 2007, 2008, 2009, 2011 and 2016. Changes in Fasting Plasma Glucose FPG), Triglycerides (TGs), HDL cholesterol (HDL-C), non-HDL cholesterol (non-HDL-C) and LDL cholesterol throughout are presented for three STEPS surveys in 2007, 2011 and 2016.
Table 2 shows the trends of meeting goals/optimum levels of risk factors among persons with and without known diabetes. In both sexes, there were significant increases in the proportion of participants with an optimum level of blood pressure (from 47 to 58% in women and 55 to 62% in men), LDL cholesterol (from 21 to 54% in women and 26 to 57% in men), non-HDL cholesterol (from 21 to 58% in women and 26 to 59% in men), and triglycerides (from 36 to 66% in women and 39 to 53% in men). Glycemic control improved in diabetic women (from 49 to 55%) (Table 2) but not in diabetic men. Nevertheless, the prevalence of subjects who met HDL cholesterol goal significantly reduced in both sexes (from 19 to 17% in women and 44 to 23% in men).
Trends of risk factors among persons without known diabetes
There were a significant reduction in mean levels of lipid profiles, specially non-HDL cholesterol (from 146 to 119 mg/dL in women and 113 to 97 in men, 2007 vs. 2016) and triglycerides (from 132 to 100 mg/dL in women and 143 to 118 mg/dL in men) and prevalence of smoking (especially in men from 29.1 in 2007 to 21.8% in 2016) in both sexes. Regarding blood pressure, declining trends for mean DBP in both sexes and mean SBP in men were observed (Fig. 1). However, there was a slight, but statistically significant, increase in FPG (from 89 to 91 mg/dL in women and from 90 to 92 mg/dL in men, 2007 vs. 2016) and waist circumference (from 88.0 to 88.8 cm in women and from 88.7 to 91.0 in men). Only men had a significant increase in BMI (from 25.2 to 25.9 kg/m2) (Fig. 1).
In terms of optimal level of risk factors, we showed a significant increase in the proportion of those who had an optimal level of blood pressure (from 74.6 to 84.1% in women and 76.7 to 83.6% in men, 2007 vs. 2016), LDL cholesterol (from 69.1 to 91.8% in women and 74.3 to 92.4% in men), non-HDL cholesterol (from 67.6 to 91.5% in women and 71.0 to 90.7% in men), and triglycerides (from 67.6 to 83.4% in women and 59.6 to 74.0% in men) in both sexes. There were also decreasing trends in meeting optimal levels of FPG (from 84.6 to 80.9 in women and 83.7 to 78.0% in men) and HDL cholesterol (from 24.4 to 23.1% in women and 46.8 to 32.2% in men, 2007 vs. 2016) (Table 2).
Difference in the trend of risk factors in persons with and without known diabetes
In both sexes, diabetic individuals showed a greater reduction of mean SBP (3.0 vs. 0.5 mmHg in women and 3.9 vs. 1.6 mmHg in men), DBP (6.4 vs. 5.11 mmHg in women and 3.3 vs. 1.8 mmHg in men), LDL cholesterol (32.4 vs. 21.1 mg/dL in women and 24.0 vs. 16.4 mg/dL in men), and non-HDL cholesterol (42.4 vs. 27.2 mg/dL in women and 30.3 vs. 21.0 mg/dL in men) compared to non-diabetics throughout 2007 to 2016 (Fig. 1).
Moreover, women without known diabetes showed an increase in FPG while there was a significant reduction among their counterparts. Waist circumference increased among men without known diabetes, while it remained unchanged among those with known diabetes (Fig. 1). Regarding meeting risk factor goals, women with diabetes had significantly more increase in the proportion that met goals of triglycerides compared to non-diabetic women (29.4 vs. 15.8). Additionally, compared to non-diabetic men, those with diabetes had significantly more reduction in the prevalence of smoking from 2007 to 2016 (8.1% vs. 2.3%) (Fig. 2).
Discussion
In this study, we assessed national trends of cardio-metabolic risk factors from 2007 to 2016 in Iran concerning diabetes status. We provided some evidence on the effects of national efforts for primary and secondary prevention of cardio-metabolic disorders in a Middle Eastern country. There were significant improvements in blood pressure levels, non-HDL lipids, and daily smoking in the Iranian population; however, a deterioration in levels of HDL cholesterol was observed among those with and without diabetes. Importantly, we found increasing levels of obesity measurements and FPG in those without diabetes. Our findings suggest that secondary prevention has been more successful than primary prevention in reducing risk factors as they showed that changes in blood pressure, non-HDL cholesterol, FPG, and obesity (only in men) were more favorable in those with diabetes than those without the condition. Despite improvements over the past decade, meeting CVD risk factor goals, particularly among those with diabetes, remained suboptimal as almost half of Iranians with diabetes did not achieve risk factor goals.
Our findings regarding improvements in blood pressure and non-HDL lipid levels are in line with those of previous studies on Iranian populations, showing similar decreasing trends10,11,12 Notably, in this study, we had a higher proportion of participants, with and without diabetes who met goals of blood pressure and non-HDL lipids (53%-92%) compared with previous studies conducted in Iran (36%-87%)10,11,12. Our findings are also in line with those of the Global Burden of Disease (GBD) and NCD Risk Factor Collaboration (NCD-RisC), which showed reductions in the burden of high blood pressure and dyslipidemia in the Middle East and Worldwide13,14,15. Investigations from other countries have shown similar trends. Declines in mean SBP, DBP, LDL, non-HDL cholesterol and rate of smoking with more significant decreases among individuals with diabetes have been reported in studies from the National Health And Nutrition Examination Survey (NHANES) and the Framingham Heart Study in the US16,17 and the Health Survey for England 18. Accordingly, the prevalence of meeting blood pressure and LDL goals has been improved in the US16,17. Decreasing trends in high blood pressure were also found in studies from France and Japan, while the prevalence of hypercholesterolemia increased19,20. The results regarding HDL-cholesterol and triglycerides are different, from decreasing to no change or increasing21,22. Regarding the management of diabetes, in line with our findings, a study across 28 low-middle income countries uncovered poor control of diabetes, indicating a significant unmet need for diabetes care in these countries23. However, our results show that around 40–50% of our diabetic men and women reached the goal for glucose control, defined as FPG < 130, versus 23% on average in these 28 low-middle income countries, with a definition of FPG < 180 mg/dl; indicating much better situation of glucose control in Iran.
As one of the first countries from the Eastern Mediterranean Regional Office of WHO, Iran has responded to "a call for action" for the prevention and control of diabetes mellitus; and the national program was designed in 1996. The aim of this program is primary, secondary, and tertiary prevention, through community and high-risk screening, and the integration of diabetes care into the primary healthcare network. After the implementation in 2016 of IraPEN, an adaptation of WHO's Package of essential NCD (PEN) interventions for primary health care, this program integrated into the guidelines for prevention and control of major NCDs in the primary health care system. The current study shows that secondary prevention in diabetic patients has been more effective than primary prevention in the general population for controlling CVD risk factors, i.e., risk factors decreased more in diabetic patients than in non-diabetic subjects in the general population. However, the rate of diabetic patients who met the designated goals for each risk factor was still suboptimal.
The favorable changes may be rooted in nutritional habits, physical activity levels, smoking, and anti-hypertension or lipid-lowering drug consumption, all of which are known to be important determinants of blood pressure and serum lipid levels10,11. Previous studies showed that Iranian families had reduced the consumption of hydrogenated oil24,25 and salt26, which could explain the favorable blood pressure and lipid trends in Iranians. Further, previous studies showed increasing use of anti-hypertension or lipid-lowering drugs among Iranian10,11,12. Nevertheless, the decreasing trends in blood pressure and lipid levels in our population could hardly be explained by an increase in physical activity, since it was shown that low physical activity is common in Iranian community27,28.
Notably, by showing a significant reduction in the prevalence of daily smoking among those without known diabetes, this study suggests that efforts for lowering the prevalence of smoking have been successful in controlling the increasing trends10. The decrease in the prevalence of daily smoking in this group might also contribute to the decline in non-HDL lipid and blood pressure given the substantial evidence on the positive correlation of smoking with high blood pressure and dyslipidemia29,30.
On the contrary, we showed a rise in levels of obesity measurements in individuals without known diabetes (WC in both genders and BMI in men), which is probably the main reason for the increasing fasting plasma glucose trends in this group31,32. Contrary to the results of the previous studies that showed growing trends for HDL cholesterol in Iranian population10, this study showed a significant reduction in HDL cholesterol in those with and without diabetes. As shown in previous studies, decreasing levels of HDL cholesterol are mostly due to poor dietary habits and low levels of physical activity33,34. Deterioration in obesity measurements and HDL cholesterol levels should raise the alarm for policymakers as it indicates efforts for improvement of dietary habits and physical activity came short in this Iranian population. Based on previous studies in Iran28,35,36,37,38, the most important barriers to healthy nutrition and physical activity were interpersonal/cultural effects, lack of access to healthy foods, food preferences, media advertisements, nutrition transition, lack of time, motivation and prioritizing other activities over sports and high costs of the facilities. Therefore, feasible and effective national intervention programs are needed to curb current obesity epidemics by overcoming the barriers to healthy nutrition and physical activity. Despite the promising findings of several community-wide lifestyle intervention programs in Iran, such as Tehran Lipid and Glucose Study39 and Isfahan Healthy Heart Program40, these programs did not scale up in national levels.
In accordance with the evidence showing a correlation between diabetes and other cardio-metabolic risk factors, we showed risk factor levels were higher in those with diabetes compared to those without it10,31. Our findings support that the efforts on controlling blood pressure, dyslipidemia and obesity had more impacts among people with diabetes rather than non-diabetics. First of all, this is because diabetic patients experienced more reduction in mean SBP, DBP and non-HDL lipids. In addition, their obesity and blood glucose measurements remained steady, while people without diabetes showed a significant increase in obesity measurements. Favorable trends in dyslipidemia, obesity and blood glucose control in known diabetics may be due to improvements in care, knowledge and attitude towards diabetes as well as better adherence to lifestyle and pharmaceutical interventions. Previous studies show advancements in the quality of diabetes care, affordability of medications, and screening for undiagnosed diabetes as well as increasing trends in consumption of glucose-lowering (twofold in men and 1.5-fold in women) and lipid-lowering drugs (fourfold in men and 2.5-fold in women) among those with known diabetes10,41. Educational interventions in Iran, such as Self-Management Education (PDSME) program, also proved to be effective in improving the knowledge and practice of diabetes42,43, which is highly correlated with control of related risk factors44.
Nevertheless, in this study, the prevalence of daily smoking remained steady in participants with diabetes, while its prevalence reduced significantly in those without the disease. These findings are in contrast with those of a previous study that showed an increasing trend for smoking in those with diabetes was significantly higher than increases in smoking prevalence in those without diabetes10. This discrepancy may indicate favorable and radical changes in the prevalence of smoking. Another explanation may be the differences in the study sample and definition of smoking in this study compared to the previous studies, which were mostly cohort studies with local study samples and various definitions of smoking10,11. Further research is needed to provide more robust evidence on trends for smoking prevalence in Iran.
Since, during the last decades, the highest number of STEPS surveys in the Middle East have been conducted in Iran, it was made possible to investigate the secular trend of CVD risk factors using national data for the first time in this region45. Standardized measurement methods throughout the study period were used and large sample sizes and multiple measurements led to high precision in estimating the prevalence and trends of different risk factors. However, there are some limitations. We only assessed these trends for 10 years. Although the sampling methods were representative of the Iranian population, there were some minor differences that were addressed using post-stratification weighting based on age, sex, region and province categories of population in 2011 as a reference for all years. Finally, the biochemical measurements were only available for three STEPs cycles.
Conclusion
Non-HDL lipids and blood pressure levels in the Iranian population improved significantly in those with and without diabetes. Moreover, obesity measurements and fasting plasma glucose worsened in diabetic persons. This study showed favorable changes in blood pressure, non-HDL cholesterol, blood glucose, and obesity (only in men) were more prominent in people with diabetes compared to those without known diabetes. This indicating secondary prevention efforts have been more effective than primary prevention in Iran.
Methods
This study is conducted on the data documented from five STEPwise approaches to Surveillance (STEPS) surveys (2007, 2008, 2009, 2011, and 2016). The first STEPS in 2005 was not included due to the inconsistency of some measurement methods. STEPS is a standardized survey designed to help the World Health Organization (WHO) member states collect and disseminate consistent data about non-communicable diseases (NCD) and enable comparisons over time. A brief explanation of the samplings of the surveys is presented as follows.
All methods in the current study were carried out following relevant guidelines and regulations, the Center for Disease Control, Ministry of Health and Medical Education in Iran approved all experimental protocols, and all participants gave informed consent.
Study population
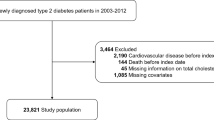
Using random cluster sampling methods based on instructions of WHO for STEPS45 23,487, 23,290, 23,334, 7551, and 23,738 adults, aged 25–65, were selected in 2007, 2008, 2009, 2011 and 2016, respectively. Despite differences in design and sampling methods, all surveys represented the Iranian population. Socio-demographic information and physical measurements were collected in all five surveys, whereas biochemical measurements were collected only in 2007, 2011 and 2016.
The sampling method in 2007, 2008 and 2009 was similar. The sampling was conducted at levels of towns, villages and districts of large cities using a randomized cluster sampling scheme. In each province, 1000 individuals were selected in 50 clusters. Each cluster included 20 individuals, 10 women and 10 men, living in neighboring households.
The 2011 survey used a multistage cluster random sampling scheme. At the first stage, distinct counties or a group of adjacent counties were listed as the primary sampling units (PSU). Fifty PSUs were then picked by applying probability proportionate to size (PPS) random sampling. Within each PSU, urban and rural areas were listed as possible secondary sampling units (SSU) from which twelve SSUs were picked by employing the PPS method similar to the previous step. In the third stage, a list of households in each SSU referenced by their 10-digit postal codes was developed, of which twenty postal addresses were selected randomly. At the final stage, one individual was selected from each selected household using Kish tables provided by WHO, and they were interviewed at their houses.
In 2016, a systematic cluster random sampling scheme was designed to select 31,050 individuals in 3105 clusters (10 subjects from each cluster) from urban and rural areas of all provinces. To estimate the minimum sample size at the province level, calculations were based on the province with the lowest population density. The sample size in other provinces was determined according to their population ratio to that province. To control non–response errors and mind the effect of sampling design, 10% was added to the estimated sample size of each province. Also, to minimize costs, in more crowded provinces (those with more than 800 clusters), half of the estimated sample size was considered, but the applied weight in the subsequent analysis was doubled.
Medical history, clinical examination and laboratory measurements
Standard questionnaires based on the WHO STEPS were used to collect demographic information as well as the past medical history of diabetes, medication use and cigarette smoking. Blood pressure was measured three times at five-minute intervals. The average of second and third readings was considered as the participants' blood pressure.
All biochemical measurements were assessed in venous samples drawn after 12–14 h overnight fasting according to a standard protocol and sent to collaborating centers. In 2007 and 2011, Fasting Plasma Glucose (FPG) was measured with enzymatic colorimetric methods with a glucose oxidase test and serum lipids, including total cholesterol, high-density lipoprotein (HDL) cholesterol and triglycerides were determined by enzymatic methods (Pars Azmun, Karaj, Iran). In 2016, venous samples were transferred to the Central Reference Laboratory in Tehran and all laboratory tests were measured using the auto analyzer (Cobas C311 Hitachi High–Technologies Corporation) approved by Reference Laboratory. Low-density lipoprotein (LDL) cholesterol was calculated by the modified Friedewald equation to be consistent among all STEPS surveys46.
Definition of terms
Known diabetes was defined as a positive response to either of the two following questions: (1) “Have you ever been told by a doctor or other health worker that you have diabetes?” and (2) “Are you currently taking insulin or oral medication for diabetes prescribed by a doctor or other health worker?”. Hypertension goal/optimum level was defined as mean systolic blood pressure (SBP) < 140 mmHg or mean diastolic blood pressure (DBP) < 90 mmHg47. Participants who smoked cigarettes daily were considered 'daily smokers'. Glycemic control was defined as a goal of FPG < 130 mg/dL in diabetic subjects and an optimum level of FPG < 100 mg/dL in non-diabetic subjects. Goals/optimum levels for non-HDL cholesterol and LDL cholesterol were defined as non-HDL cholesterol < 130 mg/dl and LDL cholesterol < 100 mg/dl in those with known diabetes and non-HDL cholesterol < 160 mg/dl and LDL cholesterol < 130 mg/dL in those without known diabetes. Goals/optimum levels for HDL cholesterol were defined as ≥ 50 mg/dl for women and ≥ 40 mg/dl for men and for triglycerides were defined as triglyceride < 150 mg/dl in both genders47,48.
Statistical analysis
Characteristics of the study population were described by mean (SE) values for continuous variables and frequency (%) for categorical variables after accounting for the survey nature of the data. Since about 10% of the data were missed, the multiple imputation method was used for the estimation of missing information. Five imputation sets were performed to impute missing information of FPG, TG, total cholesterol, BMI, and blood pressure, using sex, area of living, and age as axillary variables. Survey analysis was performed in Stata ver. 12 and the results of all STEPS were weighted using "poststratum weights" according to the national Iranian census in 2011; "poststrata" was defined based on categories of age (25–44 years, 45–64 years), sex, residential area (rural, urban) and the provinces; in this way, the results of all STEPS would be comparable.
The trend of prevalence rates and averages of risk factors in diabetic and non-diabetic subjects were examined separately using logistic and linear regressions. The interaction between the trend of risk factors and diabetes status was evaluated by adding the interaction term of time × diabetes to the models in pooled data from diabetic and non-diabetic subjects.
References
Baena-Díez, J. M. et al. Risk of cause-specific death in individuals with diabetes: a competing risks analysis. Diabetes Care 39, 1987–1995. https://doi.org/10.2337/dc16-0614 (2016).
U. K. Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ 317, 703–713 (1998).
Pan, A., Wang, Y., Talaei, M. & Hu, F. B. Relation of smoking with total mortality and cardiovascular events among patients with diabetes mellitus: a meta-analysis and systematic review. Circulation 132, 1795–1804. https://doi.org/10.1161/CIRCULATIONAHA.115.017926 (2015).
Betteridge, D. J. Lipid control in patients with diabetes mellitus. Nat. Rev. Cardiol. 8, 278–290. https://doi.org/10.1038/nrcardio.2011.23 (2011).
Collins, R. et al. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet 361, 2005–2016. https://doi.org/10.1016/s0140-6736(03)13636-7 (2003).
Hansson, L. et al. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. HOT Study Group. Lancet 351, 1755–1762. https://doi.org/10.1016/s0140-6736(98)04311-6 (1998).
Shepherd, J. et al. Effect of lowering LDL cholesterol substantially below currently recommended levels in patients with coronary heart disease and diabetes: the Treating to New Targets (TNT) study. Diabetes Care 29, 1220–1226. https://doi.org/10.2337/dc05-2465 (2006).
Ali, M. K. et al. Achievement of goals in U.S. diabetes care, 1999–2010. N. Engl. J. Med. 368, 1613–1624. https://doi.org/10.1056/NEJMsa1213829 (2013).
Saydah, S. H., Fradkin, J. & Cowie, C. C. Poor control of risk factors for vascular disease among adults with previously diagnosed diabetes. JAMA 291, 335–342. https://doi.org/10.1001/jama.291.3.335 (2004).
Jahangiri-Noudeh, Y. et al. Trends in cardiovascular disease risk factors in people with and without diabetes mellitus: a Middle Eastern cohort study. PLoS ONE 9, e112639. https://doi.org/10.1371/journal.pone.0112639 (2014).
Kheirandish, M. et al. Secular trends in serum lipid levels of a Middle Eastern adult population; 10 years follow up in Tehran lipid and glucose study. Lipids Health Dis. 13, 20. https://doi.org/10.1186/1476-511X-13-20 (2014).
Eslami, A., Lotfaliany, M., Akbarpour, S., Azizi, F. & Hadaegh, F. Trend of cardiovascular risk factors in the older Iranian population: 2002–2014. Geriatrics Gerontol. Int. 18, 130–137. https://doi.org/10.1111/ggi.13154 (2018).
Farzadfar, F. et al. National, regional, and global trends in serum total cholesterol since 1980: systematic analysis of health examination surveys and epidemiological studies with 321 country-years and 3.0 million participants. Lancet 377, 578–586. https://doi.org/10.1016/S0140-6736(10)62038-7 (2011).
Zhou, B. et al. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet 389, 37–55. https://doi.org/10.1016/s0140-6736(16)31919-5 (2017).
Azizi, F. et al. Metabolic health in the Middle East and north Africa. Lancet Diabetes Endocrinol. https://doi.org/10.1016/S2213-8587(19)30179-2 (2019).
Sun, X. & Du, T. Trends in cardiovascular risk factors among U.S. men and women with and without diabetes, 1988–2014. BMC Public Health 17, 893. https://doi.org/10.1186/s12889-017-4921-4 (2017).
Preis, S. R. et al. Trends in cardiovascular disease risk factors in individuals with and without diabetes mellitus in the Framingham Heart Study. Circulation 120, 212–220. https://doi.org/10.1161/circulationaha.108.846519 (2009).
Samaranayaka, S. & Gulliford, M. C. Trends in cardiovascular risk factors among people with diabetes in a population based study, Health Survey for England 1994–2009. Primary Care Diabetes 7, 193–198. https://doi.org/10.1016/j.pcd.2013.04.010 (2013).
Karam, C. et al. Trends in cardiovascular disease risk factor prevalence and estimated 10-year cardiovascular risk scores in a large untreated French Urban Population: the CARVAR 92 study. PLoS ONE 10, e0124817. https://doi.org/10.1371/journal.pone.0124817 (2015).
Hata, J. et al. Secular trends in cardiovascular disease and its risk factors in Japanese: half-century data from the Hisayama Study (1961–2009). Circulation 128, 1198–1205. https://doi.org/10.1161/circulationaha.113.002424 (2013).
Carroll, M. D. et al. Trends in serum lipids and lipoproteins of adults, 1960–2002. JAMA 294, 1773–1781 (2005).
Carroll, M. D., Kit, B. K., Lacher, D. A., Shero, S. T. & Mussolino, M. E. Trends in lipids and lipoproteins in US adults, 1988–2010. JAMA 308, 1545–1554 (2012).
Manne-Goehler, J. et al. Health system performance for people with diabetes in 28 low-and middle-income countries: A cross-sectional study of nationally representative surveys. PLoS Med. 16, e1002751 (2019).
Torabi, P., Zare, F., Shekholeslam, R. & Safavi, S. M. in 12th Nutritional Congress. Tabriz; Iran.
Mohammadifard, N. et al. Improvement of dietary oil consumption following a community trial in a developing country: The role of translational research in health promotion. ARYA Atherosclerosis 9, 29–37 (2013).
Jafari, M., Mohammadi, M., Ghazizadeh, H. & Nakhaee, N. Feasibility and outcome of reducing salt in bread: a community trial in Southern Iran. Global J. Health Sci. 8, 163. https://doi.org/10.5539/gjhs.v8n12p163 (2016).
Esteghamati, A. et al. Physical activity in Iran: results of the third national surveillance of risk factors of non-communicable diseases (SuRFNCD-2007). J. Phys. Activity Health 8, 27–35 (2011).
Momenan, A. A., Delshad, M., Mirmiran, P., Ghanbarian, A. & Azizi, F. Leisure time physical activity and its determinants among adults in Tehran: Tehran Lipid and Glucose Study. Int. J. Prevent. Med. 2, 243–251 (2011).
Primatesta, P., Falaschetti, E., Gupta, S., Marmot, M. G. & Poulter, N. R. Association between smoking and blood pressure: evidence from the health survey for England. Hypertension 37, 187–193. https://doi.org/10.1161/01.hyp.37.2.187 (2001).
Venkatesan, A., Hemalatha, A., Bobby, Z., Selvaraj, N. & Sathiyapriya, V. Effect of smoking on lipid profile and lipid peroxidation in normal subjects. Indian J. Physiol. Pharmacol. 50, 273–278 (2006).
Derakhshan, A. et al. Sex specific incidence rates of type 2 diabetes and its risk factors over 9 years of follow-up: Tehran Lipid and Glucose Study. PLoS ONE 9, e102563. https://doi.org/10.1371/journal.pone.0102563 (2014).
Mooy, J. M. et al. Prevalence and determinants of glucose intolerance in a Dutch caucasian population. The Hoorn Study. Diabetes Care 18, 1270–1273. https://doi.org/10.2337/diacare.18.9.1270 (1995).
Wilson, P. W., Anderson, K. M., Harris, T., Kannel, W. B. & Castelli, W. P. Determinants of change in total cholesterol and HDL-C with age: the Framingham Study. J. Gerontol. 49, M252-257. https://doi.org/10.1093/geronj/49.6.m252 (1994).
Azizi, F. et al. Determinants of serum HDL-C level in a Tehran urban population: the Tehran Lipid and Glucose Study. Nutr. Metab. Cardiovasc. Dis. NMCD 12, 80–89 (2002).
Farahmand, M., Tehrani, F. R., Amiri, P. & Azizi, F. Barriers to healthy nutrition: perceptions and experiences of Iranian women. BMC Public Health 12, 1064. https://doi.org/10.1186/1471-2458-12-1064 (2012).
Enjezab, B., Farajzadegan, Z., Taleghani, F. & Aflatoonian, A. Internal motivations and barriers effective on the healthy lifestyle of middle-aged women: A qualitative approach. Iran. J. Nurs. Midwifery Res. 17, 390–398 (2012).
Kelishadi, R. et al. Barriers to physical activity in a population-based sample of children and adolescents in Isfahan, Iran. Int. J. Prevent. Med. 1, 131–137 (2010).
Farahmand, M. et al. What are the main barriers to healthy eating among families? A qualitative exploration of perceptions and experiences of Tehranian men. Appetite 89, 291–297. https://doi.org/10.1016/j.appet.2015.02.025 (2015).
Harati, H. et al. Reduction in incidence of type 2 diabetes by lifestyle intervention in a middle eastern community. Am. J. Prevent. Med. 38, 628–636 e621. https://doi.org/10.1016/j.amepre.2010.03.003 (2010).
Sarrafzadegan, N. et al. Do lifestyle interventions work in developing countries? Findings from the Isfahan Healthy Heart Program in the Islamic Republic of Iran. Bull. World Health Organ. 87, 39–50. https://doi.org/10.2471/blt.07.049841 (2009).
Noshad, S., Afarideh, M., Heidari, B., Mechanick, J. I. & Esteghamati, A. Diabetes care in Iran: where we stand and where we are headed. Ann. Global Health 81, 839–850. https://doi.org/10.1016/j.aogh.2015.10.003 (2015).
Shakibazadeh, E. et al. Patients’ perspectives on factors that influence diabetes self-care. Iran. J. Public Health 40, 146–158 (2011).
Shakibazadeh, E., Bartholomew, L. K., Rashidian, A. & Larijani, B. Persian Diabetes Self-Management Education (PDSME) program: evaluation of effectiveness in Iran. Health Promot. Int. 31, 623–634. https://doi.org/10.1093/heapro/dav006 (2016).
Niroomand, M. et al. Diabetes knowledge, attitude and practice (KAP) study among Iranian in-patients with type-2 diabetes: a cross-sectional study. Diabetes Metab. Syndr 10, S114-119. https://doi.org/10.1016/j.dsx.2015.10.006 (2016).
World Health Organization. NCDs | STEPwise approach to surveillance (STEPS), <https://www.who.int/ncds/surveillance/steps/en/> (2019).
Chen, Y. et al. A modified formula for calculating low-density lipoprotein cholesterol values. Lipids Health Dis. 9, 52. https://doi.org/10.1186/1476-511X-9-52 (2010).
American Diabetes, A. Standards of medical care in diabetes-2017 abridged for primary care providers. Clin. Diabetes 35, 5–26. https://doi.org/10.2337/cd16-0067 (2017).
Association, A. D. 6. Glycemic targets: standards of medical care in diabetes—2019. Diabetes Care 42, S61–S70 (2019).
Acknowledgements
We appreciate NCD office at the Ministry of Health and NCD Research Center, Tehran University of Medical Sciences for preparing the STEPS data.
Author information
Authors and Affiliations
Contributions
H.M., M.L. and D.K. carried out the initial analysis and interpretation of data and drafted the manuscript. D.K. and F.H. supervised the study and approved the contents of the manuscript. A.O. and M.Y. coordinated and supervised the STEPS surveys and F.F. and F.A. critically reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Malekzadeh, H., Lotfaliany, M., Ostovar, A. et al. Trends in cardiovascular risk factors in diabetic patients in comparison to general population in Iran: findings from National Surveys 2007–2016. Sci Rep 10, 11724 (2020). https://doi.org/10.1038/s41598-020-68640-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-68640-9
This article is cited by
-
Type 2 diabetes mellitus and In-hospital Major Adverse Cardiac and Cerebrovascular Events (MACCEs) and postoperative complications among patients undergoing on-pump isolated coronary artery bypass surgery in Northeastern Iran
BMC Cardiovascular Disorders (2023)
-
Detection of high risk people for diabetes by American diabetes association risk score in PERSIAN Guilan cohort study
BMC Endocrine Disorders (2023)
-
The trend of 10-year cardiovascular risk among diabetic and non-diabetic participants in Tehran Lipid and glucose study: 1999–2018
BMC Public Health (2022)
-
Prevalence and trends of coronary artery disease risk factors and their effect on age of diagnosis in patients with established coronary artery disease: Tehran Heart Center (2005–2015)
BMC Cardiovascular Disorders (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
