
Abstract
In sarcopenic obesity, the importance of evaluating muscle and fat mass is unquestionable. There exist diverse quantification methods for assessing muscle and fat mass by imaging techniques; thus these methods must be standardized for clinical practice. This study developed a quantification software for the body composition imaging using abdominal magnetic resonance (MR) images and compared the difference between sarcopenic obesity and healthy controls for clinical application. Thirty patients with sarcopenic obesity and 30 healthy controls participated. The quantification software was developed based on an ImageJ multiplatform and the processing steps are as follows: execution, setting, confirmation, and extraction. The variation in the muscle area (MA), subcutaneous fat area (SA), and visceral fat area (VA) was analyzed with an independent two sample T-test. There were significant differences in SA (p < 0.001) and VA (p = 0.011), whereas there was no difference in MA (p = 0.421). Regarding the ratios, there were significant differences in MA/SA (p < 0.001), MA/VA (p = 0.002), and MA/(SA + VA) (p < 0.001). Overall, intraclass correlation coefficients were higher than 0.9, indicating excellent reliability. This study developed customized sarcopenia-software for assessing body composition using abdominal MR images. The clinical findings demonstrate that the quantitative body composition areas and ratios can assist in the differential diagnosis of sarcopenic obesity or sarcopenia.
Similar content being viewed by others
Introduction
The term ‘sarcopenic obesity’ has been proposed to identify obesity with low skeletal muscle function and mass1. The current definitions of sarcopenic obesity combine sarcopenia [which was registered in the International Classification of Diseases (ICD-10-CM) in 2016]2 as defined through variable criteria, with the presence of obesity either defined as body mass index (BMI) or adiposity levels3,4,5,6. To date, there has been growing interest in sarcopenic obesity or sarcopenia. Several studies have reported that sarcopenia is closely associated with obesity7,8, physical disorders, a decline in quality of life9, metabolic complications, disease incidence10,11, and in particular, the treatment effects of cancer patients12,13. These studies indicate that more patients within the obese population have a weakened musculoskeletal system or increased fat mass in all age groups, and the risks and prevalence of sarcopenia increased with diseases such as liver fibrosis, obesity and metabolic syndrome7,8,11. However, current studies regarding the quantitative assessment of sarcopenia and/or sarcopenic obesity remain insufficient as diagnostic criteria and measurement techniques for muscle mass (or muscle loss) have not yet been established. Furthermore, it is unclear whether the specific mechanism of sarcopenic pathological responses involved in the decrement of muscle mass is aging14,15. Therefore, there is an unmet need for the establishment of a standardized method to assess muscle and fat mass.
Recent studies regarding diagnostic methods for sarcopenia or sarcopenic obesity have focused on the use of methods for the quantitative evaluation of body composition. Body composition imaging typically refers to the quantification of body fat and muscle mass, with evaluation methods including anthropometry, bioelectrical impedance analysis (BIA), and medical imaging16,17,18. Among these, the medical imaging techniques are regarded as the gold-standard in order to assess whole-body and specific regional muscle and fat mass. Medical imaging methods have included dual-energy X-ray absorptiometry (DEXA), computed tomography (CT), and magnetic resonance imaging (MRI). MRI, specifically shows great promise for quantifying the soft tissues including muscle, fat, nerve and ligaments and no ionizing radiation for patients19,20,21. There are only a few whole-body MRI studies focusing on quantification of actual body composition22,23. However, the application of whole-body MRI is restricted in clinical settings as the manual assessment of whole-body organ and tissue mass is time consuming. Several studies have investigated the use of single slices to estimate whole-body composition as an alternative method. Quantified composition on individual slices obtained at the lumbar spine showed a strong correlation with total visceral fat, subcutaneous fat and muscle mass24,25,26,27. Adipose tissue areas 5–10 cm above L4–L5 showed the strongest correlation with total visceral fat volume, whereas there was no association with subcutaneous fat areas. The area ~ 5 cm above L4–L5 was established as a predictor of total body-muscle volume28. In both genders, a single MRI scan at the level of the third lumbar spine (L3) is the best compromise as a site to assess total volume of visceral fat, subcutaneous fat and muscle24. Therefore, the use of single slice and automatic quantification software with a rapid processing time is useful for clinical implementation. Currently, there are few studies focusing on the quantification of body composition in sarcopenic obesity or sarcopenia.
For this study, we developed a semi-automatic quantification software for body composition imaging using abdominal MR images and compared the differences between sarcopenic obesity and healthy controls for clinical application.
Results
Patient characteristics
The averaged enzyme levels in both groups are shown in Table 1. The serum biochemistry showed significant differences between the two groups as follows: aspartate aminotransferase (AST, p < 0.001), alanine aminotransferase (ALT, p < 0.001), fasting glucose (p = 0.014) and triglycerides (TG, p < 0.001). However, there was no significant difference in γ-glutamyl transpeptidase (GGT, p = 0.249) or alkaline phosphatase (ALP, p = 0.170). Compared with those of healthy controls, these changes in serum levels can closely suggest the changes in the metabolic status such as those in sarcopenia and obesity.
Measurements of body composition contents using developed software
Five anonymized MRIs with the same slice at the L3 location (Fig. 1) were selected and provided to six reviewers. Each reviewer independently analyzed the major composition contents in sarcopenic obesity (i.e., muscle, subcutaneous fat, and visceral fat). Table 2 lists the processes for qualitative and quantitative analyses. Figure 2 demonstrates the graphic user interface (GUI) of the developed software and an example image for major composition contents. The mean time for quantifying muscle and fat areas was 20.84 min per image (range 19.56–21.84 min) for the original software and 3.24 min per image (range 2.86–3.36 min) for the developed software. The total processing time using the developed software was reduced by 6.43 times compared with the original software (84% reduced time: Fig. 3).

Abdominal MR images at third lumbar spine (L3, inside red-line) level.

The graphic user interface (GUI) of developed software ‘sarcopenia plug-in’ (upper) including of (A) ImageJ-platform basic menubar, (B) sarcopenia plug-in window, (C) region of interest (ROI) manager window and (D) result window. An example (lower) demonstrated the ROI extraction (inside yellow-line) for quantifying muscle, subcutaneous fat and visceral fat mass in a patient with sarcopenic obesity using developed ‘sarcopenia plug-in.’ The original ImageJ software (ver.1.51t, Java 1.8.0_191 64bits) is available at https://imagej.nih.gov/ij/.

Comparison of total processing time obtained from 6 independent reviewers using original software (Avg. 20.84 min) and developed software (Avg. 3.24 min).
Differentiation of muscle and fat mass in sarcopenic obesity
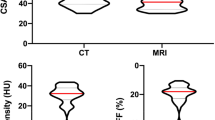
MR image data in 30 patients with sarcopenic obesity and 30 healthy controls were analyzed with the developed software. The averaged areas (A) and ratio of muscle (M), subcutaneous fat (S), and visceral fat (V) in two groups are summarized in Table 3. There were significant differences in the subcutaneous fat area (SA); (p < 0.001; Fig. 4B) and the visceral fat area (VA); (p = 0.011; Fig. 4C), whereas no significant difference was found in the muscle area (MA); (p = 0.421; Fig. 4A). In the ratios, there were significant differences in MA/SA (p < 0.001; Fig. 4D), MA/VA (p = 0.002; Fig. 4E), and MA/(SA + VA); (p < 0.001; Fig. 4F). Therefore, the ratios derived from muscle and fat areas are expected to be more powerful indexes for distinguishing sarcopenic obesity to healthy control.

Box plots demonstrated the areas of muscle (MA, A), subcutaneous fat (SA, B), visceral fat (VA, C) and the ratios as MA/SA (D), MA/VA (E), MA/(SA + VA) (F) in sarcopenic obesity and healthy control groups using developed software ‘sarcopenia plug-in’.
Inter-rater agreement
The interobserver variability in muscle and fat areas between 2 observers is summarized in Table 4. There was no significant difference between the averaged muscle and fat areas of the 2 observers. Overall, intraclass correlation coefficients (ICCs) were higher than 0.9, indicating an excellent reliability. The ICCs (range 0.952–0.994) were 0.977 for the measurements in sarcopenic obesity patients and 0.971 for the healthy control group, respectively. Therefore, the overall muscle and fat measurements of both observers showed an excellent agreement (p < 0.001).
Discussion
This study developed semi-automated software for assessing body composition on the basis of ImageJ. The study analyzed the difference between people with sarcopenic obesity and a healthy control group by measuring body composition areas from retrospective MRI datasets. In our study, abdominal MR images with 3-dimensional T1 high-resolution isotropic volume excitation (THRIVE) pulse sequence demonstrated good discrimination in diagnosing sarcopenic obesity patients (as SA and VA; p < 0.05). Moreover, the ratios of muscle and fat areas with better discrimination are MA/SA, MA/VA and MA/(SA + VA) (p ≤ 0.002) compared to areas. Therefore, our findings demonstrate that the areas & ratios of muscle and fat composition quantified at the single slice level of L3 can be useful for diagnosing sarcopenic obesity.
This study investigated the reproducibility of inter-observer assessment. The muscle and fat areas measured by two observers were excellent with regard to inter-rater agreement (> 0.9), indicating reproducibility. Therefore, the sarcopenia software-based body composition measurements can be reproduced in clinical abdominal MR images. Compared with the original ImageJ program, the processing steps of developed software for quantification were simplified from 11 to 5 processes. Consequently, total processing times were greatly reduced to approximately 3 min per subject as shown in Fig. 2. Thus, our semi-automatic sarcopenia software with a rapid processing time would be beneficial for clinical implementation. Also, the advantage of the ImageJ program is that it is an open source platform based on the Java programming language. It provides high scalability through a Java plug-in and macro functionality. Further study is required, to test our software and other segmentation software such as the medical imaging interaction toolkit (MITK) and the imaging interaction toolkit (ITK). Further study could validate the performance efficacy of our software to measure voluminal muscle and fat in a similar manner and time.
With regard to our study design, this retrospective study used inclusive criteria on the basis of BMI29 and blood biochemistry from electrical health records (EHR) for enrollment of sarcopenic obesity patients. This retrospective enrollment may be considered a potential bias or variation. The potential risk factors in the selection of the patients (age, sarcopenic severity, gender and so on), the clinical conditions (initial management, drug type or dosage, treatment and etc.) and imaging setting (type of scanners/pulse sequences) or any combinations with the sources may represent bias. In the present study, the evaluation method for overweight obesity included the Korean standard BMI (> 25.0 kg/m2) in conjunction with elevated serum enzyme alanine aminotransferase (ALT) levels. The BMIs and ALT levels in the sarcopenic obesity group were higher than those in the healthy control group. Image-based fat quantification is well reflected in the differences in the subcutaneous and visceral fat in the patient group, but not in the MA. A recent study reported that T2 (or T2*-corrected) Dixon MRI and MR spectroscopy (MRS) techniques can provide reliable quantification of fat composition using proton density fat fraction (PDFF) and proton density water fraction (PDWF) while minimizing MR-specific effects30. Thus, this finding may be considered a good indicator for assessing the severity of obesity. Further cross-validation studies are essential in order to confirm the muscle/fat composition of a large cohort population together with other imaging methods.
This study had several limitations. First, our study dealt with middle aged subjects in both groups. Several studies reported that aging affects muscle mass and maximum muscular strength including individual differences10,11. In addition to the muscle/fat assessment, the volumetric muscle measurement and muscle composition must be quantitatively investigated as these factors can differ greatly between individuals. This depends on many confounding factors such as physical activity, smoking and nutrition31,32. However, in this study, there was no consideration for aging, physical activity, smoking and nutrition as potential variables, which could influence the evaluation of the muscle mass and muscular strength. Further correlative studies are essential in order to clarify the physiological responses and how those potential variables affect sarcopenic obesity. Moreover, we suggest a standardized study protocol/design with prospective, large-scale cohort investigations according to age group (20–60 years and above). Second, BMI assessment is the simplest method for assessing obesity. However, it is limited to evaluate actual body composition because the values are indirect indices based on body weight, height, and waist circumference (i.e., not the actual muscle and fat mass). The BMI cut-offs as criteria of overweight and obesity are different from those in the World Health Organization (WHO) Expert committee (25.0–29.9 kg/m2), the Western Pacific Regional Office (WPRO) of WHO (> 23.0 kg/m2), the Asia Pacific region (> 25.0 kg/m2) and other various countries16. Thus, a standardized index is required in order to accurately measure the actual amount of muscle and fat mass in patients with obesity or sarcopenia. To overcome this issue, we believe that our imaging-based quantification software could be a solution and could provide accurate muscle and fat information to physicians. Third, there is the issue of selecting a single slice at the L3 level for body composition measurement. Selecting a single slice instead of a whole-body MRI analysis may hold true in a cross-sectional study design. However, weight change estimates with a single slice cannot replace whole body assessments24,33. Thus, a single slice MR analysis should be carefully used to assess weight change in patients with sarcopenia. Also, MRI estimates of skeletal muscle mass are on mass rather than on tissue composition. The current issue of fat infiltration into muscle should be focused on actual muscle mass measurement. When compared with MRI, CT estimates include attenuation which provides further information of clinical relevance34. A solution could be a multivoxel MRS protocol for fat infiltration35. Fourth, most of the issues regarding sarcopenia relate to the skeletal muscles of the arms and legs (i.e., peripheral skeletal mass). This is again associated with the sequelae of sarcopenia, e.g., frailty. Thus, future studies must clarify the association between skeletal muscle estimates at L3 and the thigh.
In conclusion, this study developed a customized sarcopenia-software for assessment of body composition using abdominal MRI images. Our software has the advantages of use in an open source platform and a rapid quantification time for clinical application. The clinical findings demonstrate that the quantitative body composition data such as areas and ratios can assist in the differential diagnosis of obesity and in determining the ratios of muscle and fat. These could be considered as imaging biomarkers for sarcopenic obesity in clinical practice.
Subjects and method
Ethics statement
We conducted a retrospective study, which was approved by the institutional review board (IRB) of Wonkwang University Hospital. Written informed consent was exempted by the approval of Wonkwang University Hospital IRB committee due to the use of anonymous archival data including MRI data and the use of electronic health records for the application of the developed software. This study was conducted in accordance with the Helsinki Declaration and Good Clinical Practice.
Study population
In compliance with the legal guidelines on safety and IRB bioethics, a total of 60 subjects consisting of 30 obese patients with suspected sarcopenia (mean age 47.3 ± 19.4 years.) and 30 healthy controls (mean age 54.6 ± 17.2 years.) were enrolled in this study from January 2014 to April 201936. The individuals complained of fatigue and inactivity, and they appeared to be weaker than their maximum muscular strength. The Korean standard BMI (kg/m2) was used as the selection criteria29. Subjects were defined with the following BMI values in conjunction with serum enzyme levels37: suspected sarcopenic obesity group with an elevated serum ALT levels of (≥ 35 IU/L) and a BMI of at least 25.0 kg/m2; and a healthy control group with BMIs of 18.0–23.0 kg/m2 and a normal ALT level of (< 35 IU/L).
Magnetic resonance imaging
Abdominal MR images were acquired from a 3 T Achieva MRI system (Philips Healthcare, Best, The Netherlands) with an array coil with 32 receiver channels. The T1 high-resolution isotropic volume excitation (eTHRIVE) images were obtained with the following parameters: repetition time (TR)/echo time (TE) = 4.2/1.97 ms; field of view = 38 × 38 × 14 cm3; number of excitation = 2; slice thickness = 0.74 × 0.74 × 2.0 mm3; number of slices = 100; matrix size = 512 × 512 pixels; and scan time = 16 s.
Measurement of body compositions on 3rd lumbar spine MRI
To measure body compositions, this study chose a single slice analysis instead of a whole body MRI analysis with a cross sectional study design24,33. The L3 level image was selected as the position for quantitative analysis (Fig. 1). Not only are visceral and subcutaneous fat visible in this position, but also the seven major muscles (the psoas, erector spinae, quadratus lumborum, transversus abdominus, external and internal obliques, and rectus abdominus) can be identified. Moreover, this L3 level includes the spine, intestines, kidneys, and liver. Hence, it is a key position for observing various anatomical areas24,28, it is considered the most suitable position at which to analyze the relationship between various conditions and diseases including sarcopenia, aging, obesity, and osteoporosis38.
Software environment and software algorithm
In order to quantitatively analyze the muscle and fat mass in the patients with sarcopenic obesity, the software was developed on the open source ImageJ multiplatform software (ver.1.51t, Java 1.8.0_191 64bits), developed by the National Institutes of Health (NIH)39. To use the software, the Java standard edition (SE) Runtime Environment is required to be installed in advance. Table 2 lists the overall processes for qualitative and quantitative analyses on the original ImageJ software and the developed sarcopenia-specialized software. The main processes are divided into four steps (execution, setting, confirmation and extraction), and the existing 11 analysis processes in the original software are simplified into five processes in the developed software.
Data processing and quantification of MR images
The procedures for MRI data processing are comprised of four steps as follows: execution, setting, confirmation and extraction.
- (1)
The execution step.
MRI data are opened from the developed sarcopenia-software in this study and analysis tools specific to the quantification of body composition are implemented as shown in Fig. 2A. A L3 level image was chosen from the axial MR images in each patient to identify the ROIs of muscle, subcutaneous fat, and visceral fat.
- (2)
The setting step.
For the pre-processing of the MRI data, the selected MR image is set in the Window. The Leveling and Threshold values as shown in Fig. 2B (F1 function key button), and their values are applied to the MRI data. After the setting, the ROIs (as shown in Fig. 2C) corresponding to the muscle, subcutaneous fat and visceral fat are roughly drawn on the MR image using the drawing tools on menu bar (Fig. 2A).
- (3)
The confirmation step.
This is the step to confirm the final ROIs for each composition content (M, S, V) after modifying and verifying the ROIs. The final ROIs are generated from the overlaid areas between the roughly drawn ROIs and the regions within Threshold value. The function key buttons for generating the ROIs are as follows: F2 button for muscle (M), F3 button for subcutaneous fat (S) and F4 button for visceral fat (V), as shown in Fig. 2B.
- (4)
The extraction step
After the quantification of the body composition is completed for the confirmed ROIs from a physician (K.H.Y), the results are extracted into several file formats such as TIFF, PNG, JPG and BMP files. These files are used for the color-labeling of the ROI images, the ROI files for the confirmed ROIs, and the CSV files for the quantification data.
To compare the original software and developed software, five anonymized MRI images at the same slice of L3 location were selected and provided to six reviewers. Each reviewer independently analyzed the major composition contents in sarcopenia (i.e., muscle, subcutaneous fat, and visceral fat). They had no knowledge of the clinical outcome or access to the readings of the other reviewers. To assess the inter-observer variability of the measurements, both radiologists independently assessed the L3 images. The overall measurements for each patient were calculated as a mean and standard deviation of the areas.
Statistical analysis
The abdominal muscle and fat contents were compared with two independent groups using the statistical package for the social sciences program (SPSS ver. 20, Chicago, Illinois). The variation in muscle and fat contents was evaluated with an independent two sample T-test. Inter-rater agreement and reliability were estimated by calculating the intra-class correlation coefficient (ICC); (and a 95% confidence interval [CI]) between the muscle and fat areas for the same subject on the same system. The ICC values were considered as the basis to evaluate the level of reliability using the following guideline40: values less than 0.5 are indicative of poor reliability, values between 0.5 and 0.75 indicate moderate reliability, values between 0.75 and 0.9 indicate good reliability, and values greater than 0.90 indicate excellent reliability. Two-sided p values less than 0.05 were considered to indicate statistical significance in all tests.
References
Barazzoni, R. et al. Sarcopenic obesity: Time to meet the challenge. Clin. Nutr. 37, 1787–1793 (2018).
Lee, K. et al. Recent issues on body composition imaging for sarcopenia evaluation. Korean J. Radiol. 20, 205–217 (2019).
Prado, C. M., Wells, J. C., Smith, S. R., Stephan, B. C. & Siervo, M. Sarcopenic obesity: A critical appraisal of the current evidence. Clin. Nutr. 31, 583–601 (2012).
Santilli, V., Bernetti, A., Mangone, M. & Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 11, 177–180 (2014).
Boutin, R. D., Yao, L., Canter, R. J. & Lenchik, L. Sarcopenia: Current concepts and imaging implications. AJR Am. J. Roentgenol. 205, W255-266 (2015).
Batsis, J. A. et al. Variation in the prevalence of sarcopenia and sarcopenic obesity in older adults associated with different research definitions: Dual-energy X-ray absorptiometry data from the National Health and Nutrition Examination Survey 1999–2004. J. Am. Geriatr. Soc. 61, 974–980 (2013).
Lee, Y. H. et al. Sarcopenia is associated with significant liver fibrosis independently of obesity and insulin resistance in nonalcoholic fatty liver disease: Nationwide surveys (KNHANES 2008–2011). Hepatology 63, 776–786 (2016).
Batsis, J. A. & Villareal, D. T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat. Rev. Endocrinol. 14, 513–537 (2018).
Tsekoura, M., Kastrinis, A., Katsoulaki, M., Billis, E. & Gliatis, J. Sarcopenia and its impact on quality of life. Adv. Exp. Med. Biol. 987, 213–218 (2017).
Shafiee, G. et al. Prevalence of sarcopenia in the world: A systematic review and meta-analysis of general population studies. J. Diabetes Metab. Disord. 16, 21 (2017).
Zhang, H. et al. Association between sarcopenia and metabolic syndrome in middle-aged and older non-obese adults: A systematic review and meta-analysis. Nutrients 10, 364 (2018).
Park, S. E. et al. Sarcopenia is poor prognostic factor in older patients with locally advanced rectal cancer who received preoperative or postoperative chemoradiotherapy. Medicine 97, e13363 (2018).
Lee, S. J., Park, Y. J. & Cartmell, K. B. Sarcopenia in cancer survivors is associated with increased cardiovascular disease risk. Support. Care Cancer 26, 2313–2321 (2018).
Han, A., Bokshan, S. L., Marcaccio, S. E., DePasse, J. M. & Daniels, A. H. Diagnostic criteria and clinical outcomes in sarcopenia research: A literature review. J. Clin. Med. 7, 70 (2018).
Carvalho Nascimento, P. R., Poitras, S. & Bilodeau, M. How do we define and measure sarcopenia? Protocol for a systematic review. Syst. Rev. 7, 51 (2018).
Yoon, J. L., Cho, J. J., Park, K. M., Noh, H. M. & Park, Y. S. Diagnostic performance of body mass index using the Western Pacific Regional Office of World Health Organization reference standards for body fat percentage. J. Korean Med. Sci. 30, 162–166 (2015).
Almada-Correia, I., Neves, P. M., Makitie, A. & Ravasco, P. Body composition evaluation in head and neck cancer patients: A review. Front. Oncol. 9, 1112 (2019).
Marra, M. et al. Assessment of body composition in health and disease using bioelectrical impedance analysis (BIA) and dual energy X-ray absorptiometry (DXA): A critical overview. Contrast Media Mol. Imaging 2019, 3548284 (2019).
Dehlendorff, C., Andersen, K. K. & Olsen, T. S. Body mass index and death by stroke: No obesity paradox. JAMA Neurol. 71, 978–984 (2014).
Chrysant, S. G. & Chrysant, G. S. The single use of body mass index for the obesity paradox is misleading and should be used in conjunction with other obesity indices. Postgrad. Med. 131, 96–102 (2019).
Edmund, J. M. & Nyholm, T. A review of substitute CT generation for MRI-only radiation therapy. Radiat. Oncol. 12, 28 (2017).
Muller, M. J., Geisler, C., Pourhassan, M., Gluer, C. C. & Bosy-Westphal, A. Assessment and definition of lean body mass deficiency in the elderly. Eur. J. Clin. Nutr. 68, 1220–1227 (2014).
Bosy-Westphal, A., Braun, W., Schautz, B. & Muller, M. J. Issues in characterizing resting energy expenditure in obesity and after weight loss. Front. Physiol. 4, 47 (2013).
Schweitzer, L. et al. What is the best reference site for a single MRI slice to assess whole-body skeletal muscle and adipose tissue volumes in healthy adults?. Am. J. Clin. Nutr. 102, 58–65 (2015).
Maislin, G. et al. Single slice vs. volumetric MR assessment of visceral adipose tissue: Reliability and validity among the overweight and obese. Obesity 20, 2124–2132 (2012).
So, R. et al. Best single-slice measurement site for estimating visceral adipose tissue volume after weight loss in obese. Jpn. men. Nutr. Metab. 9, 56 (2012).
Demerath, E. W. et al. Approximation of total visceral adipose tissue with a single magnetic resonance image. Am. J. Clin. Nutr. 85, 362–368 (2007).
Shen, W. et al. Total body skeletal muscle and adipose tissue volumes: Estimation from a single abdominal cross-sectional image. J. Appl. Physiol. 97, 2333–2338 (2004).
Seo, M. H. et al. 2018 Korean society for the study of obesity guideline for the management of obesity in Korea. J. Obes. Metab. Syndr. 28, 40–45 (2019).
Grimm, A. et al. Repeatability of Dixon magnetic resonance imaging and magnetic resonance spectroscopy for quantitative muscle fat assessments in the thigh. J. Cachexia Sarcopenia Muscle 9, 1093–1100 (2018).
Laskou, F. & Dennison, E. Interaction of nutrition and exercise on bone and muscle. Eur. Endocrinol. 15, 11–12 (2019).
Chiolero, A., Faeh, D., Paccaud, F. & Cornuz, J. Consequences of smoking for body weight, body fat distribution, and insulin resistance. Am. J. Clin. Nutr. 87, 801–809 (2008).
Shen, W. et al. A single MRI slice does not accurately predict visceral and subcutaneous adipose tissue changes during weight loss. Obesity 20, 2458–2463 (2012).
Engelke, K., Museyko, O., Wang, L. & Laredo, J. D. Quantitative analysis of skeletal muscle by computed tomography imaging-State of the art. J. Orthop. Translat. 15, 91–103 (2018).
Forbes, S. C. et al. MRI/MRS evaluation of a female carrier of Duchenne muscular dystrophy. Neuromuscul. Disord. 22(Suppl 2), S111-121 (2012).
Han, K. et al. Sarcopenia as a determinant of blood pressure in older Koreans: Findings from the Korea National Health and Nutrition Examination Surveys (KNHANES) 2008–2010. PLoS ONE 9, e86902 (2014).
Bekkelund, S. I. & Jorde, R. Alanine aminotransferase and body composition in obese men and women. Dis. Markers 2019, 1695874 (2019).
Hirabayashi, H. et al. Characteristics of L3 nerve root radiculopathy. Surg. Neurol. 72, 36–40 (2009).
Schneider, C. A., Rasband, W. S. & Eliceiri, K. W. NIH image to ImageJ: 25 years of image analysis. Nat. Methods 9, 671–675 (2012).
Koo, T. K. & Li, M. Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 15, 155–163 (2016).
Acknowledgements
This study was supported by the grants of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare (HI18C1216), and the Technology Innovation Program or Industrial Strategic Technology Development Program (20001234).
Author information
Authors and Affiliations
Contributions
All authors contributed to this work. Conceived and designed the experiments: S.J.K., T.-H.K., C.-W.J., and K.-H.Y. Performed the experiments: S.J.K., C.S.L., S.H.N., and J.E.K. Analyzed the data: S.J.K., T.-H.K., C.S.L., S.H.N., and J.E.K. Interpreted the data: T.-H.K., C.-W.J., and K.-H.Y. Wrote the paper: S.J.K., T.-H.K., C.-W.J., and K.-H.Y.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kim, S., Kim, TH., Jeong, CW. et al. Development of quantification software for evaluating body composition contents and its clinical application in sarcopenic obesity. Sci Rep 10, 10452 (2020). https://doi.org/10.1038/s41598-020-67461-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-67461-0
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
