
Abstract
Increasing life expectancy and a growing share of older people around the world spotlight the issue of health during additional years of life. Research on trends of proportions of older people with activity limitations for low and middle income countries is sparse. We use data from the World Health Survey and the UN World Population Prospects to predict prevalence of activity limitations for 23 low and middle income countries for the upcoming 30 years. Our projections highlight huge variation in the proportion of older adults with limitations across investigated countries and this variation is not expected to diminish. However, these countries are facing considerable demographic changes and even though prevalence rates appear almost constant, absolute numbers are changing which require policy interventions. Furthermore, variations across countries reflect not only disparities in health conditions, but also differences in cultural peculiarities of reporting and historical perception of health.
Similar content being viewed by others


Introduction
For several decades upper-middle and high income countries are facing changes in their population compositions with shares of older adults increasing and shares of younger population declining. In many lower-middle and low income countries the proportion of young people remained high while life expectancy increased in particular within the last decade. Therefore, the proportion of unhealthy older adults may be expected to increase in those countries. However, additional life years are not necessarily spent with activity limitations but could also be spent in healthy conditions.
There are numerous studies on health trends in upper middle and high income countries. Studies on European countries and the United States showed an inconsistent pattern when it comes to health trends and disabilities. For instance, Jagger et al. identified only little changes in healthy life expectancy for Europeans1, while the trend in healthy life expectancy developed differently for the high and low educated population in the United States2. Lafortune and Balestat found similar results of an increasing, declining and even stable rates in disability among older adults from 12 OECD countries3,4. In the near future, the share of older adults with severe activity limitations in Europe is expected to remain constant, even though an increase in absolute numbers is expected5,6. These studies on upper middle and high income countries might guide some ideas about global future disability trends.
Research on health trends in low and middle income countries is sparse, although these countries are facing pronounced demographic changes in upcoming decades. A number of them, including China, the Russian Federation, and the Ukraine expect a considerable increase of the proportion of people at older ages7,8,9. Further, disability rates are higher in older age and moreover they are higher in low and middle income countries than in high income countries10,11. Studies show that the health status fell as the population grew older in low income countries in particular12 and that the total burden of disability increased by 52% between 1990 and 2017 due to aging population and noncommunicable diseases13. In Asia and the Pacific, fastest aging countries faced greatest increase in health dependencies14. Interestingly, in China disability prevalence is expected to decrease partly due to higher education and urbanization15. A study on Koreans aged at least 65 years also found a decline in disability rates during 1994 and 200416. However, results depend on the metric of disability17 and thresholds (e.g. mild disabilities versus severe disabilities)18.
This paper looks at the health status based on activity limitations of older adults across the world and forecasts the share of older adults with severe activity limitations for the upcoming 30 years in 23 low and middle income countries. In particular, we focus on males and females above age 50 applying an innovative methodology of forecasting5,19.
Results
Disparities in activity limitations across countries
Data on self-reported activity limitations provide a very heterogenous picture across low and middle income countries. For instance, in China only 2.4% of the female population in the age group 60–69 years reported severe activity limitations, whereas about 69% of their counterparts in Morocco reported those limitations (Table 1). The variation in prevalence of conditions with activity limitations was slightly more narrow for males then for females for all age categories. Pronounced differences are also observed between sexes in some countries. In general, less men reported activity limitations than their female counterparts (Table 1). However, it is important to note, that pronounced differences in prevalence of severe activity limitations among selected countries might be to a large extent attributed to the different style of reporting subjective conditions of activity limitations.
Trends in ratio of activity limitations free life expactancy to life expectancy
Our random coefficient regression showed a decline in the ratio of activity limitations free life expectancy to life expectancy by age, as expected, and an overall smaller ratio for women than for men (Table 2). Moreover, the country estimates for men and women indicated a slightly bigger variation in logit(r) across countries for women with a variance of 0.53 and 0.49 for men (Table 2). More reproducible, we present estimates of the random country effects, which highlight the difference in country effects by gender with an SD of 0.73 for women and an SD of 0.71 for men (Table 3).
Forecasting severe activity limitations by 2047
Our projections show that the prevalence of 60+ year olds with severe activity limitations is expected to change very little in the next 30 years, among men showing a change of at most 2.1 percent points (Table 4) in particular. Thus, we can still expect about 50% of the male population above age 60 in Morocco to report severe activity limitations while we expect only about 2.6% of males in Uruguay to report similar conditions. The highest increase in the prevalence of activity limited adults can be expected for the population of females 60+ in Mauritius. It will increase from 27% in 2017 to 30% in 2047 (Table 4).
Ages with similar prevalence
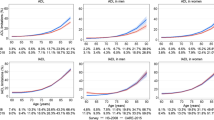
Our results also demonstrate a large variation across countries in comparing ages when a fixed level of prevalence is reached. We estimated the ages when 25% prevalence of activity limitations was attained. On average, every fourth woman was expected to report severe activity limitations at the age of only 51 years in India, 55 years in Georgia, and 57 years in Turkey in 2017. In contrast, every fourth woman in China, Ecuador, and Malaysia at the age of 80 and above reported activity limitations. Hence, they considered themselves having the same level of activity limitations at higher ages than their counterparts in India and Georgia at younger ages (Table 5, Fig. 1). This pattern won’t change much within the upcoming 30 years (Table 5, Fig. 2). Since at each age in most cases men report less activity limitations than women, it is not a surprise that 25% prevalence rate was reached by men at higher ages then by women. Nevertheless, we still find quite some differences across countries (Table 5, Fig. 1) with every fourth man in Tunisia and Georgia aged about 60 reporting activity limitations while the same rate was reached by men in Malaysia and China at about 90 years in 2017.

Men’s and women’s age at which 25% prevalence rate of living with severe activity limitations is attained in 2017 by country.

Men’s and women’s age at which 25% prevalence rate of living with severe activity limitations is attained in 2047 by country.
Discussion
In this analysis of WHO and United Nations data, we studied self-reports in activity limitations of older adults in 23 low and middle income countries. Our results showed that prevalence rates of older adults with severe activity limitations vary considerably across countries, as well as within countries between sexes.
Of course to a large extent this difference in reporting activity limitations reflects s not only health conditions in the countries, but also a different style of reporting which might be due to the cultural and historical perception of health20,21,22,23. However, different health measures show a varying magnitude in reporting bias21. Previous research on reporting mobility difficulties support our results showing significant cultural differences in self-reports of older adults from low- and middle income countries20. Further, differences across European countries in self-reported health measures suggested cultural differences in reporting styles in addition to differences in other national factors5,19,24. The reasons for cultural differences in reporting might be manifold. For instance, the threshold for reporting difficulties in activities might vary across cultures as it was shown for reporting difficulties in walking25. Moreover, culture influences the value of health, which corresponds with health promoting life styles shown for Taiwanese and American adolescents26. We further speculate that cultures with a higher value of health might also correspond to a lower threshold for reporting health limitations, thus this might lead to more reports than in other countries with a lower value of health and higher thresholds. Nevertheless, research on determinants of cultural differences in self-reports is sparse, for low and middle income countries in particular. Thus, we should not pay too much attention to the level of prevalence. Instead we should compare the dynamics of prevalence in each particular country.
Our major important finding shows for the first time that despite expected increases in life expectancy in all selected countries, the prevalence rate of people living with severe activity limitations is expected to change very little over time. However, the absolute number of people with activity limitations will still increase with the increase in older adults.
Previous studies have investigated trends in disabilities and activity limitations of older adults for high income countries such as Singapore, the United States and European countries5,27,28,29. Their findings were similar to our results on low and middle income countries expecting a constant prevalence rate, but an increase in absolute numbers.
In addition, we also highlighted the ages with the same prevalence rates as age might be a more common metric. When comparing ages with the same prevalence of severe activity limitations we observe considerable variations. For instance in 2017 79-year old women in Mexico demonstrate the same prevalence rate in activity limitations as their 51 year old counterparts in India. However, one should also be cautious in comparing different countries since the same argument that is mentioned above about different culture in reporting can be applied here. Further research on objective measures need to be conducted to exclude a potential cultural reporting bias.
Methods
Data source
In this study we used two different data sources: the World Health Organization’s World Health Survey and the United Nations World Population Prospects 2017. The World Health Survey (WHS)30 was conducted once in 2002–2004 to monitor the health outcomes of the population aged 18 years and above in more than 70 countries. We use the national representative survey data for low and middle income countries (World Bank classification 2003)31, which provide information on self-perceived activity limitations within the last month prior to their interview. The WHS includes the most recent available data enabling comparable international investigations on activity limitations, health and aging32,33. We excluded some countries due to sample size issues and reliability and ended up with a sample of 23 countries.
In addition to the WHS survey data source, we used sex specific abridged life tables for the period 2000–2050 from the United Nations9. Country specific population estimates and projected population trends were also retrieved from the United Nations World Population Prospects 2017. We used the population projections for 23 selected countries from the medium scenario by sex and 5-year age groups for the period 2015 to 2050.
Health status
Our analysis is based on the responses to the WHS question related to self-perceived activity limitations. In the survey the question was asked: “Overall in the last 30 days, how much difficulty did you have with work or household activities?”. Participants could rate their response ranging from none, mild, moderate to severe, and extreme/ cannot do. We dichotomized the responses into no severe limitations (combining the response categories none, mild and moderate), and severe limitations (merging severe and extreme limitations). This health question is very similar to the well acknowledged Global Activity Limitation Indicator (GALI) except of the investigation period of one month instead of six months34,35. The validity and reliability of GALI is verified by several studies not only on an European population but also on an Asian population36,37.
Statistical analysis
For each country we calculated the prevalence of people without severe activity limitations by 5-year age groups and for a first descriptive overview also by three selected 10-year age groups. Time of the survey was 2003. Sample weights were applied to account for non-response and to allow nationally representativeness for non-institutionalized population. We applied Sullivan’s method38 to compute activity limitations free life expectancy (HLE) for each country by sex and 5-year age groups and computed r, the ratio of activity limitations free life expectancy to life expectancy1,5,19.
In our analysis, we excluded outliers in r that fell outside of three standard deviations (SD) in the initial estimation, which might be due to a very low sample size within a particular sex-specific age group within a country. This was necessary for some observations of the 85+ population and the age group 80–84 (in total 11 observations out of 598). We identified a significant random variation in the logit(r) with likelihood ratio tests, which supported the applied random coefficient models. We run the following random coefficient model:
considering a linear and quadratic effect of age on the logit(r); with i indicating the first level and c the country (second level). Further, following earlier research on European data5,19, our regressions did not consider changes of ric over time, however changes in life expectancy over time are accounted for by using life tables through 2050. Thus, the ratio of HLE to life expectancy was assumed to remain constant over time, which means that increases in life expectancy occur together with increases in HLE. In all countries investigated life expectancy is expected to increase. In a next step, we used the remaining life expectancies by age from the life tables provided by the United Nations9 to project HLE by sex, age, and country and prevalence of activity limitations subsequently. We estimated country, sex and age specific \({\bar{r}}_{ic}\) considering also the random variation by sex across countries. Next, we projected the share of older men and women with severe activity limitations from 2017 to 2047 for all 23 countries using sex specific population projections provided by the United Nations9.
Finally, we employed the constant characteristic age approach introduced by Sanderson and Scherbov39, which enabled comparisons on the very common age metric. Fixing 25% prevalence in severe activity limitations for each sex and country we estimated the age at which this level of prevalence was attained. These estimates were produced for 2017 and 2047.
Data availability
The World Health Survey (WHS) data that support the findings of this study are available from the Central Data Catalog of the World Health Organisation (http://apps.who.int/healthinfo/systems/surveydata/index.php/catalog/whs). UN World Population Prospects data can be obtained from the United Nations (https://population.un.org/wpp/Download/Standard/Population/).
References
Jagger, C. et al. Mind the gap—reaching the European target of a 2-year increase in healthy life years in the next decade. Eur. J. Public Health 23, 829–833 (2013).
Crimmins, E. M. & Saito, Y. Trends in healthy life expectancy in the United States, 1970-1990: Gender, racial, and educational differences. Soc. Sci. Med. 52, 1629–1641 (2001).
Lafortune, G. & Balestat, G. Trends in Severe Disability Among Elderly People: Assessing the Evidence in 12 OECD Countries and the Future Implications, https://doi.org/10.1787/217072070078 (2007).
Lafortune, G., Balestat, G. & Disability Study Expert Group Members. Trends in Severe Disability Among Elderly People: Assessing the Evidence in 12 OECD Countries and the Future Implications, http://www.oecd-ilibrary.org/docserver/download/217072070078.pdf?expires=1493904995&id=id&accname=guest&checksum=A7644043C4C60F5072361208FE3AE6E5 (2007).
Scherbov, S. & Weber, D. Future trends in the prevalence of severe activity limitations among older adults in Europe: a cross-national population study using EU-SILC. BMJ Open 7, e017654 (2017).
Guzman-Castillo, M. et al. Forecasted trends in disability and life expectancy in England and Wales up to 2025: a modelling study. Lancet Public Health 2, e307–e313 (2017).
Scherbov, S. et al. Russian Demographic Data Sheet 2019, http://pure.iiasa.ac.at/15652 (2019).
United Nations. World Population Ageing 2019, https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (2019).
UN. World Population Prospects: The 2017 Revision, http://esa.un.org/unpd/wpp/ (2017).
Mitra, S. & Sambamoorthi, U. Disability prevalence among adults: estimates for 54 countries and progress toward a global estimate. Disabil. Rehabil. 36, 940–947 (2014).
World Report on Disability 2011. (World Health Organization, 2011).
Chatterji, S., Byles, J., Cutler, D., Seeman, T. & Verdes, E. Health, functioning, and disability in older adults–present status and future implications. Lancet Lond. Engl. 385, 563–575 (2015).
Findings from the Global Burden of Disease Study 2017. (IHME, 2018).
Chomik, R., McDonald, P. & Piggott, J. Population ageing in Asia and the Pacific: Dependency metrics for policy. J. Econ. Ageing 8, 5–18 (2016).
Lu, B., Liu, X. & Yang, M. A Budget Proposal for China’s Public Long-Term Care Policy. J. Aging Soc. Policy 29, 84–103 (2017).
Jang, S.-N., Cho, S. & Kawachi, I. Is socioeconomic disparity in disability improving among Korean elders? Soc. Sci. Med. 71, 282–287 (2010).
Ofstedal, M. B. et al. Short-term trends in functional limitation and disability among older Asians: a comparison of five Asian settings. J. Cross-Cult. Gerontol. 22, 243–261 (2007).
Crimmins, E. M. Trends in the health of the elderly. Annu. Rev. Public Health 25, 79–98 (2004).
Sanderson, W. C. & Scherbov, S. Remeasuring aging. Science 329, 1287–1288 (2010).
Capistrant, B. D., Glymour, M. M. & Berkman, L. F. Assessing mobility difficulties for cross-national comparisons: results from the World Health Organization Study on Global AGEing and Adult Health. J. Am. Geriatr. Soc. 62, 329–335 (2014).
Spitzer, S. & Weber, D. Reporting biases in self-assessed physical and cognitive health status of older Europeans. PLOS ONE 14, e0223526 (2019).
Crossley, T. F. & Kennedy, S. The reliability of self-assessed health status. J. Health Econ. 21, 643–658 (2002).
Coman, L. & Richardson, J. Relationship between self-report and performance measures of function: a systematic review. Can. J. Aging Rev. Can. Vieil. 25, 253–270 (2006).
Hardy, M. A., Acciai, F. & Reyes, A. M. How Health Conditions Translate into Self-Ratings: A Comparative Study of Older Adults across Europe. J. Health Soc. Behav. 55, 320–341 (2014).
Melzer, D., Lan, T.-Y., Tom, B. D. M., Deeg, D. J. H. & Guralnik, J. M. Variation in thresholds for reporting mobility disability between national population subgroups and studies. J. Gerontol. A. Biol. Sci. Med. Sci. 59, 1295–1303 (2004).
Chen, M.-Y., James, K. & Wang, E. K. Comparison of health-promoting behavior between Taiwanese and American adolescents: a cross-sectional questionnaire survey. Int. J. Nurs. Stud. 44, 59–69 (2007).
Thompson, J. et al. Projecting the number of older singaporeans with activity of daily living limitations requiring human assistance through 2030. Ann. Acad. Med. Singap. 43, 51–56 (2014).
Choi, H., Schoeni, R. F. & Martin, L. G. Are Functional and Activity Limitations Becoming More Prevalent among 55 to 69-Year-Olds in the United States? PLOS ONE 11, e0164565 (2016).
Rosenberg, M. W. & Moore, E. G. The health of Canada’s elderly population: current status and future implications. Can. Med. Assoc. J. 157, 1025–1032 (1997).
WHO. WHO World health survey. WHO, http://www.who.int/healthinfo/survey/en/ (2004).
World Development Indicators 2003. (World Bank Group, 2003).
Beard, J. R. et al. The World report on ageing and health: a policy framework for healthy ageing. The Lancet 387, 2145–2154 (2016).
Ofstedal, M. B. Data Sources for Health Expectancy Research. in International Handbook on Health Expectancies (eds. Jagger, C. et al.) vol. 9 69–86 (Springer, 2020).
van Oyen, H., Van der Heyden, J., Perenboom, R. & Jagger, C. Monitoring population disability: evaluation of a new Global Activity Limitation Indicator (GALI). Soz.- Präventivmedizin 51, 153–161 (2006).
EHLEIS team. Assessment of the GALI question used in SILC since 2008, www.eurohex.eu (2011).
Van Oyen, H., Bogaert, P., Yokota, R. T. C. & Berger, N. Measuring disability: a systematic review of the validity and reliability of the Global Activity Limitations Indicator (GALI). Arch. Public Health 76, (2018).
Hsiao, R.-L., Wu, C.-H., Hsu, C.-W., Saito, Y. & Lin, Y.-H. Validation of the global activity limitation indicator in Taiwan. BMC Med. Res. Methodol. 19, 52 (2019).
Sullivan, D. F. A single index of mortality and morbidity. HSMHA Health Rep. 86, 347–354 (1971).
Sanderson, W. C. & Scherbov, S. The characteristics approach to the measurement of population aging. Popul. Dev. Rev. 39, 673–685 (2013).
Acknowledgements
This work was supported by the European Research Council (Grant Number ERC2012-AdG 323947-Re-Ageing).
Author information
Authors and Affiliations
Contributions
All authors made a substantial contribution to conception and design. D.W. conducted the data analysis and modelling. All authors contributed to interpreting the results, drafting the manuscript and revising it critically.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Weber, D., Scherbov, S. Prospects of activity limitations among older adults in 23 low and middle income countries. Sci Rep 10, 10442 (2020). https://doi.org/10.1038/s41598-020-67166-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-67166-4
This article is cited by
-
A qualitative perspective of working women care providers and care receivers on eldercare: a study from India
BMC Geriatrics (2024)
-
The effect of long-term care insurance on healthcare utilization of middle-aged and older adults: evidence from China health and retirement longitudinal study
International Journal for Equity in Health (2023)
-
Using multiple imputation and intervention-based scenarios to project the mobility of older adults
BMC Geriatrics (2022)
-
Research to inform health systems’ responses to rapid population ageing: a collection of studies funded by the WHO Centre for Health Development in Kobe, Japan
Health Research Policy and Systems (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
